
Abstract
Culturally and racially responsive practice continues to be a common challenge among Mental Health Practitioners (MHPs). To the authors’ knowledge, this systematic review was the first to collate and synthesize clients’ perspectives of MHPs’ cultural and racial awareness and responsiveness from around the world. Original studies that were published between 2010 and 2021 reporting on qualitative data about clients’ perspectives regarding MHPs’ cultural-racial awareness and responsiveness were included in the review. The studies’ key findings that addressed this review’s question were synthesized and analyzed using reflexive thematic analysis. This review found 48 papers that met inclusion criteria, which represented the views of 652 clients across 10 countries. Three major themes and eight subthemes were established that concerned characteristics of the MHP, the client, and the therapeutic alliance. The results of this review indicate individual and systemic factors that influence mental health access for people from culturally and racially marginalized groups. Ongoing training of MHPs, increased racial and cultural representation among MHPs, inclusive physical settings, and reduced discrimination by MHPs are among the key findings and directions based on the results of this review.
Keywords
Racially and/or culturally marginalized groups often have poorer mental health than privileged groups (e.g., white people from Anglo backgrounds), yet less frequently seek assistance from Mental Health Practitioners (MHPs e.g., psychologists, counselors, social workers; Burkett, 2017; Narendorf et al., 2018). Common mental healthcare access barriers experienced by racially and culturally marginalized people include stigma, low familiarity with services, language barriers, racism, and discrimination (Colucci et al., 2017; Khawaja, 2007; Priebe et al., 2012). Although untreated mental illness alone culminates in complex negative outcomes, additional (common) experiences of racism and discrimination often worsens marginalized people’s mental health, educational, employment, social, and financial outcomes (Maura & Weisman de Mamani, 2017; Skiba et al., 2011). It is therefore vital that researchers and practitioners explore the perspectives of marginalized communities towards MHPs, to understand their healthcare needs and to help circumvent mental healthcare access barriers.
Current evidence suggests many MHPs do not readily recognize they lack the understandings and skills to address the experiences of racially or culturally marginalized people. Specifically, researchers in the USA (Newell et al., 2010) and Australia (Sadusky et al., 2021) have reported a training-practice gap between the amount of multicultural training provided to psychologists and the skills they require to successfully fulfil their role. Moreover, a review of tertiary-level counselling programs revealed that, while elements of multiculturalism are sometimes taught in the curriculum, ethnoracial issues relating to power, oppression, and social injustices are underrepresented across curricula (Motulsky et al., 2014). Consequently, many MHPs are not explicitly trained in the historical and current healthcare structures that have fostered racial supremacy (e.g., whiteness), which continue to hinder racially or culturally marginalized people from accessing adequate care (Gonzalez & Cokley, 2021).
Risk Factors for Poor Mental Health Among Marginalized Groups
Several factors can account for the higher rates of mental illness seen within racially and culturally marginalized groups compared to privileged groups. For example, migrants and refugees often arrive in their new country with a history of colonialism; displacement from family; and/or exposure to conflict, war, or terrorism (George, 2010; Sullivan & Simonson, 2016). These experiences increase the risk of mental illness for these people (Sangalang & Vang, 2017). Moreover, Indigenous people frequently experience higher rates of disadvantage, trauma, discrimination, and racism compared to non-Indigenous people, which negatively impacts their mental health (Herring et al., 2013; Paradies & Cunningham, 2012; Priest et al., 2011; 2013; Watego et al., 2021). Indigenous people have also endured chronic trauma related to colonization; genocide; forcible removal of Indigenous children from their families; the absence of treaties or acknowledgement of the invasion and continued occupation of Indigenous land; and ongoing injustices, systemic discrimination, and racism (Dudgeon et al., 2017; Menzies, 2019). In all, people who culturally and/or racially differ from the dominant (white) group often face many forms of systemic disadvantage which, in turn, fosters mistrust in mental health sectors that are often borne from the customs of the dominant group (Alang, 2019; Hui et al., 2021).
Mental Health Treatment for Marginalized Groups
Racially or culturally marginalized people receive substantially less mental health support than people who comprise the dominant culture. A large study that compared the utilization of mental health services between unaccompanied refugee minors (n = 920) and a Dutch adolescent control sample (n = 1059) found that nearly 60% of the refugee youth sample reported a need for mental health support, compared to only 8.2% of the Dutch sample reporting such needs (Bean et al., 2006). Even when marginalized communities access mental healthcare, the provided support is often of reduced quantity, quality, and/or appropriateness when compared to the care received by culturally or racially dominant group members (Lê Cook et al., 2014). For example, many MHPs utilize treatment protocols that were originally developed for white people (i.e., through Eurocentric and colonial lenses) and therefore can be culturally inappropriate for marginalized groups (Woods-Giscombe et al., 2016). Having negative experiences with mental healthcare services can subsequently reduce marginalized people’s trust in mental healthcare services (Woods-Giscombe et al., 2016) and thus deter them from seeking much needed support, which can exacerbate their mental health conditions (Alang, 2019). Finally, a disparity in the types of offered mental healthcare treatment has been observed (Holden et al., 2013). Specifically, marginalized groups tend to be less likely than white people to receive newer and more comprehensive treatment modalities, which can be attributed to racism and a lack of cultural or racial competency across MHPs (Holden et al., 2013). In all, research has repeatedly demonstrated a paucity in practices that are responsive to the needs of culturally and racially marginalized people (Miller & Berger, 2020) which, in turn, perpetuate injustices and disadvantages (Hui et al., 2021).
Mental Healthcare Professions and Marginalized Communities
The mental health profession has a long history of systemic racism (e.g., eugenics practices, race/IQ assertions) that likely contributes to its inadequacy in servicing marginalized communities, and in a psychologically safe or trauma-informed manner (American Psychiatric Association, 2022; Buchanan et al., 2021; Kinouani., 2021; Mensah et al., 2021; Roberts et al., 2020; Tinsley-Jones, 2001). The extent of systemic racism, discrimination, and stigma endured by marginalized people within the mental healthcare system has been publicly acknowledged, and apologized for, by authoritative psychology organizations including the American Psychological Association (APA, 2021; 2022) and the Australian Psychological Society (APS, 2016). MHPs, some of whom have been harmed by systemic racism themselves, have mixed reviews regarding the authenticity of these apologies but mostly agree that true reconciliation requires actions beyond apologies to help rectify the harm caused within mental health-related research and practice (Association of Black Psychologists [ABPsi], 2021; Buchanan et al., 2021; Carey et al., 2017; Dudgeon et al., 2017; Roberts et al., 2020; Tinsley-Jones, 2001). This highlights that more needs to be done in the mental health sector to increase access and delivery of appropriate services and treatment to racially and culturally marginalized people, towards eliminating oppression within the field.
Review Aims
As far as the authors are aware, there have been no systematic reviews that have collated and synthesized clients’ perceptions regarding MHPs’ cultural and racial awareness and responsiveness. The key limitations of research in this area have been that sample sizes are too small and/or findings cannot be extended beyond the race or culture that was examined. Thus, this systematic review aimed to collate clients’ voices, around the world, with the primary purpose of informing general global guidelines for how to develop and deliver appropriate mental healthcare services to culturally and marginalized people, and in ways that prioritize emancipation from hegemonic and hierarchical ideologies.
Employed Definitions in this Study
For this study, marginalized people was defined as “those excluded from mainstream social, economic, educational, and/or cultural life” due to racism, discrimination, and other forms of systemic oppression (Sevelius et al., 2020, p. 2009). Marginalization cannot happen without macrosystems that disproportionately advantage only certain groups (Nixon, 2019). Race was considered a non-biological, socially-constructed status (that often perpetuates white hegemony in society; Watego et al., 2021). Culture was defined as a dynamic and complex interaction between the acquisition and transmission of group knowledge, norms, and behaviors across time and context/s (Smedley & Smedley, 2005). Importantly, stable definitions for race and culture across the literature are elusive due to the plethora of experiences that can define these constructs in idiosyncratic ways (e.g., some people experience these constructs interconnectedly while others do not; Yared et al., 2020).
Method
This systematic review was conducted in the following order: database search, title and abstract screening, full text screening, data extraction, quality checking, data analysis, and reporting of the results. The protocol of this systematic review was registered in PROSPERO on 12 June, 2021 (for details, see https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021252705).
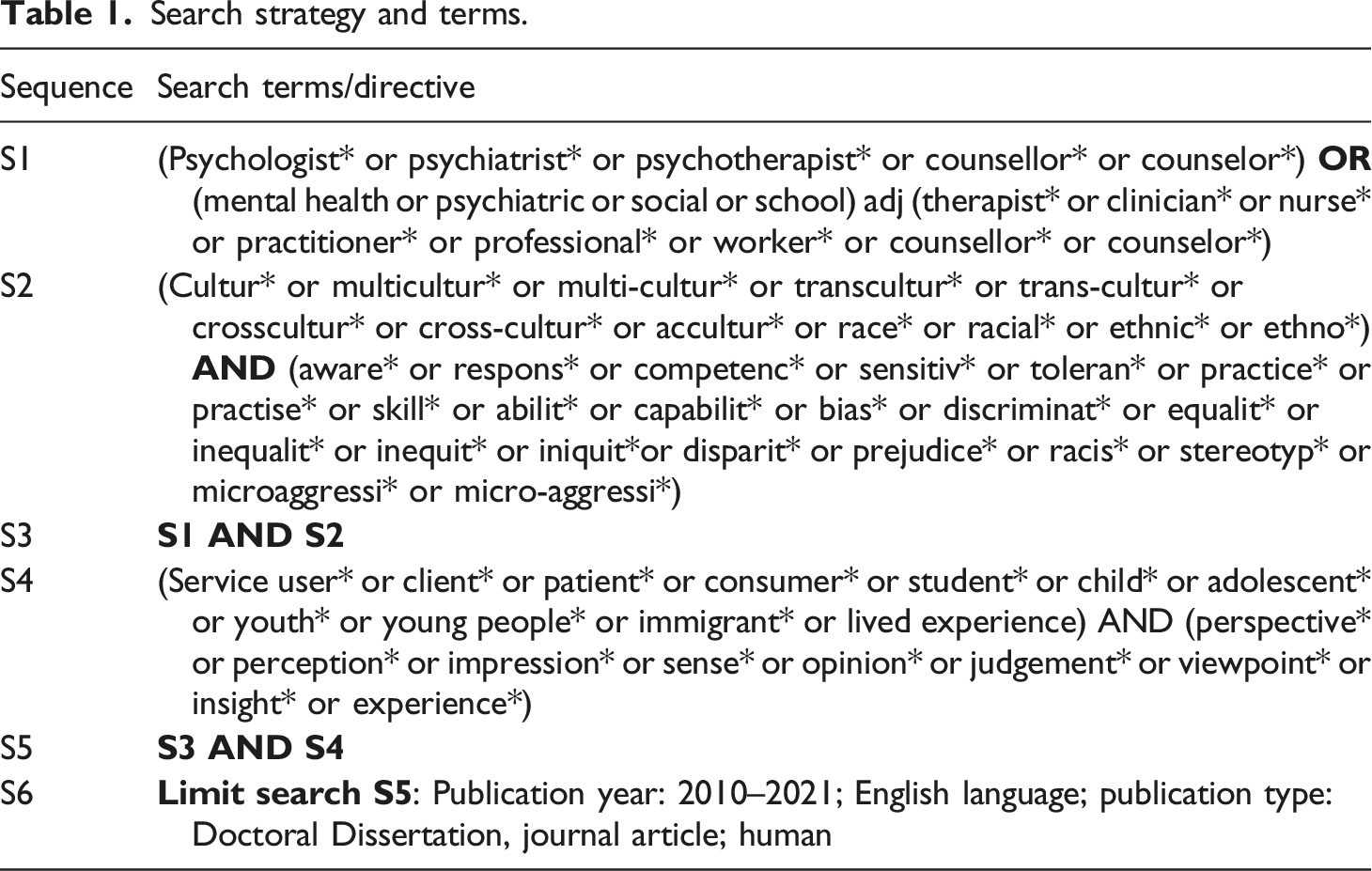
Database Search Strategy
Search strategy and terms.
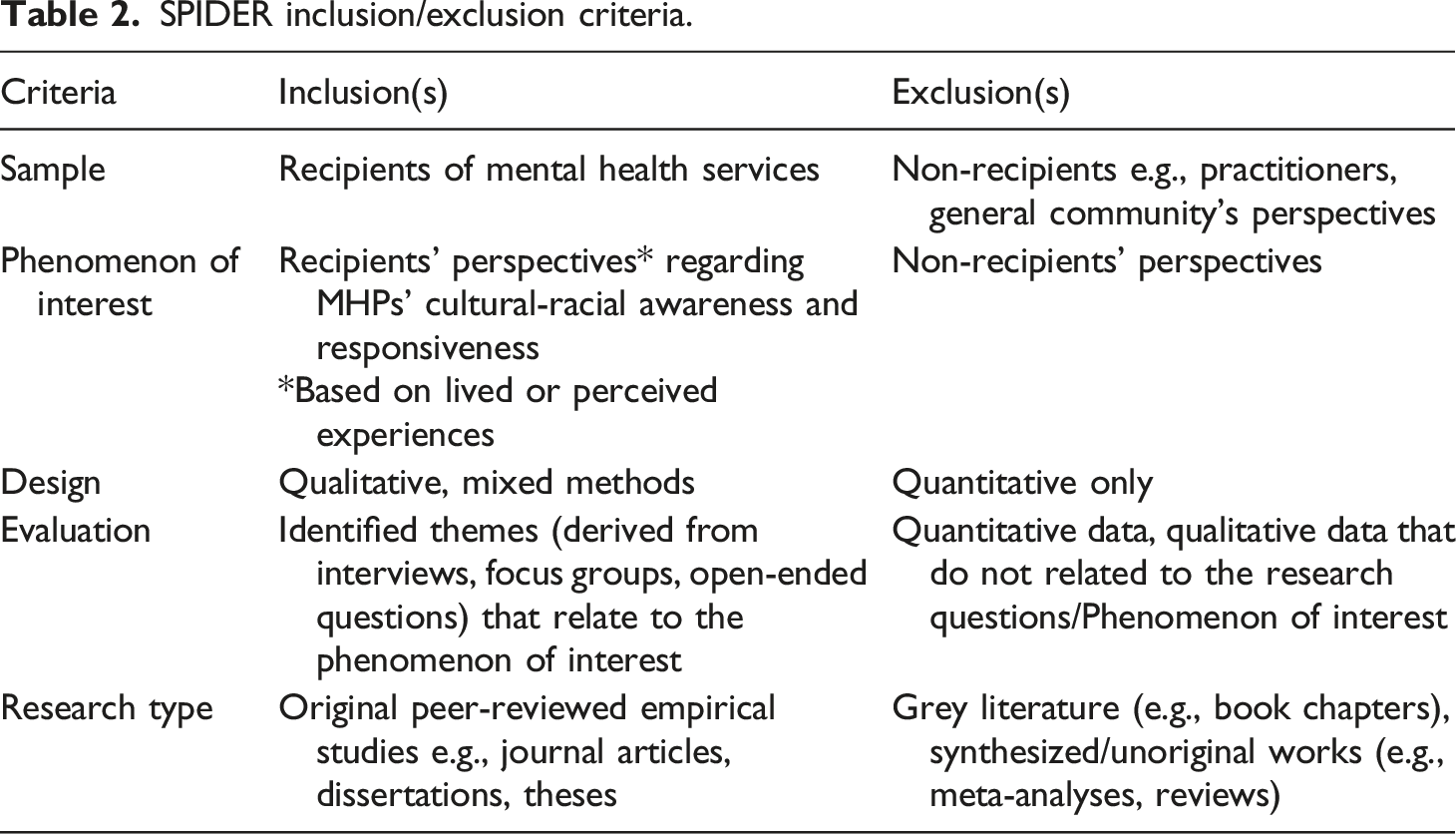
Inclusion and Exclusion Criteria
SPIDER inclusion/exclusion criteria.
Screening Strategy
All four authors participated in title and abstract screening and full text screening. During both the title and abstract, and full text screening phases (1) each author screened approximately a quarter of the papers, and (2) each paper was screened by two authors before proceeding to the next stage or being excluded. Where conflicts over inclusion/exclusion decisions occurred, a third author independently reviewed the paper in question (i.e., without feedback from the two authors who initially screened the record) and made the final inclusion/exclusion decision. Figure 1 illustrates how many papers progressed through each stage of the review. Covidence PRISMA flowchart of review Progression.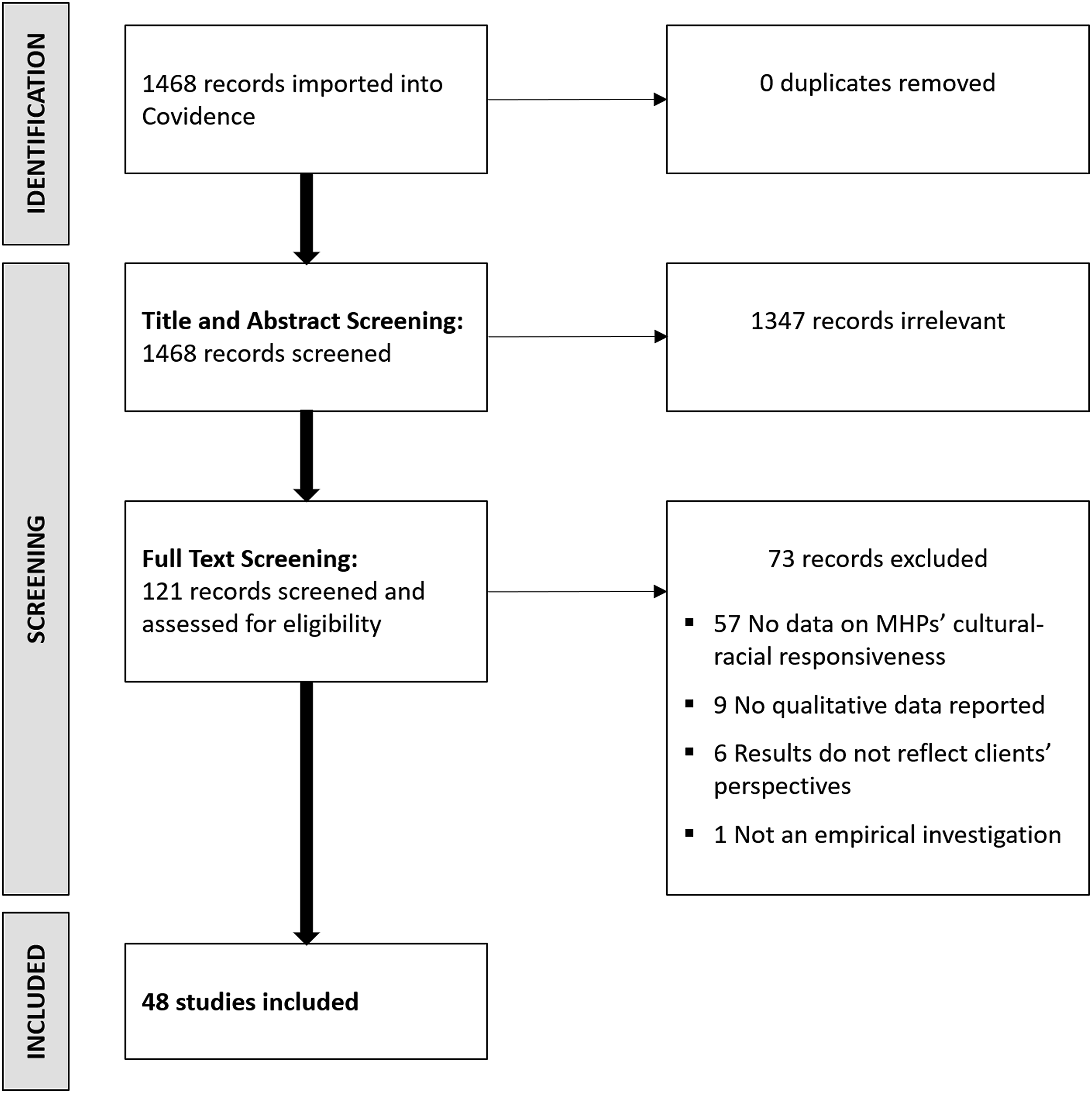
Quality Appraisal
Satisfactory CASP quality appraisal ratings (“Yes”) of included studies (n = 48).
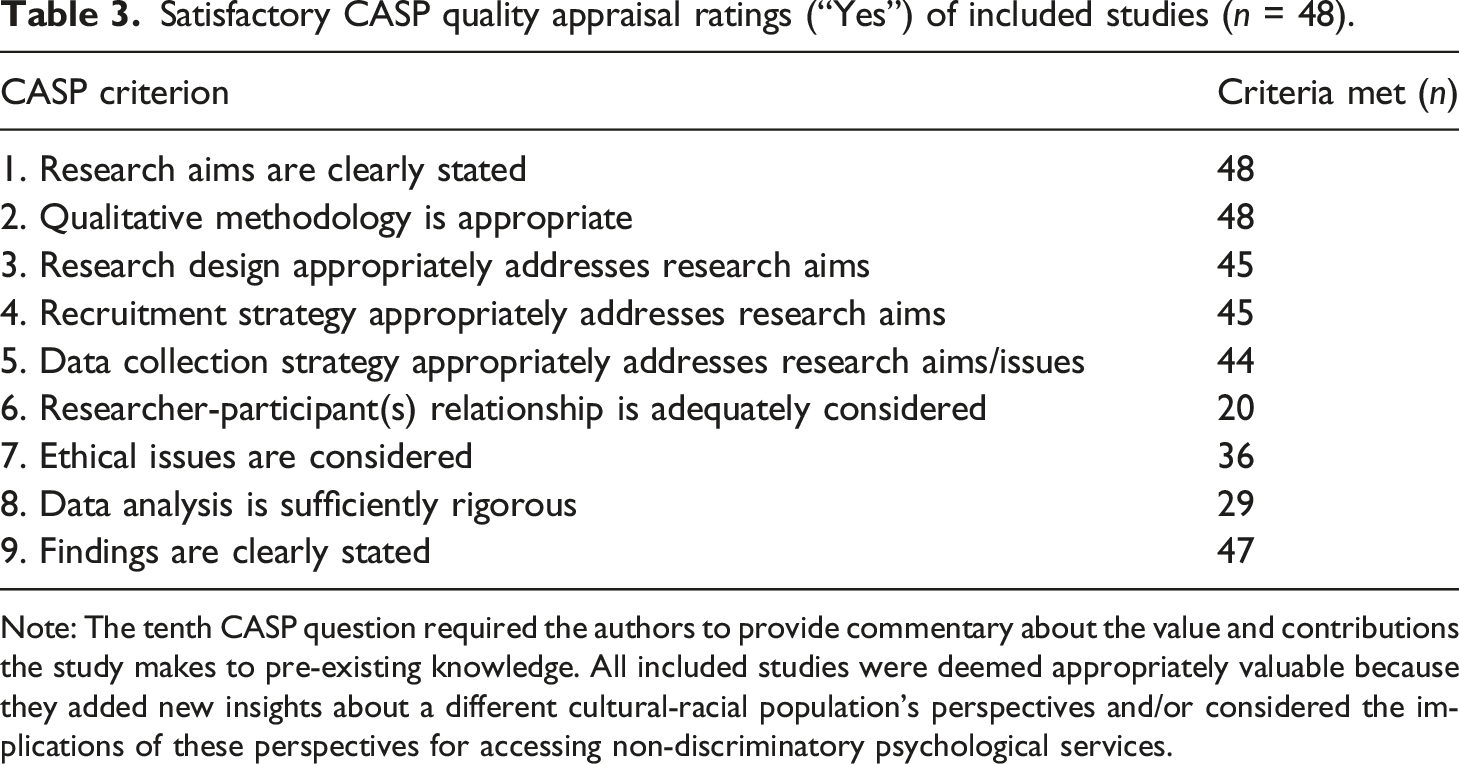
Note: The tenth CASP question required the authors to provide commentary about the value and contributions the study makes to pre-existing knowledge. All included studies were deemed appropriately valuable because they added new insights about a different cultural-racial population’s perspectives and/or considered the implications of these perspectives for accessing non-discriminatory psychological services.
Data Extraction
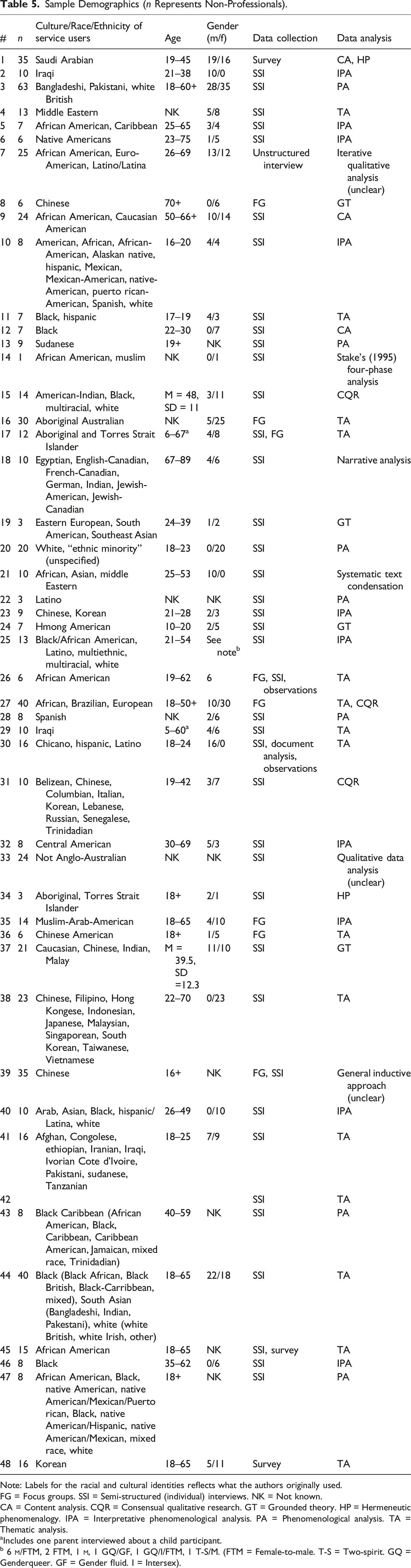
Three authors (AS, HY, and PP) and a research assistant (KO) each extracted approximately one-quarter of the included papers’ data into a shared spreadsheet. Each spreadsheet row represented one included paper, while each column contained a different type of extracted information. The data that was extracted from the papers included: • Demographics about the studies (e.g., country and participant/MHP characteristics; see Tables 4 and 5). • Key findings that related to this review’s research questions (i.e., the extractors’ initial coding efforts). • Excerpts and quotes that illustrated each study’s key findings. Paper demographics. Note: T = Thesis/dissertation. PA = Peer-reviewed journal article. CO = Counsellors. MD = Medical doctor (e.g., general practitioner, physician). MHC = Mental health clinicians. PSYC = Psychologists. PSYT = Psychiatrists. P/T = Psychotherapists/therapists (unspecified). SW = Social workers. NK = Not known. Sample Demographics (n Represents Non-Professionals). Note: Labels for the racial and cultural identities reflects what the authors originally used. FG = Focus groups. SSI = Semi-structured (individual) interviews. NK = Not known. CA = Content analysis. CQR = Consensual qualitative research. GT = Grounded theory. HP = Hermeneutic phenomenalogy. IPA = Interpretative phenomenological analysis. PA = Phenomenological analysis. TA = Thematic analysis. aIncludes one parent interviewed about a child participant. b 6

Data Analysis
Authors AS and PP conducted the data analysis using Clarke and Braun’s (2013) reflexive thematic analysis method. Data analysis was split into three phases: independent analysis by AS and PP, collaborative analysis between the two authors, and lastly team-based verification by AS, PP, HY and EB. Themes were discussed first between AS and PP and then between the entire authorship team until consensus was reached around the final set of themes and subthemes. Where necessary, the authors referred to original papers to assist them in making decisions about the inclusion and/or structure of themes and subthemes. Details about process used to derive themes, across all data analysis stages, are in the Appendix.
Authors’ Positionalities
All authors were involved in conducting this review and interpreting and reporting its findings. As such, it is important to highlight their positionalities in relation to this research, which may influence their perceptions of the results.
All of the authors are registered psychologists with the Board of Australia and practice on the unceded lands of the Kulin Nation. Their positionalities in relation to this investigation were as follows:
Andrea Sadusky (Author 1) identifies as a white, able-bodied woman and mother. She is Australian-born and has a Cypriot Greek ethnic background. Her relevant research knowledge includes critical disability studies which critique macrosystem-level oppressions that are parallel to those explored in this study.
Hannah Yared (Author 2) identifies as a second-generation Eritrean cisgender woman whose research explores race and racism within education and psychology. Her research is shaped by this Black settler/African-diaspora positionality.
Pamela Patrick (Author 3) identifies as an Indian, able-bodied cisgender woman who was born in Singapore. Her research expertise is in intergenerational transmission of mental illness. She currently counsels high school students from various cultural and ethnic backgrounds.
Emily Berger (Author 4) is a white Senior Lecturer with over 14 years’ research experience. She was born in Australia and comes from European ancestry. She has worked as a child and family psychologist in a variety of settings and with people from a variety of backgrounds and cultural groups for 8 years.
Results
Paper Demographics
Of the 48 papers included in the review, the majority (66.67% n = 32) were conducted in the USA and/or were peer-reviewed articles (60.42% n = 29). For details about each studies’ demographics (location, publication type, MHP types discussed, aims), see Table 4. Two included papers represented the same sample (i.e., Valibhoy, Kaplan, & Szwarc, 2017; Valibhoy, Szwarc, & Kaplan, 2017) but addressed separate research questions. If it is assumed that only Valibhoy, Kaplan, and Szwarc (2017) and Valibhoy, Szwarc, and Kaplan (2017) represented the same participants, and no other participant-overlap occurred between other studies, then this review synthesized the views of 652 clients across 10 countries. Except for one participant who described their 6-year-old child’s interactions with MHPs (Hepworth et al., 2015), all clients represented in this review were aged at least 16-years-old. Moreover, only five studies reported views of youth aged 17 years and younger. Table 5 details each study’s (1) participants’ demographics and (2) data collection and analyses methods.
The outcomes of the reflexive thematic analysis in this review resulted in three broad themes and eight subthemes. In describing the theme structure, a theme summary has been provided before details of each subtheme and representative quotes from participants. To accurately report the results, we have used the same terms as the original papers to describe participants’ racial, cultural, ethnic, or sexual identities; and/or the aims and outcomes. However, they acknowledge that preferences for terminology can vary between individuals and the original terminology adopted may not suit all people’s preferences.
Theme 1: MHP Factors – Knowledge, Skills, and Competencies
Many clients’ views about MHPs’ cultural and racial responsiveness were specific to behaviors manifested by MHPs. A sentiment commonly shared by clients was the need for MHPs to undergo training to enhance their cultural and racial awareness. MHPs who appeared to overestimate their knowledge about different cultural or racial groups tended to rupture the therapeutic alliance. Clients considered MHPs’ openness and willingness to listen as pivotal for the provision of culturally and racially responsive therapy.
Lack of Cultural and Racial Awareness and/or Training
Clients highlighted how some MHPs lacked the appropriate information to behave in a culturally safe manner. They often emphasized the need for MHPs to be educated about how various cultures and racial groups perceive mental healthcare services, and for these services to be tailored accordingly to meet clients’ needs: then I went to a psychiatrist … and it was amazing! It was the opposite of the first psychiatrist … in addition to paying attention to my current situation, she was also concerned with my situation here as an immigrant. – client’s race was unclear (Moleiro, 2013, p. 89, p. 89) I don’t think they [MHPs] had any clue of my background or anything like that or understanding Armenians or Lebanese … They don’t really have a clue of how many cultures really come from the Middle East, how many different backgrounds or religions or ways the cultures come from that area. I never felt any kind of understanding of that. – Armenian client from Lebanon (Boghosian, 2011, p. 70)
Some MHPs showed limited ability to be culturally responsive, such as not adjusting how directive they were when guiding clients. While some clients appreciated a non-directive approach, others expected a top-down approach whereby MHPs are viewed as experts who provide clients with explicit instructions: If the patient knows what to do, they wouldn’t come to you … they are more scared to make a decision than being told what to do because they don’t know what decision to make, [whether] it will be right or wrong. They don’t know, they don’t have the professional training. –East Asian client living in the USA (Tsai et al., 2017, p. 1045, p. 1045)
Overestimating One’s Cultural and Racial Knowledge
Several clients also noted how MHPs seemed to overestimate their cultural or racial knowledge, which was experienced as alienating and dismissive. For example, clients noted that some MHPs quickly assumed characteristics about them based on their cultural or ethnic background. This idea was articulated well by a Lebanese client whose MHP made homogenizing assumptions about clients from different cultural and ethnic backgrounds: She said she had a client who was Egyptian so I got a sense she knew she had dealt with this difference before. She didn’t make me feel like ‘Oh I understand,’ she kind of was just like ‘oh I heard this before, I’ve touched upon this before with another client.’ – Lebanese female client in the USA (Rogers-Sirin et al., 2015, p. 262, p. 262)
Openness to Listen
Clients did not expect their MHPs to know everything about their culture or race but appreciated it when practitioners acknowledged their limited understanding and invested effort into listening more about the client’s background. When MHPs expressed curiosity and openness to listen about their client’s cultural or racial backgrounds, clients reported feeling seen, respected, and validated as unique individuals: [My counselor is] open to my beliefs. And without her open to my beliefs it would make an impact on my mental health care. So it does make a big difference how I believe and how she views that. Like if she didn’t believe it, then that would create a big gap in our communication. And I’m afraid that it would affect it so much that I’d probably either have to go to somebody else or someone that did believe in what I believe in. – American Indian client (Hack et al., 2014, p. 72, p. 72)
Theme 2: Client Factors – Apprehension Towards MHPs
Clients’ perceptions of MHPs’ cultural and racial awareness were further shaped by their preconceived notions and/or lived experiences concerning mental healthcare services. These indirect and direct experiences of MHPs subsequently influenced clients’ willingness to engage in therapy. Specifically, clients who held negative views about MHPs felt apprehensive about engaging in mental healthcare services due to fears of being stigmatized, discriminated against, and otherwise further marginalized due to racism.
Preconceptions about MHPs
Preconceived fears and assumptions about what mental healthcare services entail shaped clients’ willingness to engage in therapy. Some of these preconceptions were culturally-derived, as illuminated by a refugee who stated, ‘‘it’s deeply rooted in our society that if you see a psychologist you’re crazy’’ (Valibhoy, Kaplan, & Szwarc, 2017, p. 28). Moreover, many clients viewed therapy as a Western practice (for white people) and preferred other methods for navigating hardships that were more responsive to their needs (e.g., seeking the advice of religious leaders). These concerns were not always based on first-hand experiences but, instead, the experiences of others in their community and/or media representations of MHPs: I’d rather go to the Imam because he knows more than me about my religion, and I want him to give me a solution about what my religion tells me is better for me, that’s what I think, not to go to the counselor. – Nigerian Muslim client (Turkes-Habibovic, 2011, p. 125, p. 125) [Y]ou get most of your ideas from the media . . . The idea of you sitting down, you’re laying down on a bed and there is a person who just sits there like a statue recording what you say . . . I came in—with those ideas about mental health—and how it just seems like a very silly profession that would not help you at all. – Client who is a refugee living in Australia (Valibhoy, Kaplan, & Szwarc, 2017, p. 28). I already had this preconceived notion … I came in like ‘you don’t understand me … I was cautious. I already had a wall up. I already figured she wasn’t going to understand me. – Native American Indian client describing their experience with a non-Native counselor (Bushey, 2018, p. 67, p. 67)
Direct Experiences with MHPs
Some clients had experiences of feeling judged and misunderstood on the grounds of their cultural or racial identity. In some instances, clients perceived MHPs’ negative judgments through their body language and facial expressions: …made him make a face at me and I didn’t see that that was very polite way to go about that. I kinda thought that was rude, but he just made it obvious how he felt about that. – Mexican-American client (Crans, 2013, p. 70, p. 70)
In other instances, clients’ feelings of being misunderstood emanated from MHPs being unaware of their positionality and power imbalances in the counseling dynamic and the experiences of their clients that are shaped by historical and current systems of oppression. This is illuminated by a Black woman describing her white counselor: Because as a white woman, first of all, she didn’t understand where I was coming from. So, to me, it’s a waste of time-I totally hated it! White women always had a stigma against Black women. (McGee, 2013, p. 67, p. 67)
Importantly, not all clients’ experiences of MHPs’ reactions to their cultural customs resulted in negative outcomes. In these instances, circumventing unpleasant client experiences appeared to be due to the MHPs’ willingness to listen and the establishment of a strong therapeutic alliance: She was definitely shocked to hear about um my family’s tradition of marriage … but she didn’t she didn’t let it affect uh, she just mostly expressed interest in what I had to say, it didn’t seem like she was disapproving. – Mexican-American client Crans, 2013, p. 73, p. 73)
Theme 3: Inter-Relational Factors – Therapeutic Enablers
Several factors shared between MHP and clients were perceived by clients to augment the therapeutic alliance and were experienced by clients as culturally and racially responsive practices. These included the physical environment, clients having a shared identity with the MHP, and the MHP showing unconditional positive regard for clients from racially and culturally marginalized backgrounds.
Physical Environment
Clients reported that the physical environments of MHPs’ consultation rooms were important for acknowledging and welcoming their cultural and racial identities. In turn, clients felt represented and validated within the therapeutic space. Latino/Latina students discussed the importance of “various displays and objects on the walls and around the offices” (Peña & Rhoads, 2019, p. 197) that were important in validating the cultural and racial identity of students. Others pointed at the presence of pictorial representations, such as images of diversity and flags of various countries, as well as the pride flag, as being significant markers of fostering an inclusive and welcoming space. Furthermore, a culturally and racially safe environment was also regarded as important in enhancing participation and adherence to therapy.
Shared Identity with MHP
Some clients reported it was valuable to their therapeutic journey when their MHP had a shared identity to them (e.g., with respect to ethnicity, race, immigration status, and socioeconomic status). Specifically, when MHPs self-disclosed their racial or cultural identities to clients, clients often noticed shared experiences which made them believe their MHP had a better understanding of them and their viewpoints. Moreover, clients felt more personally connected and comfortable with their MHP when they knew they had similar racial or cultural experiences, as articulated by a Latino client: …maybe they have struggled or they are like me, I feel more connected to them. I actually feel comfortable going to their office and asking for help. (Peña & Rhoads, 2019, p. 197, p. 197)
The importance of a shared identity appeared to extend beyond cultural or racial identity to include intersecting identities such as gender as well: It was all the more important to be with somebody who is trans and who has struggled with the different aspects of that experience. – genderqueer/intersex/female-to-male client whose racial and cultural identity was unspecified (McCullough et al., 2017, p. 427, p. 427)
The reverse also applied. That is, when clients perceived MHPs as having dissimilar cultural or racial identities and experiences to them, they felt unconfident or wary that the MHP would not have the capability to comprehend their experiences. Subsequently, some clients expressed disconnection from, or uncertainties towards, MHPs who had a different racial or cultural background to their own: I thought she seemed a little privileged and she may not understand some of the issues I came in there with … I was thinking, “Well, she has probably never had to deal with that, so she doesn’t know.” … I felt more comfortable with the Native counselor than I did with the non-Native. – Native American Indian client (Bushey, 2018, p. 68, p. 68) I wanted to practice oral English when seeking counseling...but now, after counseling, I would like to have counselors who are from Chinese or Asian backgrounds. At least we share similar family values, and he/she can understand what I talk about ... this is not usually an option. – Chinese client (Liu et al., 2020, p. 283, p. 283) I think it would seem likely for me to relate to somebody who was Trinidadian or even a Caribbean professional. I probably would have more likely stayed in counseling or more likely to have discussed more things. – Black client (Venner & Welfare, 2019, p. 652, p. 652)
Therapeutic Alliance
Clients appreciated empathy from MHPs. Specifically, clients reported trust and psychological comfort when MHPs demonstrated unconditional respect, listening, and genuineness. When MHPs were perceived as warm and trustworthy, clients felt more confident to honestly disclose their innermost thoughts and feelings: he was bright and caring and seemed to take more of an interest in me, and probably all his patients, than I would have thought another therapist would. So I was impressed by his professionalism and I was impressed with his sincerity. – White Jewish client (Hunter, 2011, p. 65, p. 65) I was talking a lot [while] she was listening. She had a great memory … so she was listening and she was definitely interested … She was warm and kind and … I feel like she wants to help me. – Client from Senegal who migrated to the USA (Rogers-Sirin et al., 2015, p. 264, p. 264)
Discussion
The current study systematically collated clients’ perceptions of MHPs’ cultural and racial awareness and responsiveness from around the world. From the 48 studies conducted across 10 countries, three broad themes and eight subthemes emerged that concerned ‘MHP factors’, ‘client factors’, and their combined interaction, referred to as ‘inter-relational factors’. Our findings overwhelmingly indicated that barriers exist for racially and culturally marginalized people who are accessing mental healthcare. Our findings also highlight some ways that MHPs can begin to engage in practices that are culturally and racially safer by (1) listening to the voices of marginalized clients, (2) engaging in professional development, and (3) showing humility in their level of cultural and racial knowledge. While these practices will not address all the barriers that marginalized people face when accessing mental healthcare services, doing these things will assist in providing safer and more accessible therapeutic spaces for marginalized clients.
Barriers to Cultural Safety
Many clients reported that their MHPs did not understand the nuances of their racial and/or cultural backgrounds. This was evidenced through MHPs having no deep understanding about the cultural or racial backgrounds of their clients and/or making homogenizing and stereotyped assumptions about their clients’ experiences and needs. These assumptions often led to MHPs making racialized comments that negatively impacted their clients’ trust in the therapeutic process and threatened their sense of cultural or racial safety. Moreover, inaccurate and/or stereotypical assumptions appeared more common when MHPs had an inflated sense of cultural or racial competency than when MHPs humbly acknowledged gaps in their knowledge (i.e., showing cultural humility; Tervalon & Murray-García, 1998). This could explain why clients seemed more receptive to therapy when MHPs accepted limitations in their knowledge of different cultural and racial groups and subsequently strove to address these by listening to perhaps learn more about these groups.
This study found that clients’ lived or vicarious experiences of discrimination and maltreatment from MHPs fueled their perceptions that MHPs lacked adequate cultural and/or racial competency. These marginalizing experiences also increased clients’ apprehension towards MHPs and mental healthcare services. This finding aligns with research that shows marginalized clients, especially Indigenous people, experience mental healthcare settings that are often uninviting, impersonal, and culturally unsafe (Curtis et al., 2019; Kendall & Barnett, 2015). Moreover, the present findings suggest that MHPs are capable of being racist or discriminatory toward clients, which has the potential to cause harm and disrupt the therapeutic alliance. This inference is further reinforced by our finding that clients reported feeling safer and more welcomed when therapeutic spaces physically portrayed messages of inclusion and anti-racism. The importance of visual displays in creating a welcoming and accepting environment has been found in earlier research (e,g., Miller & Berger, 2021).
Promoting Cultural and Racial Awareness and Responsiveness
This review found that MHPs who had a shared racial or cultural identity with their clients were perceived to have greater insight into their clients’ experiences of marginalization when compared with MHPs with dissimilar backgrounds. Unsurprisingly, the latter group of MHPs were thus perceived and/or observed to have limited skills for addressing their clients’ needs, which parallels indications that MHPs lack sufficient responsiveness training (Newell et al., 2010; Sadusky et al., 2021). Although identity-matching between clients and MHPs has clear benefits (e.g., increased comfort in accessing mental healthcare), a lack of shared identity does not necessarily inhibit MHPs from working effectively with marginalized clients. Specifically, this review highlighted that genuine empathy and warmth from MHPs can assist in helping culturally and racially marginalized clients feel comfortable, thus echoing the importance of empathy in nurturing the therapeutic alliance (Elliott et al., 2018). It is therefore incumbent on MHPs to recognize their limitations in their knowledge of different cultural and racial groups and be willing to pursue professional development that addresses these gaps.
Addressing Whiteness in Mental Healthcare
The three broad themes identified in this study included evidence of whiteness within the mental healthcare sector. To understand marginalized clients’ worldviews and preferences, MHPs must first become self-aware of their own assumptions, values, prejudices, perspectives, and social positionality that are informed by their racial and cultural backgrounds and more (Roysircar, 2009). Such self-awareness can help reduce harmful in/actions from occurring that can impede marginalized clients’ mental health outcomes (Roysircar, 2009).
In addition, given clients’ preferences for therapists who have similar lived experiences of marginalization, creating equitable access to MHP tertiary training should be prioritized for marginalized people looking to practice as MHPs. This is especially crucial as people from racially or culturally marginalized groups encounter significant tertiary education access barriers due racism from academic processes (e.g., publication, teaching), spaces (e.g., white-centric curricula), peers, and educators (Buchanan et al., 2021; Cameron & Robinson, 2013; Consoli & Myers, 2022; Constantine et al., 2008; Constantine & Sue, 2007; DeLapp & Williams, 2015; Dudgeon & Walker, 2015; Gillborn et al., 2021; Roberts et al., 2020; Tinsley-Jones, 2001; Wainwright et al., 2012).
Although such reflexive practices and increases in representation can be useful at the micro-transactional or interpersonal levels, it is important to note that they do little for addressing the structural inequities and barriers faced by racially or culturally marginalized clients or MHPs themselves (Truong et al., 2014). Thus, a multifaceted approach that addresses both individual and systemic barriers is needed.
Limitations of this Review
Most of the included studies were conducted in the USA and with adults and thus limits the extent to which the results of this review can be generalized to other countries or age groups. There was also heterogeneity in the types of MHPs of interest and the cultural/racial backgrounds of participants, which limits inter-study comparisons. Moreover, the included studies did not uniformly report the racial or cultural identities of the MHPs that the participants provided their perspectives on. Consequently, it remains unclear in this study whether there are differences in cultural and racial competency between MHPs from different backgrounds – a topic which could be explored in future research. Further, only 20 of the 48 included studies adequately reported the positionality of the researcher(s), which rendered it challenging to determine how this may have affected their interpretations of their results. Finally, due to the lack of consensus regarding the definitions of race, ethnicity, nationality, and culture (Yared et al., 2020), comparisons between studies’ outcomes are limited due to likely differences in how these constructs were operationalized. Notwithstanding these limitations, this review can guide future research focusing on specific subgroups of MHPs and clients from different cultural or racial backgrounds.
Conclusion and Future Directions
Historically, research has tended to focus on MHPs’ perceptions of their own cultural competencies (Benuto et al., 2018; Lee & Khawaja, 2013). Although valuable, such research remains fraught with social desirability bias, self-report bias (i.e., MHPs cannot report what they are unaware of about themselves) and fails to emphasize an emancipatory agenda which places clients’ voices as the central foci (Truong et al., 2014). Thus, this systematic review provided a unique analysis of service users’ experiences of MHPs’ cultural and racial awareness and responsiveness.
The findings of this review have important implications for future practice and research, at the global level. Given the benefits of identity-matching between clients and MHPs, it is imperative that the training and recruitment of marginalized MHPs is increased. Moreover, preservice tertiary courses and MHP registration boards should incorporate mandatory cultural and anti-racism training to help equip MHPs with adequate knowledge to support marginalized clients and help dismantle systemic barriers to equitable care. Specifically, such training should include information about information at the individual level (e.g., cultural customs) and systemic level (e.g., racism, power, whiteness, privilege) to be comprehensive and effective (Curtis et al., 2019; Truong et al., 2014). Physical environment also played an important role for clients’ feeling comfortable, and the established body of research on this topic should be consulted for guidance in creating culturally and racially safe spaces for marginalized clients (Hall et al., 2016; Wexler & Gone, 2012; Zigarelli et al., 2016). Finally, future research would benefit from a continued focus on the perspectives and experiences of marginalized communities to place their voices at the center of finding solutions to meet their idiosyncratic mental healthcare needs.
Footnotes
Acknowledgements
The research team acknowledges and thanks Dr. Katelyn O’Donohue for her time and assistance in the data extraction process.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Given the nature of the data collected in this review, this study was exempt from requiring approval from an ethics committee to be conducted.