
Abstract
Funding problems are increasingly affecting major international organizations (IOs). From the World Food Programme (WFP) to the United Nations Educational, Scientific and Cultural Organization (UNESCO), many IOs are today forced to rely on closely earmarked and unpredictable sources of funds, with negative implications for their functioning. However, these challenges are neither unprecedented nor uniform in their causes and consequences. Drawing on literature on delegation, performance, and the earmarked funding of IOs, we propose a sequential process whereby preference heterogeneity among an IO’s stakeholders leads to heightened donor control through funding, which, in turn, reduces IO autonomy and performance. Empirically, we illustrate how major state and non-state actors have often used money as a control mechanism in the absence of influence via weighted voting or formal voting rights. With a longitudinal case study of international health institutions spanning from the 1920s to the 2010s, we examine—drawing from primary including archival sources—how the League of Nations Health Organisation (LNHO) and the World Health Organization (WHO) have repeatedly had to contend with irregular and conditional funding. We also investigate how this has undermined their autonomy and to what extent it has impaired their performance. The article contributes to the literature by offering a clearer understanding of the causes and consequences of IO funding practices, providing an in-depth, longitudinal analysis of IO funding in global health, and elucidating the sustained impact of non-state actors as influential sources of funding.
Keywords
Introduction
International organizations face mounting challenges in securing predictable and sustainable funding. Institutions like the United Nations (UN) specialized agencies are increasingly reliant on voluntary and typically earmarked contributions, often at the expense of assessed, predictable funding. These shifts in funding patterns have raised concerns about the autonomy and performance of IOs, with implications for their ability to address global challenges effectively. Although the often-negative causal effect of earmarked funding is relatively well-documented (Baumann and Weinlich, 2020; Ege and Bauer, 2017; Reinsberg and Siauwijaya, 2024; Schmid et al., 2021), the underlying mechanisms linking funding modalities and IO performance require further refinement. Our research addresses this desideratum by asking (a) how and why IO stakeholders use funding practices—particularly earmarked funding—to control IOs and (b) the extent to which this can affect IOs’ autonomy and performance.
This article makes three key contributions to the study of IO governance and funding. First, we contribute to theories of funding “substitution,” that is, the use of funding for control over an IO when the latter is not feasible via voting (Graham and Serdaru, 2020), by systematically incorporating the role of non-state actors, such as philanthropic foundations. This integration is essential because non-state actors increasingly drive IO activities yet remain undertheorized, despite their distinct operational logic. Non-state actors increasingly influence IOs through earmarked contributions, often introducing complexities beyond traditional state-centered models of principal-agent relationships (Patz and Goetz, 2019). Second, we refine conventional views that earmarking generally undermines organizational performance by developing a conditional perspective. Specifically, the effects of earmarking depend on the heterogeneity of preferences among the IO’s stakeholders and donors’ subsequent active use of funding for control. This theoretical refinement clarifies when earmarking can align with IO priorities, advancing understanding of earmarking’s nuanced impacts. Third, our unique longitudinal case study of international health governance fills an empirical gap left by predominantly ahistorical IO scholarship. Covering a century of international health, we clarify how funding practices evolve, persist, and influence IO autonomy and performance. Analyzing the LNHO and its successor, WHO, from the 1920s to the 2010s, we uncover how evolving stakeholder preferences and funding practices have shaped IO autonomy and performance across time.
The article proceeds as follows. In the Literature and new theoretical insights section, we lay the theoretical groundwork by reviewing the literature on earmarked IO funding and outlining key expectations about the use of funding for control and its effects on organizational autonomy and performance. We propose a sequential process linking stakeholders’ preferences, donors’ funding practices, and their effects on IOs’ autonomy and performance. The Research design section details the methodological approach and empirical data. In the Empirical analysis section, an in-depth case study is presented, beginning with LNHO’s historical challenges and strategies concerning funding and then examining WHO’s financial evolution from the 1960s to the 2010s, focusing on changes in funding sources and modalities and their impacts on WHO’s autonomy and performance. The conclusion synthesizes the findings and considers their broader implications for IO research and practice.
Literature and new theoretical insights
Earmarking in IOs: funding at what cost?
All international organizations require funding to fulfill their mandates (Reinsberg, 2023). Broadly, we distinguish funding along two dimensions: assessed versus voluntary and core versus earmarked. Assessed contributions are mandatory payments from member states based on pre-agreed criteria, while voluntary contributions are optional payments from state and non-state donors. Contributions are further differentiated by their flexibility. Core resources are unrestricted funds provided by donors, typically allocated at the discretion of the organization’s leadership and constituting the primary financial foundation of IOs (Haug et al., 2022). By contrast, earmarked resources are funds designated by donors for specific purposes and projects. Earmarked funding allows donors to specify how the funds should be utilized and requires the organization to achieve particular objectives or adhere to specific methodologies. Earmarked resources commonly take various forms, including trust funds 1 (Eichenauer and Hug, 2018; Reinsberg, 2017b; Reinsberg et al., 2017), multi-bi funding 2 (Barder et al., 2019), special funds (Wakolbinger and Toyasaki, 2011), and general private funding (Seitz and Martens, 2017).
Over the past decades, governments and non-state actors have increasingly turned to earmarked funding as their preferred mechanism to finance IOs and influence their operations and strategies (Figure 1). This trend has attracted scholarly attention. Existing research highlights the growing dominance of earmarked funding across a broad range of institutions (Heinzel et al., 2023), from generalist institutions like the World Bank (Barder et al., 2019; Reinsberg, 2017a, 2017b; Reinsberg et al., 2017; Wagner, 2016) and the United Nations Development Programme (UNDP) (Baumann, 2021; Schmid et al., 2021) to agricultural development agencies (Reinsberg, 2023), humanitarian organizations (Besiou et al., 2014), international climate finance bodies (Graham and Serdaru, 2020), and global health institutions (Chi and Bump, 2018; Daugirdas and Burci, 2019; Sridhar and Woods, 2013).
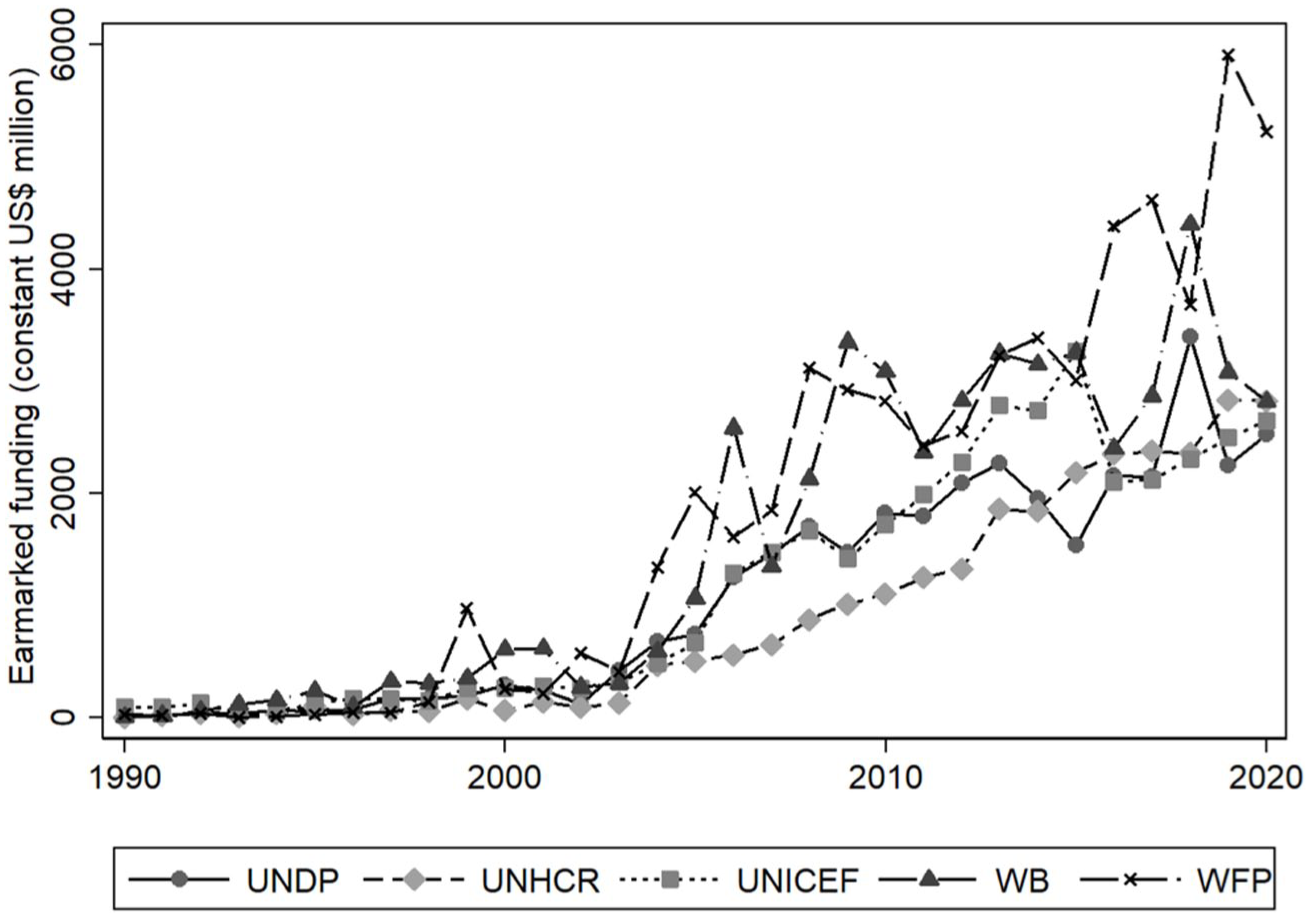
Top five IOs in terms of earmarked funding.
Although academic interest in earmarked funding has grown only recently, the practice itself is not new. As Graham (2017) documents, flexible funding arrangements granting states more control began spreading in the UN system in the late 1950s, with organizations like the UN High Commissioner for Refugees (UNHCR) favoring a less rigid approach over budgetary matters to maintain state support. Despite these early developments, few studies have taken a longitudinal perspective on the evolution of funding structures. Notable exceptions include Graham (2017), tracing changes in funding rules within UN economic development institutions from 1946 to 2010, and Bayram and Graham (2017), examining US funding practices toward the UN between 1946 and the 1980s. However, much literature on earmarked funding adopts the early 1990s as a historical starting point (Eichenauer and Reinsberg, 2017; Heinzel et al., 2023; Reinsberg et al., 2024), attributing the rise of earmarking to the diffusion of neoliberal reforms promoted by international development organizations (IDOs) (Jakupec et al., 2020). While the expansion of earmarking has accelerated in recent decades, neglecting the earlier, gradual development of such practices risks overlooking that often donor preferences for more flexible funding mechanisms emerged alongside the IOs themselves. In this respect, our work moves beyond the usual temporal scope by examining the role and diffusion of earmarked funding in global health since the early 20th century. We argue that adopting this diachronic lens enables us to better identify the possible sequential and time-specific steps shaping donors’ decisions to channel resources through earmarked contributions.
Scholars have also explored the drivers of earmarking. Earmarked aid serves multiple purposes (Eichenauer and Reinsberg, 2017). Most often, donors use earmarked contributions to exert influence, leveraging financial resources to shape the policy agendas and operational practices of multilateral institutions (Reinsberg, 2017b). For example, Chi and Bump (2018) and Wagner (2016) show how earmarking can distort aid allocation criteria away from traditional concerns like fairness, performance, and efficiency. Graham (2017) and Bayram and Graham (2017) find that earmarking becomes more likely when donors seek to expand an organization’s scope of activity or when their preferences diverge from those of the prevailing decision-making coalition. Similarly, Reinsberg et al. (2017) argue that states use earmarked funding to assert their specific national interests in particular policy areas and development goals. Baumann (2021) identifies three mechanisms sustaining earmarking practices: collective action breakdowns, evolving norms of appropriateness, and institutional fragmentation. Some studies have also examined how egalitarian voting rules relate to permissive earmarking regimes, with mixed findings—both positive (Graham and Serdaru, 2020) and negative (Eichenauer and Hug, 2018). While these and other studies examine donor motivations, most focus primarily on sovereign governments as the key actors (Reinsberg et al., 2024). However, although states remain the primary source of earmarked funding, they are not alone. Multilateral institutions, public-private partnerships, and non-state actors have become significant contributors to earmarked financing (Weinlich et al., 2020). Our work expands upon this literature by emphasizing the role of non-state actors—particularly philanthropic foundations—in the diffusion and institutionalization of earmarking practices within global health governance. This expansion is especially relevant as non-state donors may follow distinct and undertheorized rationales for engaging in earmarking. By broadening the analytical scope accordingly, our study develops a more comprehensive understanding of the diverse drivers leading different types of donors to favor earmarked contributions.
Finally, scholars have examined the consequences of earmarked funding for recipient organizations and multilateralism more broadly. Several studies assess how funding structures impact IO performance. For instance, Reinsberg (2023) finds that earmarked contributions generally impair both outcome and process performance, although the effects vary depending on organizational context and performance dimension. Similarly, Reinsberg (2017a) and Reinsberg and Siauwijaya (2024) argue that earmarked resources distort programmatic priorities away from recipient needs and raise transaction costs for IO staff. Heinzel et al. (2023) also highlight increased administrative burdens, while Schmid et al. (2021) emphasize that earmarking leads to financial volatility, unrecouped overhead costs, and intensified inter-organizational competition. This article expands upon this literature by zooming in on the conditions that make earmarking “bad” for performance.
This section has reviewed key scholarly findings on the scope, drivers, and consequences of earmarked funding across policy domains and time. Theoretically and empirically, this article aims to advance scholarly understanding by (a) identifying the specific mechanisms that link donor preferences, funding modalities, and the performance of international organizations; (b) presenting a longitudinal historical case study of earmarked funding in global health governance; and (c) highlighting the critical—yet often overlooked—role of non-state actors in shaping this trajectory.
Earmarking in IOs: theoretical refinements
Our theoretical approach captures the complex relationship between an IO’s stakeholders’ preferences, funding practices, and their effects on IOs’ autonomy and performance. Focusing on funding-related instruments donors use to exert control over IOs, we show how they often impair IO autonomy and, in turn, performance. However, we show how this process is not automatic. When donor objectives broadly align with the IO’s core mission, earmarking can enhance performance by supporting targeted initiatives without compromising autonomy. Our analysis centers on practical rather than formal-legal changes, aligning with Graham’s (2023) finding that it is funding practices (rather than just rules) that undermine UN multilateralism, and Lall’s (2023) finding that de facto autonomy, rather than de jure autonomy, is what influences IO performance. The remainder of this section introduces our key concepts, theoretical refinements, and theorized sequential process.
Key concepts
Many international institutions, particularly within the UN system, operate under “egalitarian norms” (Graham and Serdaru, 2020), where decision-making follows a one-country-one-vote rule, requiring broad consensus among member states for collective action. In this context, donors may want to exert bilateral financial control individually. When significant disagreement (preference heterogeneity) arises among donors about the institution’s mission or mandate, they often resort to using financial contributions as a substitute control mechanism. Importantly, this logic extends beyond state donors to include non-state ones, such as public-private partnerships and private foundations, which have gained increasing prominence in the international system. Therefore, what matters is preference heterogeneity not only among member states, but among the various state and non-state actors involved with an IO (i.e., the IO’s key stakeholders 3 ). For instance, when non-state donors’ preferences diverge significantly from those of donors with voting rights, we expect a greater use of individual control through funding, similar to the case of a member state with frustrated divergent preferences.
For the IO, more donor control via funding due to higher preference heterogeneity among its stakeholders may lead to reduced de facto autonomy (henceforth autonomy). 4 Intuitively, autonomy is closely tied to the quantity and quality of funding, as these factors directly impact an IO’s staffing (Ege and Bauer, 2017) and agenda-setting (Lall, 2023). Key dimensions of autonomy then include the quantity and quality of funding, whereby more flexible and predictable funding corresponds to higher autonomy, the number of staff and quality of their contracts, whereby proper staff with long-term contracts contribute to greater autonomy than non-staff and short-term contracts, and de facto agenda-setting power, whereby an IO is more autonomous when it can determine and implement its thematic priorities.
For our analysis, it is crucial to qualitatively assess autonomy, evaluating how donor-control mechanisms shape autonomy and, consequently, IO performance. We define performance as the IO’s progress toward its organizational outcome preferences, observable through the successful implementation of key programs, achievement of stated objectives, and effective allocation of resources. 5 While high levels of donor control via funding do not necessarily hinder individual project success, they often lead to efficiency losses and a drift from organizational goals as the IO becomes increasingly subject to individual donor preferences. Consequently, overall performance suffers when an IO cannot effectively set its agenda, prioritize programs, or maintain adequate staffing due to insufficient or inflexible funding.
Theoretical refinements
Existing literature has established that donor states use funding as a substitute control mechanism when they cannot exert disproportionate influence via voting (Graham and Serdaru, 2020). However, research has largely focused on state actors and assumed a generally negative impact of earmarking on IO autonomy and performance (Reinsberg, 2023). Our framework systematically incorporates the growing influence of non-state actors, such as philanthropic foundations, and highlights under what conditions earmarking may align with IO priorities to enhance autonomy and performance. In many multilateral organizations, control is generally exercised collectively through governing bodies requiring the IO’s administration to regularly report on its activities. We look at a specific control mechanism donors use to shape IOs’ activities and priorities, namely funding practices. Financial contributions serve as a substitute control mechanism in the absence of weighted voting or formal voting rights. Importantly, we extend this “logic of substitution” beyond traditional state-based frameworks to encompass both non-member states and non-state actors in various historical periods even beyond the lifetime of the UN. While traditionally excluded from de jure decision-making circles, these actors may wield significant de facto influence through their financial contributions. Hence, we argue that funding practices offer a conduit for major donors—state or non-state—to exert influence, circumventing conventional pathways of control. 6
Furthermore, we enrich recent literature that largely critiques earmarking as detrimental to performance by offering a more nuanced explanation of when earmarking impairs institutional performance. While some transaction costs—such as reporting burdens or limited donor coordination—are inherent to earmarking, we argue that its impact is not uniformly negative but context-dependent. More specifically, we contend that earmarking impairs performance when it is deliberately used as a control tool, as described in the causal process above. However, earmarked funding can also arise from a key stakeholder’s established practices. In this case, earmarking can actually enhance an IO’s performance because it increases its autonomy through the availability of more financial resources. Complementing Graham’s (2023) argument, which suggests that some well-intentioned donors unwittingly set the stage for others to exploit earmarking later, we suggest that earmarking can also stem from a key stakeholder’s very own established funding practices. Over time, these initial design choices may, however, inadvertently facilitate the exercise of control via earmarking by this stakeholder. Besides these theoretical refinements, we also go beyond the typically quantitative literature on earmarking by covering additional financial instruments, such as withdrawals, payment delays, or threats thereof. While reducing an IO’s financial resources has long been recognized as a control mechanism (Hawkins et al., 2006), we show how other funding modalities—such as delaying payments—also enable donors to exert control.
At its core, our theory synthesizes and refines recent scholarly insights from multiple strands of research into a coherent causal process. In most, especially contemporary cases, earmarking is a consequence of preference heterogeneity among key stakeholders. However, the importance of this precise cause for the consequences of earmarked funding has rarely been made explicit in extant scholarship. In addition, we emphasize the importance of deliberate practices by individual actors. What is decisive is not the mere existence of, for example, a certain financial arrangement, such as earmarking, but the active use of this tool as a control mechanism. Accordingly, context is crucial for understanding the effects of earmarked funding. Our theory thus closes gaps in the understanding of earmarking in particular and funding practices more generally, adds a new perspective on the relationship between preference heterogeneity among stakeholders and IO autonomy, and synthesizes different scholarly advances around the funding, autonomy, and performance of IOs.
Sequential steps
Having introduced the key concepts and theoretical refinements for our framework, we briefly outline the main sequential steps connecting donors’ preferences, funding practices, and effects on IOs’ autonomy and performance. First, we propose that greater preference heterogeneity among stakeholders increases the likelihood of donors exerting control through financial contributions. Second, this increased control via funding, exercised individually, is expected to reduce the IO’s autonomy. Finally, reduced autonomy is anticipated to diminish organizational performance, as the IO becomes less capable of achieving its set goals. The sequential steps are as follows:
S1. Higher preference heterogeneity among key stakeholders involved with the IO leads donors to exert more individual control via funding
S2. Increased use of funding as an individual control mechanism reduces the autonomy of the IO
S3. Decreased autonomy results in diminished IO performance
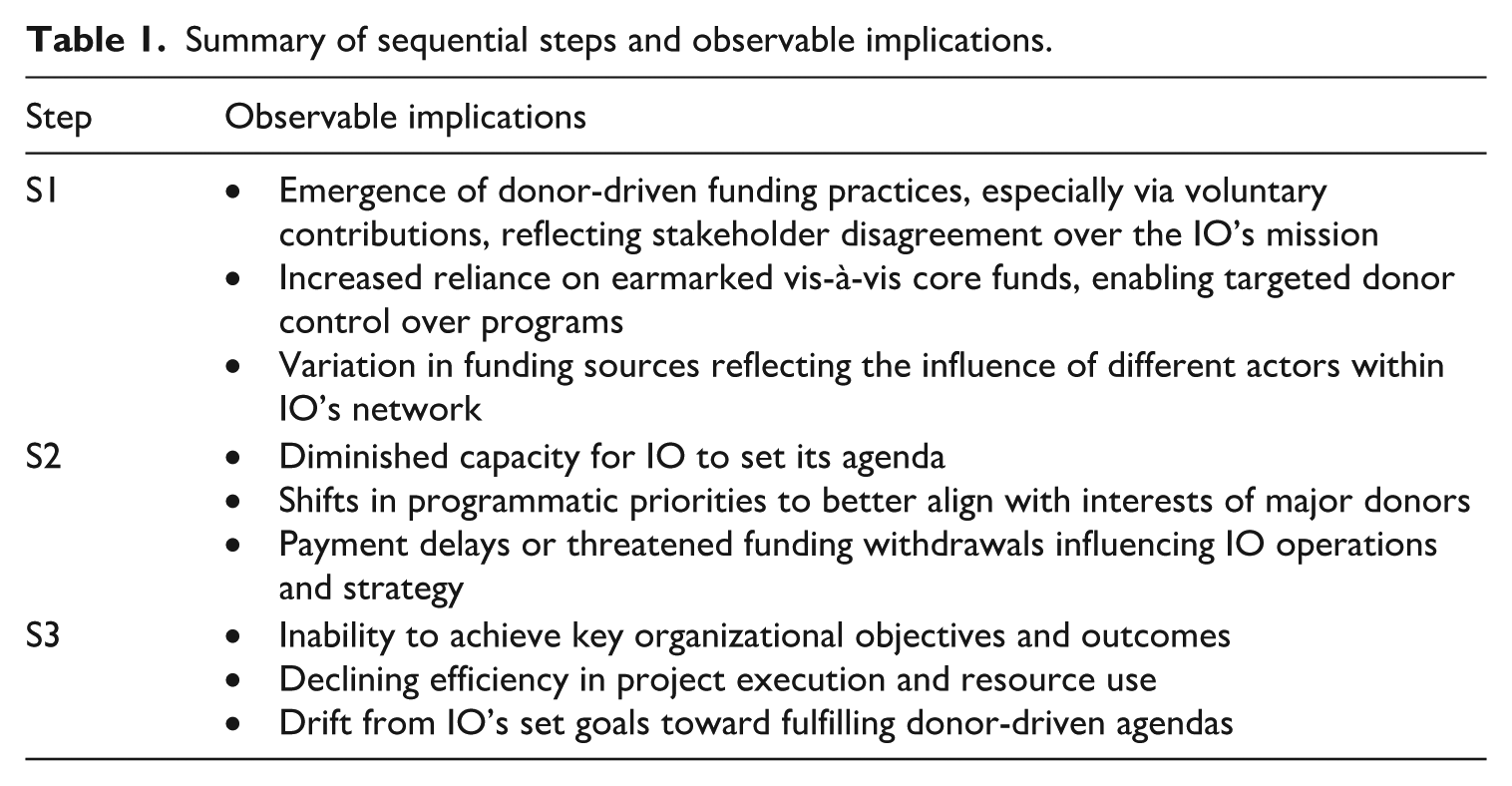
Table 1 summarizes the observable implications of the theorized sequential steps.
Summary of sequential steps and observable implications.
Research design
To illustrate our theorized process, we examine the role of state and non-state actors’ funding practices in the evolution of global health governance over the past century. We use within-case analysis to both illustrate our expectations and demonstrate the empirical relevance of our theoretical propositions (Eckstein, 1975). Specifically, we present three different empirical illustrations drawn from the historical trajectories of two major international health organizations, the League of Nations Health Organisation and the World Health Organization. While these organizations present some differences (most relevantly, LNHO typically relied more on non-state funding than WHO), they can collectively be considered a least-likely case for evaluating the impact of earmarked funding on IOs (Gerring, 2007). Whereas some interwar and postwar institutions—such as UNICEF—could only rely on voluntary contributions, both LNHO and WHO had rules ensuring members had to pay assessed contributions to support their activities and operational expenses. Therefore, one might anticipate the influence and relevance of earmarked resources to be relatively limited for these two organizations. Because historical data demonstrate otherwise, the support we find for our theoretical expectations can provide substantial leverage (Levy, 2008).
By exploring the role of money in shaping global health governance, this article addresses a case characterized by significant internal variation. This stems from the long (and heterogenous) historical periods analyzed and the fact that LNHO and WHO, for all the continuities and parallels between them, are two significantly different organizations regarding, for example, their membership. This internal and external variation enhances the overall generalizability of the article’s empirical and theoretical findings. By examining the case of international health governance, we thus aim to undergird a more general sequential process elucidating the role of funding for IOs’ autonomy and performance.
We draw on ample qualitative evidence, specifically documents publicly available in WHO’s online repository of the World Health Assembly and Executive Board meetings. These include statements by member states, WHO’s directors-general, and other policy officers, and external assessments by diverse entities, from the UN Joint Inspection Unit (JIU) to private consultancies and review panels. Regarding WHO’s funding and budget, sources include statistics by the UN System Chief Executives Board for Coordination. For LNHO, we rely on archival materials from the League of Nations (LoN) Archives Database and the Online Collection and Catalog of the Rockefeller Archive Center, including official meeting minutes for various committees, dossiers on specific projects and partnerships, reports, financial statements and private correspondence and diaries of relevant personnel that have since been made publicly available. Finally, we draw on global health research which has examined the evolution of global health governance over the past century (Chorev, 2012; Cueto et al., 2019; Gatti, 2025; Lee, 2009) and the role of financing and budgeting practices (Eckl, 2024; Patz and Goetz, 2019; Reddy et al., 2018).
Empirical analysis
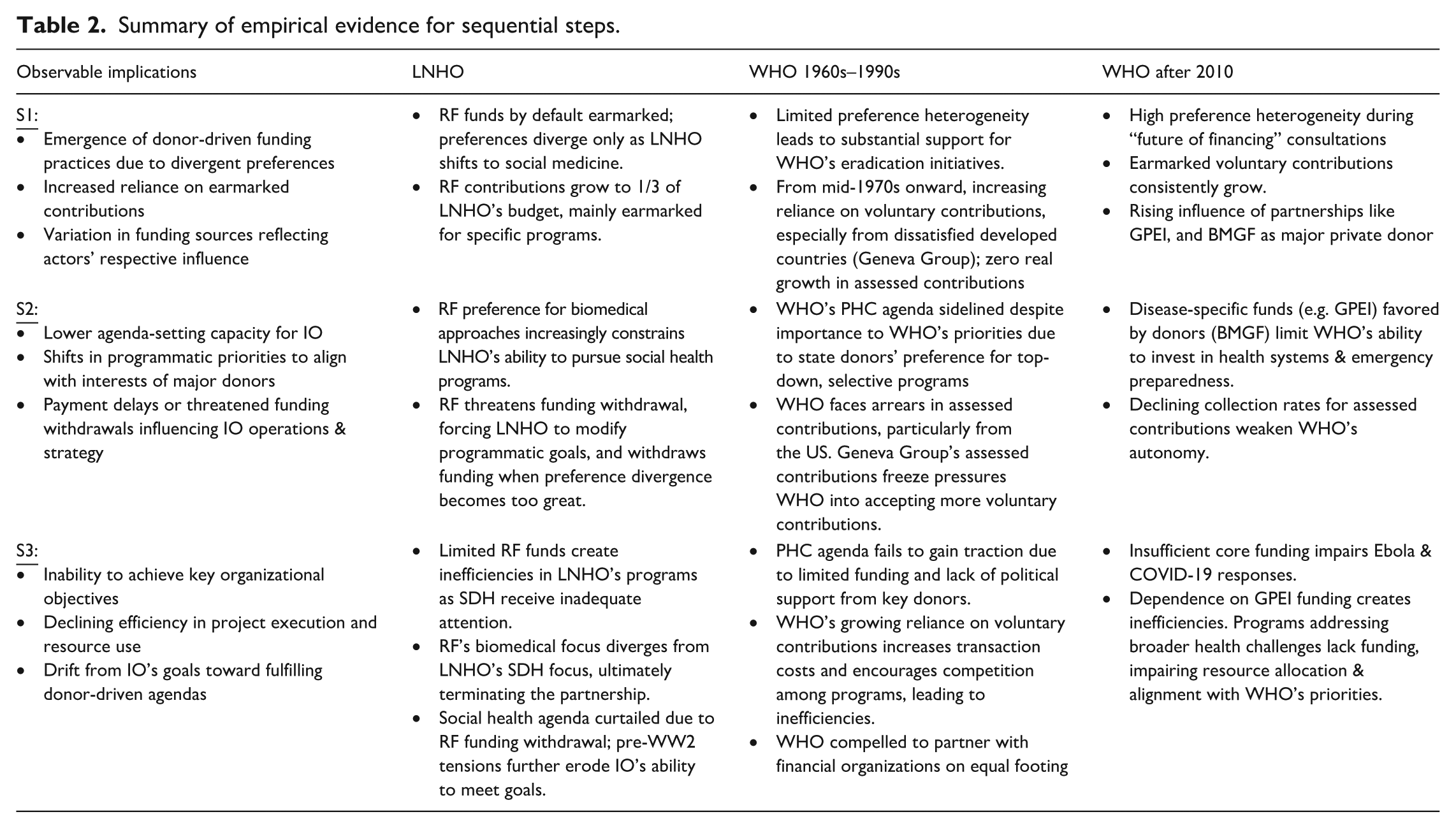
We examine three distinct periods in the history of international health institutions over the past century (Table 2). The first covers the League of Nations Health Organisation and its relationship with state and non-state donors, especially the Rockefeller Foundation (RF), in its efforts to shape the emerging international health discourse and practice. The second period concerns LNHO’s successor, the World Health Organization, in the 1960s to 1990s to highlight how wealthy states markedly influenced the organization’s agenda and activities through financial mechanisms. The final period is WHO after 2010, examining the impact of financial challenges and diverging preferences among state and non-state actors, such as the Bill and Melinda Gates Foundation (BMGF), on WHO’s autonomy and performance.
Summary of empirical evidence for sequential steps.
League of Nations Health Organisation
LNHO is WHO’s direct predecessor, lending personnel, procedures, and lessons learned to the latter. Despite variation in membership, voting, and funding structures, empirics highlight significant continuity in our theoretical expectations, including the use of funding practices to influence international health and institutional agendas. Over its two decades, earmarked funding practices were significant for LNHO’s initial relative success and the increasing tension between stakeholders in its later programmatic evolution and performance. Throughout, earmarking, contrary to existing narratives, did not axiomatically lead to bad performance. Rather, preference heterogeneity between stakeholders did.
At LNHO, financial control mechanisms were largely used by non-state actors due to the institution’s decision-making structure. Established by the LoN in 1921, LNHO was led by a small, technocratically composed internal body, the Health Committee (HC). Its experts did not represent stakeholder states equally. In the initial HC, for example, not all states involved in LNHO activities were represented. Even then, only four of the fifteen nationalities present were non-European, including India, a then-colony of Britain (Borowy, 2009). Moreover, countries with national members “in the room” did not necessarily have a direct vote in the proceedings. Members were—at least ostensibly—on the Committee for their qualifications, not to forward national interests (LoN, 1923). Thus, HC members were supposed to act as public health experts rather than government representatives (LoN, 1922: 114). With these uneven and diluting effects, voting influence for states was egalitarian in neither quantity nor quality.
Without a one-state-one-vote system, agenda-setting power was disproportionately concentrated by European states. These stakeholders could forward their preferences more successfully through traditional avenues of HC voting structures. Consequently, Western countries had limited incentives to control IO agenda-setting through bilateral financial mechanisms. In addition, states with less direct representation within the HC—and, by extension, less agenda-setting power—did not have the wealth necessary to successfully wield finances as a control mechanism. In other words, while there was preference heterogeneity among state-based stakeholders, states with the power to wield financial control mechanisms had little need and those who might wish to do so had little capacity. While not the only cause, this is certainly a factor in the persistent financial difficulties that plagued LNHO. Luckily, another potential stakeholder, the Rockefeller Foundation, was willing to help alleviate these pressures.
The RF was the most important non-state actor in LNHO and international health generally in the early 20th century. Health was a strategic investment for John D. Rockefeller for several reasons, all informing the RF’s programmatic preferences. A major factor was its convenient reportability. Health projects could focus on specific, quantifiable issues, using specific, quantifiable tools, to present specific, quantifiable outcomes. This was necessary for the RF’s “philanthrocapitalism,” as it had to demonstrate tangible results to its board of trustees and improve the oil baron’s struggling public image (Birn, 2014; Farley, 2003). In addition, improved health could provide RF endeavors with greater geoeconomic security, increased productivity, and a stronger international foothold (Birn, 2014).
These considerations, paired with increasing biomedical advances, informed the RF’s preferred concept of health. When the RF created its International Health Division (IHD) (also known as the International Health Board) in 1913, it clearly preferred a “vertical” approach to health, categorized by top-down agenda-setting, specific parameters for success, and narrow interventions on causal factors of disease (Birn et al., 2018). LNHO initially shared this preference, making for a natural partnership. In 1921, Ludwik Rajchman, LNHO’s Medical Director, was approached by IHD Director Wickliffe Rose. A year later, after extensive conversation, the RF announced its readiness to collaborate in the new international health project (LoN, 1922).
From the beginning, RF funds were earmarked for predetermined programs—initially epidemiological surveillance and expert interchanges (LoN, 1922). The specificities of these earmarked funds were stressed throughout the grant process. Interestingly, the RF strongly emphasized it was not attempting to influence LNHO through these mechanisms, often in the same breath as giving specific instructions on how these critical funds must be used. In his private diary, Rose outlines a conversation with the US Surgeon General Hugh Cumming regarding such practices: . . . The International Health Board has committed itself in definite sums in support of the International Epidemiological Service which the League is proposing to conduct and also in support of the scheme for International Interchange of Sanitary Personnel; it was further explained that the Board is not undertaking to determine the policy for the Committee or to interfere in any way in its procedures . . . it was also explained that the Board is not interested to see the Committee undertake too rapid progress in either of these two projects; it is understood that sound policy will probably require beginning on a very small scale and gradually developing the undertaking as its soundness and usefulness are demonstrated. —Wickliffe Rose Diary Entry, October 6, 1922 (Rose, 1922)
This initial arrangement proved useful to both stakeholders, and the RF soon increased its funding. In 1924, due to increasing LNHO financial difficulties, the RF raised its donations from US$60,000 to US$100,000 (IHB Minutes 20 May and 24 July 1924, as cited in Borowy, 2009). Over time, its contributions rose to a third of LNHO’s budget (Figure 2). 7 This funding included health personnel exchange schemes, epidemiological reports, and other RF-selected projects. By 1933, 15 of the 42 technical posts at LNHO were directly RF-funded (Weindling, 1997: 278).
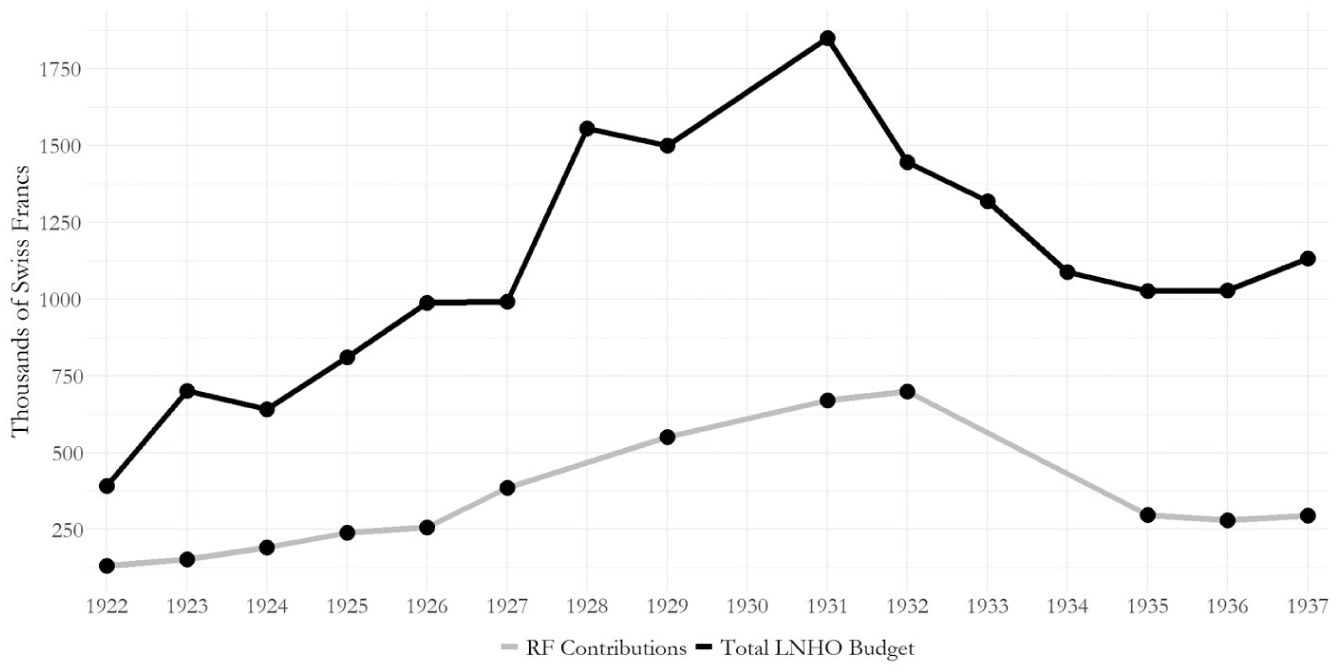
Total LNHO budget and RF contributions from 1922 to 1937.
Throughout, the RF earmarked all funds for its preferred activities and maintained a temporary basis for funding to maintain financial—and, by extension, programmatic—control (Weindling, 1997). LNHO HC personnel were aware of this influence. British HC member George Buchanan voiced his prescient concerns to Rajchman early-on, proposing LNHO take measures to protect their autonomy. “We should endeavour,” he wrote, “to apply these [RF] funds to services which are essentially auxiliary. . . . Unless this distinction is made, we may reach a dangerous position, in which the League might make the fulfilment of its health obligations always dependent on outside money being obtained” (LoN, 1922: 44). While Rajchman may have pondered this advice, it was not acted upon. The RF funding was readily accepted and put toward the RF-specified programs that would become central to LNHO’s functions.
This cash inflow further bolstered LNHO activities where other LoN bodies struggled to acquire sufficient funds from member states, causing many to consider LNHO a rare example of the League’s success (Dubin, 1995). The presence of financial control mechanisms did not, therefore, automatically impair organizational performance, partially because early preferences between the RF and LNHO were homogeneous. Both favored a narrow, vertical approach to health programming. As such, even though LNHO’s agenda-setting capacity was limited to RF-backed projects, performance did not decrease because these projects aligned with LNHO’s own agenda preferences. Performance began to suffer only when these preferences began to diverge. Under Rajchman, LNHO began to use its momentum in the early 1930s to expand into broader, social issues like poverty and living conditions. The RF, however, maintained its preference for biomedical approaches. Despite its financial dependence, preference heterogeneity between LNHO and its main donor rose as it gained greater momentum, leading the RF to pursue greater oversight.
As a non-state stakeholder, the RF had no direct voting power over LNHO’s agenda. However, earmarking practices already in place now became an alternative route for the RF to forward its increasingly divergent preferences (S1). While initial designs for its financial mechanisms had been administrative in nature (the RF maintained earmarking practices across its charitable partnerships), existing earmarking practices allowed the RF to influence LNHO’s actions with greater intentionality (S2). While LNHO could technically undertake programs without RF funding, it would have to do so with very limited state-based funds and often without the expertise also provided by the RF. RF-backed programs were therefore much more likely to succeed and be pursued. The RF was thus able to persistently forward its preferences for a biomedical approach over LNHO’s increasingly antagonistic preference for a more social medical approach even as it continued to lack formal voting power (S2).
The RF faced increasing hesitations about its partnership with LNHO as Rajchman continued to pursue broad, social-oriented programs, including nutrition, labor, and housing conditions, despite the RF’s attempts to check its autonomy via financial control mechanisms (Borowy, 2009). Consequently, the RF further curtailed autonomy and hindered LNHO’s efforts to achieve its changing performance goals (S3). New RF presidents who were less supportive than Rose were more intentional about curtailing LNHO autonomy in favor of RF principles, and earmarking—an initially administrative function—was increasingly employed to influence IO autonomy (Farley, 2003). Complications were already showing by 1931, when the RF signaled its displeasure by announcing plans to end all grants to LNHO (S2). Rajchman and his colleagues were able to successfully convince them otherwise on this occasion. However, this did result in reforms to institutional activities. Moving forward, the RF would explicitly fund only research issues (Weindling, 1997: 279). While the RF did favor temporary funding as an organizational strategy, the abrupt nature of this decision and the further narrowing and specification of funds suggests increasingly divergent preferences, not institutional procedure, to be the main driving force behind the RF’s growing apprehension toward LNHO.
By 1934, diverging stakeholder preferences for biomedical versus social medicine had taken their toll. The RF decided its partnership with LNHO was no longer sustainable and announced a timeline for funding termination (Tournès and Gharibian, 2022; Weindling, 1997). Ironically, this termination agreement included US$400,000 free of any of the designations otherwise typical of the RF’s contributions (Weindling, 1997: 279). Consequently, Rajchman could fund many programs the RF had previously avoided funding. Yet this departing gift would not be the lifeline LNHO may have hoped for. Increasing pre-war geopolitical tensions and the rise of League director Joseph Avenol, an antagonist to Rajchman and his social medical approach, presented external problems for the IO (Balińska, 1998; Borowy, 2009). Rajchman was fired, LNHO came under more direct League supervision, and projects began to fizzle with decreased funds, participation, and willpower in the face of oncoming war (S3).
LNHO maintained certain functions during World War II, but was subsequently dissolved to make way for its direct successor, WHO. The RF persisted in its original form for several years, but by 1951, the IHD was gone, too (Farley, 2003). Yet, the ideological dialogue between LNHO and RF continues within the “pendulum” swings between biomedical and social health (Farley, 2003; Packard, 2016).
WHO in the afterwar decades (1960s–1990s)
After LNHO’s dissolution, money remained crucial in shaping the institutional development of its successor, the World Health Organization. This sub-section examines the decades from the 1960s to the 1990s, when earmarked funding gradually became a mechanism of control especially by developed countries. By leveraging their financial contributions, these countries were able to influence WHO’s strategies and policy agendas, aligning them more closely with their own preferences and programmatic priorities, with far-reaching consequences for WHO’s autonomy and performance. 8
Approved in 1948, WHO’s initial budget of around US$5 million consisted mainly of member states’ assessed contributions based on economic and demographic factors. Intuitively, this made the agency highly dependent on a few countries, chiefly the US. While WHO had been set up to be the “directing and coordinating authority” on all matters relating to international health work (WHO, 1948), such in-built financial insecurity forced it to scale down its activities. By the early 1950s, WHO’s operating program budget stagnated due to states’ withdrawals 9 and arrears in the payment of assessed contributions (WHO, 1951). Things started to improve a decade later, when WHO’s growing membership entailed a substantial funding increase. WHO’s working budget quadrupled, from US$14 million in 1957 to US$56 million in 1967 (WHO, 1961, 1967). Importantly, WHO promoted innovation in the practices concerning voluntary funding from governments, companies, and privates. Reinterpreting the provisions in Article LVII of its Constitution (WHO, 1948), the agency created a Voluntary Fund for Health Promotion (WHO, 1960). The Fund consolidated all existing special accounts already established for voluntary contributions (Clift, 2013). These resources were earmarked for specific purposes, intended to expand the overall scope of WHO’s activities and services. By attracting contributions from privates, organizations, and member countries, the Voluntary Fund allowed to coordinate external support to WHO more effectively. The net results were encouraging, as by 1967, almost US $30 million had been pledged through the Fund (WHO, 1968). This influx of earmarked funding was particularly vital in supporting WHO’s early eradication efforts against malaria and smallpox. In fact, these campaigns aligned closely with the priorities of actors already engaged in regional health initiatives—such as the RF and UNICEF—and powerful governments, chiefly the US and the Soviet Union, which viewed eradication programs as strategic tools to assert their influence over global health policy (Brown and Cueto, 2010). Thanks to this relative convergence of preferences between WHO leadership and major donors, the agency could leverage external earmarked resources to pursue its goals with some autonomy. For example, in 1965, WHO secured a significant budget increase including a US$2.4 million contribution, fully earmarked for smallpox eradication through the establishment of a Special Account for Smallpox Eradication.
In the early 1970s, however, the end of dollar convertibility to gold entailed a significant appreciation of the Swiss franc, in turn increasing the resources required to cover WHO’s expenditures. Within the IO, preferences diverged on how to respond. Low-income countries expected industrialized nations to bear the additional costs, while the latter pressed for WHO to cut expenditures. Caught between these conflicting expectations, WHO sought to improve its standing with member states. Consequently, the agency began shifting from a traditional input-oriented, accountancy-based budget to a new results- or output-oriented program budget. This reform aimed to enhance WHO’s capacity for self-evaluation, accountability, and transparency in spending decisions—ideally encouraging member states to increase their assessed contributions (WHO, 1977). Despite these moves, WHO’s financial distress left it increasingly vulnerable to member states’ efforts to expand individual control. This became evident with the significant increase of extrabudgetary funds (EBFs) provided by donors outside WHO’s regular budget. While these accounted for 20 percent of total funds in 1965, their share had grown to 26 percent in 1973, with the trend showing no sign of slowing (S1). Initially, WHO considered EBFs—largely earmarked for specific programs aligned with donor priorities—essential to fulfilling its mandate given stagnating regular budgets (WHO, 1975). In fact, a 1975 internal study concluded that “the constructive influence of extrabudgetary resources [was] potentially greater than the risks” (WHO, 1975).
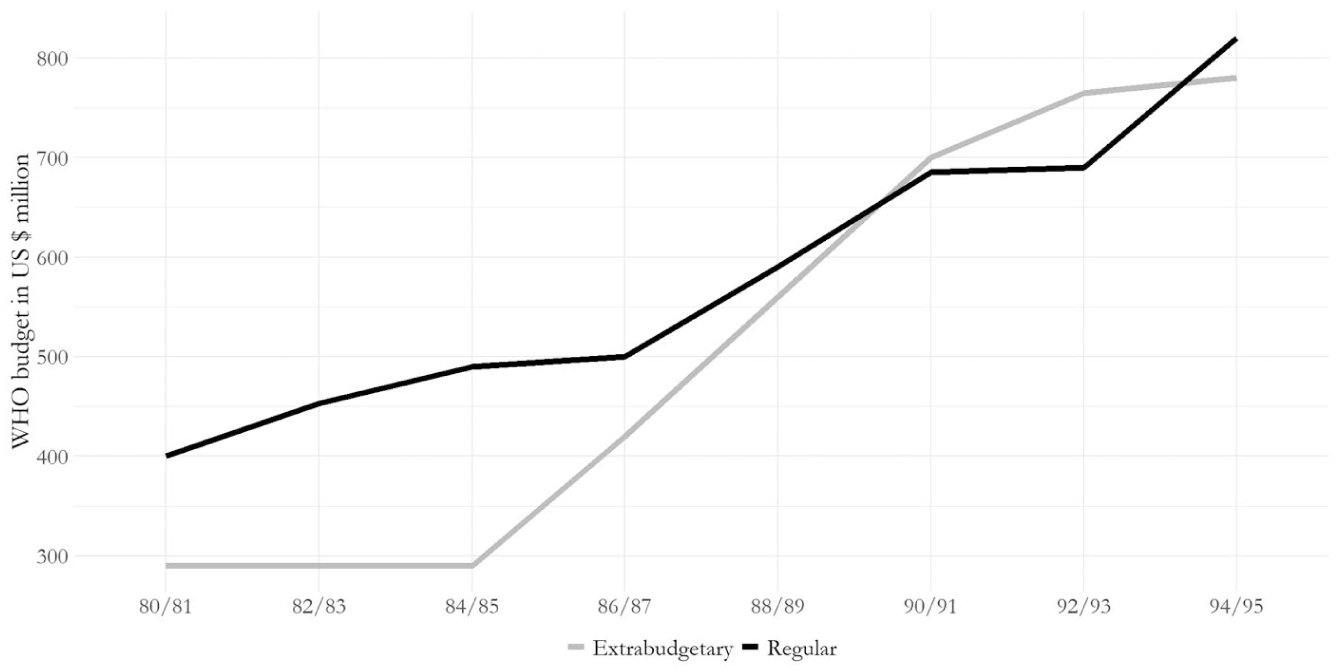
However, WHO’s financial situation continued to deteriorate subsequently. Arrears in assessed contributions reached new highs, with the collection rate dropping to 72 percent in 1986, the lowest since 1950 (WHO, 2011). This erosion of budgetary support was further compounded by a significant shift in the US government’s stance toward international agencies. Under the Reagan Administration, the US became the primary driver behind the consolidation of the Geneva Group, an informal coalition of the UN’s largest contributors, mostly developed countries. Originally established to improve governance and management across the UN system, the Geneva Group began, following conservative electoral victories in the US, the UK, and West Germany, to advocate for limiting increases in assessed contributions to specialized agencies. In the early 1980s, the Group’s efforts led to a new policy—applied across all UN organizations—mandating zero real growth in assessed contributions (Chorev, 2012). Additional withholdings to the UN budget materialized in 1985–86, when the Reagan Administration approved two further pieces of legislation to link payments of contributions with progress toward weighted voting on budgetary issues in the General Assembly. The implications for WHO were significative. In proposing the program budget for 1988–89, director-general Mahler highlighted the growing challenges the organization faced in fulfilling its mandate amid declining resources. While assessed contributions remained constant—and were sometimes even withheld or delayed—WHO was nonetheless “expected to provide the same level of program activities as before, [living] with the pretense that nothing had changed, whereas in actual fact a great deal had changed.” (WHO, 1987)
Opposing requests from the WHO’s Secretariat and developing countries to increase assessed contributions, industrial countries instead opted to tighten their individual control over the agency (S1). Accordingly, EBFs took on unprecedented importance, growing from a quarter of WHO’s total budget to nearly matching regular funds in 1986–87 (Figure 3). Four years later, EBFs exceeded the regular budget (Vaughan et al., 1996). This shift marked a significant departure from WHO’s original funding rules and practices. Unlike the regular budget—closely supervised by the director-general and the World Health Assembly—accountability for EBFs was minimal and poorly systematized. For example, donors were “free to designate their EBFs to different programmes without even consulting the central WHO management” (Vaughan et al., 1996), resulting in most resources being earmarked for centrally managed programs in disease control and human reproduction. Consequently, reliance on EBFs became the preferred strategy for those donors—mostly developed countries—seeking greater influence over WHO’s priorities and strategies (Chorev, 2012).
The prominence of closely earmarked funds significantly impacted WHO’s strategies and ability to set priorities autonomously (S2). This influence was evident in the failure of the agency’s flagship initiative during the 1970s and 1980s, its Primary Health Care (PHC) agenda. Starting in the mid-1970s, WHO recognized the necessity to integrate its health promotion activities with the development of national basic health services. A 1973 report by the Executive Board (WHO, 1973) pointed out that health service delivery worldwide was largely based on transferring health technologies from developed to developing regions and from urban to rural areas (WHO, 1974). While this approach helped address specific diseases, like smallpox, it failed to tackle the non-medical factors significantly influencing health outcomes. These social, economic, and environmental factors called for a comprehensive, whole-of-society approach to address the interconnected aspects of physical, mental, and social health and wellbeing. This innovative approach, referred to as primary health care, emphasized involving local populations in designing healthcare activities and integrating health services with broader developmental efforts in areas like agriculture, education, and housing. From the outset, WHO underscored that a substantial financial commitment to developing basic health services and strengthening health systems was essential to the success of PHC.
Despite WHO’s expectations, these priorities failed to gain donors’ attention. WHO’s Executive Board warned already in 1981 that “the increased reliance on extrabudgetary funding, and the creation of new management structures and financing arrangements for special programmes [. . .] [was resulting in a] departure from the policies, strategies and directions laid down by the regional committees, the Executive Board, and the Health Assembly.” (WHO, 1981) These concerns proved well-founded. By the early 1980s, EBFs were increasingly earmarked to centrally managed, high-impact projects targeting narrowly defined priorities, as these programs provided donors with clear targets and discernible short-term outputs—an approach reminiscent of the Rockefeller Foundation’s strategy in the 1920s. Such bias in favor of high-profile, disease-specific initiatives “tended to undermine the broader and more integrated policies of primary health care.” (Vaughan et al., 1996: 258) Consequently, financial resources for core priorities identified by the PHC agenda—for example, epidemiological and health systems research—were denounced by WHO as “disquietingly low” (WHO, 1983). Certainly, the decline of PHC had several causes, including growing ideological opposition to PHC’s egalitarian, community-led approach, the economic consequences of the 1980s debt crisis, and, sometimes, limited political commitment within developing countries themselves. Nonetheless, major donors—from wealthy states to influential multilateral and private actors like the World Bank and the RF—were undoubtedly critical in diverting resources away from PHC toward narrower, more measurable interventions. This shift was famously institutionalized already in 1979, when representatives from the US government, the World Bank, and key private foundations met in Bellagio to promote Selective PHC, a streamlined package of high-impact interventions presented as a more feasible alternative to PCH’s multi-sectoral and politically empowering vision.
By the early 1990s, the outlook for WHO became bleaker, as a new rule of zero nominal growth for assessed contributions shrank the agency’s effective budget. The stagnation in budgetary growth forced WHO to choose its priorities and programs selectively, while relying increasingly on extrabudgetary, earmarked contributions. WHO’s dependence on non-regular funding sources had many dramatic repercussions at both organizational and systemic levels. First, it contributed to transferring “the effective power of decision-making to the donors themselves” (WHO, 1997: 253). Second, WHO’s program managers developed a general interest in raising additional extrabudgetary resources for their programs to extend their own influence within WHO (Chorev, 2012). This contributed to higher in-house competition for money, fueling corruption and cronyism. Finally, WHO’s overreliance on earmarked funding forced it to promote new working arrangements with external organizations (Lidén, 2014). Unlike the past, these were not typical humanitarian agencies close to WHO. On the contrary, WHO was compelled to increasingly collaborate with financial organizations such as the World Bank, the International Monetary Fund, and regional development banks. In such collaborations, WHO was typically just one partner among many. Perhaps more importantly, the fact that WHO had to rely on external organizations for financial aid and occasional technical support implied its shrinking ability to autonomously shape the global health agenda (S3).
By the late 1990s, WHO was caught between crossfires. While its stated goal of integrated PHC appealed to low-income countries, which expected more help and support than were feasible given WHO’s precarious financial condition, WHO’s reliance on closely earmarked resources made it prone to high-profile programs that most often failed to address the broader social determinants of health (SDH). In this context, wealthy countries—particularly the US—doubled down their criticism of the agency, lamenting WHO’s inability to adapt to the neoliberal imperatives of cost-effectiveness and prioritization. By 1995, the rate of collection of assessed contributions, at 56 percent, was the lowest ever in WHO’s history, with unpaid contributions reaching a record US$243 million 12 (WHO, 1996). In a glaring illustration of WHO’s financial distress, the then director-general Hiroshi Nakajima had to borrow a large amount of cash from the agency’s reserve funds, further undermining its ability to respond to sudden challenges (Godlee, 1996).
WHO after 2010
The past two decades have seen significant shifts in WHO’s finances at both the micro and macro levels amid high preference heterogeneity. These shifts concern not only the amount but also the quality and sources of funds, in turn drastically impacting WHO’s autonomy and—particularly in major emergencies such as Ebola and COVID-19—performance. Overall, assessed contributions constituted only a small fraction of WHO’s funding (Figure 4). Notable is the fluctuation of voluntary earmarked contributions, demonstrating the growing reliance on earmarked funding as a control mechanism by donors. Voluntary core—that is, unearmarked—contributions are rather insignificant for WHO, while voluntary non-core—that is, earmarked—contributions vary significantly and overall increased substantially.
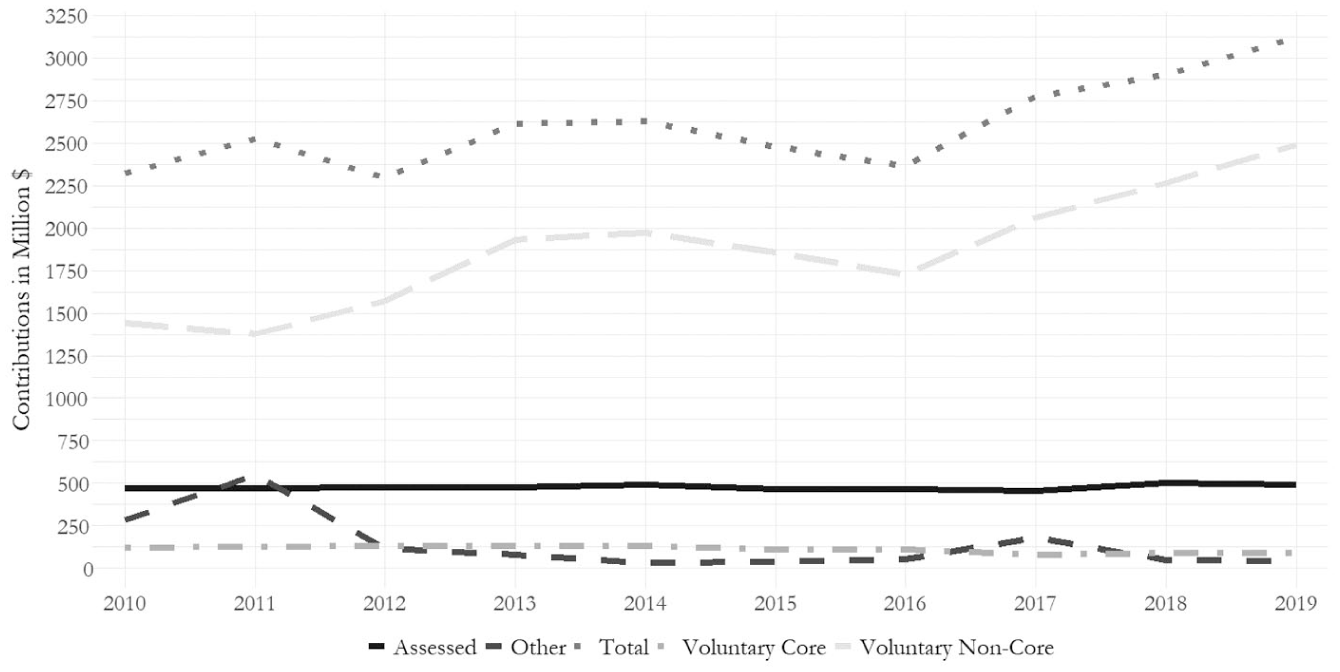
WHO funding by type.
The global financial crisis exacerbated WHO’s dependency on external donors’ support. While its overall working budget remained stable, the portion not financed through net assessments on member states reached 79 percent in the 2010–11 biennium (WHO, 2009). Consequently, areas not considered priorities by donors—such as emergency preparedness—suffered from significant budget cuts. Subsequent discussions concentrated on two issues: how to align WHO-set priorities with the actual monies available and ensure greater predictability and stability of financing (WHO, 2010a). What started as a debate about money evolved into profound discussions about WHO’s priorities, specifically whether WHO’s mandate should extend beyond technical-advisory functions to include operational, for example, humanitarian, work (WHO, 2010a). In this “future of financing” consultation in 2010, preference heterogeneity was high. Many member states primarily called on the WHO Secretariat to further reduce administrative costs and narrow the organization’s spectrum of activities (UNJIU, 2012: iii). For additional funding, WHO would first have to demonstrate its “value for money” (WHO, 2010a: 12). Simultaneously, other states wished to expand WHO’s mandate and funding (WHO, 2010b: 3). Preference heterogeneity among member states was explicitly noted as a problem in the consultation (WHO, 2010b: 2) (S1).
Instead of alleviating the funding problems, the consultation hence led to more fundamental reform efforts. Seeing that few of WHO’s largest contributors were willing to change their funding practices, director-general Chan reoriented her efforts to find new funding sources and mechanisms. Strengthening collective control remained a major issue and was further addressed in funding discussions in 2015 (WHO, 2015). Nonetheless, these improvements, for example, concerning transparency, did not satisfy member states. Whereas the collection rate of assessed contributions—considered a measure of member states’ satisfaction—stood at almost 100 percent in 2008–09 (Clinton and Sridhar, 2017: 92), it fell subsequently (Figure 5). Likewise, voluntary core contributions were not a substantial factor (Figure 4). This suggests that more collective control does not increase donors’ satisfaction in a situation of high preference heterogeneity, fostering the substitution of individual control via funding. Figure 5 is even more remarkable considering that total voluntary contributions from member states increased over the same period. Having become only more visible since the “future of financing” consultation, high preference heterogeneity made greater alignment difficult and even those member states generally preferring higher flexible funding reluctant to provide flexible contributions (WHO, 2010b: 5; 2017b: 11) (S1).
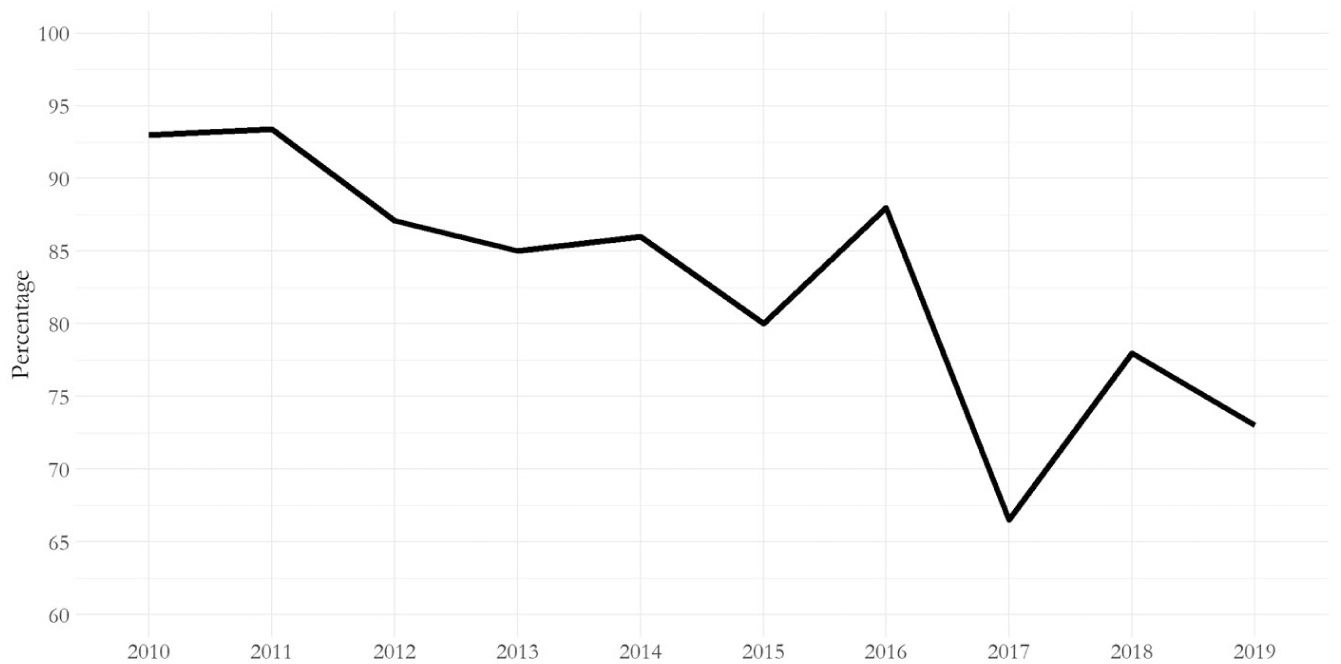
Assessed contributions collected by 31 December.
These financial difficulties severely undermined WHO’s autonomy and performance (S2, S3). WHO responded late and slowly to the 2014 Ebola outbreak in West Africa. A subsequent report by the Ebola Interim Assessment Panel (2015) found that the shrinkage of core contributions had eroded WHO’s capacity for emergency response. In the years before the outbreak, WHO had reduced its pandemic and emergency response team from 94 to 34 staff members due to its funding situation (Clinton and Sridhar, 2017: 93). Subsequent reform efforts requiring agreement among member states, such as more core funding, proved impracticable. Consequently, funding increases remained confined to specific programs—especially health emergencies. More than half of WHO’s total funding increase from 2016 to 2019 (see Figure 4) was for emergency-related funds (WHO, 2020a: 6).
One of these emergency funds, the Global Polio Eradication Initiative (GPEI) strikingly illustrates how such earmarked funding affects WHO. As a multistakeholder initiative driven significantly by private contributions, especially from the Bill and Melinda Gates Foundation, the GPEI highlights the influential role of global health partnerships in shaping WHO’s activities and the constraints on its autonomy due to the low predictability of the associated funding (S2, S3). While the approved budget for polio decreased in the late 2010s, funding remained—not least due to setbacks in eradication efforts—persistently high, at over US$1 billion per biennium, making polio one of the largest and one of few overfunded program components (WHO, 2020b: 69). Importantly, WHO’s polio program has not narrowly focused on vaccinations but strengthened entire health systems. WHO has used polio funding for core functions for which genuine core funding was lacking. The cynical implication is that ‘hanging over WHO is the impending eradication of polio. Nearly 20 percent of WHO staff (about 1,300) have been funded by this program, financed almost entirely by voluntary contributions [. . .]. The eradication of polio will leave a large hole in WHO’s budget and its capabilities’ (Clift and Røttingen, 2018: 1).
Dreading this possible funding drain, WHO argued for these capabilities to be sustained by gradually transferring the polio program into WHO’s base funding and core work (WHO, 2020b: 15–16, 71)—a program funded at only 82 percent even after being apportioned sizable flexible funds (WHO, 2020b: 19, 48). An arguably related move was admitting the BMGF into “official relations” with WHO in 2017 (WHO, 2017a). Because the BMGF’s contributions to WHO have mostly been earmarked for polio eradication, it seems plausible that this is part of the larger strategy for the GPEI to transition into WHO’s core work. By granting the BMGF “official relations” status, WHO might hope to ensure longer-term funding beyond polio eradication. Yet, this may come at a cost. For example, the BMGF entry in WHO’s non-state actor register for 2017–19 includes a section on “Leadership and governance,” which reads that the BMGF “anticipates providing further support to the overall reform efforts at WHO based upon the evidence acquired over the past three years. The foundation will again track the impact of these investments by improved effectiveness and efficiency of WHO” (WHO, 2017–2019). Whether or not the BMGF’s influence over WHO will increase, 13 the GPEI underlines how preference heterogeneity eventually leads to lower autonomy, as the IO needs to cater to specific, narrowly defined interests, and allocate its resources, including staff, accordingly (S1, S2). Overall, the result was a WHO performing well in smaller emergencies yet remaining insufficiently prepared for a large-scale one. This proved fatal once more in the COVID-19 pandemic when WHO was already lacking money for its emergency response in March 2020. The Independent Panel for Pandemic Preparedness and Response (2021: 30) found that the necessity for “perpetual fundraising efforts” impaired WHO’s performance during COVID-19 (S3).
Conclusion
The increase of earmarked funding in recent decades represents one of the most consequential trends to monitor when assessing the present and future viability of IOs. It significantly affects the functioning of the multilateral system, as earmarked resources can enable individual donors to independently contract out for specific areas of interest. This, in turn, may impair the performance and internal functioning of IOs (Reinsberg, 2023), while undermining the multilateral nature of global governance (Graham, 2023).
Starting from these premises, the article has made two main theoretical contributions. First, it has advanced a refined, more granular understanding of the motivations behind donors’ funding decisions. Expanding on arguments by Graham (2023) and Graham and Serdaru (2020), it has shown how preference heterogeneity among key stakeholders leads donors to use funding as a control mechanism in the absence of weighted voting systems or formal voting rights. Second, the article has provided new insights into how and when earmarked funding can compromise IOs’ autonomy and performance. Using an in-depth, longitudinal case study, it has illustrated how earmarked funding from external donors can skew IOs’ priorities (e.g. WHO’s role in polio eradication), disrupt predetermined agendas (e.g. WHO’s PHC agenda), and generally subject IOs to donor-driven biases. However, the article has shown how the impact of earmarking on IOs’ autonomy and performance depends on the context. When earmarking finances initiatives aligning with the IO’s predetermined priorities, it can indeed enhance organizational autonomy and effectiveness. Here, our primary analysis of LNHO data adds a crucial perspective on both the potential and pitfalls of donor-driven funding practices. While the RF’s priorities initially aligned with LNHO’s goals, enabling effective collaboration, the eventual divergence in preferences shows how earmarking, when actively used as a control mechanism, undermines IO autonomy and, consequently, performance. Highlighting these historical nuances enriches our theoretical understanding by demonstrating that the implications of earmarked funding, while consistent in their core mechanisms, vary significantly depending on the motives and preferences of stakeholders involved.
Our unique longitudinal case study has also provided important empirical insights into the phenomenon of earmarking. First, earmarked funding, while often linked to post-Cold War neoliberalism, was already central to organizations like LNHO a century ago. Second, the article has highlighted how even IOs like WHO, which, in principle, are resourced by assessed contributions, have long depended on voluntary, often earmarked funds. Arrears in assessed contributions and growing demands from stakeholders have forced these IOs to seek alternative, sometimes problematic funding sources. Finally, the article has foregrounded the influence of non-state actors as providers of earmarked resources. Specifically, it has emphasized the role of philanthropic foundations, analyzing the Rockefeller Foundation’s contributions to LNHO and the BMGF’s to WHO. It thereby adds to debates on the implications of private philanthropy for democratic transparency and accountability (Bishop and Green, 2015; McGoey, 2012, 2021).
Our contributions align with further research agendas in International Relations. Most prominently, the article complements recent literature examining the influence of earmarked funding in global governance. Empirically, it contributes to and differs from existing research by (a) focusing on global health, a relatively under-investigated field in International Relations, (b) adopting a long-term perspective extending beyond the usual post-1990s period, and (c) employing a rich small-N qualitative analysis rather than a large-N quantitative one. Finally, the article adds to institutional theory on the life and death of IOs, which has suggested specific reasons IOs either “die” or remain “alive and functioning” (Dijkstra and Debre, 2022; Eilstrup-Sangiovanni, 2020; Gray, 2018). As extant studies have often undertheorized the causal role of funding, a greater focus on money can offer new insights into the subtler determinants of IOs’ vitality. Hence, this article provides a valuable starting point for better understanding the influence of money on institutional development. The article clarifies the motivations behind IO funding practices; offers an in-depth, longitudinal analysis of IO funding, autonomy, and performance in global health; and emphasizes the lasting impact of non-state actors as sources of funding.
Our findings carry significant implications for contemporary global governance. As multilateral institutions increasingly depend on earmarked voluntary funds, understanding the roots of earmarking and its consequences for IO performance is crucial for designing more resilient governance structures. This seems even more relevant in global health after the Trump administration’s recent (renewed) decision to withdraw the US from WHO (Trump, 2025), likely triggering another massive WHO fundraising effort targeting governments and private donors. Policymakers face the challenge of crafting funding strategies that align divergent stakeholder priorities with organizational mandates, reducing the risks of donor-driven inefficiencies and ensuring IOs remain effective in addressing global challenges. This is particularly pertinent as IOs navigate complex crises, from pandemics to climate change, which demand both flexibility and coordinated, multilateral action. Its empirical and historical depth makes our study instructive for anyone interested in long-term understanding and improvement of the funding of multilateral institutions.
Footnotes
Acknowledgements
Previous versions of this article were presented at the 2023 OxPo Workshop on Multilateralism and Security at Nuffield College and at the International Studies Association 2024 Annual Convention. We are grateful to all participants for their comments. We are particularly indebted to Ranjit Lall, Dominic Pfister, Bernhard Reinsberg, Duncan Snidal, and Sarah Tanke. We also thank the anonymous reviewers and the journal’s editors for their thoughtful feedback and suggestions.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.