
Abstract
Background:
The relationship between attendance at specialized multiple sclerosis (MS) clinics and mortality has not been fully evaluated.
Objective:
We investigated the association between visits to specialized care in Danish MS clinics and mortality.
Methods:
We collected data from Danish national registers to assess survival among people with MS according to the number of visits in MS clinics. We employed the Kaplan–Meier method and extended Cox regression modelling.
Results:
In total, 9929 patients with MS were included in the study, contributing 105 115 person-years at risk. A total of 316 patients with MS died during a median follow-up of 10.3 years. Cumulative visits were not statistically associated with mortality (hazard ratio (HR), 95% confidence interval (CI) = 1.00, 0.99–1.02). Female sex (0.68, 0.53–0.87), being divorced (0.56, 0.37–0.86), being married or in a partnership (0.60, 0.45–0.79) and higher education (0.64, 0.45–0.91) were independently associated with reduced mortality. Expanded Disability Status Scale (EDSS) ⩾ 3 (2.38, 1.60–3.54), ischaemic cerebrovascular disease (1.97, 1.42–2.75) and pneumonia (7.03, 5.48–9.02) were associated with an increased mortality.
Conclusion:
We found no association between visits to specialized care and mortality. Our findings suggest that improving survival in patients with MS may require a focus on quality and content of care and proactive management of comorbidities.
Introduction
Multiple sclerosis (MS) itself is not inherently fatal; however, studies indicate a decreased life expectancy compared to the general population.1,2 People with MS have a higher likelihood of experiencing a decrease in overall survival and increased risks of death from conditions such as vascular diseases, respiratory infections, accidents and suicide.3–5 Several factors contribute to shorter survival in people with MS, including higher disability levels, the presence of comorbidities and health behaviours like smoking and low physical activity levels.5,6
Several studies7–10 from general or other chronic disease populations have observed elevated risk of mortality due to no or low utilization of healthcare and fragmentation of healthcare services. Previous studies have also linked infrequent utilization of healthcare services to poor control of chronic conditions such as diabetes mellitus 11 and hypertension. 12 People with MS often live with several conditions to manage,13,14 and the possible care fragmentation may result in higher rates of potentially inappropriate medication use and increased mortality in these patients.
Existing studies have compared mortality rates between people with MS and the general population, but the role of utilization of specialized MS clinics and mortality has not been fully evaluated. Exploring the potential association between visits to specialized care and mortality may offer insights into whether disparities in care access could be linked to differences in health outcomes. Thus, our objective was to investigate the possible relationship between the accumulated number of visits to specialized care in MS clinics and mortality risk in Danish people with MS. Our hypothesis posits that people with MS who have a lower number of clinical visits to specialized MS care are at an elevated risk of mortality in the Danish population. The cumulative number of visits is a proxy measure for the level of interactions with specialized care.
Materials and methods
Study design and population
We conducted a longitudinal register-based study on individuals with a confirmed diagnosis of MS in Denmark from 2000 to 2020 and identified participants through the Danish Multiple Sclerosis Registry (DMSR). 15
Exclusion and inclusion criteria
All individuals with a confirmed MS diagnosis between 2000 and 2020 were included. Individuals with no date of diagnosis, an age below 18 years at diagnosis, emigration after their diagnosis, no defined phenotype or a disease duration less than 2 years were excluded (Figure 1).
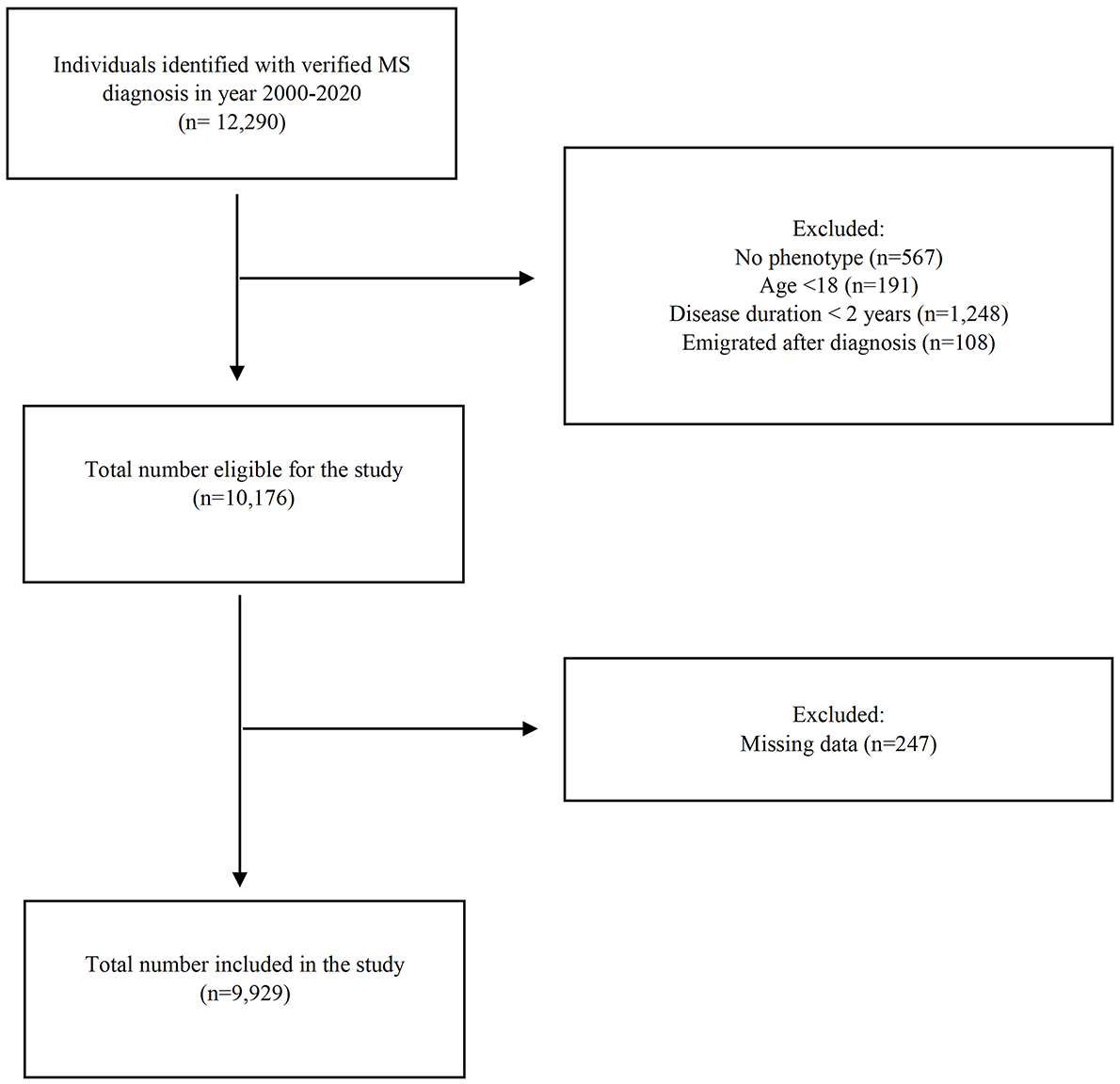
Flow chart of the selection of patients with MS for the study.
Outcome
The primary outcome of interest was all-cause mortality. Participants were followed longitudinally from the time of study entry (date of diagnosis) until date of death or end of follow-up (31 December 2020). The date of death was collected from the Danish Causes of Death Registry and right-censoring occurred when participants did not experience the event by the end of the follow-up.
Variables and data collection
Baseline characteristics recorded at the time of study entry included phenotype, Expanded Disability Status Scale (EDSS) score, sex, age in years, disease duration before study entry, marital status, employment status, area of residence and symptomatic treatment (Supplementary Table 1). Symptomatic treatment served as an indicator of whether symptomatic treatment was provided at baseline including medication for symptoms such as difficulty walking, pain, urinary disorders, spasticity, spasms, convulsions and fatigue (Supplementary Table 2). Further data collection was conducted at each visit on ischaemic heart diseases, ischaemic cerebrovascular diseases, phlebitis and thrombophlebitis, and pneumonia (Supplementary Table 1). Comorbidities have previously been associated with poorer health outcomes and were included in the analysis to account for their possible impact on mortality risk.
Information on sex, age, diagnosis, clinic use and EDSS score was obtained from DMSR. Data from DMSR were linked to data from Statistics Denmark (DST) 16 using the personal identity number to combine information on the study population. Information on time of death, symptomatic treatment and comorbidities was obtained from the Danish National Health Data Authority responsible for the national health registers 17 (Danish National Patient Registry, Causes of Death Registry and Registry of Pharmaceutical Sales). Information on marital status, education, employment and residence was obtained from Statistics Denmark (National Income Registry, Education registry and the Employment Classification Module). All data management and analysis were conducted on the DST server accessed through a virtual private network connection from Zealand University Hospital. 16
Statistical analyses
Data were assembled in STATA 18.0 for the analysis. We used descriptive statistics to portray the study population according to baseline characteristics and relapsing remitting MS and progressive phenotypes. The cumulative number of visits during follow-up was incorporated as time-varying exposure to avoid immortal time bias. The Kaplan–Meier survival curves were plotted according to sex and MS phenotypes, and differences between the groups were assessed using the log-rank test.
We utilized an extended Cox regression model, adjusting for baseline characteristics and time-varying exposure. Results are reported as hazard ratios (HRs) with 95% confidence intervals (CIs) and statistical significance was set at p < 0.05. We included n = 11 variables in the full model (Supplementary Table 1). Models were tested to assess the proportionality of hazards, which were found to be violated by age and phenotype. To address this, the age was grouped, and we adjusted the model for age and phenotypes as strata. Furthermore, recognizing that progressive phenotypes have a higher mortality than those with relapsing remitting MS and are not comparable in age and disease duration, we conducted separate analyses. To increase statistical power secondary progressive multiple sclerosis (SPMS) and primary progressive multiple sclerosis (PPMS) were grouped as progressive MS phenotypes, achieving almost 80% power, while the relapsing remitting MS group achieved a power of 80%–85%.
Several variables exhibited missing values. The extent of missingness and the chosen method for handling it are detailed in Supplementary Table 3. To assess the robustness of our findings, we performed sensitivity analysis using complete case analysis.
Ethical statement
The study was reported to the National Committee on Health Research Ethics (SJ-971 (anm.nr. 88070) EMN-2022-00118), and according to Danish law, no formal approval or informed consent was needed. 18 The study was reported to and approved by the institutional review board at Zealand University Hospital (Data and Development support, Research inventory, REG-160-2021) and was conducted according to the Declaration of Helsinki 19 and General Data Protection Regulation (GDPR). 20
Results
A total of 9929 individuals were included in the study, contributing 105 115 person-years at risk (Table 1). In total, 316 patients died during a median follow-up period of 10.3 years [interquartile range (IQR) = 6.0–15.1]. Most patients were female (68.1%), and the median age at diagnosis was 39 years [31–48]. In total, 77% of the patients had medium or high education levels, 50% were married and 38% were single at baseline. The median EDSS score at baseline was 2 [1.5–3]. Individuals with progressive MS phenotypes were older at diagnosis (48 years [40–55]), had a higher EDSS score (3.5 [2–5]) and a lower level of education (Table 1).
Population characteristics.
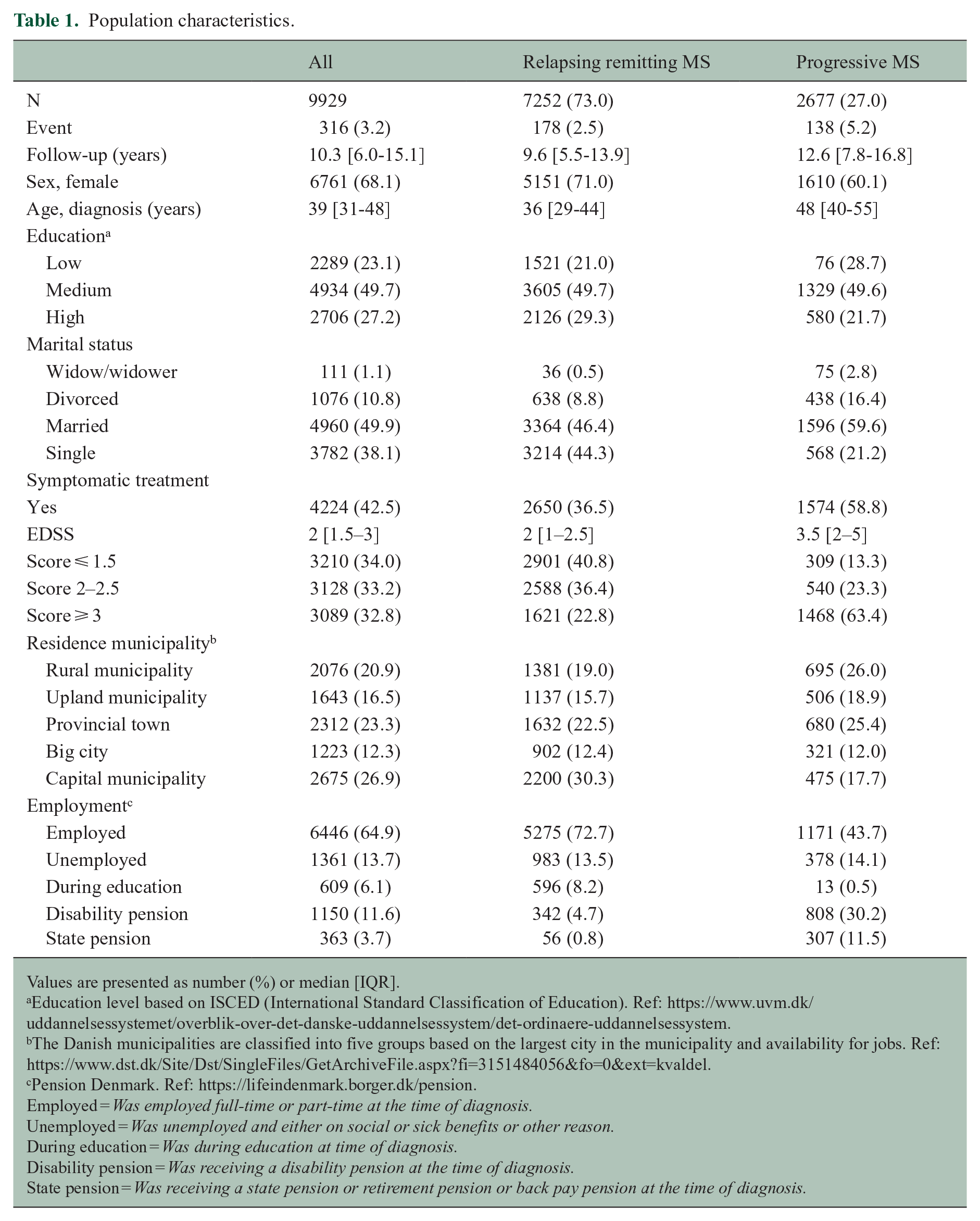
Values are presented as number (%) or median [IQR].
Education level based on ISCED (International Standard Classification of Education). Ref: https://www.uvm.dk/uddannelsessystemet/overblik-over-det-danske-uddannelsessystem/det-ordinaere-uddannelsessystem.
The Danish municipalities are classified into five groups based on the largest city in the municipality and availability for jobs. Ref: https://www.dst.dk/Site/Dst/SingleFiles/GetArchiveFile.aspx?fi=3151484056&fo=0&ext=kvaldel.
Pension Denmark. Ref: https://lifeindenmark.borger.dk/pension.
Employed = Was employed full-time or part-time at the time of diagnosis.
Unemployed = Was unemployed and either on social or sick benefits or other reason.
During education = Was during education at time of diagnosis.
Disability pension = Was receiving a disability pension at the time of diagnosis.
State pension = Was receiving a state pension or retirement pension or back pay pension at the time of diagnosis.
Survival probability
The overall rate of mortality was 3.0 (95% CI = 2.7–3.3) per 1000 person-years, with 91% (95% CI = 89%–92%) survival probability in the population (Figure 2). The survival was lower in males compared to women (log-rank p < 0.001) and in patients with progressive MS phenotypes compared to patients with relapsing remitting MS (log-rank p < 0.001) (Figure 2). The rate of mortality was higher for patients with progressive phenotypes (4.2, 95% CI = 3.6–5.0, per 1000 person-years) compared with patients with relapsing remitting MS (2.5, 95% CI = 2.1–2.8, per 1000 person-years).
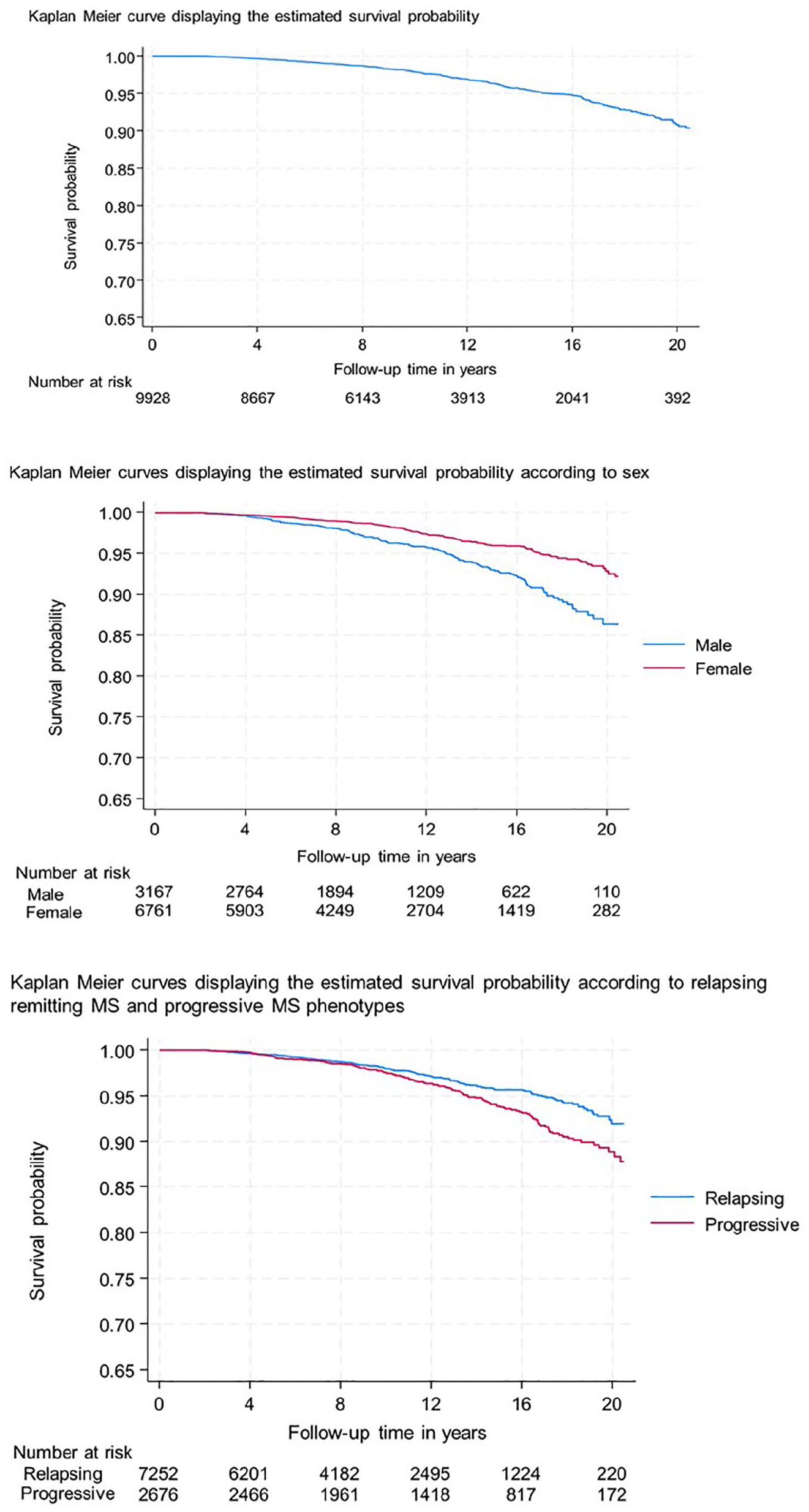
Kaplan–Meier curves displaying the estimated survival probability, overall and in stratified analyses.
Risk of death, adjusted analysis
In an extended Cox proportional hazards model incorporating visits to specialized care as a time-varying exposure, we found no statistically significant association between the number of visits and risk of death among individuals with MS in Denmark (HR = 1.00; 95% CI = 0.99–1.02) (Figure 3). Similar findings were observed when stratifying the analysis by relapsing remitting MS (HR = 0.99; 95% CI = 0.97–1.01) (Figure 4) and progressive phenotypes (HR = 1.01; 95% CI = 0.99–1.04) (Figure 5).
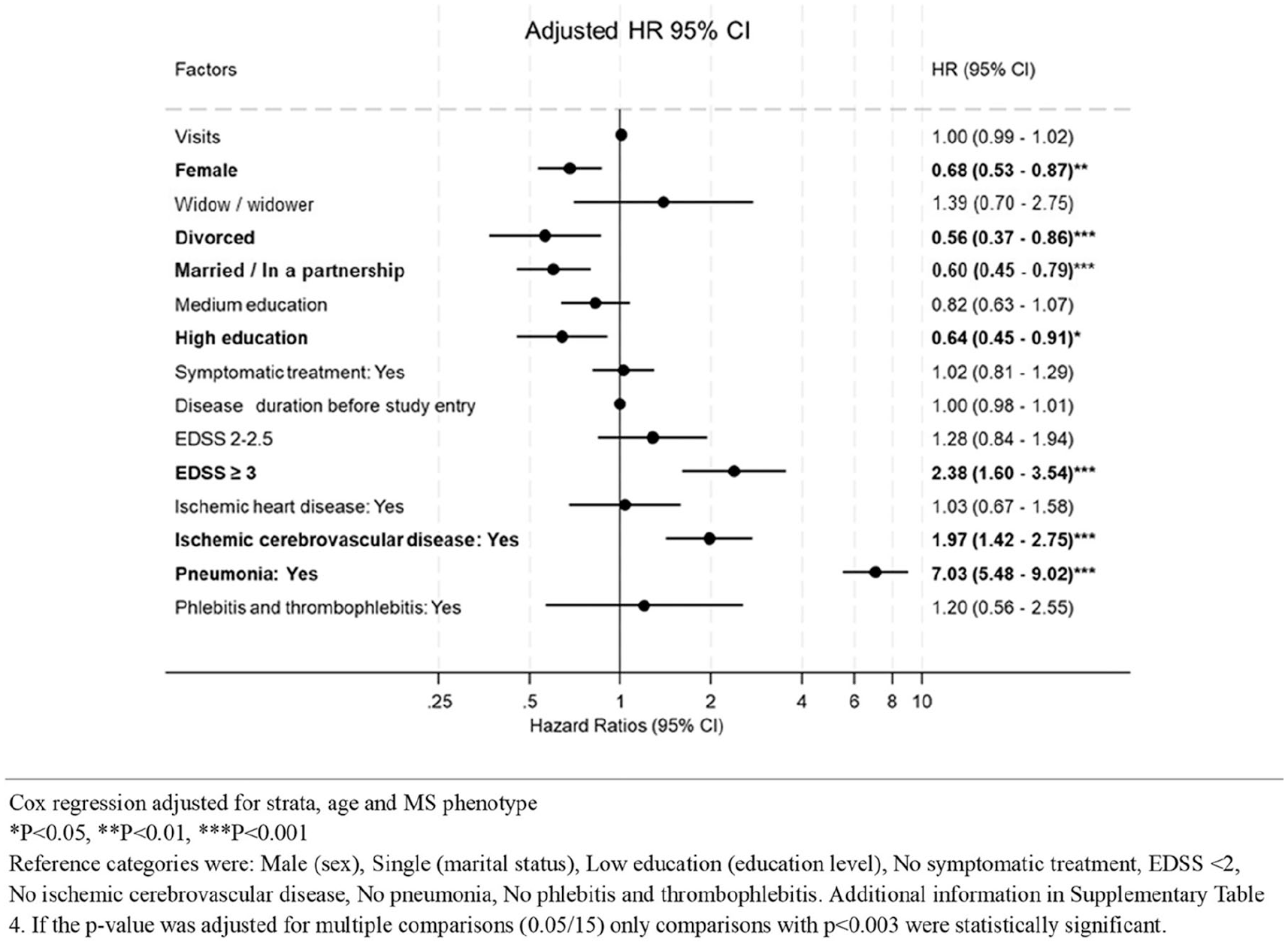
Risk of death in individuals with MS in Denmark.
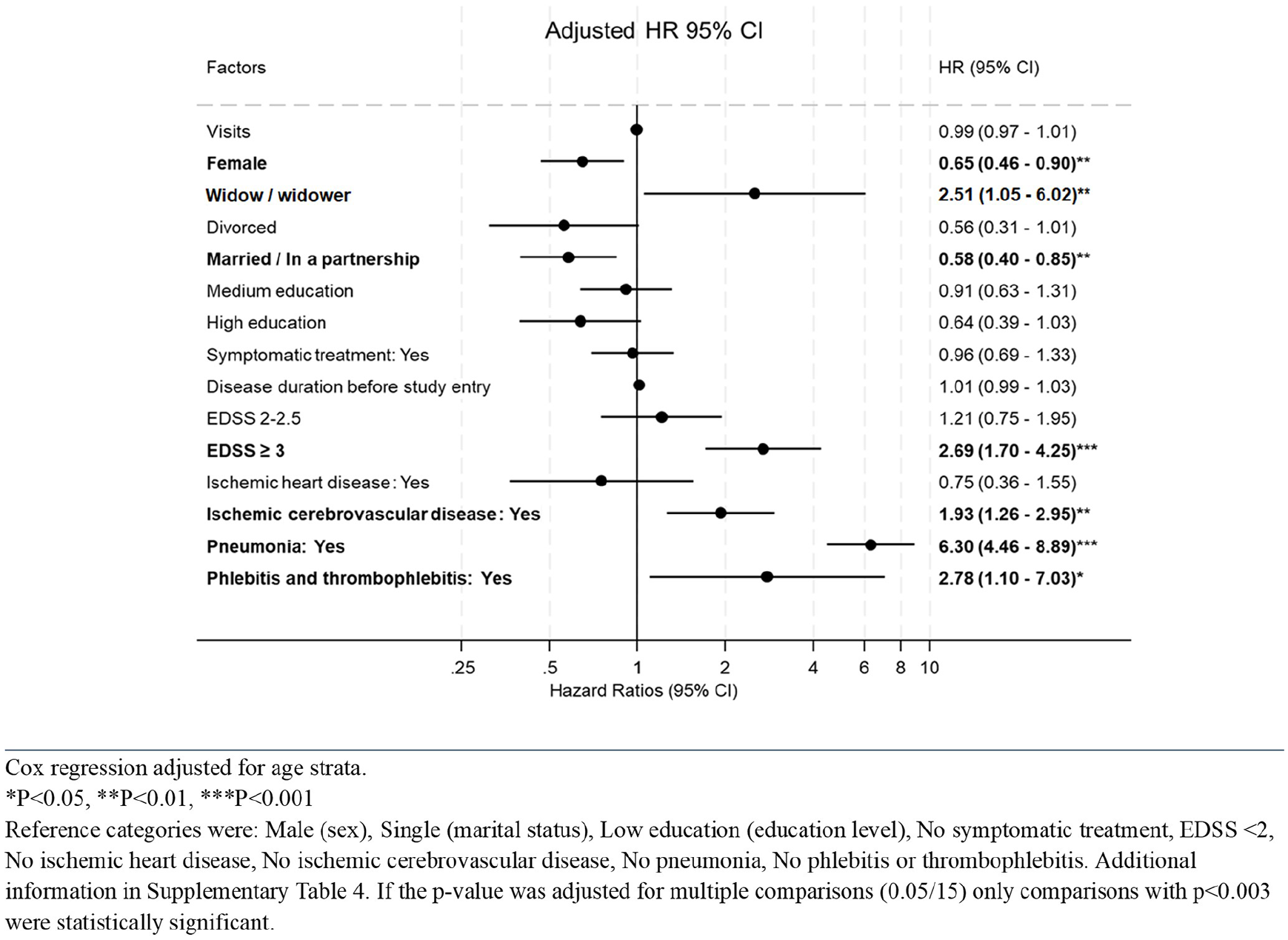
Risk of death in individuals with relapsing remitting MS in Denmark.
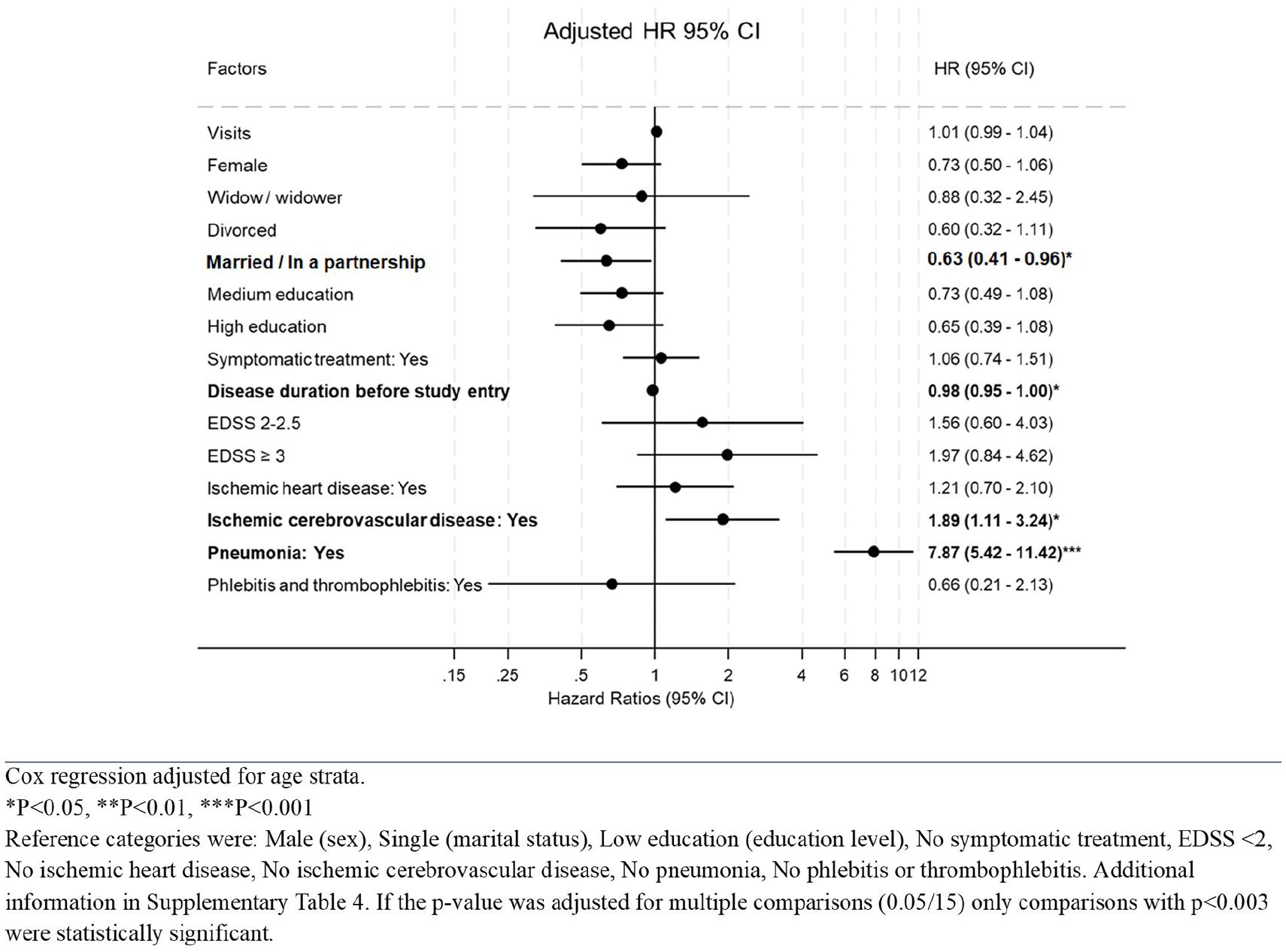
Risk of death in individuals with progressive MS phenotypes in Denmark.
Several baseline factors showed independent associations with mortality. Female sex was associated with a decreased hazard of death (HR = 0.68; 95% CI = 0.53–0.87) compared to males, and being divorced or married was associated with a lower mortality risk relative to being single (HRs = 0.56 and 0.60, respectively). Higher education was associated with reduced mortality compared to low education (HR = 0.64; 95% CI = 0.45–0.91). No significant associations were observed for medium education level. Disease severity measured by EDSS score was strongly associated with mortality. Compared with individuals with EDSS < 2, individuals with EDSS ⩾ 3 had an increased hazard for death of 2.38 (95% CI = 1.60–3.54). The use of symptomatic treatment and disease duration before study entry was not statistically associated with mortality after adjustment (Figure 3). Time-varying comorbidities were important predictors. Ischaemic cerebrovascular disease (HR = 1.97; 95% CI = 1.42–2.75) and pneumonia (HR = 7.03; 95% CI = 5.48–9.02) were both associated with a significantly increased hazards of death, whereas ischaemic heart disease was not (Figure 3).
Stratified analysis by MS phenotypes (Figures 4 and 5) yielded consistent findings with no association between visits and mortality observed, and pneumonia remained the strongest predictor of mortality across subgroups.
Sensitivity analysis
Results for the main analysis using multiple imputation by chained equation (MICE) modelling for imputation are presented in Supplementary Table 4. In Supplementary Table 5, the results of complete case analysis are presented for comparison. Overall, the sensitivity analysis revealed consistent findings across the models.
Discussion
In this large nationwide cohort of individuals with MS in Denmark, we found no evidence of visits to specialized care was associated with mortality. Visits were incorporated as time-varying exposure, allowing for dynamic assessment over time, yet the adjusted HRs were statistically not significant across the analysis, including after stratification by MS phenotypes. These findings suggest that simply increasing the number of visits to specialized care, without regard to visit content or quality, may not in itself improve survival benefits.
People with MS often have complex healthcare needs, and access to specialists experienced in managing the condition and providing effective care could influence both treatment success and overall health outcomes. 21 The strong association of mortality with comorbidities such as pneumonia and ischaemic cerebrovascular disease highlights that interventions aimed at comorbidity prevention and management may have a greater potential to improve survival than visit frequencies alone. These findings are consistent with prior research suggesting that respiratory and vascular diseases contribute to increased mortality among people with MS.3,22
Being female was linked to a reduced risk of mortality compared to males, consistent with existing evidence on mortality in individuals with MS.22,23 Lifestyle and behavioural factors may play a role, as males may engage less frequently in health-seeking behaviours, contributing to poorer health outcomes.24,25 These findings highlight the importance of focusing on sex differences in clinical practice to address challenges faced by male patients.
Lower education was associated with increased mortality. Higher education provides access to better employment, earnings and health care while enhancing health knowledge and social resources.26,27 Promoting education may benefit individuals with MS.
A high EDSS score at baseline was associated with increased mortality. This is consistent with previous research showing that higher levels of disability are associated with poorer health outcomes and mortality. 3 This highlights the importance of addressing disability progression through both pharmacologic and non-pharmacologic interventions.
Overall, our findings suggest that while specialized care remains essential for the management of MS, the number of visits alone does not appear to reduce mortality. Focused efforts on quality of care, prevention and management of comorbidities and early treatment initiation may be more impactful targets for improving survival outcomes in patients with MS in Denmark.
Strength and limitations
Our study benefits from a large sample size and incorporation of time-varying covariates; however, some limitations should be addressed.
Although we adjusted for a wide range of factors, residual confounding may exist. Unmeasured lifestyle factors, for example, smoking, physical activity and obesity, were not included due to a lack of data availability, which could impact survival and health outcomes. Moreover, we did not adjust for factors such as accidents and suicide, depression, cancer and chronic lung diseases that are known to increase mortality among people with MS.
We conducted the analysis for relapsing remitting MS and progressive phenotypes separately, so the existing differences were less likely to influence the results. 28 However, the analysis of the group with progressive phenotypes was slightly underpowered which should be taken into consideration when interpreting the results. While the study’s findings are applicable to Denmark’s MS population, generalizing them to other countries may be limited by differences in healthcare systems, MS care protocols and demographic factors.
Because the exposure of interest, visit, was not known at baseline, it required to be modelled as a time-varying covariate using an extended Cox model. This approach ensured that patients were classified as having had a visit only at the time it occurred, thereby updating the exposure status over time. By doing so we prevented misclassification and avoided introducing immortal time bias,29,30 which could otherwise lead to false associations between exposure and the outcome.
The study benefits from linking multiple high-quality national registries, providing reliable and validated information, and the long follow-up period allows for robust survival analysis, capturing long-term outcomes and trends in mortality among MS patients. Future research should explore whether specific types of specialized care visits might influence survival differently.
Conclusion
We found no association between the frequency of visits to specialized care in Danish MS clinics and mortality. Our finding suggests that improving survival in patients with MS may require a focus on quality and content of care, as well as proactive management of comorbidities, rather than simply increasing visit frequency. Disparities in survival by sex, education and marital status underscore the need to address social determinants alongside clinical care.
Supplemental Material
sj-docx-1-msj-10.1177_13524585251353079 – Supplemental material for Assessing the association between mortality and clinical follow-up visits in multiple sclerosis
Supplemental material, sj-docx-1-msj-10.1177_13524585251353079 for Assessing the association between mortality and clinical follow-up visits in multiple sclerosis by Agata Beczek, Eskild Morten Landt, Melinda Magyari, Lars Kristian Storr and Morten Dahl in Multiple Sclerosis Journal
Footnotes
Acknowledgements
The authors thank participants and staff of the Danish Multiple Sclerosis Register for their important contribution.
Data Availability Statement
Additional technical details, statistical codes, and derivative data are available from the principal investigator. Access to data for further analyses can be arranged through direct collaboration or locally managed agreements with the principal investigator.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Dr M.D. has consultancies or sponsored talks with Chiesi, Takeda and Grifols. Dr M.M. has served on scientific advisory board for Sanofi, Novartis, Merck, Moderna and has received honoraria for lecturing from Biogen, Merck, Novartis, Roche, Sanofi and Bristol Myers Squibb. The other authors declared no conflict of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study is initiated by the Department of Neurology Region Zealand, Denmark, and supported by grants from the Multiple Sclerosis Comprehensive Plan by The Danish Ministry of Health. The sponsor of the study is a public and non-profit organization that had no role in the study’s design, conduct or reporting.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.