
Abstract
Background:
Investigations of a prodrome in multiple sclerosis (MS) usually have included adults.
Objective:
To compare rates and reasons for health care use in youth with and without MS, considering time relative to the MS index date and to birth.
Methods:
This retrospective cohort study used population-based administrative data (1991–2020) from Ontario, Canada. We matched youth (<18 years) with MS up to 5:1 to youth without MS by sex, birth year, region, and duration of observation (full cohorts). Subcohorts had data from birth to MS index date (first demyelinating disease claim). We compared health services use, adjusting for age, sex, area-level income, region, and year.
Results:
We included 451 individuals with pediatric-onset MS and 1422 without MS. As of 6 years pre-index, the full MS cohort had higher physician services use (year 6: rate ratio (RR) = 1.45; 95% confidence interval (95% CI) = 1.25–1.67) and hospitalizations (RR = 2.79; 95% CI = 1.31–5.94). Findings were similar in subcohorts. The MS subcohort had elevated physician visit rates in early life that rose as the MS index date approached.
Discussion:
Youth with pediatric-onset MS exhibit increased health care use from birth. Early life may be a risk period for MS. A prodromal phase may emerge 6 years before the onset of typical MS symptoms.
Introduction
Multiple reports indicate changes in health care use preceding presentation with multiple sclerosis (MS) by 5–10 years, observed using clinical or administrative databases.1,2 These changes in health care use could reflect prodromal disease; rises in serum neurofilament light chain levels 6–10 before clinical presentation biologically support this concept.3,4 The identification of prodromal disease could lead to earlier intervention and clarify the etiologically relevant period for preventing MS.
Most studies have focused on adult populations1,2 in which confounding may occur due to comorbidities, diagnostic delays, and unrelated life experiences. Pediatric populations have a lower comorbidity burden and fewer irrelevant events, offering the opportunity to better characterize the features and onset of prodromal disease. A German study reported that obesity, vision disorders, and skin sensation disturbances were more common 5 years before a first MS diagnostic code among youth with MS than those without MS or with juvenile inflammatory arthritis. 5 This study was limited to physician billings, suggesting further exploration of health care use preceding presentation with pediatric-onset MS is warranted. However, fluctuations in health care use in childhood related to well-childcare must be considered.
We used population-based data to compare rates of and reasons for hospitalizations and physician services use in youth with and without MS, considering time relative to the MS index date and time relative to birth.
Methods
Setting
We conducted this matched retrospective cohort study in Ontario, where 38% of the Canadian population resides. 6 The publicly administered, provincial health insurance plan covers medically necessary physician, hospital, and related services.
Data sources
We used multiple administrative datasets, held by ICES, which capture health services used by Ontario residents including the registered persons’ database; discharge abstract database; Ontario Health Insurance Plan database; and ICES Physician Database over the period April 1991 to March 2020 (see Supplemental E-Methods). Diagnoses are recorded using the International Classification of Disease (ICD) 9th edition or 10th edition—Canadian modification. These datasets were linked using unique encoded identifiers and analyzed at ICES. We obtained ethics approval from the University of British Columbia’s Clinical Research Ethics Board. Data access (via ICES) was authorized under section 45 of Ontario’s Personal Health Information Protection Act.
Study populations
We identified individuals with pediatric-onset MS, aged < 18 years, using a validated case definition (see Supplemental E-Methods). 7 The earliest ICD-9/10-CA claim for demyelinating disease was the index date. We excluded individuals lacking valid registration numbers, ineligible for health care coverage at the index date and lacking health care coverage ⩾90% of the 5 years preceding the index date, or between the index date and third MS claims.
Each individual with MS was matched to individuals without MS (“non-MS”), by sex, exact birth year, first three digits of the postal code at the index year, and duration of observation; a minimum of one match was required, and we selected up to five matches where available. We also identified subcohorts of individuals with and without MS with data available from birth to index date.
Outcomes
Outcomes included (1) annual rates of health care use including inpatient hospitalizations and physician visits; (2) annual rates of use by types of physicians/specialists seen (see Supplemental E-Methods); and (3) reasons for health care use grouped by ICD chapters over the entire study period (Supplemental Table e1).
Covariates
Covariates included sex, area-based income derived from census data in quintiles at the index date, urban/rural region based on the second character of the postal code at the index date, and index year.
Analysis
We compared rates of each outcome between the matched cohorts using rate ratios (RRs; 95% confidence intervals (95% CI)) based on a Poisson distribution using the time scale of year relative to the index date (i.e. year 1 is 1 year pre-index). To test the association between year relative to the index date, cohort (MS vs. non-MS), and each outcome, we constructed negative binomial regression models, using the natural log of person-time as the model offset and generalized estimating equations (exchangeable working correlation matrix) to account for repeated measurements. We adjusted for age (continuous), sex (male as reference), area-based income quintile (linearized), region (rural as reference), and index year (continuous). To examine whether rates of health care use differed over time between cohorts, we included an interaction term between the year pre-index and cohort, for consistency with the adult literature. 1 We tested for effect modification by age and sex. Since cohort size and follow-up duration varied over the observation period, we repeated the analysis in MS and matched cohorts with complete data from birth.
For the subcohorts only, we also examined the rates of each outcome according to a second time scale, year relative to birth (i.e. birth year is year < 1). The second time scale illustrated the changes in health care use experienced early in life due to well-childcare visits. We modified the multivariable regression models to use year relative to birth as the time scale (as a categorical variable), and then adjusted for year relative to the index date (as a continuous variable). We included interaction terms: year relative to birth*cohort, year relative to the index date*cohort, year relative to birth*year relative to the index date, and year relative to birth*cohort*year relative to the index date. Non-significant terms were dropped.
Complementary analyses
We repeated analyses in the subcohort of individuals aged ⩾ 12 years to exclude possible misdiagnoses due to myelin oligodendrocyte protein antibody disease (MOGAD); while MOGAD can occur at all ages, the relative proportion of incident demyelinating events due to MOGAD versus MS is the highest in those < 12 years. Second, for the most coded ICD chapters, we explored the frequency of diagnosis codes over the entire observation period within the total MS cohort and MS subcohort for whom data were available at birth. Those analyses focused on physician visits, as the number of codes was sufficiently high to be generally stable and to avoid small cells. Third, we used reported delays between symptom onset and diagnosis in pediatric MS 8 to generate a distribution of diagnostic lags of mean (SD) 2.5 (5.04) years, which we randomly assigned to MS cases and matched controls, then repeated analyses related to hospitalizations and physician visits (see Supplemental E-Methods). Fourth, we tested whether the associations observed in the primary analysis were modified by diagnostic criteria changes (see Supplemental E-Methods). Finally, among MS cases with mental illness visits pre-index, we examined mental illness visits post-index (see Supplemental E-Methods). Statistical analyses used SAS V9.4 (SAS Institute Inc., Cary, NC, USA).
Results
We evaluated 451 individuals with pediatric-onset MS and 1422 individuals without MS in the main analysis (Supplemental Figure e1 and Table 1). The median duration of follow-up was 11 years pre-index date, with 441 MS and 1384 non-MS individuals contributing 5 years of data, 274 MS and 947 non-MS individuals contributing 10 years, and only 32 MS and 32 non-MS individuals contributing 18 years. Almost two-thirds of each cohort were female; half were aged 16 to < 18 years and most lived in urban areas at the index date.
Characteristics of the Pediatric-Onset MS and the Matched Cohorts at the Index Date.
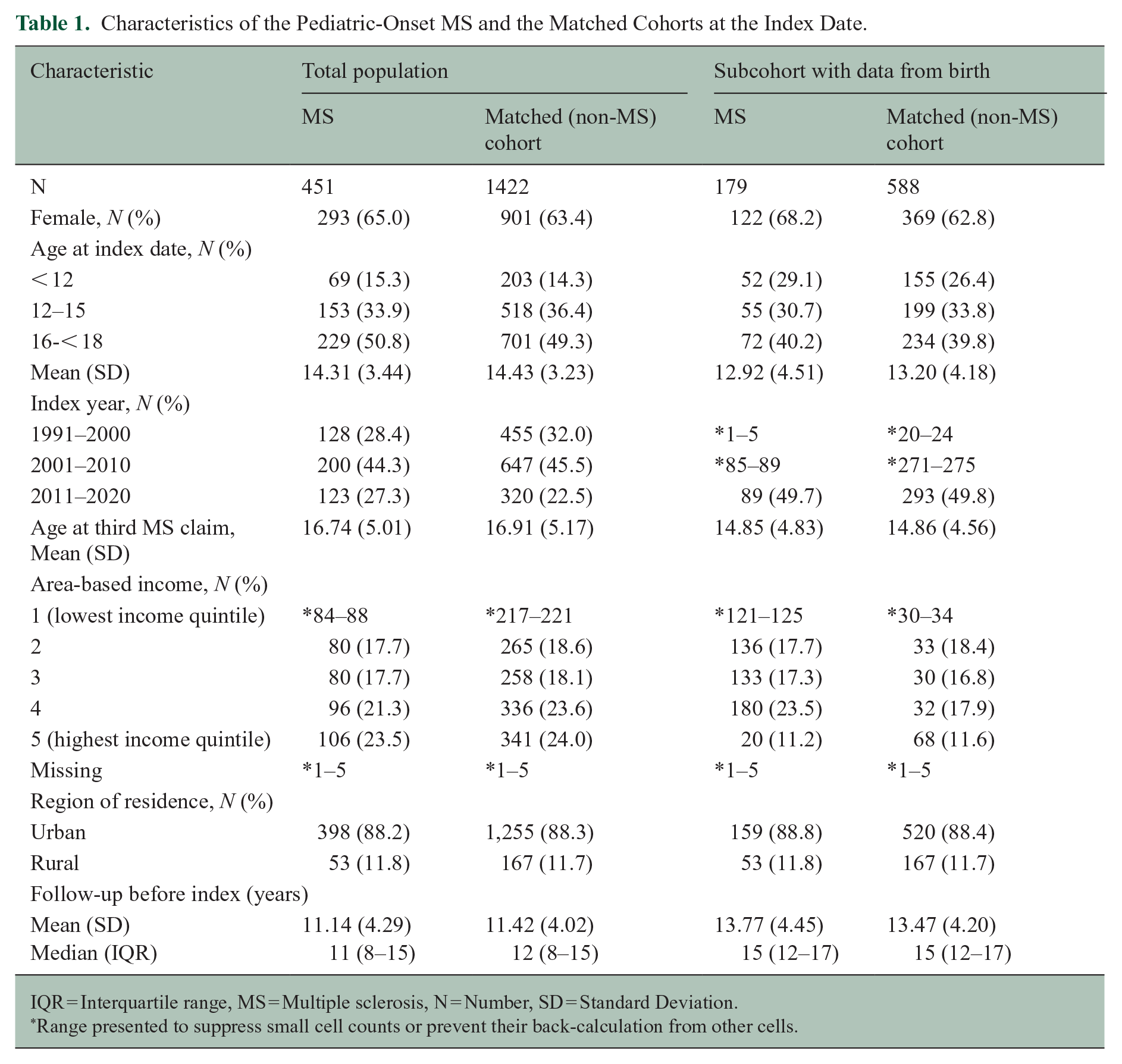
IQR = Interquartile range, MS = Multiple sclerosis, N = Number, SD = Standard Deviation.
Range presented to suppress small cell counts or prevent their back-calculation from other cells.
The subcohort comprised 179 individuals with MS and 588 without MS. A slightly lower percentage (40.2%) were aged 16 to < 18 years at the index date as compared to the whole cohort, and correspondingly the mean (SD) age at the index date was 12.92 (4.51) in the MS subcohort (vs. 14.31 (3.44) years in the total MS sample), and duration of follow-up was longer. Other characteristics examined were comparable to those in the whole cohort (Table 1).
Annual rates of health care use relative to MS index date
Unadjusted
In the MS cohort, rates of physician services use resembled a U-shaped curve, with rates decreasing from year 18 to year 7, following which rates rose again to year 1. In the non-MS cohort, rates of physician services use decreased from year 18 to year 5 and remained stable thereafter (Figure 1(a)). Rates of physician services use were consistently higher in the MS than in the non-MS cohort except for year 16; the highest rate ratios were in year 1 (RR = 2.50; 95% CI = 2.40–2.59). Although hospitalization rates were lower, we similarly observed the highest hospitalization rates in years 18 and 17. These rates declined in both cohorts, remaining relatively flat thereafter until year 2 in the MS cohort, when they rose again (Figure 1(b)) (see Supplemental Figure e2 for subcohorts).
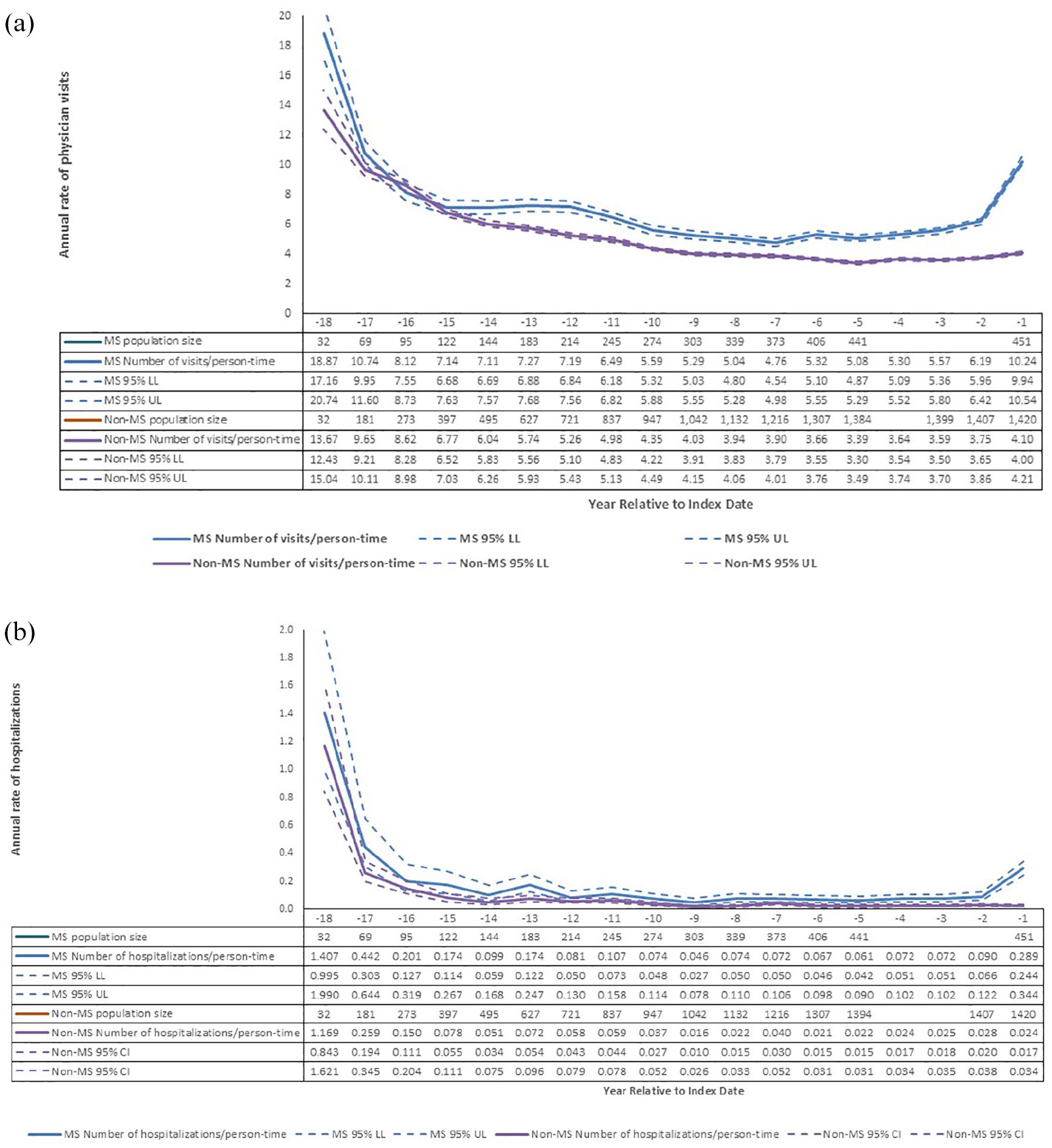
Crude rates of health care use in multiple sclerosis (MS) and non-MS cohorts before the first demyelinating disease claim: (a) physician visits; (b) hospitalizations.
Adjusted
For the whole cohorts, the MS cohort had higher adjusted rates of physician services use from year 18 onward (RR = 1.43; 95% CI = 0.99–2.07), although these differences were not statistically significant for years 15 through 18. Rate ratios were generally stable, ranging from 1.21 to 1.39 until year 6 when they rose consistently, with a more marked divergence between the MS and non-MS cohorts emerging at year 2 (RR = 1.63; 95% CI = 1.43–1.85, Figure 2(a) and Table e2).
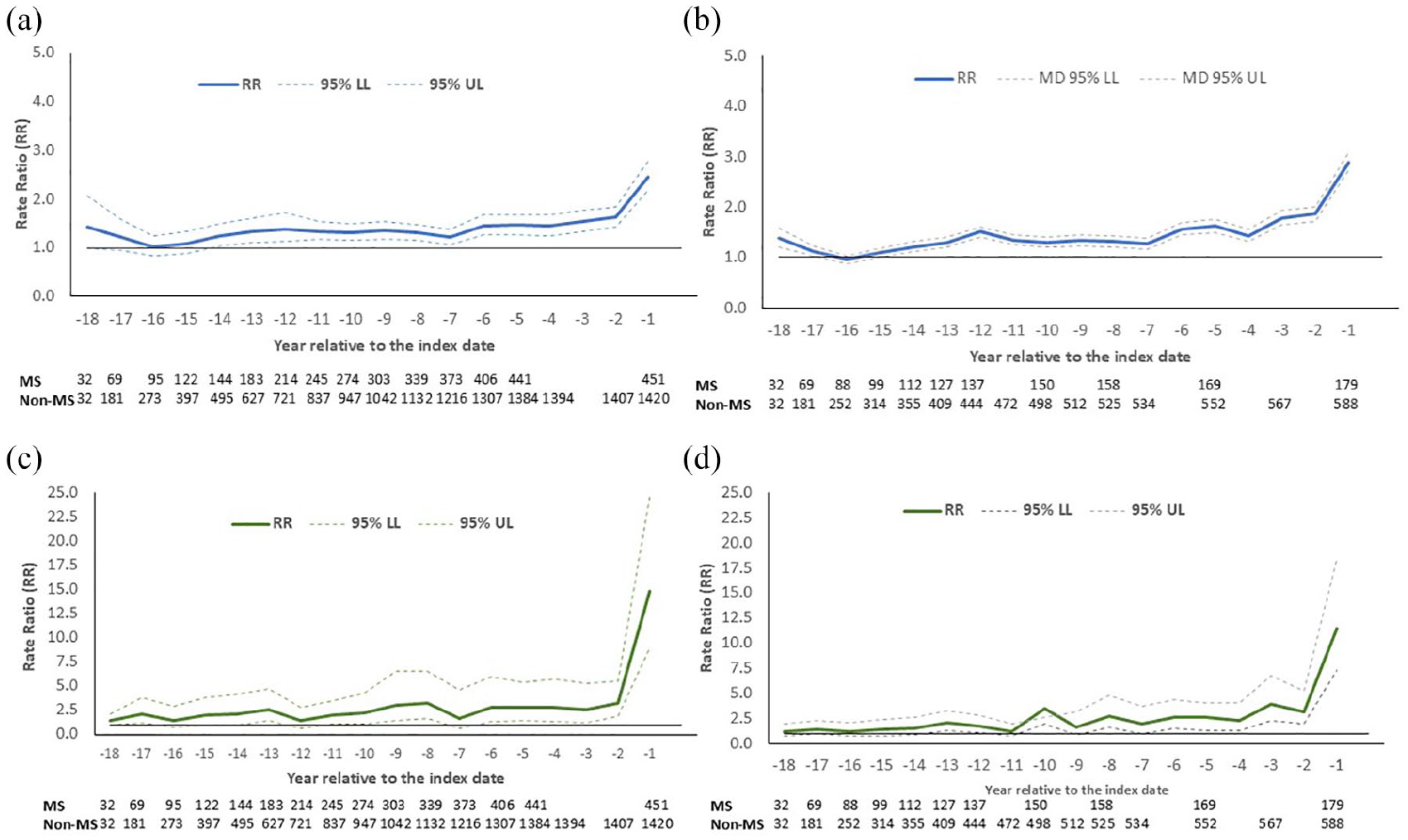
Adjusted rate ratios (RR) for association between multiple sclerosis and rates of health care utilization according to year relative to the index date: (a) physician visits in the whole cohort; (b) physician visits in the subcohort with data to birth; (c) inpatient hospitalizations in the whole cohort; (d) inpatient hospitalizations in the subcohort*.
Patterns were similar for hospitalizations, although differences between the MS and non-MS cohorts fluctuated regarding the statistical significance and magnitude of associations, most marked at year 2 (Figure 2(c) and Table e2).
In the subcohort with data from birth to the index date, we observed the same pattern and similar strengths of association for physician visits and hospitalizations (Figure 2(b) and (d)), albeit with more variability. We did not observe effect modification by sex or age at index.
Annual rates of health care use relative to birth
In unadjusted analyses, using the time scale relative to birth, the highest rate of physician visits and hospitalizations in both cohorts was in the first 2 years of life, decreasing to a nadir between ages 9 and 11 years, then increasing thereafter (Supplemental Figure e3).
In adjusted analyses for physician visits, cohort interacted with time relative to birth (χ2 = 40.6, p = 0.0011) and time relative to the MS index date (χ2 = 7.4, p = 0.0064), indicating physician visit rates differed over time between the MS and non-MS cohorts for both time scales. Specifically, the MS cohort had higher physician visit rates up to 10 years before the index date (RR in year 10 = 1.29; 95% CI = 1.13–1.49), and in early life (RR birth year = 2.12; 95% CI = 1.56–2.89; year 5 = 1.32; 95% CI = 1.11–1.57) which persisted at older ages (Table 2).
Adjusted rate ratios (95% confidence intervals): association of subcohort (multiple sclerosis vs. non-multiple sclerosis) with health care use by: (A) year relative to birth and (B) index date (selected years)*.
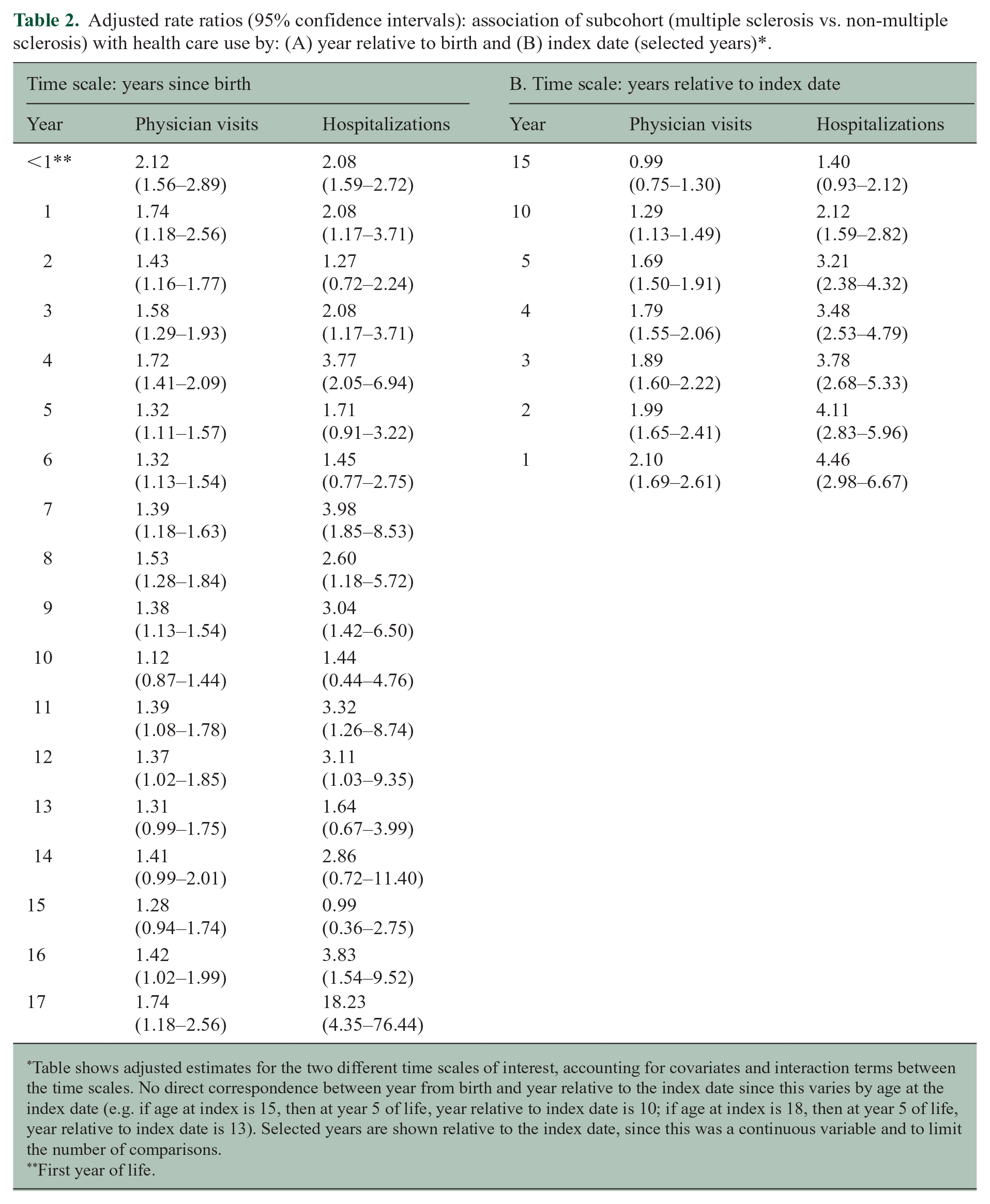
Table shows adjusted estimates for the two different time scales of interest, accounting for covariates and interaction terms between the time scales. No direct correspondence between year from birth and year relative to the index date since this varies by age at the index date (e.g. if age at index is 15, then at year 5 of life, year relative to index date is 10; if age at index is 18, then at year 5 of life, year relative to index date is 13). Selected years are shown relative to the index date, since this was a continuous variable and to limit the number of comparisons.
First year of life.
Findings were similar for hospitalizations, where we also observed interactions between cohort and both time scales (birth χ2 = 34.0, p = 0.0084; index date χ2 = 10.1, p = 0.0015). Considering these interactions, the MS cohort had higher hospitalization rates up to 10 years before the index date (RR in year 10 = 2.12; 95% CI = 1.59-2.82) when compared to the non-MS cohort. The MS cohort also had higher hospitalization rates in early life (RR year 0 = 2.08; 95% CI = 1.59–2.72; year 4 = 3.77; 95% CI = 2.05–6.94) (Table 2).
Specialists
Over the entire observation period, the MS cohort had higher rates of visits to nearly all specialist types examined in unadjusted analyses; rates were 14-fold higher for neurologists and neurosurgeons, 5-fold higher for psychiatrists, and 4-fold higher for physiatrists (Table 3). When examined by year, the elevated visit rates with neurologists emerged at year 15, with neurosurgeons at year 13, and psychiatrists at year 12, the latter being consistently statistically significant from year 7 onward (Supplemental Table e3A and e3B).
All years before the first demyelinating claim: unadjusted rate ratios for physician encounters by specialty, comparing cohorts with and without multiple sclerosis.
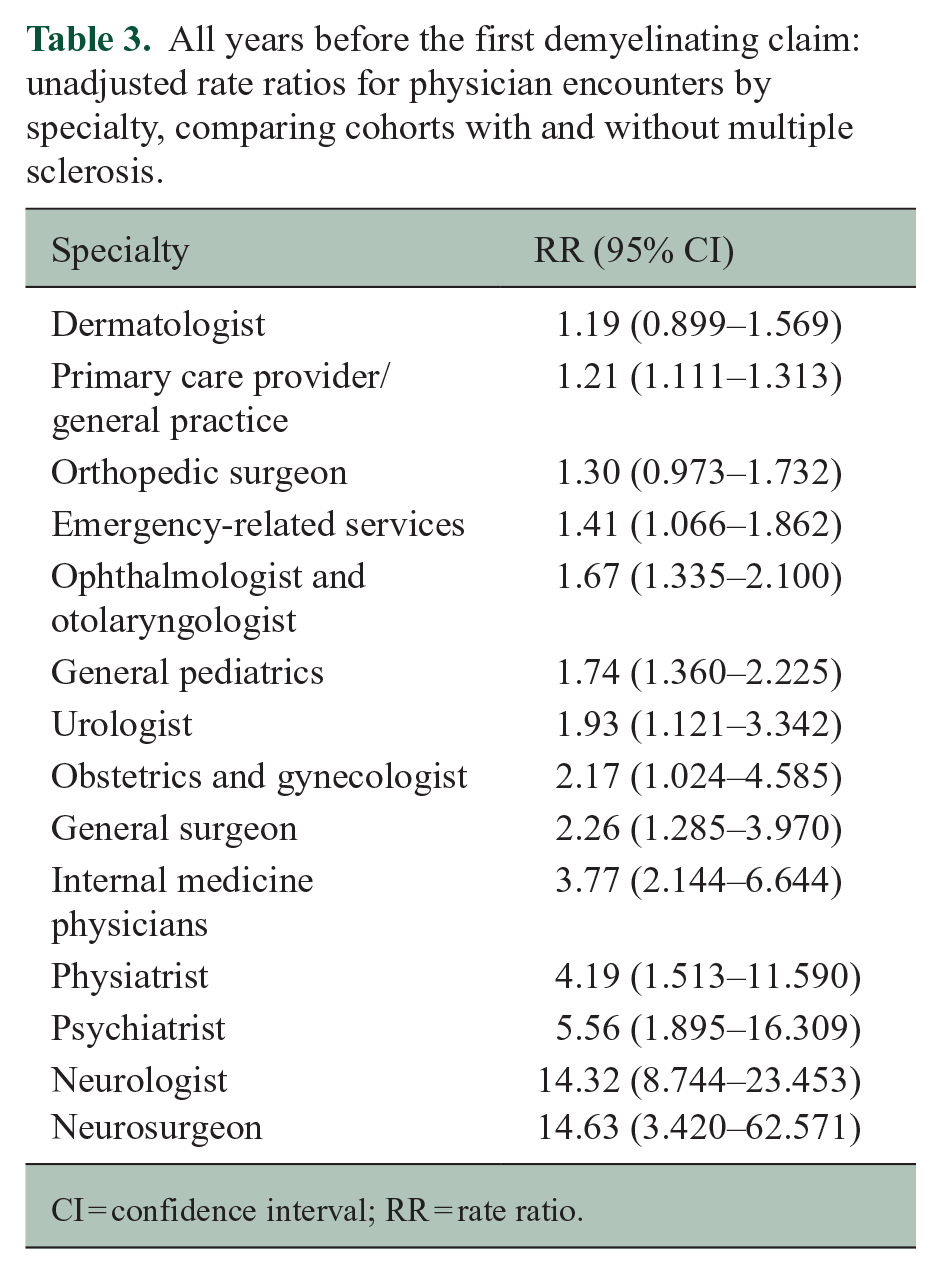
CI = confidence interval; RR = rate ratio.
In the subcohorts with data from birth, across the entire observation period, the providers with the highest relative visit rates remained the same (neurologists, psychiatrists, physiatrists) although the magnitude of the associations differed slightly, and confidence intervals were broader (Supplemental Table e4). The timing of the elevated visit rates was also similar (Supplemental Table e5A and e5B). In the first year of life, the MS cohort had higher rates of visits to internists, neurologists, dermatologists, primary care providers, general pediatricians, and urologists (Supplemental Table e6).
Complementary analyses
Analyses limited to the subcohort with data from birth and age of MS index ⩾ 12 years, the direction of the associations was like those in the full subcohort (from Table 2), although some confidence intervals were broader (Supplemental Table e7). In analyses accounting for diagnostic lag, the magnitude of some associations in the full cohorts was attenuated, the pattern and years with statistically significant findings remained similar (Supplemental Table e8). This was also true in the subcohorts for physician visits; most associations for hospitalizations (where event rates were lower) were no longer statistically significant (Supplemental Table e9).
Over the entire observation period, the MS cohort had higher rates of health care use for all ICD-9 chapters except diseases of the blood and blood-forming organs and diseases of the skin and subcutaneous organs, although some 95% CIs were broad, particularly for hospitalizations (Supplemental Table e10, E-results). The association between MS and physician visits relative to the index date persisted across all index year groups (Supplemental Table e11). Of 211 children with a mental health visit pre-index, all had a mental health visit within 1 year post-index; mental health visits continued for an average (SD) of 16.5 (6.7) consecutive years.
Discussion
In this population-based study, health care use differed between youth with and without MS from birth onward. These differential patterns resembled a U-shaped curve with particularly elevated relative rates in the earliest years of life, less evident but persistent differences in early childhood, and subsequent progressive divergence in the last 6–7 years before the index date. The MS cohort had higher rates of health care use for nearly all specialist types and nearly all ICD-9 chapters examined; differences were most marked for neurologists, neurosurgeons, psychiatrists, physiatrists, diseases of the circulatory system, congenital anomalies, symptom signs and ill-defined conditions, and neoplasms.
Differences in health care use in the earliest years of life suggest that perinatal maternal-fetal-neonatal interactions may be associated with the risk of pediatric-onset MS, as observed in other chronic diseases.9–11 Several studies have suggested that exposures occurring perinatally may affect MS risk. In a meta-analysis, higher gestational vitamin D levels were associated with lower MS risk in adulthood. 12 In a case–control study, maternal prenatal illness was associated with increased odds of pediatric-onset MS, whereas delivery by Cesarean section was associated with reduced odds. 13 A more recent systematic review identified 33 studies that did not identify any consistent prenatal or perinatal risk factors; vitamin D was not evaluated. 14 Nonetheless, our findings suggest exploration of early life as a critical exposure window is warranted.
Health care use diverged further between the MS and non-MS cohorts as the MS index date approached. In adults, differences in health care use 5–10 years before the first identified health contact for demyelinating disease or the neurologist-recorded MS symptom onset, 1 or the first code for MS in primary care datasets, 2 have been interpreted as reflecting a possible prodromal phase of disease. Biological evidence of a prodrome has included elevated serum neurofilament light levels among individuals who developed MS 6–10 years before onset of typical clinical manifestations.3,4,15 Comparable work in the pediatric MS population is limited. In our prior study using Ontario administrative data, youth with MS had higher health care use than youth without MS in the year before the index date. 16 The present work substantially extended the observation period pre-index. A recent study involving 21 youth with MS evaluated at a US tertiary care center reported higher health care use in the year before their incident demyelinating event 17 for neurological and non-neurological (infections, musculoskeletal, dermatologic issues, and injuries) reasons. One-third of the cohort had neurological symptoms over 2 years before the incident event. A German study also used administrative data, but focused on physician billing data, and the 5 years before a first MS diagnosis code. As compared to youth without MS or with another inflammatory disease, juvenile inflammatory arthritis, obesity, vision disorders, and skin sensation disturbances were more common. 5 Identification of vision disorders and skin sensation disturbances in that study raised the question as to whether these findings reflect missed opportunities for diagnosis, an issue also raised in studies of adult MS populations. 18 However, the findings in the present study likely cannot be fully explained by this. First, we observed differences in health care use beginning in the first year of life. Second, although some diagnoses recorded such as Bell’s palsy or trigeminal neuralgia could reflect missed opportunities for diagnosis, the number of such diagnoses was too low to substantially change the findings and those diagnoses were not unique to the MS cohort. Third, the age of MS onset in our cohorts was similar to findings in clinical cohorts.19,20
The MS cohort had elevated rates of visits to psychiatrists up to 12 years, and consistently from 6 years, before the index date. This raises the question as to whether psychiatric illness is a risk factor or a prodromal factor for MS. A Mendelian randomization study found that depression was not a risk factor for MS. However, the incidence of psychiatric illness is elevated 5–10 years before typical onset of MS in adult cohorts21,22 and in cohorts with inflammatory bowel disease and rheumatoid arthritis. Since higher genetic burden confers an increased incidence of depression and anxiety in MS,23,24 psychiatric illness likely cannot be attributed simply to coping with early signs or symptoms of an undiagnosed disease.
Study strengths include the pediatric population, which is less likely to experience irrelevant health care events and has a low burden of comorbidity, the population-based design, application of a valid case definition to identify pediatric MS, purposeful analysis of data from birth for a subcohort to understand trajectories relative to birth, and the robust nature of the matched design coupled with regression analysis. However, limitations should also be considered. Administrative data may not accurately identify disease onset and diagnosis. However, our sensitivity analyses, imposing a conservative diagnostic delay and excluding individuals < 12 years to account for potential misclassification of some cases of MOGAD, produced similar findings considering the reduced sample size. We cannot exclude residual confounding, and it is difficult to fully disentangle the effects of chronological age and time relative to the MS index date. Finally, the findings may not generalize to other regions with differing payment systems or differing access to care.
Youth with pediatric-onset MS exhibit higher rates of health care use than youth without MS from birth. The perinatal and early childhood periods may be risk periods for MS. A prodromal phase may emerge several years before the onset of typical symptoms of MS, that is, in early childhood/pre-puberty. Further investigation of these periods may elucidate the etiology and early pathobiology of MS.
Supplemental Material
sj-docx-1-msj-10.1177_13524585251338745 – Supplemental material for Health care use preceding pediatric multiple sclerosis: A population-based study from Ontario, Canada
Supplemental material, sj-docx-1-msj-10.1177_13524585251338745 for Health care use preceding pediatric multiple sclerosis: A population-based study from Ontario, Canada by Ruth Ann Marrie, Colleen J Maxwell, Karl Everett, Feng Zhu, Ping Li, Kyla A McKay, Yinshan Zhao and Helen Tremlett in Multiple Sclerosis Journal
Footnotes
Acknowledgements
This document used data adapted from the Statistics Canada Census (1996, 2001, 2006, 2011, 2016) and from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from ©Canada Post Corporation and Statistics Canada. Parts of this material are based on data and/or information compiled and provided by CIHI, the MOH, and Statistics Canada. The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
Authors’ note
Statistical analyses were performed by K.E.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.A.M. receives research funding from CIHR, MS Canada, Crohn’s and Colitis Canada, the National Multiple Sclerosis Society, CMSC, The Arthritis Society, the US Department of Defense, the Public Health Agency of Canada, the UK MS Society, MMSF, and is a co-investigator on studies receiving funding from Biogen Idec, Roche Canada, and the Pfizer Foundation. C.J.M. receives research funding from a University of Waterloo Research Chair, CIHR, MS Canada, National Multiple Sclerosis Society, CMSC, and the Public Health Agency of Canada. K.E. reports no disclosures relevant to the manuscript. F.Z. reports no disclosures relevant to the manuscript. P.L. reports no disclosures relevant to the manuscript. K.A.M. is funded by the Swedish Research Council for Health, Working Life, and Welfare and has received speaker honoraria from Biogen (2022) and Sanofi-Aventis (2023). Y.Z. reports no disclosures relevant to the manuscript. H.T. has received research support from the Canada Research Chair Program, the National Multiple Sclerosis Society, the Canadian Institutes of Health Research, MS Canada, the Multiple Sclerosis Scientific Research Foundation, and the EDMUS Foundation (“Fondation EDMUS contre la sclérose en plaques”); has had travel expenses or registration fees prepaid or reimbursed to present at CME conferences or attend meetings (as a member of the International Advisory Committee on Clinical Trials in Multiple Sclerosis) from the Consortium of MS Centers (2023), the Canadian Neurological Sciences Federation (2023), the National MS Society (2022, 2023, 2024), ECTRIMS/ACTRIMS (2017–2024), American Academy of Neurology (2019); and speaker honoraria are either declined or donated to an MS charity or to an unrestricted grant for use by HT’s research group.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded in part by the National MS Society and MS Canada (RG5063A4/1/RFA-2103-37392; EGID: P002/903124/3743; PI: H.T.). This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). The study funders had no role in the methods, analyses, writing of the manuscript, or the decision to submit it for publication.
Data availability
The study datasets are held securely in coded form at ICES. Legal data-sharing agreements prohibit ICES from making the dataset publicly available. However, access may be granted to those who meet pre-specified criteria for confidential access, available at ![]() (email
(email
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.