
Abstract
Background:
Mothers with MS face an increased incidence and prevalence of peripartum mental illness as compared to mothers without MS.
Objective:
To determine the factors associated with the risk of peripartum mental illness among mothers with MS.
Methods:
We identified mothers with MS with live births between 2002 and 2019 using linked population-based administrative data from Ontario, Canada. Using validated definitions, we estimated the incidence of mental illness (depression, anxiety, bipolar disorder) from conception through the first post-partum year (peripartum period). We used multivariable Poisson regression to assess the association between age, delivery year, area-level deprivation (Ontario Marginalization Index), disease duration, disability, and comorbidity and incidence of peripartum mental illness.
Results:
Among 1745 mothers with MS, the mean (SD) age at conception was 31.2 (4.8) years. Mothers living in communities that lacked cohesion had increased rates of peripartum depression (incidence rate ratio [IRR] 1.25; 1.11–1.42) and anxiety (IRR 1.20; 1.07–1.33). Elevated MS disability level was associated with elevated peripartum depression rates (IRR 1.51; 1.12–2.04).
Conclusion:
Higher area-level deprivation and disability levels are associated with an increased incidence of peripartum mental illness. These findings may assist clinicians in identifying women with MS who may benefit from peripartum mental health support.
Introduction
Multiple sclerosis (MS) is associated with an increased incidence of psychiatric disorders, including depression, anxiety, and bipolar disorder.1,2 For women, this elevated risk extends into the peripartum period.3–5 Since peripartum mental illness adversely affects the mother and child,6,7 early identification and effective treatment are important to improve outcomes. Prevention would be even more effective.
Effective interventions exist to prevent maternal peripartum depression, 8 but health care providers must know to whom they should be targeted. Yet, risk factors for peripartum mental illness in MS have received little attention,3,9 and may differ from those in the general population. 10 One study reported fatigue and bladder dysfunction were associated with emotional distress at 1 month post-partum but did not consider specific mental illnesses or the full year post-partum. 9 Another small study found that adverse socioeconomic factors were associated with depression in the third trimester. 3
We assessed factors associated with the risk of peripartum mental illness among mothers with MS, hypothesizing that greater area-level deprivation and disability would be associated with an increased incidence of peripartum mental illness.
Methods
Setting
With 14 million residents, Ontario comprises nearly 40% of the Canadian population. 11 Health care is universal and publicly funded for medically necessary services, including hospitalizations and physician visits. Prospectively collected population-based (administrative) health service records are available to researchers; 12 we used these to conduct a retrospective cohort study. The University of Manitoba Health Research Ethics Board approved the study. Analyses were conducted at ICES, an independent, non-profit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement.
Data sources
ICES holds databases derived from health service delivery which can be linked deterministically at the individual level using unique encoded identifiers. Databases (and data elements used) were: the Registered Persons Database (unique identifier, dates of birth and death, sex, region of residence [postal code], and dates of health insurance coverage); Discharge Abstract Database (hospital admission and separation dates, and discharge diagnoses); the Ontario Health Insurance Plan (OHIP, dates of physician claims and one diagnosis); the Ontario Mental Health Reporting System (admissions to adult inpatient mental health beds and discharge diagnoses); 13 National Ambulatory Care Reporting System (NACRS, dates of emergency department visits and diagnoses); the Home Care Database (dates of home care receipt); Continuing Care Reporting System-Long-term Care (admission and discharge dates); National Rehabilitation Reporting System (admission dates to rehabilitation hospitals); the Ontario Drug Benefit Plan (ODB, prescriptions dispensed and location, such as long-term care) and the MOMBABY data set (gestational age at delivery, singleton/multiple birth, and live birth/stillbirth). Postal codes were linked to census data from Statistics Canada. Depending on the year, discharge diagnoses are coded using International Classification of Diseases (ICD)-9 or 10-Canadian modification (CA) codes, while NACRS uses ICD-10-CA codes and OHIP uses 3-digit (modified) ICD-9 codes. ODB is only population-based for persons receiving home care, long-term care or ⩾65 years old. The MOMBABY dataset captures all hospital births; mothers and their newborns have been deterministically linked using the medical chart number since 2002. 14
Study populations
We identified individuals with MS using a validated administrative case definition (positive predictive value 99.5%, negative predictive value 97.5%) 15 that used all available hospital and physician claims for the period 1 April 1988 and 31 December 2020. Individuals had to accumulate ⩾3 diagnostic encounters with an ICD-9/ICD-10-CA code for MS (340/G35). For all individuals, we designated the earliest ICD-9 or 10-CA code for demyelinating disease as the diagnosis date. 15 We linked the MS cohort to the MOMBABY dataset to select mothers with a delivery date (birth) between 1 January 2002 to 31 March 2019, then chose their first pregnancy in that interval. Consistent with our prior work, 5 the index date was 365 days before the estimated conception date. We subtracted gestational age from the newborn’s date of birth to determine conception date. We applied the following exclusions: (1) index date before 1 January 2000 or after 31 March 2017; (2) mother with invalid registration number; (3) newborn with invalid registration number; (4) non-resident in the province and ineligible for provincial health insurance for ⩾12 months before the index date; (5) missing sex; (6) <15 years old or >49 years at conception date; (7) died before the delivery date; or (8) birth <22 weeks gestational age (Supplementary Figure e1).
Study period
Index dates ranged from 1 January 2000 to the 31 March 2017 to provide a 1-year lookback period at the index date and 3-year follow-up period after delivery. Thus, the maximum observation period comprised the 1-year lookback period, the pre-pregnancy year, pregnancy (prenatal period) and years 1–3 post-delivery (post-partum). For comparability to the literature, we examined mental illness during the prenatal and first-year post-partum period combined (hereinafter referred to as “peripartum” period).
Incident peripartum mental illness
As previously described, 5 we identified depression, anxiety and bipolar disorder using validated case definitions (Supplementary Tables e1 & e2). We included sensitive definitions relying on one encounter with a diagnostic code for the illness (depression, bipolar disorder), and specific definitions relying on multiple encounters (depression, anxiety, bipolar disorder). To identify incident mental illness in the peripartum period, the mother could not have any diagnosis codes for the mental illness of interest for 2 years before conception. The two-year window reflected prior work showing that the median time between depression claims was 24.0 (36.0–121.0) days; the 99th percentile of the distribution was 497 days. 16 We focused on incident, rather than prevalent, mental illness because of our interest in prevention.
Characteristics of interest
At the index date we captured maternal social determinants of health based on the one-year lookback period. These included the Ontario Marginalization Index, urban/rural residence, and health care use. The Ontario Marginalization Index is an area-based measure of marginalization at the level of dissemination areas and census tracts, using Statistics Canada data. 17 It includes four factor scores constructed using principal component analysis, labeled as households-dwellings, racialized-newcomer populations, age-labor force, and material resources. Each score has a mean of zero and standard deviation of one; higher scores indicate more marginalized areas. 17 The households and dwellings score relates to family and neighborhood stability and cohesiveness, where cohesive communities are thought to be socially supportive environments. Racialized and newcomer populations relates to proportions of individuals in the area who are recent immigrants or belong to racialized groups based on race, ethnicity, language, religion, or culture. Age and labor force reflects the area-level concentration of individuals who lack income from employment because of age (children, older adults), uncompensated work, or inability to work due to disability. The material resources score reflects poverty and captures the inability to attain material needs related to food, housing, clothing and education. Residence in census metropolitan areas with populations of ⩾100,000 was classified as urban. Health care use was summarized as the annual number of physician visits at the index date. Access to prenatal care was summarized as use of prenatal ultrasound (present/absent) and number of prenatal visits for obstetrics reasons whether to primary care providers or obstetricians.
Maternal disease characteristics at index included disease duration, based on disease diagnosis date. Disability status was measured at conception using a validated regression equation that incorporated age, home care and long-term care use, admission for rehabilitation, and symptoms of spasticity and paraparesis; 18 like the Expanded Disability Status Scale score against which this algorithm was validated, 0 indicates no disability, and 3 indicates moderate disability. We categorized disability status as <3 versus ⩾3 to identify mothers with moderate or greater disability.
We captured maternal pregnancy-related characteristics including age at conception, delivery year, multiple birth (yes/no), and maternal comorbidity at conception. Comorbidity was assessed using the Obstetric Comorbidity Index, 19 a weighted index associated with maternal morbidity. We modified the index to exclude alcohol and drug abuse, since substance use is highly comorbid with the other mental illness outcomes of interest and categorized it as 0 vs ⩾1 to address small cell sizes. The number of mothers affected (n = 14) precluded using substance use as a separate covariate. We measured domestic assault requiring emergent care in the year before conception based on at least one presentation to emergency departments with ICD-10 diagnosis codes for maltreatment (T74), neglect and abandonment (Y06), or other maltreatment by spouse/parent/friend/other person (Y07.0-Y07.2, Y07.8-Y07.9). Maternal complications were identified using ICD-9/10-CA codes and included placental abruption, premature rupture of membranes, pre-gestational hypertension, preeclampsia and eclampsia, pre-gestational diabetes, gestational diabetes, maternal infection and chorioamnionitis (Supplementary Table e3). These were combined into a single variable indicating the occurrence of any maternal complication.
Other covariates
We categorized delivery year as 2002–2009 versus 2010–2019 based on length of the study period and achieving reasonable cell sizes for all outcomes. This factor was included to account for temporal trends, not as a clinical predictor.
Analysis
Using descriptive statistics, including means (standard deviations [SD]), median (interquartile range [IQR]), and frequency (percent), we summarized cohort characteristics. We used bivariate analyses to compare mothers with and without moderate disability, and with and without incident depression, anxiety and bipolar disorder in the peripartum period using standardized differences. We used incidence rate ratios (IRR) and 95% confidence intervals (95%CI) to compare incidence rates for mental illness stratified by disability status, given the association of disability and peripartum mental illness in the general population; 20 overall rates of mental illness have been reported elsewhere. 5
To test the association between the potential risk factors of interest and the mental illness outcomes of depression and anxiety during the peripartum period, we used multivariable Poisson regression. We included the natural log of the population as the model offset and scaled the deviance. Independent variables included age at conception (continuous since testing did not suggest non-linearity), delivery year (2002–2009 [reference]), prior birth, 4 dimensions of the Ontario Marginalization Index (continuous variables), disease duration, obstetric comorbidity index at conception (0 as reference), and disability at conception (<3 as reference). We were unable to include substance use, urban residence or domestic violence as covariates due to small numbers and similarly could not model risk factors for bipolar disorder. We report adjusted incidence rate ratios (RR) and 95% CI.
Complementary analysis
First, we repeated the analyses excluding mothers with any comorbidity given the small number affected. Second, we extended the observation interval and added pregnancy period (prenatal, post-natal years 1, 2 and 3) to the regression models given differences in incidence rates over those time periods observed previously. 5 We tested whether disability modified the association between pregnancy period and incidence of mental illness using an interaction term.
Statistical analyses used SAS V9.4 (SAS Institute Inc., Cary, NC).
Results
We included 1745 mothers with MS (Table 1), two-thirds of whom were aged 25–34 years at conception. Most had singleton births and lived in urban areas. The burden of comorbidity as measured by the obstetric comorbidity index was low. Nearly 15% (257/1745) of mothers had a disability score of ⩾3; they were more likely to have a more recent delivery year and reside in areas with greater deprivation based on the material resources and racialized-newcomer population scores.
Characteristics of the study population.
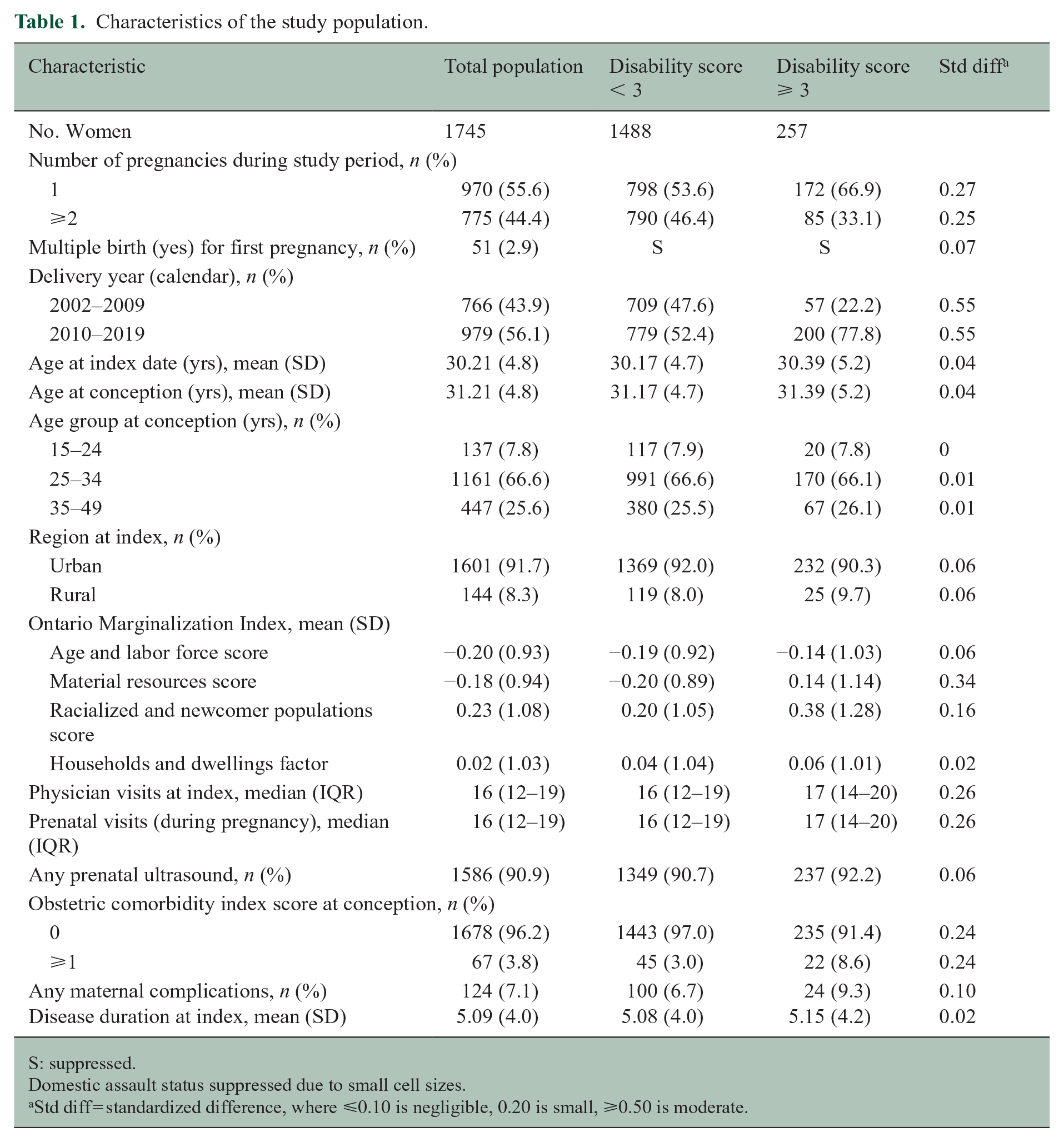
S: suppressed.
Domestic assault status suppressed due to small cell sizes.
Std diff = standardized difference, where ⩽0.10 is negligible, 0.20 is small, ⩾0.50 is moderate.
Disability status and mental illness
During the peripartum period, greater disability was associated with an elevated incidence of depression (both definitions), but not with anxiety or bipolar disorder (Supplementary Table e4).
On bivariate analysis several factors other than disability were associated with depression (sensitive definition) during the peripartum period including having higher average deprivation scores with households-dwellings, and higher health care use (Table 2). Being aged 25–34 was associated with a lower incidence of anxiety than the other age groups whereas a higher households-dwellings deprivation score was associated with a higher incidence (Table 2). Mothers with incident bipolar disorder during the peripartum period were younger and had worse deprivation scores and higher health care use (Supplementary Table e5).
Characteristics of mothers with and without incident mental illness during the peripartum period.
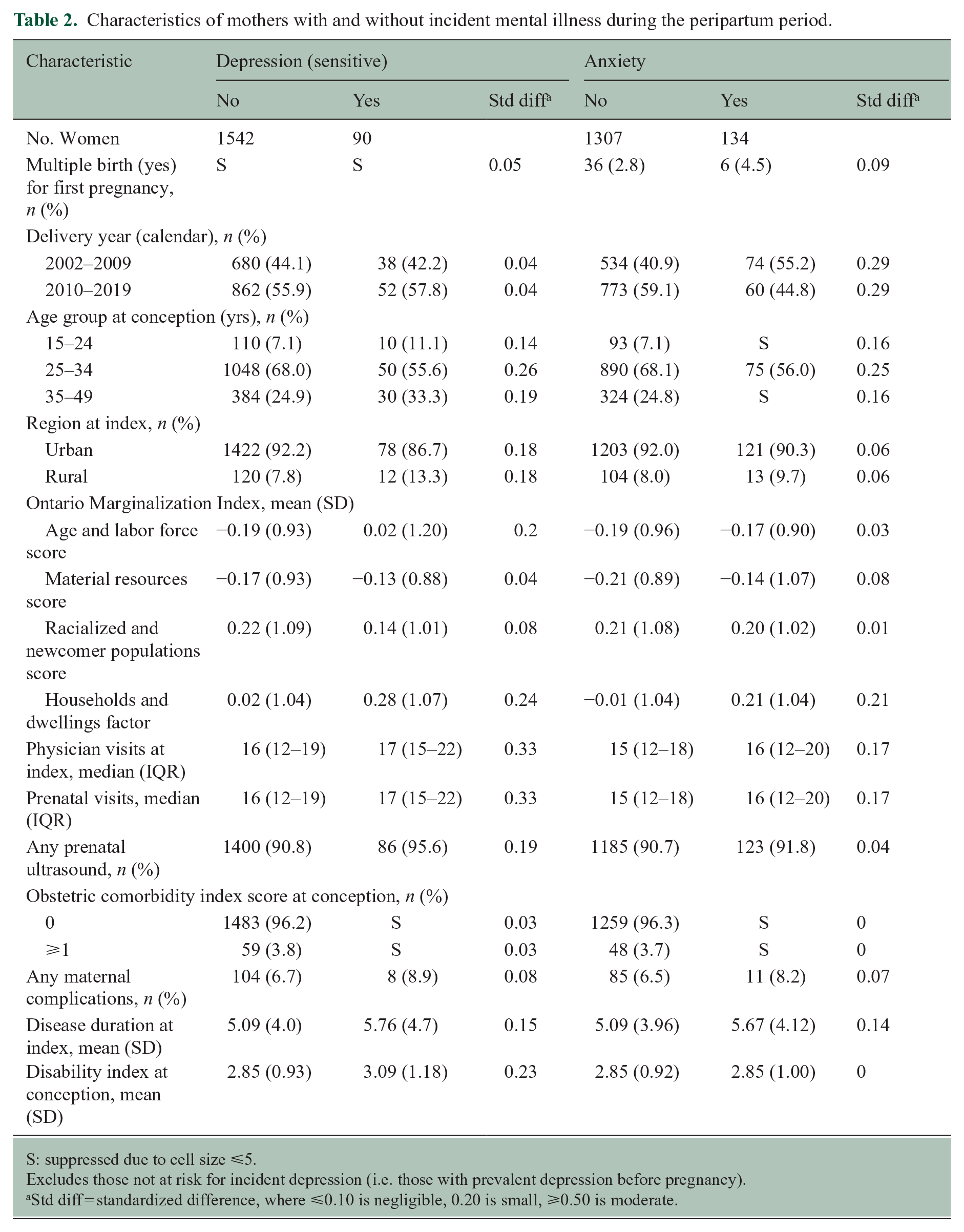
S: suppressed due to cell size ⩽5.
Excludes those not at risk for incident depression (i.e. those with prevalent depression before pregnancy).
Std diff = standardized difference, where ⩽0.10 is negligible, 0.20 is small, ⩾0.50 is moderate.
Multivariable analysis
When we examined factors associated with rates of incident mental illness during the peripartum period, age was not associated with rates of mental illness (Table 3). Later delivery year was associated with lower rates of anxiety disorder. Greater deprivation with respect to households-dwellings was associated with elevated rates of depression and anxiety. Greater deprivation with respect to racialized-newcomer populations was associated with lower rates of depression (specific definition). Elevated disability was associated with elevated rates of depression (sensitive definition) and longer disease duration was associated with elevated rates of depression and anxiety.
Adjusted incidence rate ratios (95% confidence intervals) for factors associated with incidence of mental illness during the peripartum period.
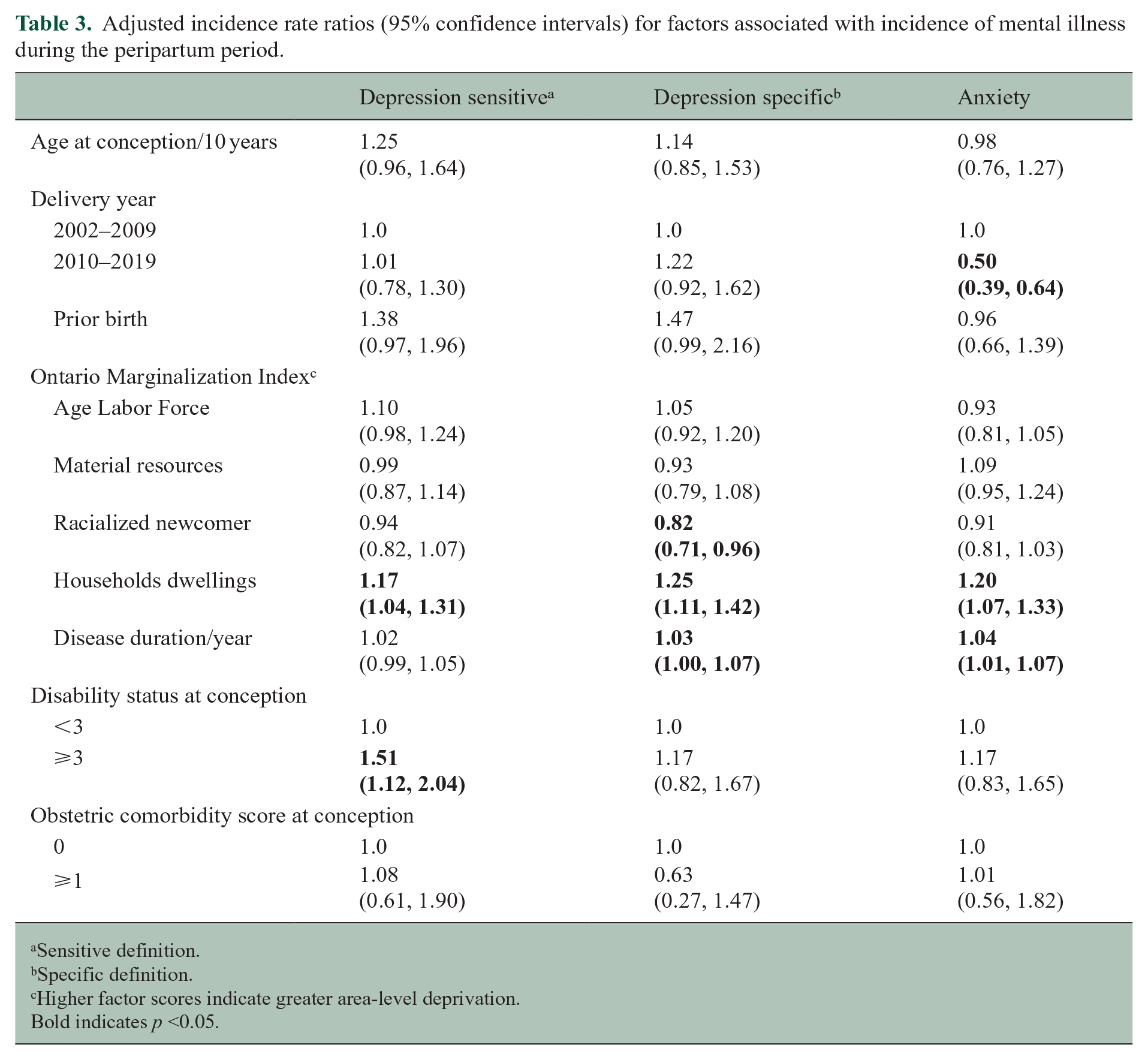
Sensitive definition.
Specific definition.
Higher factor scores indicate greater area-level deprivation.
Bold indicates p <0.05.
Complementary analyses
Findings were relatively unchanged when we repeated the analyses removing mothers with any obstetric comorbidity (Supplementary Table e6). When we adjusted for pregnancy period (i.e. post-partum year 1, 2, and 3 vs prenatal), findings were similar with respect to age, delivery year, two of the deprivation measures (racialized-newcomer deprivation, and households-dwellings), disease duration, and disability (Supplementary Table e7). In contrast, prior birth was associated with higher depression and anxiety rates. Increased material resource deprivation was associated with higher rates of depression (specific definition) and anxiety.
Compared to the prenatal period, the first post-partum year was a higher risk period for depression (both definitions) but not anxiety. In post-partum years 2 and 3 findings for depression were not consistent across the two definitions, but the incidence of anxiety was lower than in the prenatal period.
We did not observe interactions between pregnancy period and disability status on incidence of mental illness.
Discussion
In this population-based cohort study involving >1700 mothers with MS we examined factors associated with an elevated incidence of peripartum mental illness. We found that greater area-level deprivation with respect to households-dwellings was associated with higher rates of depression and anxiety, whereas the opposite finding was observed for deprivation with respect to racialized-newcomers. A higher disability level score was associated with elevated peripartum depression rates. Findings were similar when we included a variable indicating the interval of the peripartum period (prenatal, post-partum year). The first post-partum year was a higher risk period than the prenatal period for depression, but for anxiety disorders the highest risk period was prenatal.
We found that higher disability levels were associated with an elevated incidence of depression during the peripartum period, but not anxiety disorders. Two prior studies among mothers with MS found that disability was not associated with prevalent peripartum depression.3,21 Among 140 mothers with MS, receiving disability benefits was not associated with prevalent depressive symptoms in the third trimester of pregnancy. 3 In a single center study of 143 births to 111 women with MS, disability was not associated with prevalent post-partum depression, 21 but 75% of mothers had an EDSS ⩽ 2.5. Our findings align with those from the US Pregnancy Risk Assessment Monitoring System which found that mothers with any physical disability had a two-fold increased frequency of post-partum depressive symptoms. 20 Qualitative studies of mothers living with physical disabilities have reported barriers to pregnancy and post-partum care related to physical accessibility needs, gaps in clinician knowledge regarding their conditions and the effects on pregnancy, and the lack of tailored information regarding pregnancy and post-partum supports. 22 These findings also appear relevant to mothers with MS.
In a study of 140 mothers with MS, adverse socioeconomic factors were associated with an increased risk of prevalent depression in the third trimester of pregnancy. 3 Based on area-level deprivation measures, we found that mothers living in communities that lack cohesion (households-dwellings) were at elevated risk of incident depression and anxiety. In the US Pregnancy Risk Assessment Monitoring System, lower levels of maternal education, lower income, and public insurance were associated with an increased risk of post-partum depressive symptoms. 20 While not consistent across both depression definitions, greater deprivation on the racialized-newcomer index was associated with a lower risk of depression. Though this finding could be interpreted as reflecting a healthy migrant effect, 23 this association may reflect important barriers to healthcare. A qualitative study of 30 pregnant or post-partum women reported multiple barriers to peripartum depression treatment for racialized women including culturally-specific stigma, low social support, difficulty getting time away from work for treatment, and prior trauma. 24 In the US Pregnancy Risk Assessment Monitoring System, identifying as Black, Asian or Other/Mixed is associated with an increased risk of post-partum depression as compared to identifying as White. In the United Kingdom, racialized women recommended that perinatal teams support them to strengthen community networks, ask about cultural values, support them to understand the intersection of culture and mental health, and culturally tailor interventions. 25
Strengths of this study included the population-based design and use of validated approaches to identify the population and outcomes. However, misclassification may occur even if validated definitions are used. Administrative data can only identify conditions for which health care is sought. We cannot exclude the possibility that some cases of incident mental illness represented recurrent disorders. Although our sample included all hospital births to mothers with MS in Ontario, it was not large enough to support analyses testing whether maternal or neonatal complications mediated the risk of peripartum mental illness. We lacked detailed clinical information about MS or mental illness and related treatments, although we applied a validated measure of disability developed for use in administrative datasets. We also could not assess the role of substance use. We used area-based measures of marginalization, but these measures do not capture all aspects of marginalization and may not classify all individuals in an area correctly. Domestic violence rates were too low to examine. Because of the focus on incident mental illness, we could not examine whether prior mental illness influenced the risk of active/recurrent mental illness during the peripartum period. We did not compare risk factors for peripartum mental illness between mothers with and without MS; this should be the subject of future work.
For the clinician, our findings can be used to guide care for women contemplating pregnancy, or already pregnant. Mothers with MS who have adverse socioeconomic circumstances and disability are at particularly increased risk of incident mental illness in the peripartum period. Screening during pregnancy and post-partum can be done effectively with the Edinburgh Perinatal Depression Scale, or with the Patient Health Questionnaire-9. 26 Importantly, counseling interventions reduce the risk of peripartum depression, 8 and our findings may help clinicians, including MS care providers, to identify mothers at highest risk of incident peripartum depression and most in need of preventive interventions.
Supplemental Material
sj-docx-1-msj-10.1177_13524585251330109 – Supplemental material for Risk factors for incident peripartum mental illness in multiple sclerosis
Supplemental material, sj-docx-1-msj-10.1177_13524585251330109 for Risk factors for incident peripartum mental illness in multiple sclerosis by Ruth Ann Marrie, James M Bolton, Vicki Ling, Charles N Bernstein, Kristen M Krysko, Ping Li, Kyla A McKay, Neda Razaz, Dalia L Rotstein, Karma Deakin-Harb and Colleen Maxwell in Multiple Sclerosis Journal
Footnotes
Acknowledgements
This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from ©Canada Post Corporation and Statistics Canada. Parts of this material are based on data and/or information compiled and provided by CIHI, and the MOH. Parts of this material are based on data adapted from Statistics Canada, Census, 2021. We thank IQVIA Solutions Canada Inc. for use of their Drug Information File. We thank the Toronto Community Health Profiles Partnership for providing access to the Ontario Marginalization Index. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
Authors’ Note
Statistical analyses were performed by Vicki Ling.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.A. Marrie receives research funding from: CIHR, MS Canada, Crohn’s and Colitis Canada, National Multiple Sclerosis Society, CMSC, the Arthritis Society, Pfizer Foundation, Public Health Agency of Canada and the US Department of Defense and is a co-investigator on studies receiving funding from Biogen Idec, Roche Canada. She holds the Multiple Sclerosis Clinical Research Chair (Dalhousie University). J.M. Bolton receives research funding from MS Canada, and the Ruth Hurd Professorship. V. Ling reports no disclosures relevant to the manuscript. C. Bernstein is supported by the Bingham Chair in Gastroenterology. CB has served on advisory Boards for AbbVie Canada, Amgen Canada, Bristol Myers Squibb Canada, Eli Lilly Canada, Ferring Canada, Innomar Pharmacy, JAMP Pharmaceuticals, Janssen Canada, Pendopharm Canada, Sandoz Canada, Takeda Canada, and Pfizer Canada; Educational grants from Abbvie Canada, Boston Scientific, Eli Lilly Canada, Fresenius Kabi Canada, Ferring Canada, Organon Canada, Pfizer Canada, Takeda Canada, and Janssen Canada. Speaker’s panel for Abbvie Canada, Janssen Canada, Pfizer Canada, and Takeda Canada. Received research funding from Abbvie Canada, Takeda Canada and Pfizer Canada. K.M. Krysko has received grants from MS Canada and the University of Toronto Division of Neurology; a contract for a study site from Roche; speaking or consulting fees from Biogen, EMD Serono, Novartis, Roche; advisory board member for Biogen, EMD Serono, Novartis, Roche; scientific advisory committee member for Bristol-Myers Squibb. K.A. McKay receives research funding from the Karolinska Institutet, the Swedish Research Council, and Bjarne Ahlström’s Foundation and has received speaker honoraria from Biogen Inc and Sanofi. N. Razaz receives funding from the Swedish Research Council. D. Rotstein receives research funding from MS Canada, the National MS Society, the Consortium of Multiple Sclerosis Centers, the University of Toronto Division of Neurology and Roche Canada. She has received consulting or speaker fees from Alexion, Amgen, Biogen, EMD Serono, Novartis, Roche, Sanofi Aventis and Touch International Medical Education. K. Deakin-Harb reports no disclosures relevant to the manuscript. C. J. Maxwell receives funding from CIHR, MS Canada, National Multiple Sclerosis Society, the Public Health Agency of Canada, and the Alzheimer Society of Canada.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by MS Canada (EGID 903015).
Data Availability
The dataset from this study is held securely in coded form at ICES. Legal data sharing agreements prohibit ICES from making the dataset publicly available. However, access may be granted to those who meet pre-specified criteria for confidential access, available at ![]() (email
(email
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.