
Abstract
Background:
Although often overlooked, patient and public involvement (PPI) is vital when considering the design and delivery of complex and adaptive clinical trial designs for chronic health conditions such as multiple sclerosis (MS).
Methods:
We conducted a rapid review to assess current status of PPI in the design and conduct of clinical trials in MS over the last 5 years. We provide a case study describing PPI in the development of a platform clinical trial in progressive MS.
Results:
We identified only eight unique clinical trials that described PPI as part of articles or protocols; nearly, all were linked with funders who encourage or mandate PPI in health research. The OCTOPUS trial was co-designed with people affected by MS. They were central to every aspect from forming part of a governance group shaping the direction and strategy, to the working groups for treatment selection, trial design and delivery. They led the PPI strategy which enabled a more accessible, acceptable and inclusive design.
Conclusion:
Active, meaningful PPI in clinical trial design increases the quality and relevance of studies and the likelihood of impact for the patient community. We offer recommendations for enhancing PPI in future MS clinical trials.
Introduction
Interest is growing in patient and public involvement (PPI) in health research in regions around the world, often supported by specific organizations or research frameworks, 1 although the terminology used differs. For example, in Canada, the Canadian Institutes for Health Research lead the development of the Strategy for Patient-Oriented Research. This strategy refers to “patient engagement” in research, whereas in the United Kingdom, the term PPI is used to indicate active inclusion of patients, their families and caregivers, or the lay public as research partners or representatives throughout the research process. In the rehabilitation literature, the term “participatory action research” is used, 2 while the US-based organization, the Agency for Healthcare Research has referred to community-based participatory research. The slogan “nothing about us without us,” a motto ascribed to the disability rights movement, 3 is sometimes used to highlight a key rationale for PPI in research. That is, people living with or affected by (i.e. family members or caregivers) a condition, such as multiple sclerosis (MS), have a right to be involved in research regarding their condition because they will receive the findings of the health research. Moreover, PPI improves the relevance of the research and enhances accountability. For this article, we will use the term people affected by multiple sclerosis (paMS) to be inclusive of people living with and affected by the condition.
Patients, caregivers, and the general public may be engaged throughout all clinical trial stages including setting of priorities, study design, recruitment, and dissemination and implementation of the findings; this has several potential benefits.4 –6 A systematic review of 26 studies found that PPI increased the odds of participant enrollment by 16% (odds ratio (OR) = 1.16; 1.10–1.34). 7 An examination of the value of PPI using financial modeling techniques that accounted for time, cost, revenue, and risk suggested substantial financial benefits. 8 Specifically, if PPI was incorporated into a pre-phase 2 project, and led to avoiding one protocol amendment as well as improved enrollment, adherence, and retention, then a $100,000 involvement activity would provide at least a 500-fold return on investment. 8
In December 2022, an international group of investigators in MS, epidemiology, biostatistics, rehabilitation and clinical trials, and people with MS met under the auspices of the International Advisory Committee on Clinical Trials in MS, sponsored by the European Committee on Treatment and Research in MS and the US National MS Society (for attendees, see Supplemental Appendix I). One of the workshop goals was to discuss strategies to enhance involvement of paMS in clinical trial design. Herein, we: (1) briefly review the current status of PPI in the design and conduct of clinical trials in MS, (2) provide a case study of PPI in the OCTOPUS platform, and (3) and offer recommendations for enhancing PPI in future MS clinical trials.
Current status of PPI in MS trials
In preparation for the workshop, we conducted a rapid review, 9 rather than a definite, comprehensive systematic review to gain insight into the use of PPI in clinical trials in MS in the last 5 years (for details regarding methods, see Supplemental Appendix II). The search identified 44 articles, of which 43 articles were retrieved successfully (Supplemental Appendix II). Of these, nine described clinical trials or constituted clinical trial protocols,10 –18 two of which referred to the same trial.16,17 Seven were conducted in the United States, at least in part. Notably, of the eight unique studies, six were funded by the Patient-Centered Outcomes Research Institute (PCORI), an organization which mandates stakeholder involvement and a focus on relevance to the end-user. 5 This highlights the key role of funders in encouraging PPI in health research, either by mandating PPI or being unlikely to fund research that does not use it.
The studies varied with respect to the degree of detail reported regarding PPI (Table 1). Most described the general activities which involved paMS and other stakeholders, such as in study design, or development of recruitment strategies. Specific examples of the ways in which that input altered study design or operations were usually not described with one exception. The COMBO-MS trial tested the comparative effectiveness of cognitive behavioral therapy, modafinil, and combination therapy. 12 PaMS as well as clinicians, individuals from advocacy groups, and payers participated in meetings four times per year to provide input into study design and operations. This input resulted in meaningful changes. For example, outcome measures were expanded to add social participation measures. The various stakeholders also provided guidance to the investigators regarding information sharing with study participants, such as providing letters reporting sleep disorder risk.
Clinical trials that reported patient and public involvement in their design and conduct.
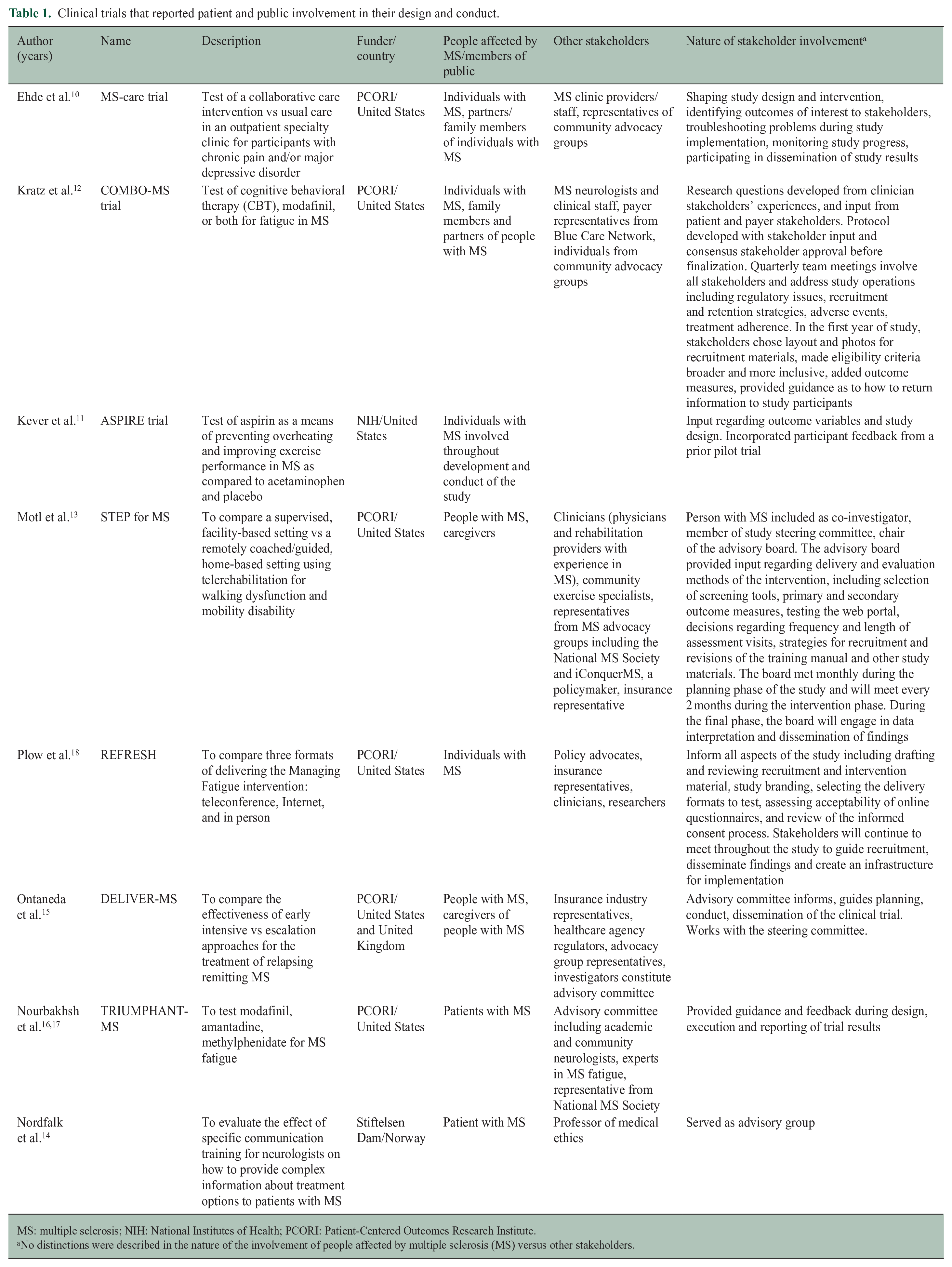
MS: multiple sclerosis; NIH: National Institutes of Health; PCORI: Patient-Centered Outcomes Research Institute.
No distinctions were described in the nature of the involvement of people affected by multiple sclerosis (MS) versus other stakeholders.
This review may have underestimated the degree of PPI in MS clinical trials for several reasons. First, rapid reviews should be interpreted cautiously as they are less comprehensive and seek to answer questions more rapidly than systematic reviews. Ongoing PPI activities will not be in published literature yet or remain in the gray literature. Second, the inconsistent terminology used to describe PPI may reduce the ability to detect all studies that had PPI. Third, PPI may not be reported even when it occurs due to barriers such as journal word limitations, the lack of recommendation to report PPI in the CONSORT statement for clinical trials, and general lack of consensus as to what type of information should be reported and in what format.
Potential approaches for PPI
Multiple methodological strategies can be employed to achieve effective PPI, 6 and within a given study, this can vary by study element. For example, identifying key priorities could involve including patients or caregivers as members of trial steering committees or advisory groups. Alternative strategies include surveys, workshops, or focus groups. This ensures that the questions and outcomes are meaningful to patients and enhances the relevance to clinical practice and policy. Involvement in study design can be achieved through inclusion in the study team, interviews, surveys, focus groups, and choice experiments. For example, surveys and focus groups can be used to identify priorities and framing of research questions during the conceptual phase of trial development. Focus groups can be used to provide insight into potential barriers and facilitators to proposed interventions or feasibility of different dosing regimens (e.g. weekly vs thrice-weekly supervised exercise regimes). When multiple potential interventions are being considered, choice experiments can help to elucidate preferences of potential participants.
Involvement in the design enables the development of interventions that are acceptable to patients and feasible, as well as the selection of outcomes that are important to patients, enhancing future uptake in clinical practice. Patient feedback regarding information provided to potential participants; 19 the consent process and study burden may facilitate recruitment and retention. PPI may be particularly important when devising materials and strategies, such as transportation support, to engage underrepresented groups as discussed further in a companion paper. 20 Patient partners/co-researchers can assist with the development of lay friendly summaries of trial results, presentation of findings to their communities, and post-trial advocacy for implementation of the findings.
Researchers need to be supported as they seek to add PPI to their work. The MULTI-ACT project was funded by the European Commission to enhance the impact of health research for individuals living with brain disorders, via a participatory and anticipatory governance model. 21 MULTI-ACT provides a toolkit of resources to assist with developing appropriate engagement plans. PCORI-funded and other efforts have also created patient engagement toolkits for researchers.22,23 Funding to address the additional expenses to successfully conduct studies with meaningful PPI is also critical.24,25
The characteristics of successful PPI in health research include (1) involvement of people and their caregivers begins as early as possible in the project, so they are involved in conception of the project; (2) involvement is maintained throughout the project; (3) the plan for involvement of patients and caregivers should be well-defined with an articulated purpose, role and structure; (4) orientation and education about PPI in research for researchers and patients; (5) provision of support and recognition for the contributions of patients and caregivers such as reimbursement for time and authorship; and (6) evaluation and reporting of PPI. 1
Because we have focused on PPI we have not discussed the role of other potential stakeholders such as healthcare providers, payers, policymakers, or advocacy organizations extensively. A commentary regarding MULTI-ACT 21 highlights the importance of identifying and involving all relevant stakeholders to enable consideration and integration of a breadth of perspectives and achieving the research goal successfully.
Case study from OCTOPUS: involvement of people affected by MS
Optimal Clinical Trials Platform for Progressive Multiple Sclerosis (OCTOPUS, ISRCTN140448364) is a multi-arm multi-stage (MAMS) adaptive platform trial that aims to accelerate the development of re-purposed or novel treatments to slow or stop the accumulation of disability progression, relative to other clinical trial designs.26,27 In MAMS trials flexibility is planned, such that interventions being tested can change over time, all of which are compared to a common control arm (multi-arm); interventions that appear effective in an early stage can continue on into a later stage (multi-stage). OCTOPUS will incorporate phase 3 evaluations of selected treatments in double-blind, randomized, comparison to standard of care. Adaptive elements incorporated into OCTOPUS include the ability to drop treatment arms at the planned interim stage, based on lack of sufficient activity against pre-specified targets, and the ability to add arms based on the pre-specified process for treatment selection.
The methods, benefits and challenges of PPI in clinical trial design are well-established.4 –6 Although PPI in the design of MAMS trials presents new challenges, it is more important for their success. MAMS trials are more complex in design and less familiar to the general public. Therefore, careful communication is needed to support participant recruitment and retention. PaMS have been involved in co-designing OCTOPUS from the early planning stages through to the ongoing management. Multiple methods have been used to ensure paMS could provide input regarding different aspects of the trial and in a variety of ways.
Methods of involvement
In 2018, the MS Society (the United Kingdom) established an Expert Consortium for progression in MS clinical trials composed of clinicians, clinical trial methodologists and statisticians, basic scientists, healthcare professionals internal and external to the MS research community, and paMS (recruited from the MS Society’s Research Network, MSRN). 28 Its objective was to design all the components of an efficient clinical trials platform for progression in MS, including infrastructure, methodology, and treatment selection that would form a program grant application to the MS Society for funding. All Expert Consortium members were equal partners and had to agree to a Charter of behavior, defined objectives, and timelines.
Initially, six paMS from MSRN joined the Governance Group (leading the direction and strategy of the Expert Consortium), the Treatment Selection Group, and the Trial Design and Delivery Group. The Trial Design and Delivery Group was further split into three working groups: (1) design, (2) outcomes, and (3) infrastructure (Figure 1). Each of these groups had paMS in their core membership. Four paMS formed a PPI Strategy Group alongside MS Society staff and a researcher with PPI experience. One of the key deliverables of this group was to determine the PPI needs of all the groups and to organize and lead a series of workshops across the United Kingdom to ensure that the trial design was shaped by a wider group than those involved in the strategy and working groups. All groups, including the PPI Strategy Group, were provided budgets to conduct the foundational work required to meet their objectives.
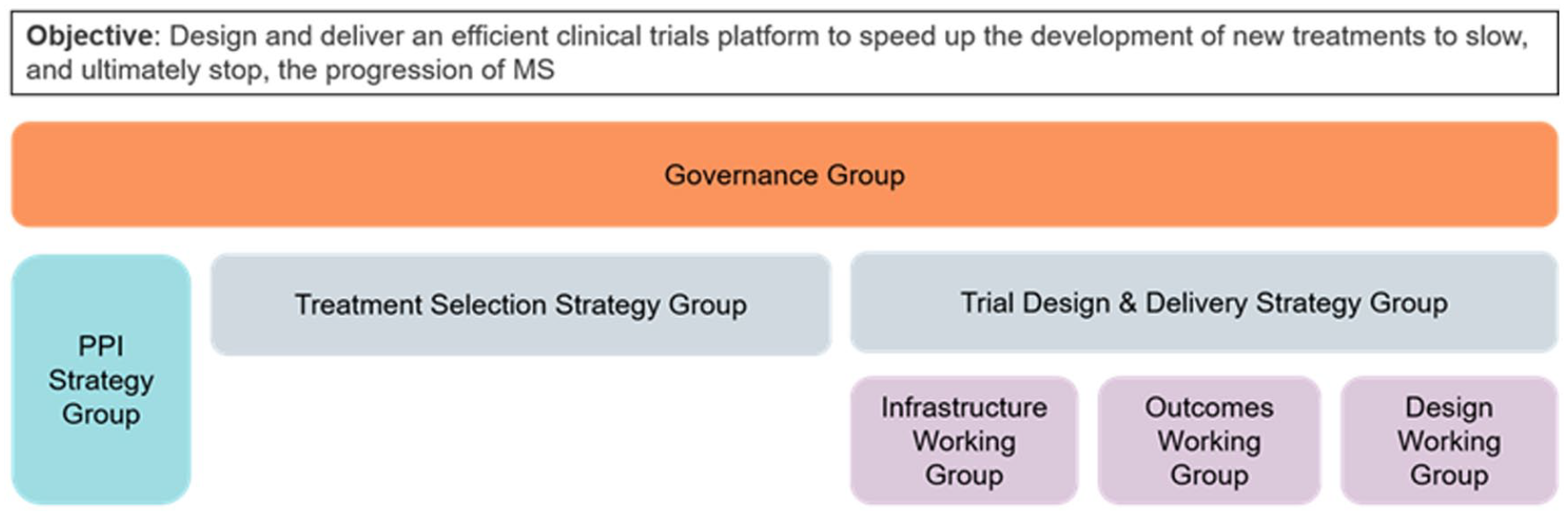
Expert Consortium for progression in MS clinical trials governance structure.
In 2019, the program grant application to the MS Society was written with a person with MS as a co-applicant. Following the awarding of OCTOPUS funding, PPI has continued to play a key role in study design and set up, including paMS on the Trial Management Group and a communication subgroup. A separate PPI Forum was established, to engage paMS who had not been involved to date, widening the diversity of paMS involved. The PPI Forum was available for the trial team to consult with on a required basis about issues arising as OCTOPUS prepared to launch recruitment.
Results of involvement
Involving paMS in the Strategy Groups, Working Groups, and workshops throughout the design process confirmed the need for OCTOPUS in the field of MS. The co-design approach enabled the creation of an inclusive clinical trial design for people experiencing a complex condition.
Treatment Selection
The Treatment Selection Strategy Group established a systematic selection method for shortlisting initial candidate treatments to enter OCTOPUS, and ongoing identification of treatments to be considered as new evidence emerges. 29 The group decided on “Drug CVs” as the method for cataloging and comparing treatments. paMS helped design the templates for the CVs and reviewed patient leaflets for the candidate drugs, extracting key information that would be important to include in the CVs. This ensured the CVs included information that would help paMS contribute to the decision-making.
Multiple Drug CVs were developed and scored by all members of the Treatment Selection Group to create a shortlist. Once the shortlist was established, the group held two panel meetings, which were open to more scientific experts and paMS to maximize the representation of those within the MS community and to alleviate pressure felt by lay members of the group. In these meetings, each drug was presented, discussed, and given an overall score. The scientific members of the committee focused on safety and efficacy. paMS scored each drug, focusing on the ease of administration, tolerability of any adverse effects, safety, and risks. They also considered their willingness to take the drug if it slowed progression of their MS. While the scientific members and paMS focused on different aspects, they scored the drugs using comparable scales ensuring the scores from paMS held as much weight as those from experts and contributed to a spirit of co-production. The comments from paMS on the Drug CVs focused on the acceptability of these drugs, a perspective that would have been missed had they not been involved in the scoring (see Table 2).
Examples of how perspective of people affected by multiple sclerosis influenced shortlisting of OCTOPUS treatment arms.
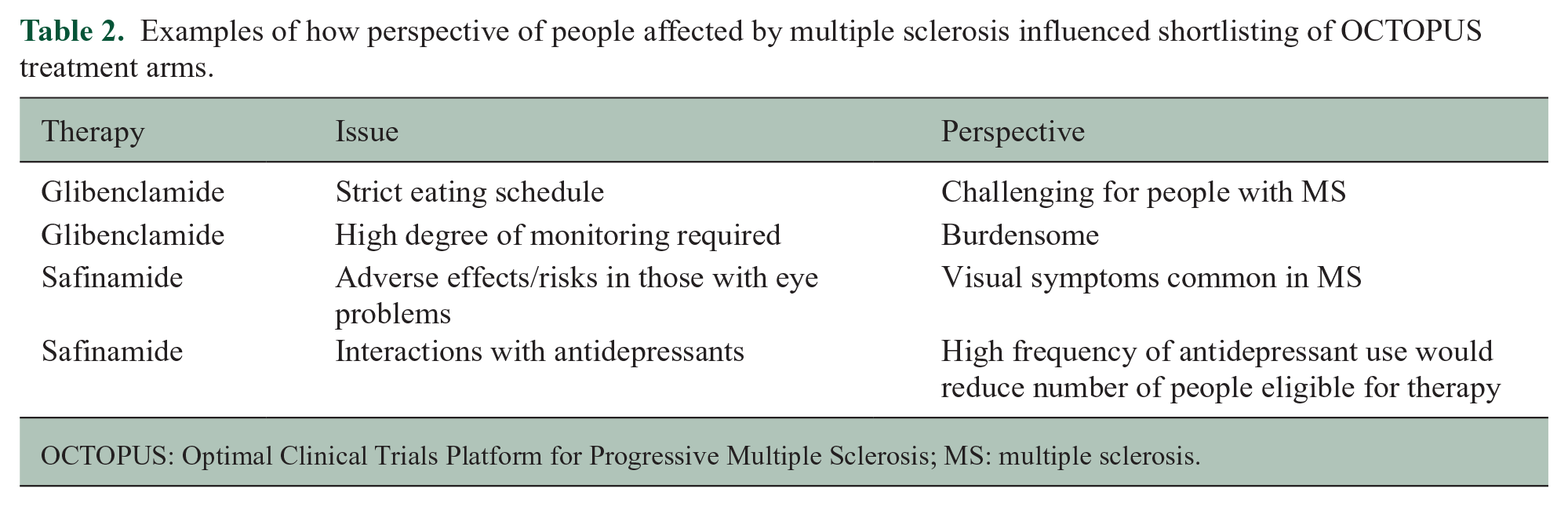
OCTOPUS: Optimal Clinical Trials Platform for Progressive Multiple Sclerosis; MS: multiple sclerosis.
Within the current OCTOPUS governance, an international Treatment Advisory Committee has taken over this area, with paMS at its core. It utilizes Drug CVs and international peer review and has recommended three additional future treatments arms for OCTOPUS.
Trial Design and Delivery
The Trial Design and Delivery Strategy Group focused on trial methodology, outcome measures, and infrastructure in close collaboration with the PPI Strategy Group.
During meetings, paMS raised important considerations about trial design. For example, fairness and access to the trial were highlighted as particularly important, as people with progressive MS often feel left out of the research process. paMS insisted that having trial sites across the United Kingdom and inclusive as possible eligibility criteria were essential. This contributed to the decision for the upper age limit to be higher than most clinical trials and aiming to have a broad distribution of sites across the United Kingdom with the creation of recruitment hubs. These hubs would receive extra funding to boost recruitment in areas where participation in trials could be improved and help build the infrastructure and relationships in different regions, helping people with progressive MS engage with research. paMS also raised how important it is to highlight the benefits of taking part in trials, such as access to nurses for symptom management, receiving standard of care, as well as having an magnetic resonance imaging (MRI) scan. The group discussed these benefits and how best to communicate them with potential participants.
As well as making valuable contributions themselves, as highlighted above, the PPI members of the Trial Design Group felt this topic needed input from a wider group of paMS. To this end, they collaborated with the PPI Strategy Group to host a series of workshops held in Edinburgh, Sheffield, and London. Workshop participants were recruited through the MSRN and via social media to attract a wider audience. The PPI Strategy Group hosted these sessions, with workshops co-presented by MS Society staff and paMS. The paMS who facilitated the discussions felt that their role improved the quality of the conversation, helped to put workshop attendees at ease, and created a more equal power dynamic.
The workshop discussions focused on designing an acceptable trial for paMS and selecting outcome measures they felt would address the key challenges of the condition (e.g. fatigue measures). One specific example they thought would make the trial attractive to paMS was the option for participants to be re-randomized from a non-performing treatment arm to an arm that was shown to demonstrate enough benefit on continue investigation. Workshop participants did not want people to be excluded from taking part in OCTOPUS in the future as a result of being part of an arm that is stopped. Other topics discussed during the workshops included eligibility criteria, engagement strategies (including regular communications via a range of channels), wearable devices, and improving the trial experience for participants.
PPI Forum
Since the late 2020, a PPI Forum was formed to provide additional input into all aspects of OCTOPUS. The group is facilitated by MS Society’s Public Involvement Manager and meets virtually on an ad hoc basis. Any member of the OCTOPUS team can bring topics for discussion to the PPI Forum, where the group can critique suggestions and develop solutions together.
The PPI Forum had several meetings with different members of the OCTOPUS team. Their first meeting was to discuss the acceptability of re-randomization. They felt overall it is a positive aspect of the design but was also important to carefully consider how this information is communicated to potential participants. Specifically, the PPI Forum raised that when people are first recruited, they should be informed that arms may be stopped but that this is not a failure, and that it means more resources can be put into arms that look more promising. Learning your treatment arm is being stopped may be concerning for some and without the right messaging might put people off from continuing to participate; the benefits of taking part in a different arm must be outlined and it must be highlighted that this is voluntary and there is no expectation that someone must continue on a different arm.
They also helped to design the expression of interest online recruitment portal on the UK MS Register, the content of the trial website and even its URL, the participant information sheet and consent form, and other external facing communications.
Lessons learned
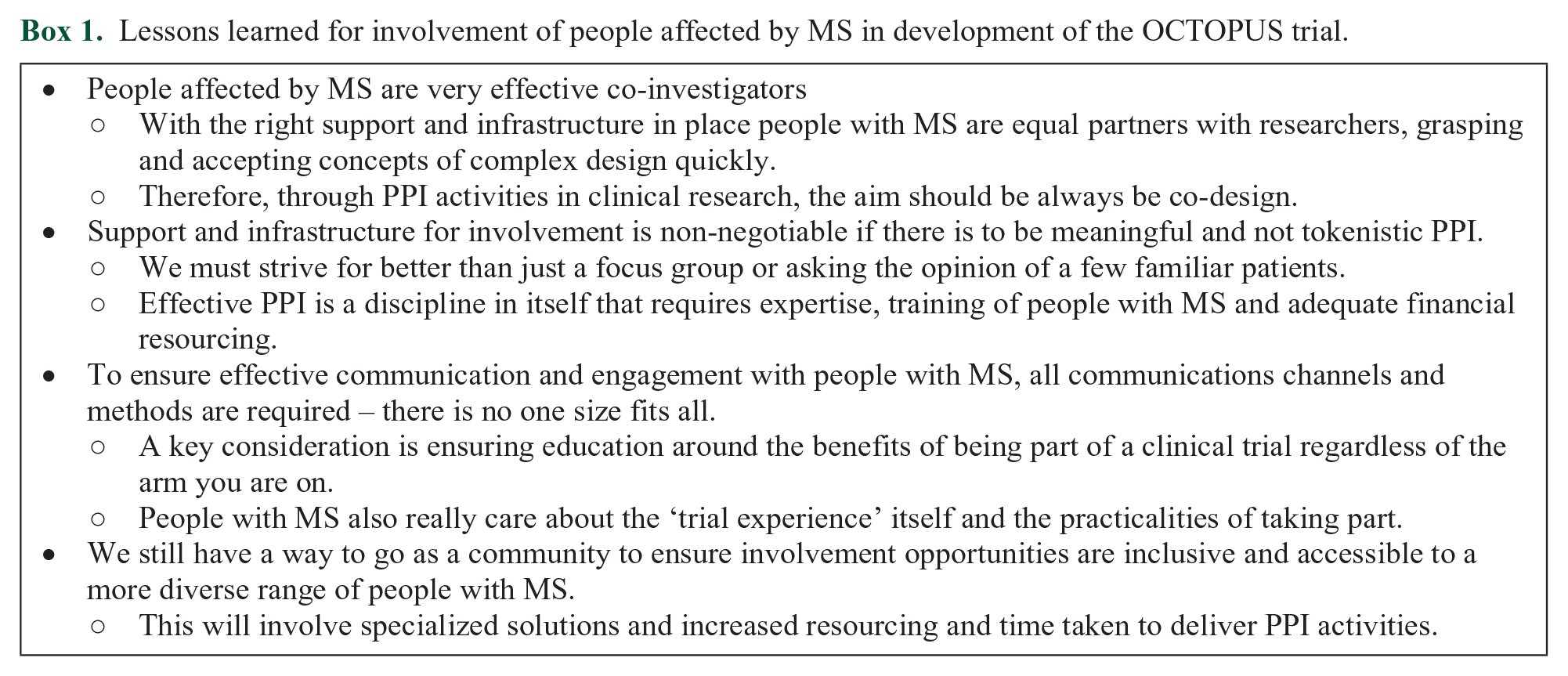
Involving paMS at an early stage has ensured OCTOPUS has been shaped by the lived experience of paMS. OCTOPUS has shown that co-designing a clinical trial is an effective and efficient way of developing a trial that works for members of the public and the research team. This collaborative approach will be continued throughout the lifetime of OCTOPUS. Several lessons and takeaways from this experience are presented to support future involvement of paMS in clinical trial design (Box 1). We still have a way to go as a community to ensure involvement opportunities are inclusive and accessible to a more diverse range of paMS. This will involve specialized solutions and increased resourcing and time taken to deliver PPI activities.
Lessons learned for involvement of people affected by MS in development of the OCTOPUS trial.
Recommendations
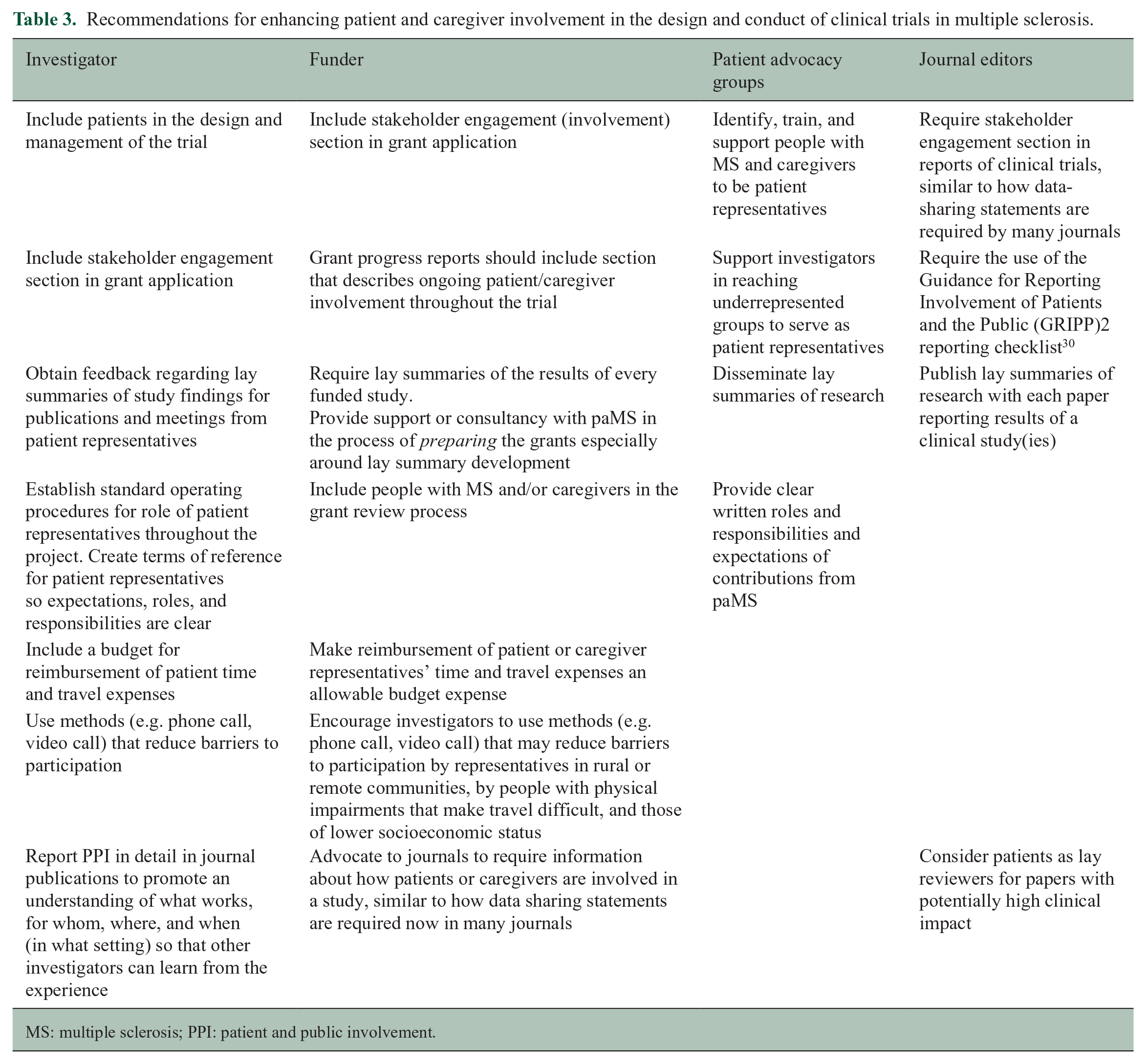
Workshop attendees agreed that paMS should be involved in all aspects of clinical trials in MS, including the trial design and outcome measures, strategies for recruitment and retention of participants, as well as communication including study materials and dissemination of results. Attendees endorsed this as relevant for all clinical trials, regardless of the type of intervention or type of funder. Specific mention was made of the importance of enhancing PPI in clinical trials sponsored by Pharma. Such trials always include a steering committee of professionals who can insist on the inclusion of paMS. Table 3 outlines recommendations to support PPI in clinical trials from the perspective of the investigator, funder, consumer advocacy group, and journal editor; collective action is needed to ensure success.
Recommendations for enhancing patient and caregiver involvement in the design and conduct of clinical trials in multiple sclerosis.
MS: multiple sclerosis; PPI: patient and public involvement.
Conclusion
Despite the knowledge of the benefits of quality PPI in all aspects of clinical trials, there remains an apparent paucity of PPI reported in the design and conduct of clinical trials in MS. This may reflect lack of PPI or lack of reporting PPI or both; methodological issues in our review may also contribute. To highlight the benefit of PPI in trial design, the OCTOPUS trial was described as an example of co-designing a complex trial with paMS, thus creating a more accessible, acceptable, and inclusive design with many lessons learnt along the way. We have offered recommendations for investigators, funders, and patient advocacy groups for enhancing PPI in future MS clinical trials knowing that this requires appropriate expertise, strategy, training, and resourcing for both researchers and paMS. As an international MS research community, PPI in clinical research must become part of the research process without exception if we are to maximize opportunity and impact for people living with and affected by MS.
Supplemental Material
sj-docx-1-msj-10.1177_13524585231189678 – Supplemental material for Enhancing involvement of people with multiple sclerosis in clinical trial design
Supplemental material, sj-docx-1-msj-10.1177_13524585231189678 for Enhancing involvement of people with multiple sclerosis in clinical trial design by Emma Gray, Anneesa Amjad, Jenny Robertson, Judy Beveridge, Susan Scott, Guy Peryer, Marie Braisher, Cheryl Pugh, Sara Peres, Ruth Ann Marrie, Maria Pia Sormani and Jeremy Chataway; in Multiple Sclerosis Journal
Supplemental Material
sj-docx-2-msj-10.1177_13524585231189678 – Supplemental material for Enhancing involvement of people with multiple sclerosis in clinical trial design
Supplemental material, sj-docx-2-msj-10.1177_13524585231189678 for Enhancing involvement of people with multiple sclerosis in clinical trial design by Emma Gray, Anneesa Amjad, Jenny Robertson, Judy Beveridge, Susan Scott, Guy Peryer, Marie Braisher, Cheryl Pugh, Sara Peres, Ruth Ann Marrie, Maria Pia Sormani and Jeremy Chataway; in Multiple Sclerosis Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.A.M. received research funding from Canadian Institutes of Health Research, Research Manitoba, MS Canada, Multiple Sclerosis Scientific Foundation, Crohn’s and Colitis Canada, National Multiple Sclerosis Society, Consortium of MS Centers, the Arthritis Society, and the US Department of Defense. She is supported by the Waugh Family Chair in Multiple Sclerosis. She is a co-investigator on a study funded in part by Biogen Idec and Roche (no funds to her or her institution). In the last 3 years, J.C. has received support from the Efficacy and Evaluation (EME) Programme, a Medical Research Council (MRC) and the National Institute for Health Research (NIHR) partnership and the Health Technology Assessment (HTA) Programme (NIHR), the UK MS Society, the US National MS Society, and the Rosetrees Trust. He is supported in part by the NIHR University College London Hospitals (UCLH) Biomedical Research Centre, London, UK. He has been a local principal investigator for a trial in MS funded by the MS Canada. A local principal investigator for commercial trials funded by Ionis, Novartis, and Roche and has taken part in advisory boards/consultancy for Azadyne, Biogen, Lucid, Janssen, Merck, NervGen, Novartis, and Roche. In the last 3 years, G.P. has worked as an independent contractor with the MS Society (UK) and Bristol-Myers Squibb. M.B. has received support from the NIHR partnership and the HTA Programme (NIHR), the UK MS Society, and the NIHR Local Clinical Network. M.P.S. has received consulting fees from Biogen, Genzyme, GeNeuro, MedDay, Merck, Novartis, Roche, and Teva. E.G., J.R., A.A., S.S., J.B., C.P., and S.P. have nothing to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The International Advisory Committee on Clinical Trials in Multiple Sclerosis and the International Conference on Innovations in Clinical Trial Design & Enhancing Inclusivity of Clinical Trial Populations were supported by the National Multiple Sclerosis Society and the European Committee for Treatment and Research in Multiple Sclerosis. There was no involvement of the sponsors in the design, collection, analysis, or interpretation of data discussed at the Conference. The opinions expressed are those of the authors. Thank you to all members of the Expert Consortium for progression in MS clinical trials including MS Society staff and in particular members of the MS Society Research Network and past and current members of the OCTOPUS PPI Forum. All underpinning work carried out by the Expert Consortium for progression in MS clinical trials were funded by grants from the MS Society (UK). OCTOPUS is funded by grant #135 from the MS Society (UK).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.