
Abstract
Background:
Rehabilitation is an essential health care service and a critical component of comprehensive multiple sclerosis (MS) care.
Objective:
As part of a 2-day meeting hosted by the International Advisory Committee on Clinical Trials in MS in December 2022, a panel initiated a discussion on the conceptual and practical issues related to selecting intermediate outcomes for clinical trials of MS rehabilitation interventions.
Results:
The overarching goal of rehabilitation – optimal functioning – was acknowledged as a complex biopsychosocial phenomenon that varies with patient priorities and environmental context. This complexity means that multiple causal pathways and potential intermediate outcomes must be carefully considered during the design of clinical trials in MS rehabilitation that aim to improve functioning. In addition, practical issues must be considered such as psychometric properties of outcome measures, measure type, and characteristics of the target population, including severity of dysfunction.
Conclusion:
This article uses the International Classification of Functioning, Disability and Health as a foundation for determining relevant intermediate outcomes for clinical trials of MS rehabilitation interventions.
Keywords
Introduction
Rehabilitation is an essential health service and a key strategy to achieving the United Nations Sustainable Development Goal #3: ensuring healthy lives and promoting well-being for all people.
1
As an essential health service, multidisciplinary rehabilitation is critical component of comprehensive MS care, across the spectrum of the disease.
2
In 2022, Cochrane Rehabilitation developed the following definition for research purposes: In a healthcare context, rehabilitation is defined as a multimodal, person-centred, collaborative process including interventions targeting a person’s capacity and/or contextual factors related to performance with the goal of optimising the functioning of persons with health conditions currently experiencing disability or likely to experience disability, or persons with disability.
3
This and previous definitions of rehabilitation4 –6 share several core elements, most notably, an overarching goal of optimising an individual’s functioning, the recognition that functioning occurs in the context of the person’s environment, and that interventions target the person, the environment, or both. Importantly, functioning–not disease–is key in rehabilitation. Of note, functioning has been proposed as a third health indicator for health systems internationally, as important as mortality and morbidity, because it reflects ‘lived health’. 7
Modifying functioning through rehabilitation is a complex process, regardless of the discipline delivering care. For most problems of functioning, there are multiple, plausible causal pathways that link a given intervention to the overarching outcome of optimal functioning. The International Classification of Functioning, Disability and Health (ICF) 8 describes how these pathways may be biological, psychological, social, person-environment, or some combination of these. Even with pathways specified, it is often not feasible to assess the final goal of rehabilitation because it is contextually bound and often requires multiple assessments or interventions over longer time periods. Fortunately, the ICF provides useful scholarly and technical resources for considering potential pathways and selecting intermediate outcome measures for MS rehabilitation trials.9 –12 An intermediate outcome is a replacement endpoint that is believed to assess the way in which an intervention affects the true outcome of interest 13 (i.e. optimal functioning). Although the terminology of intermediate outcomes is familiar in pharmaceutical trials, it is not commonly used in rehabilitation trials. Instead, a rehabilitation researcher is more likely to refer to outcomes as proximal (immediately after the intervention concludes) or distal (ones that take longer to achieve).
Regardless of the terminology used, the concept of a replacement endpoint to capture change towards the true outcome of interest is a shared one. To date, MS rehabilitation trials have generally been characterised by small, often single-site studies of convenient clinical samples using a traditional two-arm trial design. 14 These trials apply one or more standardised interventions to enhance a specific aspect of functioning, while in clinical reality, interventions would be tailored to the patient’s profile and preferences, for example, when addressing MS related fatigue. To support the translation of trial findings into clinical practice, more explicit discussions about causal pathways and intermediate outcomes would be beneficial. These discussions could increase transparency about when an intervention is expected to work best, particularly if it is expected to impact early rather than later phases of a pathway to optimal functioning (e.g. reducing pain severity to improve work productivity). More explicit discussion of intermediate outcomes in MS rehabilitation trials would also support increased collaboration across MS researchers through the use of common language, and enhance trial efficiency through the use of innovative designs. 15
One of the goals of a 2-day meeting hosted by the International Advisory Committee on Clinical Trials in MS in December 2022 was to consider the role of intermediate outcomes, composite outcomes, and differential individual responses across outcomes in supporting efficient trial design and personalised care. 15 This goal was achieved through a series of invited talks, panel presentations, and break-out group discussions. One panel presentation with four speakers (M.F., P.F., U.D., and D.K.) focused specifically on the use and challenges of intermediate outcomes in MS rehabilitation trials, with a break-out group generating possible research strategies to address these challenges. These scholarly discussions formed the foundation for this article (see Supplemental Material for the participant list). As we further considered intermediate outcomes for MS rehabilitation clinical trials, the definition of rehabilitation and the notion that functioning is ‘lived health’ became critically important: both indicate that rehabilitation trials are likely to have a different overarching goal than pharmaceutical ones. Rather than having a primary focus on modifying the biological aspects of disease activity and progression, rehabilitation trials incorporate a focus on changing the experience of living with MS. Change may occur through interventions guided by biological, psychological, social or contextual theories to prevent dysfunction, restore function, compensate for loss of function and/or support adaptation to decline of function. While we fully support the growing interest in whether and how rehabilitation interventions might modify biological aspects of disease activity and progression, especially at earlier disease stages, the focus of this article is on conceptual and practical issues associated with the selection of intermediate outcomes for trials of rehabilitation interventions that are more pragmatic in orientation and seek to optimise functioning and enhance ‘lived health’.
Domains of and contributors to optimal functioning: the ICF
The ICF is part of World Health Organisation’s family of classification systems, and is complementary to the International Classification of Diseases. 12 The ICF offers both a conceptual model 8 and a classification system 16 that can be used to describe human functioning, interventions targeting functioning, and related outcome measures. The ICF model is a biopsychosocial one, and therefore not specific to any particular health problem or disease. The ICF can be used to describe functioning of any person across three domains: body structure and function, activity, and participation. 12 All three domains interact with health conditions (if they are present) and contextual factors, which include environmental and personal. It is important to note that the ICF does not support direct inferences from one domain of functioning to the other due to the complex, dynamic interplay among the model components. 12 Figure 1 depicts the ICF model, and illustrates the application of the classification system using the example of accidental falls.
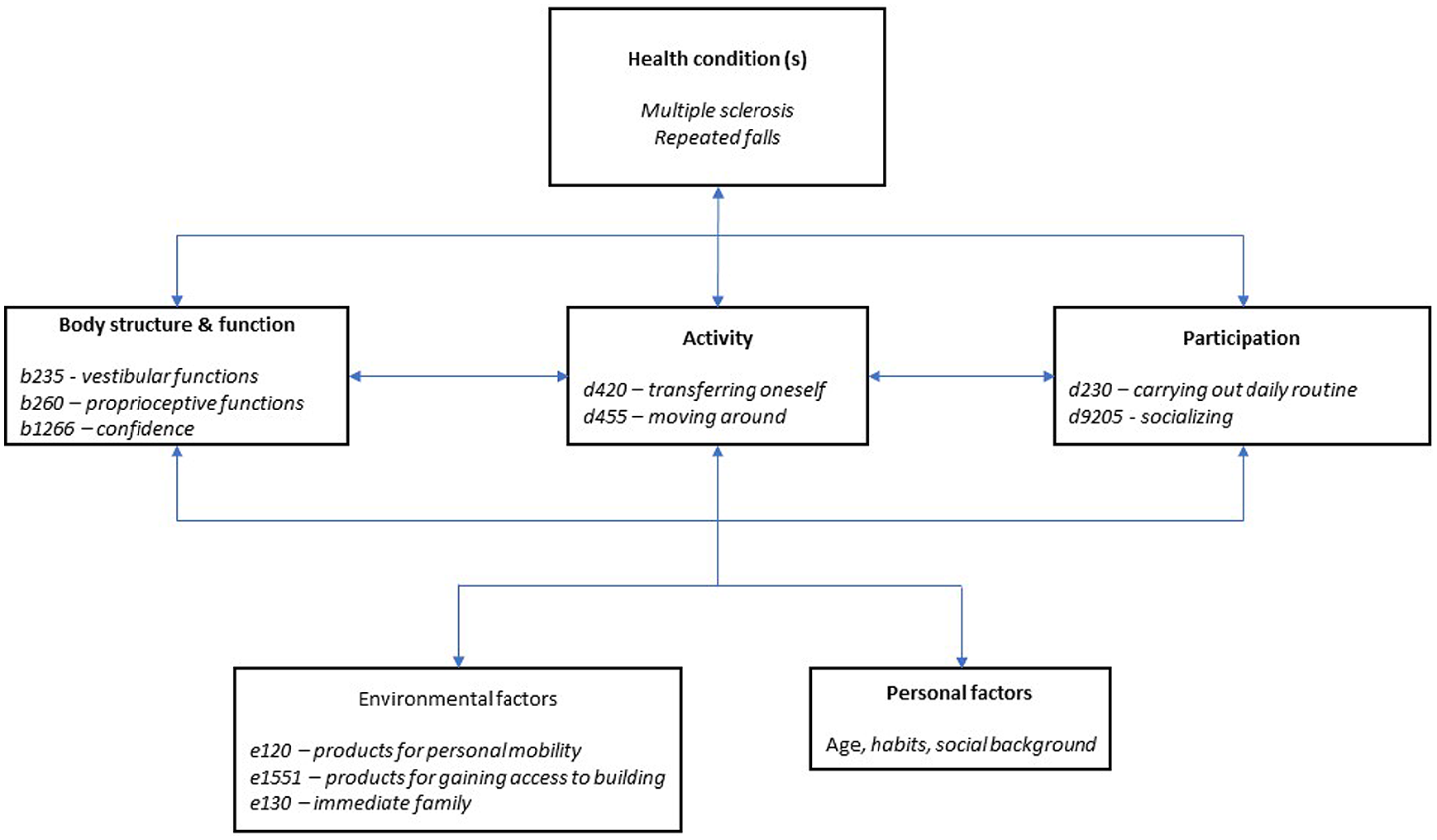
The ICF domains and contextual factors, with a few key examples of codes and names from the ICF browser that are relevant to accidental falls for some people with MS. Examples are not meant to be comprehensive.
When considering intermediate outcomes for MS rehabilitation trials, application of the ICF offers a unified and consistent terminology for human functioning. The online browser for the classification system 16 provides codes (e.g. d430 in the activity domain), names (e.g. lifting) and definitions (e.g. ‘raising up an object in order to move it from a lower to a higher level, such as when lifting a glass from the table’) for specific aspects of functioning and environmental factors. The system is organised hierarchically in different chapters and levels. 16 A specific aspect of functioning can be rated using ICF qualifiers, which are fully described in several technical resources.11,12 Furthermore, aspects of functioning can also be matched to standardised outcome measures using established linking rules. 9
Similarly, rehabilitation interventions can target specific aspects of functioning, the environment, or both. Within an intervention, capacity and/or performance may be addressed. According to the ICF, performance reflects what a person does in their actual environment. Capacity reflects what a person does in a standardised situation, such as in an evaluation setting where context has been made irrelevant. 12 Importantly, a change in capacity is not necessarily associated with a change in performance in daily life. For example, a change in fastest walking speed or distance (d4500 Walking short distances) using a standardised test (e.g. timed 25-foot walk [T25FW] or 6-min walk test [6MWT]) may not always be related to how much a person walks in their own home or community, or whether they are able to achieve their own personal walking goals. 17 The gap between capacity and performance provides useful information about how the environment can be modified to improve performance. 8 For example, if a person with MS scores well using a standard cognitive battery like the MACFIMS, 18 but still reports struggling to keep up with the cognitive demands at work, changes in the workplace to minimise visual and auditory distractions, manage workflow, or alter task sequencing may support performance.
The ICF provides a solid foundation for conceptualising functioning and the factors that influence it, thereby supporting the design of rehabilitation clinical trials, including the selection of intermediate outcomes. Nevertheless, additional and more specific theories are necessary to fully map potential causal pathways and identify mechanisms of action linking a problem of functioning, how and why a particular intervention is expected to work, an intermediate outcome, and optimal functioning or ‘lived health’. These ideas are elaborated below.
Conceptual considerations: Selecting intermediate outcomes for optimal functioning
Figure 2 offers a visual summary linking a perceived, observed or expected problem of functioning, and the broad categories of possible, theoretically informed causal pathways (biological, psychological, social, contextual) and intervention types (body structure and function, activity, participation, environment) as described by the ICF. Examples of specific theories that are often used to guide MS rehabilitation research include motor-control and neuroplasticity theories (biological), behaviour change and goal setting theories (psychological), social cognitive and adult learning theories (social), and person–environment fit. The choice of theory guides the focus of the intervention, which is aligned with the functioning domains of the ICF, as well as the environmental and personal characteristics of the intended participants (e.g. young vs older adults; individuals with access to community services vs those without). Theory choice may also inform intervention content and delivery process. Strategies to describe interventions, which apply ICF terminology, are available.19,20
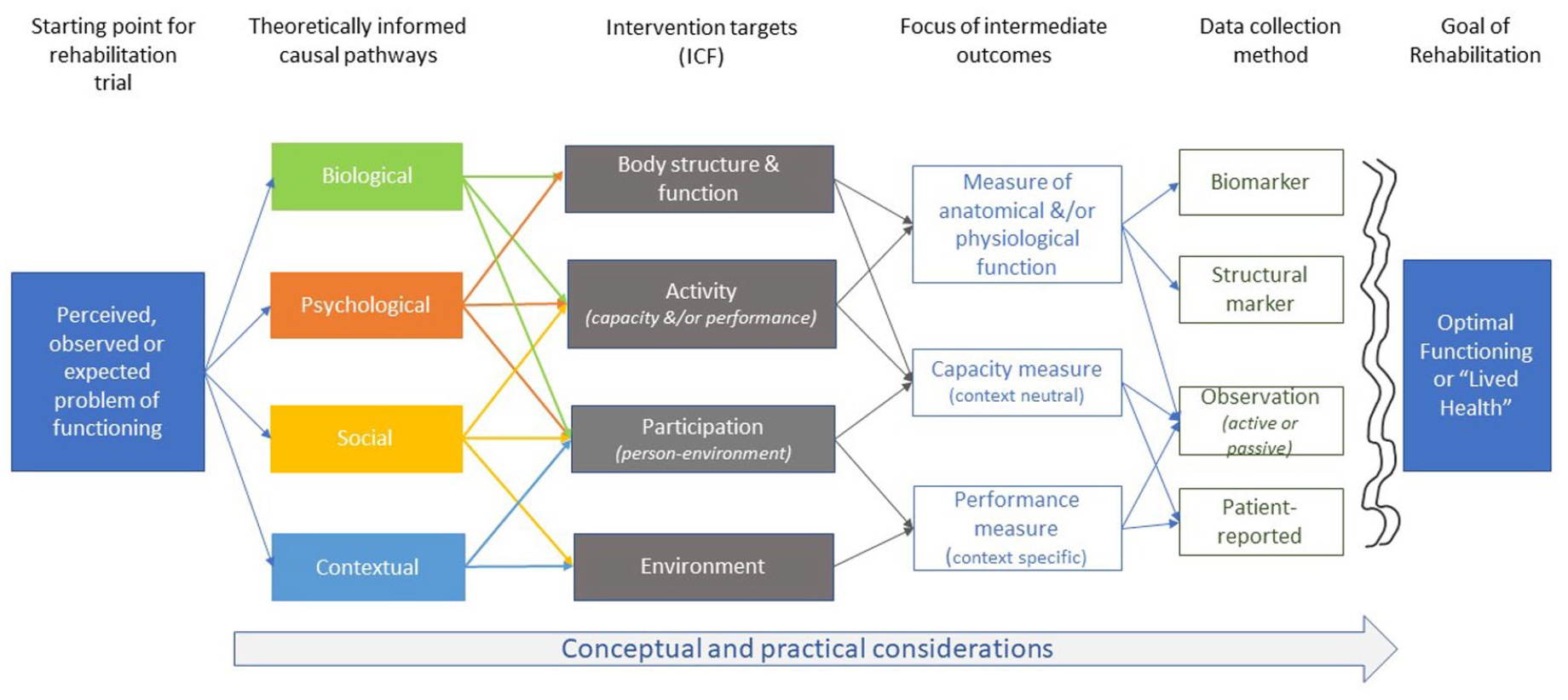
Process for selecting intermediate outcomes for MS rehabilitation trials, which start with the identification of a problem of functioning. The problem informs the selection of a theory to guide thinking about the causal pathway linking the intervention target and the focus of intermediate outcomes. The possibilities for causal pathways, intervention targets and focus of intermediate outcomes are all informed by the ICF. Once the focus of the intermediate outcome is determined, the specific method of data collection must be selected. Regardless of the data collection method, there is likely to be a gap between the measure obtained through that method and optimal functioning or lived health.
The focus of the intervention, in turn, informs the specific focus of the intermediate outcome, that is, a measure of anatomical and/or physiological function (e.g. joint range of motion), a capacity measure (context neutral; e.g. laboratory tested walking speed or hand function) or a performance measure (context-specific; e.g. accelerometry or ecological momentary assessment over 7 days). Once the focus of the outcome is determined, investigators then must determine the most appropriate method by which to collect data for that outcome, which may include biomarkers, structural markers, observation (active or passive) or a patient-reported outcome. Ultimately, the selection of an intermediate outcome, both in terms of focus and method of collection, must be conceptually congruent with the intervention being tested, and the pathway that is chosen to explain why and how the intervention is expected to influence optimal functioning or ‘lived health’.
It is important to emphasise that, for the many problems of functioning experienced by people with MS, each of the causal pathways could be at play, although some may be more critical than others at particular points in the disease or life course, in particular environmental situations, or based on patient goals. If we take the problem of activity curtailment related to the experience of accidental falls as an example (see Figure 1), there are plausible biological, psychological and environmental explanations.21 –24 Few if any rehabilitation interventions will be able to address all of them.25,26 This reality emphasises that rehabilitation (and functioning in general) cannot easily apply a reductionist paradigm, but rather benefits from a more holistic approach that can accommodate complexity. The downside is that rehabilitation researchers often select multiple outcomes to capture this complexity, which requires accounting for multiple comparisons, selecting a hierarchy when evaluating and interpreting the outcomes, or using composite outcomes. Importantly, composite outcomes must be considered carefully and interpreted together rather than separately. 27
Figure 2 suggests that choosing the ‘best’ causal pathway and a single intermediate outcome can be challenging to determine for a rehabilitation clinical trial. Failure to find significant effects at the end of the trial may not mean the intervention is ineffective, but may point to a mismatch across the selected causal pathway, the intervention, the profile of the study participants, and the intermediate outcome. Minimising the risk of this situation can be facilitated by considering a number of practical issues when selecting an intermediate outcome for a rehabilitation trial.
Practical considerations
Optimal functioning is a complex, multidimensional and dynamic construct, and ICF technical resources emphasise that direct inferences across domains of functioning are not appropriate because of the influence of contextual factors. 12 In other words, we cannot assume that an improvement in pain (body structure and function) will translate directly into greater mobility (activity) or engagement with friends (participation) for people with MS. This increases the importance of specifying and evaluating causal pathways to advance the science of MS rehabilitation. Articulating what specific changes are expected to occur, when, and in what sequence because of the intervention is therefore critical, particularly since rehabilitation interventions range from mechanistic to pragmatic, and are conducted in research laboratories as well as in community settings. What outcomes matter and when on a causal pathway will be influenced by the focus and features of the intervention.
Outcomes must be clearly defined and aligned with the functioning domain being targeted by the intervention, and be appropriate for the chosen study sample. For example, the evaluation of sit-to-stand transfer capacity is more important than walking in an advanced disease stage, while short walking tests do not capture the mobility requirements needed to navigate crowds in a shopping mall for those with mild disability. Ideally, an outcome measure would be applicable to individuals across the disability spectrum, but this is not always possible. Since the level of functioning of people with MS is heterogeneous, from early to late stages of the disease, investigators must decide to select a narrow patient population for a trial or to find a measure that can capture change and produce meaningful results across a diverse sample. The latter decision requires consideration about the impact of the evaluation process on study participants (i.e. can more disabled participants tolerate particular testing), whether there are modified and validated approaches to administer an outcome for individuals with different levels of disease severity (e.g. Symbol Digit Modalities Test (SDMT) by paper or computer), and whether the measure has known issues that would influence use and interpretability in particular sub-groups (e.g. floor or ceiling effects, learning effects, response shift, different minimal clinically important differences (MCID) or minimal detectable change (MDC) values across disability levels)28,29 (Figure 3).
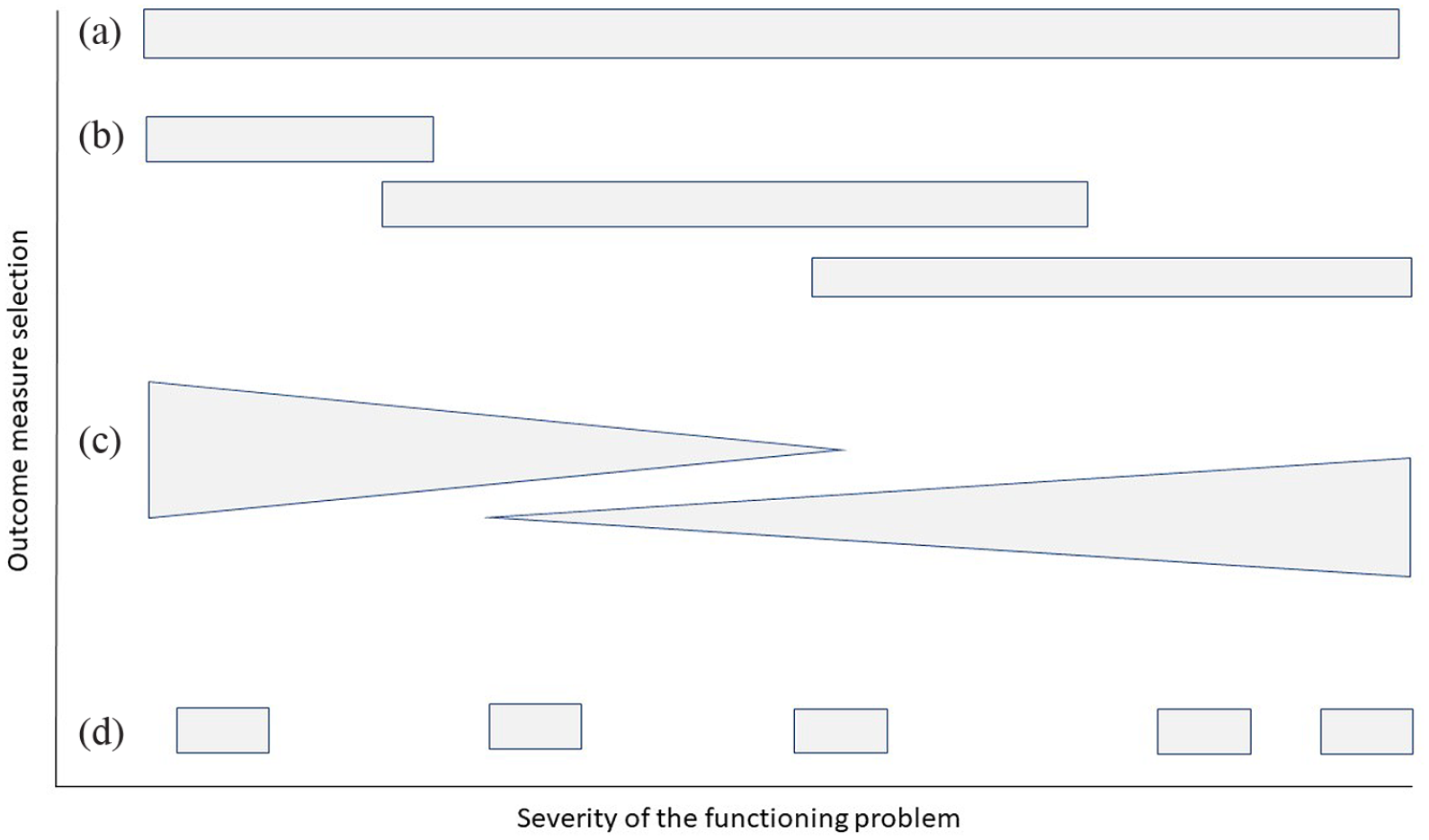
Graphical illustration of the applicability of outcome measures depending on the severity of the functioning problem. (a) Optimally, an outcome measure is capturing minimal, mild, moderate and severe disability, for example a patient outcome measure for pain or fatigue. (b) Outcome measures may have floor or ceiling effects (e.g. hand function), leading to applicability only for minimal/mild or moderate/severe problem of a functioning aspect. (c) Meaningful change may decrease or increase across the disability spectrum (e.g. walking tests). (d) Some outcome measures may require larger inter-test intervals because of learning effects (e.g. some cognitive tests) or response shifts (e.g. confidence).
The ICF Core Set for MS can be a helpful starting point, 30 as it provides 138 ICF items relevant to MS in the comprehensive version and 19 categories in the brief version. The core set identifies aspects of functioning deemed most important for describing functioning of people with MS. Importantly, the core set has been examined by people with MS, 31 and their perspective on what aspects of functioning are important for evaluation can be particularly helpful in trial design. 32 Considering the core set, the guiding theory, the intervention being tested, and then using the ICF linking rules 9 to examine specific outcome measures offers a robust approach to considering intermediate outcome options, across the MS disability spectrum.
Selecting outcomes also requires consideration of the psychometric properties of the measure being considered. Resources are available to guide the selection of psychometrically sound outcome measures by ICF level (https://www.sralab.org/rehabilitation-measures) or to evaluate measures for which these properties are not adequately documented (https://www.cosmin.nl). Knowing how to interpret changes on a selected measure pre to post intervention must also be considered. Changes need to exceed at least the smallest change detected by the outcome that is not the result of measurement error (i.e. the minimal detectable change; MDC). However, changes should also exceed the MCID to have a relevant impact on functioning. MDC and MCID values are available for some but not all measures used in rehabilitation trials, and may differ depending on the severity of the functioning aspect that is being measured. 28
The use of patient-reported outcomes is common in rehabilitation practice, as well as clinical trials. Yet, patient-reported outcomes are often subject to response shift over time, that is, the meaning of some measures is time-dependent because people understand them differently as they live with the disease and make adjustments based on experience. 33 Fortunately, statistical strategies are available to manage response shifts and allow the continued use of patient-reported outcomes. 33 Furthermore, the recently developed global Patient-Reported Outcomes Initiative for MS (PROMS) will be a resource as MS researchers consider the use of these measures. 34
Finally, future MS rehabilitation studies should consider novel outcomes that are not limited to collections at single time points, given day-to-day fluctuations and interplay of biological, psychological, social and environmental factors. Careful consideration on when repeated measures are necessary, and add value and statistical power to analysis, is encouraged. Technology is now allowing us to capture data over longer time periods (e.g. physical activity monitoring using wearables or ecological momentary assessment). These options may offer more sensitive outcomes that better reflect real life settings and, in the end, ‘lived health’.
Recommendations
The careful selection of intermediate outcomes will aid in understanding how and why rehabilitation interventions work, which, in turn, will support comprehensive MS care and improve optimal functioning of people affected by the disease. Based on the conceptual and practical issues raised in this article, we recommend the following list of actions to advance MS rehabilitation trials:
People affected by MS need to be explicitly and actively involved in rehabilitation trial design to facilitate the selection of meaningful intermediate outcomes and their interpretation through the lens of lived experience. 32 Their expertise needs to be integrated with available knowledge about the psychometric properties of outcome measures, and data available for interpretation of change (e.g. normative data, MDC and MCID).
The complexity of functioning requires explicit articulation of the theories, causal pathways and expected mechanisms of action underlying a rehabilitation trial, and their alignment with the intervention and outcome of interest. Visuals or other supplemental documents could provide this information if word count limitations make the inclusion of these details challenging in published articles. Including details of the intervention and its delivery as part of these documents, using a tool such as TiDIER, 35 would further support the understanding of how and why functioning changes.
Since rehabilitation delivered in clinical settings is tailored to patient goals and context, the use of innovative trial designs 15 and the development of new and innovative outcome measures that accommodate flexibility, diversity and a holistic approach should be encouraged as a way of promoting application of research findings into practice. In addition, greater use of multisite studies may strengthen our understanding of contextual factors and their influence on study outcomes.
If is determined that multiple outcomes are necessary for a rehabilitation trial, primary and secondary outcomes must be clearly articulated, be appropriate for the selected patient profile, and a pre-defined statistical analysis plan must be in place. Sequencing of multiple outcomes relative to the delivery of the intervention must be considered from a theoretical standpoint to capture that some functioning outcomes may be expected to emerge more quickly than others. Ideally, the selection of primary outcomes in a more pragmatic trial should be informed by the findings of more explanatory (mechanistic) studies.
Finally, advancing our understanding of how and why rehabilitation interventions modify functioning or ‘lived health’ would benefit from greater collaboration between rehabilitation scientists, neuroscientists, social scientists and disability scholars. Such collaborations would facilitate the development or elaboration of testable causal pathways linking the various domains of functioning to underlying biology, the way functioning is impacted by environmental demands, and how physical, cognitive and social demands of the environment are influenced by policies, systems and social attitudes. These collaborations need to span the full spectrum of trials, from explanatory to pragmatic.
Conclusion
The rehabilitation outcomes panel held as part of a 2-day meeting hosted by the International Advisory Committee on Clinical Trials in MS in December 2022 launched an important discussion about the relevance and applicability of intermediate outcomes in MS clinical trials. Although the language of intermediate outcomes is not common in rehabilitation research, the concept of using a replacement endpoint that can capture how or why a rehabilitation intervention affects optimal functioning or lived health has value. High quality rehabilitation trials that test explicit causal pathways in relevant samples with appropriate intermediate outcomes will advance MS care, regardless of whether they are conducted in a laboratory or the community. Greater collaboration, use of common language, and innovative designs will further support advances in the science of MS rehabilitation and help to change the experience of living with MS.
Supplemental Material
sj-docx-1-msj-10.1177_13524585231189674 – Supplemental material for Intermediate outcomes for clinical trials of multiple sclerosis rehabilitation interventions: Conceptual and practical considerations
Supplemental material, sj-docx-1-msj-10.1177_13524585231189674 for Intermediate outcomes for clinical trials of multiple sclerosis rehabilitation interventions: Conceptual and practical considerations by Marcia Finlayson, Peter Feys, Ulrik Dalgas and Daphne Kos in Multiple Sclerosis Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: M.F. is a co-investigator on projects funded by the Patient-Centered Outcomes Research Institute, the University Hospitals Kingston Foundation and the National Multiple Sclerosis Society. She has received consulting or teaching honoraria from Novartis and Biogen. P.F. received funding from the FWO Flanders, MS Society Flanders, KBS King Baudouin Foundation, MS Canada and Promobilia. Teaching honoraria were received from Roche. U.D. has received research support, travel grants and/or teaching honoraria from Biogen Idec, Merck Serono, Novartis, Bayer Schering and Sanofi Aventis as well as honoraria from serving on scientific advisory boards of Biogen Idec and Genzyme. D.K. has received consultancy or teaching honoraria from Roche, Almirall, Sanofi Genzyme, Biogen, Merck, Novartis and Teva.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The International Advisory Committee on Clinical Trials in Multiple Sclerosis and the International Conference on Innovations in Clinical Trial Design & Enhancing Inclusivity of Clinical Trial Populations were supported by the National Multiple Sclerosis Society and the European Committee for Treatment and Research in Multiple Sclerosis. There was no involvement of the sponsors in the design, collection, analysis or interpretation of data discussed at the Conference. The opinions expressed are those of the authors. Open access was made possible by the participation of Queen’s University in the Canadian Research Knowledge Network.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.