
Abstract
We described emergency department (ED) visits (all visits and infection-related) by persons with multiple sclerosis (MS) in British Columbia, Canada (1 April 2012 to 31 December 2017). We identified 15,350 MS cases using health administrative data; 73.4% were women, averaging 51.4 years at study entry. Over 4.9 years of follow-up (mean), 56.0% of MS cases visited an ED (mean = 0.6 visits/person/year; total = 37,072 visits). A diagnosis was documented for 25,698 (69.3%) ED visits, and 18.4% (4725/25,698) were infection-related. Inpatient admissions were reported for 20.4% (5238/25,698) of all and 29.2% (1380/4725) of infection-related ED visits. Findings suggest that the ED plays a substantial role in MS healthcare and infection management.
Introduction
Emergency department (ED) presentations represent an important aspect of health care utilization in the general population.1,2 Compared to the general population, persons with multiple sclerosis (MS) frequently access the healthcare system, with infections contributing to this higher healthcare use. For example, persons with MS had 41% more infection-related physician claims (adjusted rate ratio = 1.41; 95% confidence interval: 1.36–1.47) versus a sex-, age-, and region-matched non-MS population. 3 However, relatively little is known about ED utilization by persons with MS.4–6 Here, we described overall and infection-related ED use in an MS population.
Methods
We performed a descriptive, population-based study in British Columbia (BC), Canada, using linked health administrative data (via Population Data BC 7 ), including Medical Service Plan Billing Information 8 (providing physician claims); the Discharge Abstract Database 9 (providing hospital admissions/discharges); PharmaNet 10 (for prescriptions filled at outpatient/community pharmacies); Census Geodata (providing socioeconomic status estimates); Registration and Premium Billing files 11 (providing BC residency status via the mandatory healthcare plan registration days); Vital Statistics 12 (capturing death dates); and the National Ambulatory Care Reporting System dataset 13 (providing ED-related visit dates and Diagnosis Shortlist codes, 14 including infections; Supplementary Table 1) starting 1 April 2012).
All MS cases were identified with a validated algorithm. 15 Study entry date was the later of the first MS/demyelinating disease-related International Classification of Diseases (ICD-9/10) code, or first disease-modifying drug (DMD) prescription filled, or 1 April 2012 (start of the ED date). All included persons were ⩾18 years old and BC residents for ⩾1 year pre-study entry; follow-up ended at the earliest of death, emigration, or 31 December 2017. Comorbidities were measured using a modified Charlson Comorbidity Index during the 1-year pre-study entry.16–18 MS cases ever filling a DMD prescription during follow-up were described.
Results
We identified 15,350 MS cases (11,270 (73.4%) women; Table 1), of whom 86.5% (13,274/15,350) entered the study in 2012/2013, as per data availability. At study entry, the mean age was 51.4 years (standard deviation (SD) =13.8), and 26.5% (4072/15,350) had ⩾1 comorbidity. During the mean 4.9 (SD = 1.6) years of follow-up, 56.0% (8603/15,350) of MS cases visited an ED, totaling 37,072 visits; 15,350 MS cases averaged 0.6 (SD = 1.6) visits/person/year. MS cases visiting an ED at least once during follow-up (n = 8603) with (vs without) comorbidity at study entry were older (mean age = 56.5 (SD = 14.3) vs 49.5 (SD = 13.7) years) and averaged more ED visits/person/year (1.3 (SD = 2.4) vs 0.9 (SD = 1.9)). More than a quarter of MS cases had ⩾3 ED visits (4064/15,350; 26.5); of these 1383 (34.0%) of 4064 had ⩾1 comorbidity at study entry. Most ED visits by MS cases did not require an ambulance (26,359/37,072; 71.1%); 28.8% required a ground ambulance (10,691/37,072) and >95% were of semi-urgent or higher priority (35,468/37,072).
Characteristics of the multiple sclerosis study population in British Columbia, Canada (2012–2017).
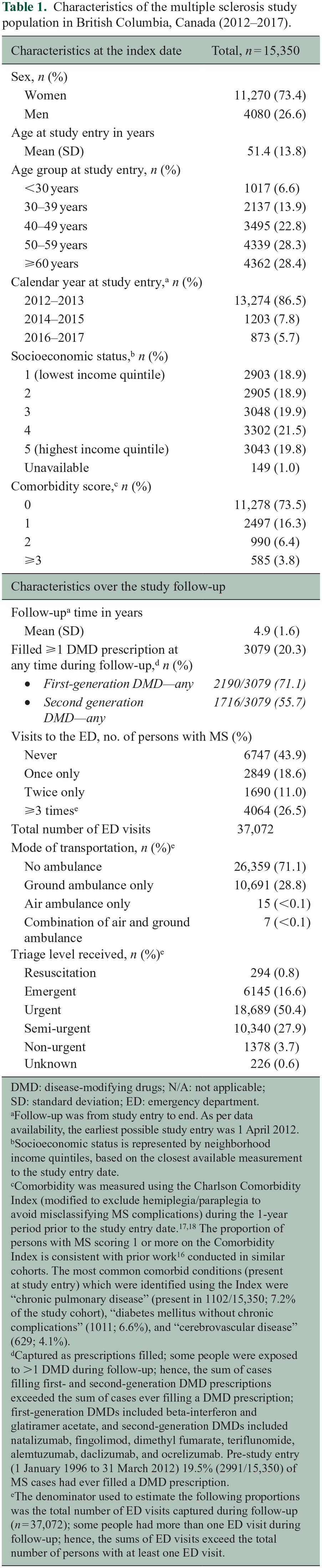
DMD: disease-modifying drugs; N/A: not applicable; SD: standard deviation; ED: emergency department.
Follow-up was from study entry to end. As per data availability, the earliest possible study entry was 1 April 2012.
Socioeconomic status is represented by neighborhood income quintiles, based on the closest available measurement to the study entry date.
Comorbidity was measured using the Charlson Comorbidity Index (modified to exclude hemiplegia/paraplegia to avoid misclassifying MS complications) during the 1-year period prior to the study entry date.17,18 The proportion of persons with MS scoring 1 or more on the Comorbidity Index is consistent with prior work 16 conducted in similar cohorts. The most common comorbid conditions (present at study entry) which were identified using the Index were “chronic pulmonary disease” (present in 1102/15,350; 7.2% of the study cohort), “diabetes mellitus without chronic complications” (1011; 6.6%), and “cerebrovascular disease” (629; 4.1%).
Captured as prescriptions filled; some people were exposed to >1 DMD during follow-up; hence, the sum of cases filling first- and second-generation DMD prescriptions exceeded the sum of cases ever filling a DMD prescription; first-generation DMDs included beta-interferon and glatiramer acetate, and second-generation DMDs included natalizumab, fingolimod, dimethyl fumarate, teriflunomide, alemtuzumab, daclizumab, and ocrelizumab. Pre-study entry (1 January 1996 to 31 March 2012) 19.5% (2991/15,350) of MS cases had ever filled a DMD prescription.
The denominator used to estimate the following proportions was the total number of ED visits captured during follow-up (n = 37,072); some people had more than one ED visit during follow-up; hence, the sums of ED visits exceed the total number of persons with at least one ED visit.
ED visits with a known diagnosis
Diagnostic codes were reported for 69.3% (25,698/37,072) of ED visits (summarized in Supplementary Table 2). These visits were made by 74.2% (6384/8603) of MS ED users. Of these, the most frequent primary diagnoses were “abdominal pain/colic” (1279/25,698 visits; 5.0%), “urinary tract infection” (1277 visits; 5.0%), and “MS” (1225 visits; 4.8%). When combined, 18.4% (4725/25,698) of ED visits were infection-related with 32.2% (2056/6384) of MS participants having at least one such visit. Nearly one-third (1380/4725; 29.2%) of infection-related ED visits led to hospitalization, while 20.4% (5238/25,698) of all ED visits made by 27.9% (2404/8603) of cases did so (Supplementary Tables 2 and 3).
DMD users versus non-users
Persons who filled ⩾1 DMD prescription(s) during follow-up (“DMD users”) were younger at study entry date than non-users (mean age = 41.9 (SD = 11.1) vs 53.8 (SD = 13.3) years). However, the proportions accessing an ED at least once were generally similar (1806/3079, 58.0% of DMD users and 6797/12,271, 55.6% of non-user), as was the study follow-up time (4.8 years (SD = 1.6) for DMD users vs 4.9 (SD = 1.6) for non-users).
Socioeconomic status
There were no clear patterns across the socioeconomic quintiles at study entry for the MS cases: ever/never filling a DMD prescription during follow-up, ever/never being hospitalized subsequent to an ED visit, or for the five most common ED diagnoses (data not shown).
Conclusion
Over 50% of persons with MS had more than one ED consultation during our nearly 6-year observation period; one-quarter visited an ED three or more times. Nearly 20% of ED visits were infection-related; one-third resulted in hospitalization, whereas one-fifth of all-cause ED visits did so. MS cases with ⩾1 (vs without) comorbidity at study entry averaged more ED visits/person/year. Our intentionally descriptive study has several limitations. While the overall burden of infection-related ED visits was considerable in our MS population, this could be higher as diagnoses were unavailable for one-third of all ED visits. Furthermore, our study lacked MS-specific clinical information, such as relapses, and a comparison to the general population. Our 1-year pre-study lookback period may have reduced the detection of comorbidities. Strengths of our study included the large cohort of MS cases identified using a validated algorithm within a geographically defined population with universal healthcare coverage, including ED visits. Our results suggest that the ED visits by MS cases often lead to hospitalizations, perhaps more so for infection-related visits. Further studies are necessary to better understand the importance of ED use by persons with MS.
Supplemental Material
sj-docx-1-msj-10.1177_13524585221078497 – Supplemental material for Emergency department use by persons with MS: A population-based descriptive study with a focus on infection-related visits
Supplemental material, sj-docx-1-msj-10.1177_13524585221078497 for Emergency department use by persons with MS: A population-based descriptive study with a focus on infection-related visits by Jonas Graf, Huah Shin Ng, Feng Zhu, Yinshan Zhao, José MA Wijnands, Charity Evans, John D Fisk, Ruth Ann Marrie and Helen Tremlett in Multiple Sclerosis Journal
Supplemental Material
sj-docx-2-msj-10.1177_13524585221078497 – Supplemental material for Emergency department use by persons with MS: A population-based descriptive study with a focus on infection-related visits
Supplemental material, sj-docx-2-msj-10.1177_13524585221078497 for Emergency department use by persons with MS: A population-based descriptive study with a focus on infection-related visits by Jonas Graf, Huah Shin Ng, Feng Zhu, Yinshan Zhao, José MA Wijnands, Charity Evans, John D Fisk, Ruth Ann Marrie and Helen Tremlett in Multiple Sclerosis Journal
Supplemental Material
sj-docx-3-msj-10.1177_13524585221078497 – Supplemental material for Emergency department use by persons with MS: A population-based descriptive study with a focus on infection-related visits
Supplemental material, sj-docx-3-msj-10.1177_13524585221078497 for Emergency department use by persons with MS: A population-based descriptive study with a focus on infection-related visits by Jonas Graf, Huah Shin Ng, Feng Zhu, Yinshan Zhao, José MA Wijnands, Charity Evans, John D Fisk, Ruth Ann Marrie and Helen Tremlett in Multiple Sclerosis Journal
Footnotes
Acknowledgements
Ethical approval was obtained; the University of British Columbia’s Clinical Research Ethics Board approved the study. Access to and use of British Columbia (BC) data were facilitated by Population Data BC and approved by the BC Ministry of Health, BC PharmaNet, and the BC Vital Statistics Agency. All inferences, opinions, and conclusions drawn in this manuscript are those of the authors and do not reflect the opinions or policies of the British Columbia Data Steward(s). We are grateful to Dr Lawrence W Svenson for supporting the team’s original funding application.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jonas Graf has received in the last 3 years travel/meeting/accommodation reimbursements from Merck Serono, Sanofi-Genzyme, and Grifols and receives a Research Fellowship from the Deutsche Forschungsgemeinschaft (project number 438899010, GZ: GR 5665/1-1). Huah Shin Ng receives funding from the MS Society of Canada/s endMS Postdoctoral Fellowship and endMS Scholar Program for Researchers IN Training (SPRINT), and the Michael Smith Foundation for Health Research Trainee Award. During the past year, she has received funding from the Canadian Institutes of Health Research (CIHR) Drug Safety and Effectiveness Cross-Disciplinary Training Program. Feng Zhu, Yinshan Zhao, José M A Wijnands, and Charity Evans declare no conflicts. John Fisk receives research funding from CIHR, the MS Society of Canada, Crohn’s and Colitis Canada, Research Nova Scotia, and the Nova Scotia Health Authority Research Fund and licensing and distribution fees from MAPI Research Trust. Ruth Ann Marrie receives research funding from CIHR, Research Manitoba, Multiple Sclerosis Society of Canada, Multiple Sclerosis Scientific Foundation, Crohn’s and Colitis Canada, National Multiple Sclerosis Society, CMSC, the US Department of Defense, Biogen Idec, and Roche and is supported by the Waugh Family Chair in Multiple Sclerosis. Helen Tremlett has received research support in the last 3 years from the Canada Research Chair program, National MS Society, Canadian Institutes of Health Research, Canada Foundation for Innovation, MS Society of Canada, and the MS Scientific Research Foundation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Canadian Institutes of Health Research (CIHR) Project and Foundation grant (PJT-156363 and FDN-159934, PI: Tremlett).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.