
Abstract
Background:
Immune-mediated demyelination and consequent degeneration of oligodendrocytes and axons are hallmark features of multiple sclerosis (MS). Remyelination declines in progressive MS, causing permanent axonal loss and irreversible disabilities. Strategies aimed at enhancing remyelination are critical to attenuate disease progression.
Objective:
We systematically reviewed recent advances in neuroprotective and regenerative therapies for MS, covering preclinical and clinical studies.
Methods:
We searched three biomedical databases using defined keywords. Two authors independently reviewed articles for inclusion based on pre-specified criteria. The data were extracted from each study and assessed for risk of bias.
Results:
Our search identified 7351 studies from 2014 to 2020, of which 221 met the defined criteria. These studies reported 262 interventions, wherein 92% were evaluated in animal models. These interventions comprised protein, RNA, lipid and cellular biologics, small molecules, inorganic compounds, and dietary and physiological interventions. Small molecules were the most highly represented strategy, followed by antibody therapies and stem cell transplantation.
Conclusion:
While significant strides have been made to develop regenerative treatments for MS, the current evidence illustrates a skewed representation of the types of strategies that advance to clinical trials. Further examination is thus required to address current barriers to implementing experimental treatments in clinical settings.
Keywords
Introduction
Multiple sclerosis (MS) is an immune-mediated neurodegenerative disease of the central nervous system (CNS) characterized by demyelination, oligodendroglial loss, and axonal pathology.1,2 Demyelination disrupts signal transmission within the CNS, causing a gradual accumulation of physical and cognitive disability.2–4 Importantly, prolonged demyelination results in progressive axon degeneration in chronic MS lesions. 5 Remyelination, the formation of new myelin, is, therefore, an essential process for maintaining the structural integrity of axons and for restoring and maintaining neurological function in MS. 6 Remyelination can occur spontaneously in demyelinating plaques; however, this capacity declines in chronic, progressive MS.6,7 While the underlying mechanisms are not fully understood, it is thought that remyelination is incomplete in progressive MS due to multiple factors, including the depletion of oligodendrocyte progenitor cells (OPCs), the reduced ability of OPCs to differentiate into mature myelinating oligodendrocytes, and the presence of inhibitory factors in the microenvironment of MS lesions.8–10 Current disease-modifying therapies (DMTs) for MS are primarily immunomodulatory to reduce neuroinflammation and prevent relapses. 11 However, these DMTs have been notably less effective in preventing the progression of neurodegeneration and disability in persons with MS. 12
Emphasized by the unmet need for regenerative therapies for MS, the development of strategies aimed at preventing oligodendrocyte and myelin damage, as well as enhancing axonal remyelination and integrity, has garnered increased recognition from researchers and clinicians in recent years. 13 These strategies include increasing trophic support for oligodendrocytes and axons, stimulating oligodendrogenesis, neutralizing inhibitors of oligodendrocyte differentiation and remyelination, and promoting axonal integrity and regeneration, among others (Figure 1). The purpose of the present systematic review is to provide a timely overview of recent advancements in the development of regenerative therapies that specifically target oligodendrogenesis and remyelination and/or exhibit neuroprotective effects in individuals with MS and preclinical models of disease.
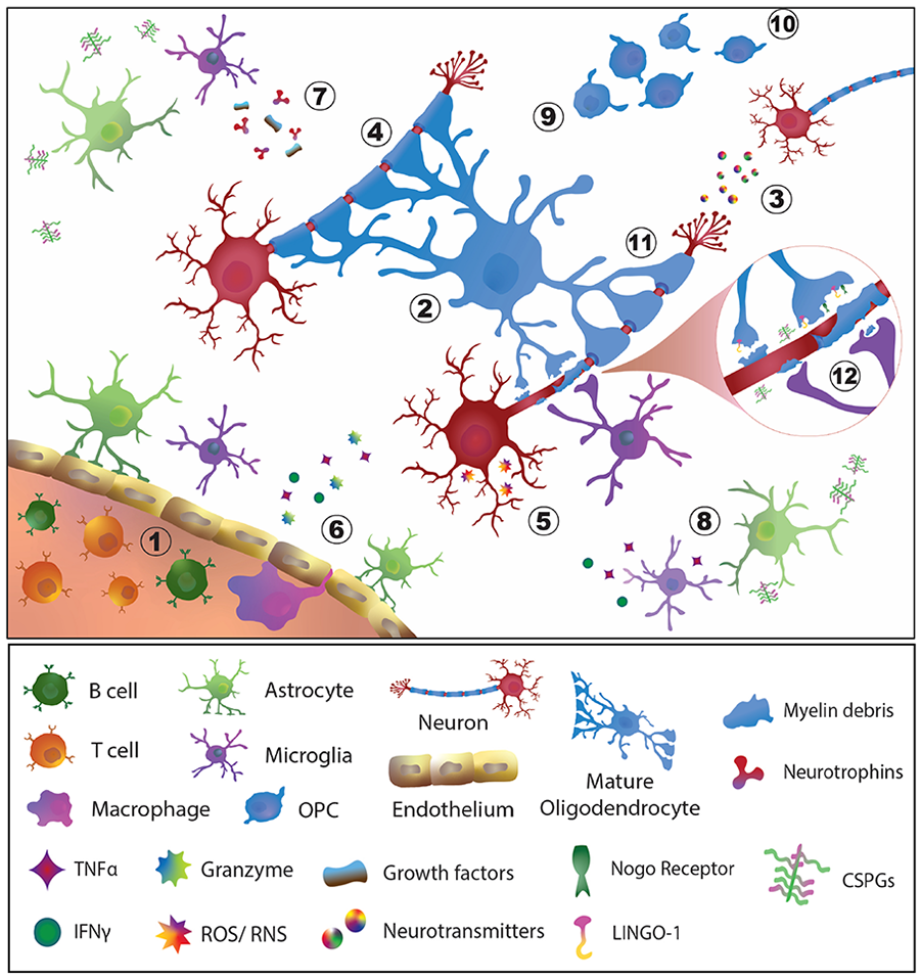
Neurodegenerative and inflammatory processes in an MS lesion amenable to preventive and regenerative therapies. Feasible points of intervention include: (1) immunomodulation, the predominant strategy of currently available therapeutics for MS; (2) promote the viability of OPCs and oligodendrocytes; (3) preserve the quantity and integrity of neurons and axons; (4) Protect myelin to prevent further loss; (5) reduce oxidative stress, apoptosis or cellular dysfunction of neurons and glial cells; (6) promote blood–brain barrier integrity; (7) stimulate neurotrophin and growth factor production; (8) reduce pro-inflammatory activation of glial cells; (9) promote the proliferation of OPCs and their differentiation into mature myelinating oligodendrocytes; (10) induce the migration and recruitment of OPCs and oligodendrocytes to sites of demyelination; (11) induce the formation of new myelin; and (12) target inhibitory factors associated with myelin debris and promote its clearance to support remyelination of denuded axons.
Methods
Search strategy
Keywords for the search strategy were defined with the assistance of two librarians and are presented in Supplementary Table S1. English-written studies were identified by searching three databases: Medical Literature Analysis and Retrieval System Online (MEDLINE), Evidence-Based Medicine (EBM) Review, and Excerpta Medica dataBASE (EMBASE). We included studies that were published from 1 January 2014 to 16 January 2020. Clinical MS studies with measures of myelination and disability were included. Preclinical animal studies with at least one direct measure of myelination, oligodendrocytes, oligodendrocytes precursor cells, or axonal regeneration were included. Studies that used preclinical animal models characterized predominantly by immune-mediated pathology (i.e. experimental autoimmune encephalomyelitis (EAE) models) were included if evidence was provided to indicate that the observed neurological benefit of the intervention was not exclusively a result of indirect peripheral immunomodulation (e.g. effects on T cells, B cells and macrophages). Full inclusion and exclusion criteria are listed in Supplementary Table S2.
Data extraction and evaluation
Studies obtained from the queried databases were imported into Covidence, web-based software for systematic review management (Veritas Health Innovation, Melbourne, Australia). For the abstract and full-text screenings, two authors independently evaluated each study based on the inclusion and exclusion criteria, and, in case of disagreement, a third author refereed. Data from all included studies were then extracted into summary spreadsheets based on the type of intervention, the study design, and the measured outcomes. Finally, we assessed the risk of bias for each study using the Cochrane Collaboration tool 14 for clinical studies and the SYstematic Review Centre for Laboratory animal Experimentation (SYRCLE) tool 15 for animal studies.
Results
The database search resulted in 7351 studies, of which 383 were screened at the manuscript level (Figure 2). After assessment of the exclusion criteria, 221 studies were included for data extraction (full list provided in Supplementary Table S3). Among the included studies, 92% were preclinical animal studies, 7% were clinical trials, and the remaining were observational human studies (Figure 3). Cuprizone was the most commonly employed agent to induce demyelination in preclinical studies, followed by active EAE induction and localized injections of lysophosphatidylcholines (LPC, lysolecithin) or ethidium bromide (EtBr) (Figure 3). The majority of included clinical trials were reported in phase II. Descriptions of the reported preclinical and clinical study designs are noted in Supplementary Table S4.
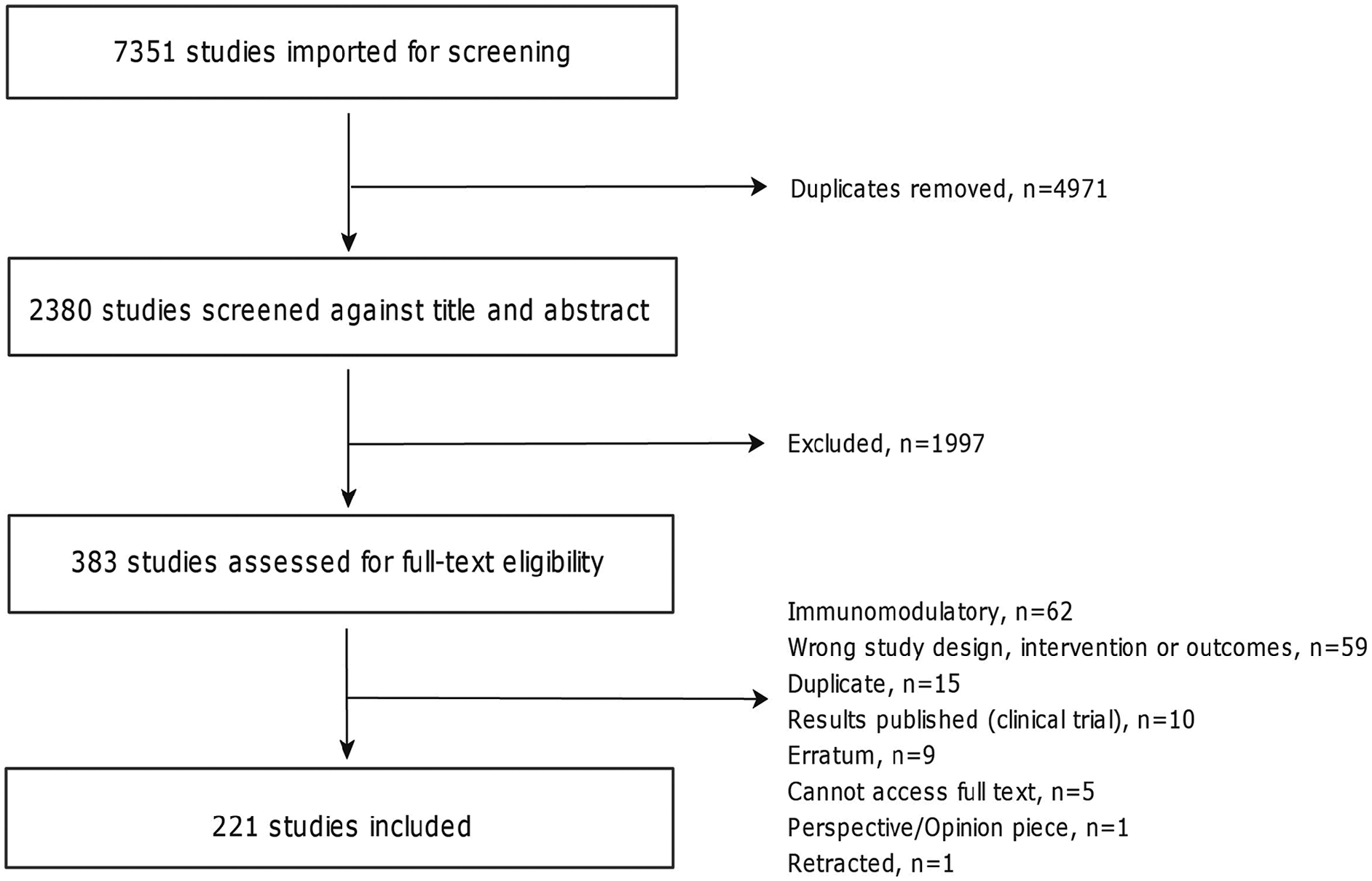
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) diagram.
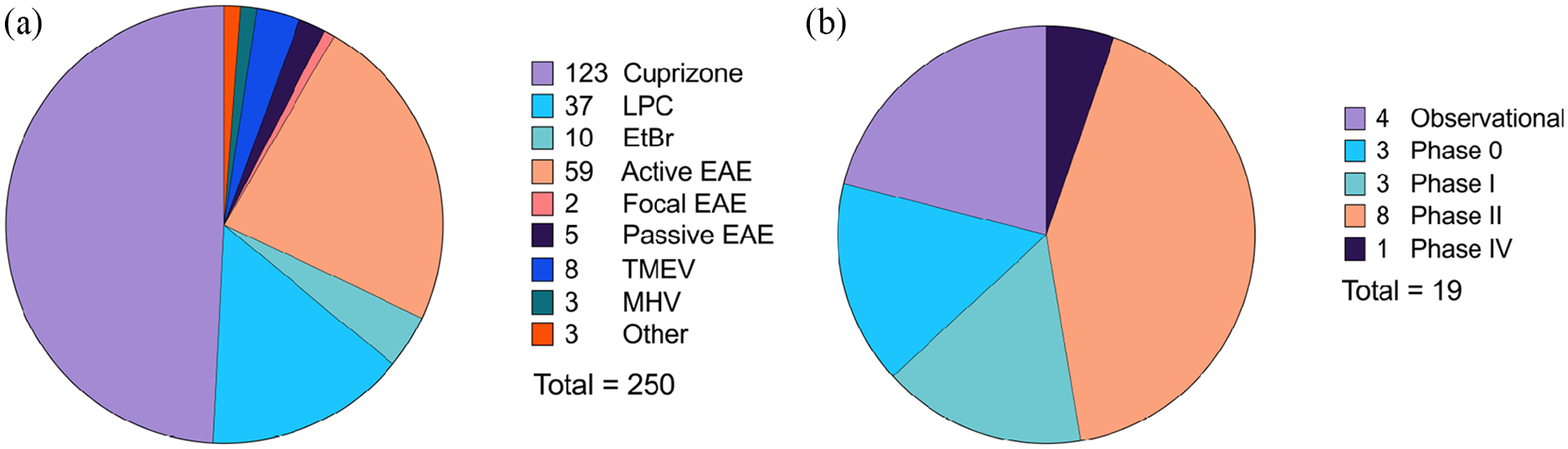
Reported preclinical models (a) and clinical trial phases (b) used to evaluate remyelinating and/or neuroprotective interventions for MS. Among the 221 included articles, a total of 250 animal model studies and 19 clinical studies were reported. Descriptions of each study type are included in Supplementary Table S4.
We assessed the risk of bias for animal studies using SYRCLE’s tool (Table 1). We found no risk of bias related to allocation concealment in preclinical studies. Similarly, we identified a low risk of bias for the following four items: similarity of groups at baseline, housing during the experiment, animal welfare, and statement of potential conflicts of interest. For most studies, however, caregivers and investigators were not blinded from the interventions received by animals during the experiment, and nearly 50% were not blinded for outcome assessments. Furthermore, 60% of studies did not report any measure of randomization, and 96% did not report sample size calculations.
Quality assessment of included preclinical and clinical studies.
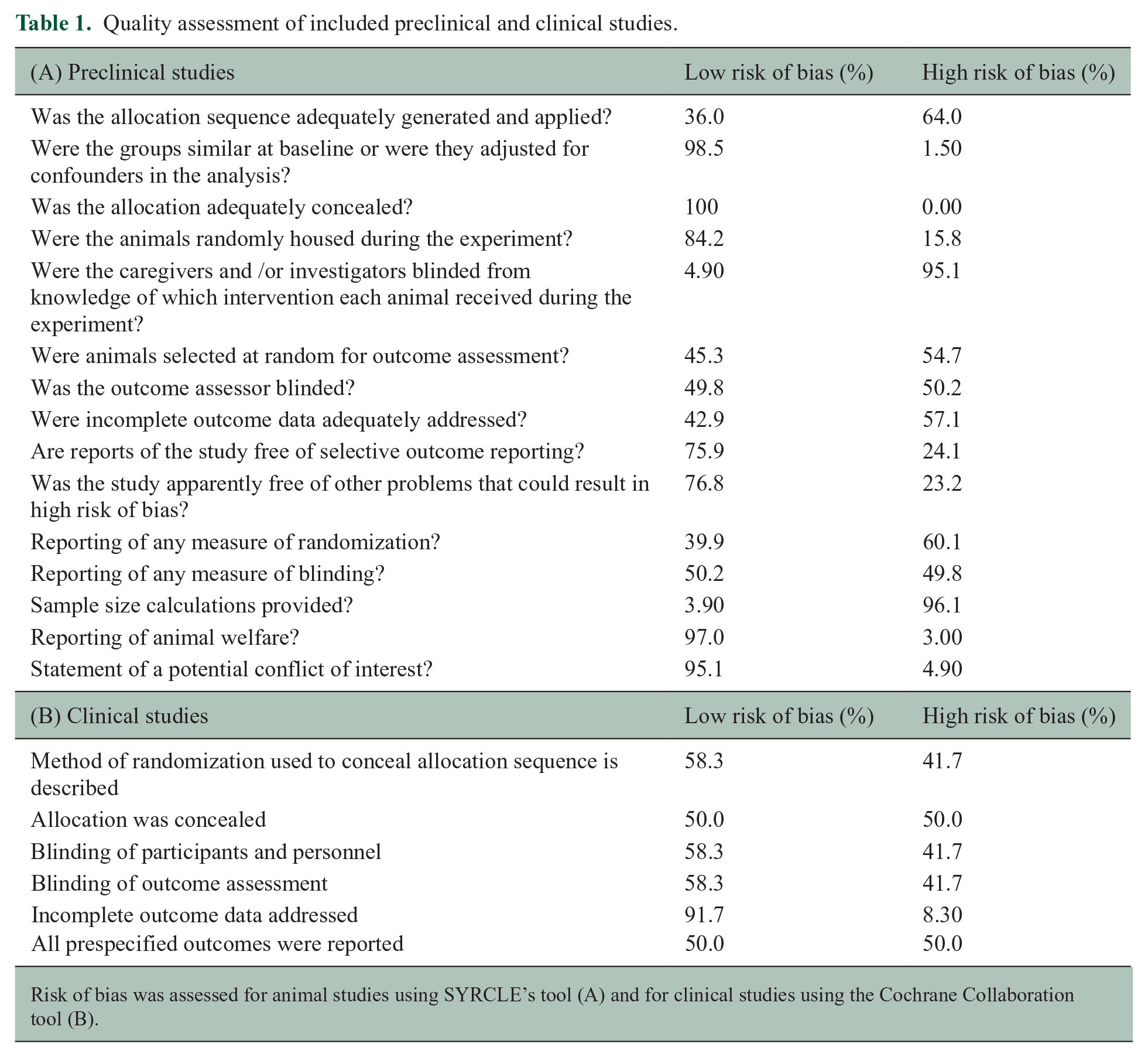
Risk of bias was assessed for animal studies using SYRCLE’s tool (A) and for clinical studies using the Cochrane Collaboration tool (B).
We also evaluated the risk of bias for 12 clinical trials; the remaining clinical studies were not included because they were abstracts or conference papers. For most clinical studies, we found a low risk of bias related to incomplete outcome data (Table 1). For the other indicators, such as allocation concealment and blinding of interventions and outcomes, we observed a high risk of bias in at least 50% of studies. It is noteworthy that the biases related to randomization and blinding were more often encountered in observational human studies than in clinical trials.
A total of 262 interventions were reported within the 221 included articles. To summarize the data, interventions were categorized into eight main classes: Small molecules, protein biologics, cellular biologics, RNA biologics, lipid biologics, dietary interventions, physiological interventions, and inorganic compounds (Figure 4). The neuroprotective and regenerative effects of the most highly represented interventions in each class are described in the main text. Structural, mechanistic, and biological effects for individual interventions within each class are listed in Supplementary Table S5.
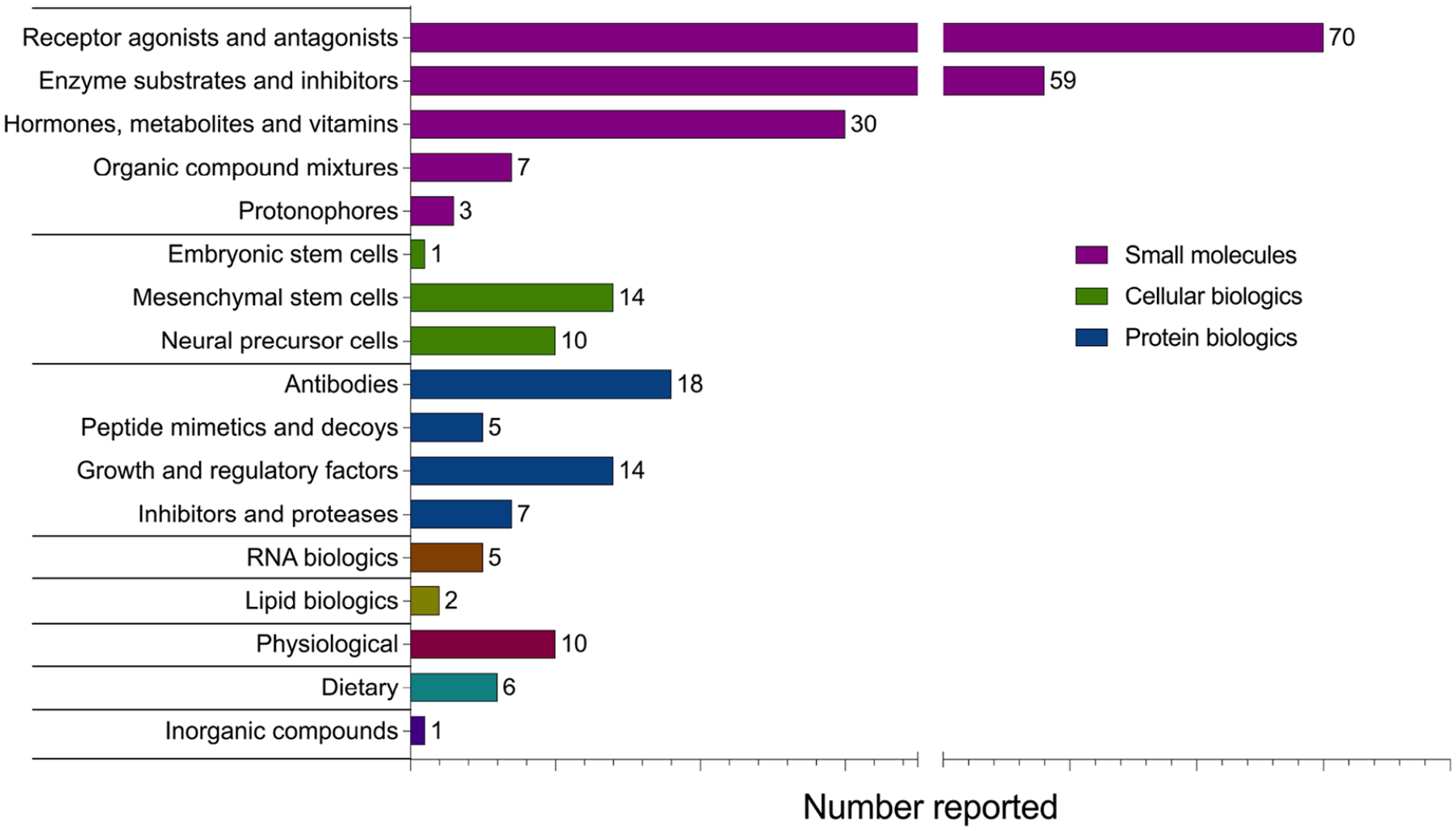
Classification of 262 interventions evaluated for neuroprotective and regenerative effects in MS patients and preclinical models of disease. Treatments applicable to multiple classes were assigned to a single class for clarity. Assessments of the same treatment in multiple different articles were counted as separate reports, for example, fingolimod (FTY720) was separately studied in and counted as 11 reports.
Small molecules
Administration of small organic molecules was the most frequently reported intervention strategy, comprising 64.5% of all reports. Small molecules, defined as low molecular weight compounds (<900 Daltons), are advantageous in clinical practice due to their ease of administration, high solubility, blood-CNS barrier penetrance, and, often, narrow target specificity. 16 Many reported small-molecule therapies are already approved by the U.S. Food and Drug Administration (FDA) and/or act through defined cellular mechanisms. A total of 23 small-molecule therapies were reported in two or more separate articles, which were subcategorized into five groups based on mechanisms of action (Tables 2–4).
Neuroprotective and regenerative effects of small-molecule receptor agonists and antagonists reported in two or more separate articles.
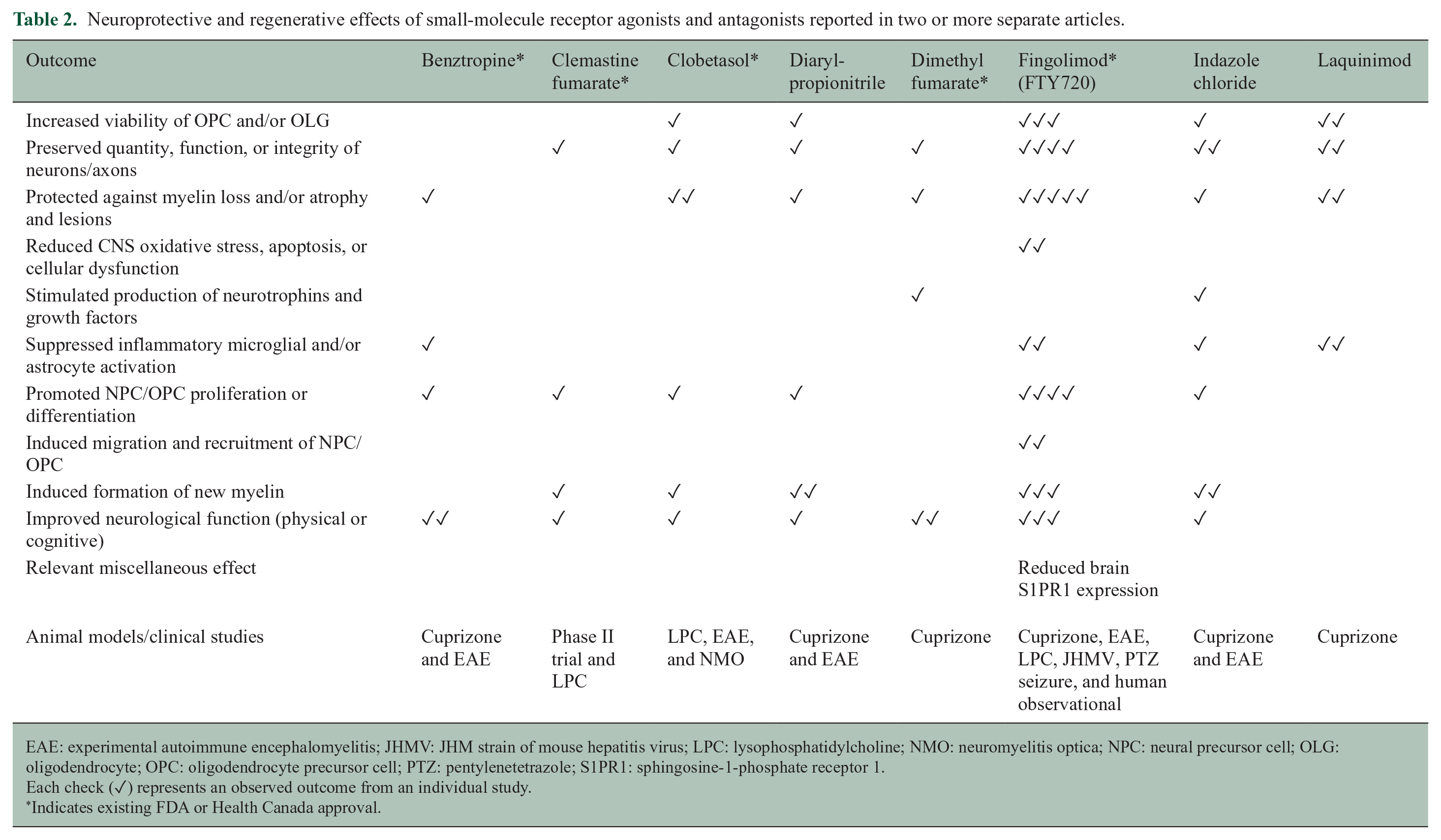
EAE: experimental autoimmune encephalomyelitis; JHMV: JHM strain of mouse hepatitis virus; LPC: lysophosphatidylcholine; NMO: neuromyelitis optica; NPC: neural precursor cell; OLG: oligodendrocyte; OPC: oligodendrocyte precursor cell; PTZ: pentylenetetrazole; S1PR1: sphingosine-1-phosphate receptor 1.
Each check (✓) represents an observed outcome from an individual study.
Indicates existing FDA or Health Canada approval.
Neuroprotective and regenerative effects of small-molecule enzyme substrates and inhibitors reported in two or more separate articles.
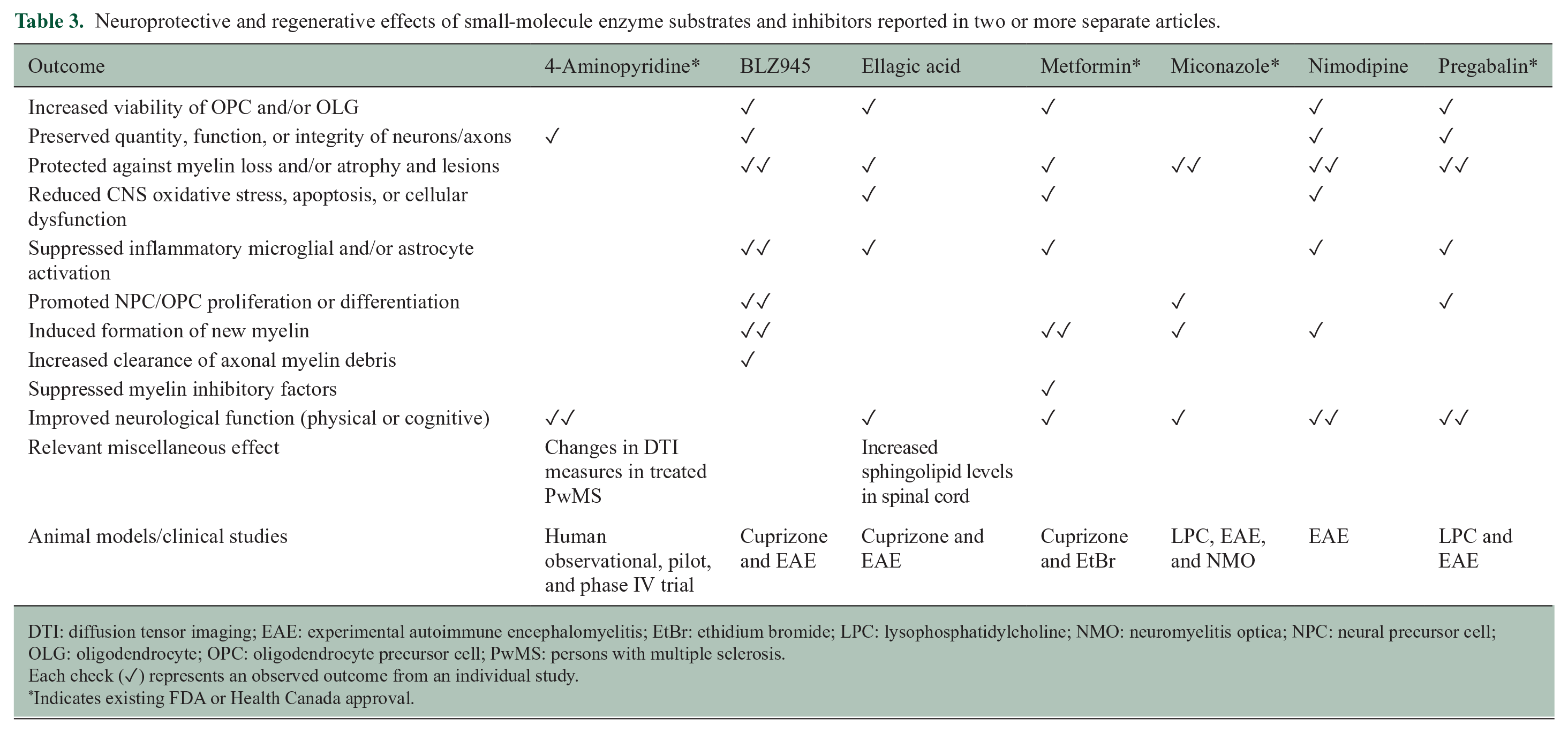
DTI: diffusion tensor imaging; EAE: experimental autoimmune encephalomyelitis; EtBr: ethidium bromide; LPC: lysophosphatidylcholine; NMO: neuromyelitis optica; NPC: neural precursor cell; OLG: oligodendrocyte; OPC: oligodendrocyte precursor cell; PwMS: persons with multiple sclerosis.
Each check (✓) represents an observed outcome from an individual study.
Indicates existing FDA or Health Canada approval.
Neuroprotective and regenerative effects of small-molecule hormone, metabolite, and vitamin administration reported in two or more separate articles.
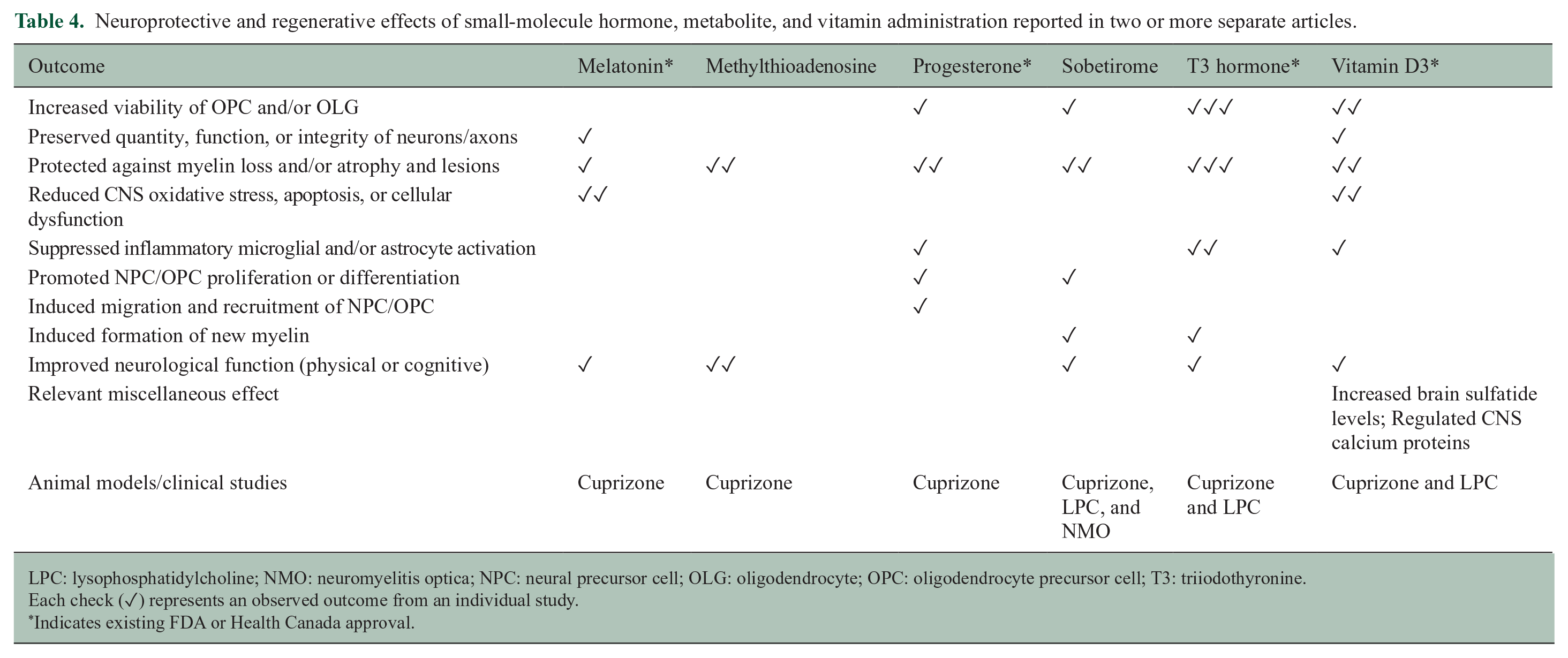
LPC: lysophosphatidylcholine; NMO: neuromyelitis optica; NPC: neural precursor cell; OLG: oligodendrocyte; OPC: oligodendrocyte precursor cell; T3: triiodothyronine.
Each check (✓) represents an observed outcome from an individual study.
Indicates existing FDA or Health Canada approval.
Receptor agonists and antagonists
Treatments within this subclass composed 41.4% of small-molecule interventions and included eight drugs reported in two or more separate articles (Table 2): benztropine, clemastine fumarate, clobetasol, diarylpropionitrile, dimethyl fumarate, fingolimod (FTY720), indazole chloride, and laquinimod. Of note, fingolimod was the most frequently reported drug to exhibit positive effects on remyelination and neuroprotection, despite some reports of null effects when administration method and preclinical study design differed among studies. Fingolimod is an approved immunomodulatory drug for relapsing-remitting MS (RRMS) that sequesters T cells in peripheral lymph nodes by blocking sphingosine-1-phosphate (S1-P) receptors and thereby suppresses autoreactive T cell migration to the CNS. 17 S1-P receptors are also expressed in the brain, where fingolimod has been shown to penetrate and accumulate in cuprizone-treated mice. 18 The existing data collectively indicate that fingolimod influences immune-independent aspects of MS pathology, in addition to its canonical effect on T cells. In addition, the reported receptor modulators methylprednisolone and GSK239512 have completed initial clinical trials for MS. In individuals with progressive MS, methylprednisolone safely improved disability and magnetic resonance imaging (MRI) measures of disease, 19 while GSK239512 treatment demonstrated a small positive effect on lesion remyelination in people with RRMS. 20
Enzyme substrates and inhibitors
Drugs that primarily interacted with enzymes in key signaling or metabolic pathways composed 34.9% of small-molecule reports and included seven drugs that were reported in two or more separate articles (Table 3): BLZ945, 4-aminopyridine (Fampridine), ellagic acid, metformin, miconazole, nimodipine, and pregabalin. In addition to these seven inhibitors, the selective sodium-channel inhibitor and antiepileptic drug, phenytoin, was neuroprotective of the retinal nerve fiber layer in persons with optic neuritis in a phase II trial. 21
Hormones, metabolites, and vitamins
Among studies that employed small molecule interventions, 17.8% entailed treatment with vitamins, simple derivatives of endogenous metabolites, or synthetic hormones/hormone mimetics. Among them, six small molecules were reported in two or more separate articles (Table 4): melatonin, methylthioadenosine, progesterone, sobetirome, triiodothyronine (T3) hormone, and vitamin D3 (calcitriol and/or cholecalciferol).
Protonophores
Two articles described the neuroprotective effects of the protonophore MP101 (2,4-dinitrophenol) and its prodrug, MP201, in EAE and cuprizone animal models.22,23 MP101 uncouples oxidative phosphorylation in a dose-dependent manner by enabling protons to translocate across the inner mitochondrial membrane, which then reduces energy production efficiency and stimulates metabolism. 23 MP101/MP201 administration in the two animal models resulted in multifaceted beneficial effects. Treatment reduced clinical disability and visual impairment, attenuated gliosis, promoted expression of brain-derived neurotrophic factor (BDNF), reduced mitochondrial dysfunction, and ameliorated myelin and axonal damage.22,23
Organic compound mixtures
Interventions classified as organic compound mixtures included composite plant and herbal extracts, as well as culturally traditional formulations that contain multiple small molecules. The reported preparations most frequently incorporated flavonoids, terpenes, polyprenols, and plant metabolites mimicking endogenous ligands. Generally, the effects of the composite treatments were ascribed to the antioxidant and anti-inflammatory actions of the numerous small molecules within the formulations. Treatment with the biflavonoid complex Kolaviron, isolated from Garcinia kola seeds, was reported in two separate studies using the cuprizone model. The reported neuroprotective effects included alleviation of clinical symptoms, reduced oxidative stress, and preservation of neural integrity in the demyelinated brain.24,25 In addition, the ∆-9-tetrahydrocannabinol (THC) and cannabidiol (CBD)-based medication, Sativex®, improved motor function, reduced glial scar formation, and protected myelin and axons in a viral demyelination model. 26 Sativex is currently approved by Health Canada to treat MS neuropathic pain and spasticity in adults; these preclinical results suggest the treatment may also be neuroprotective. 26
Protein biologics
Protein therapies comprised 16.8% of all reported strategies. Five treatments were reported to have neuroprotective or regenerative effects in two or more separate articles, including two antibodies, one peptide mimetic, and two growth factors (Table 5).
Neuroprotective and regenerative effects of protein biologics reported in two or more separate articles.
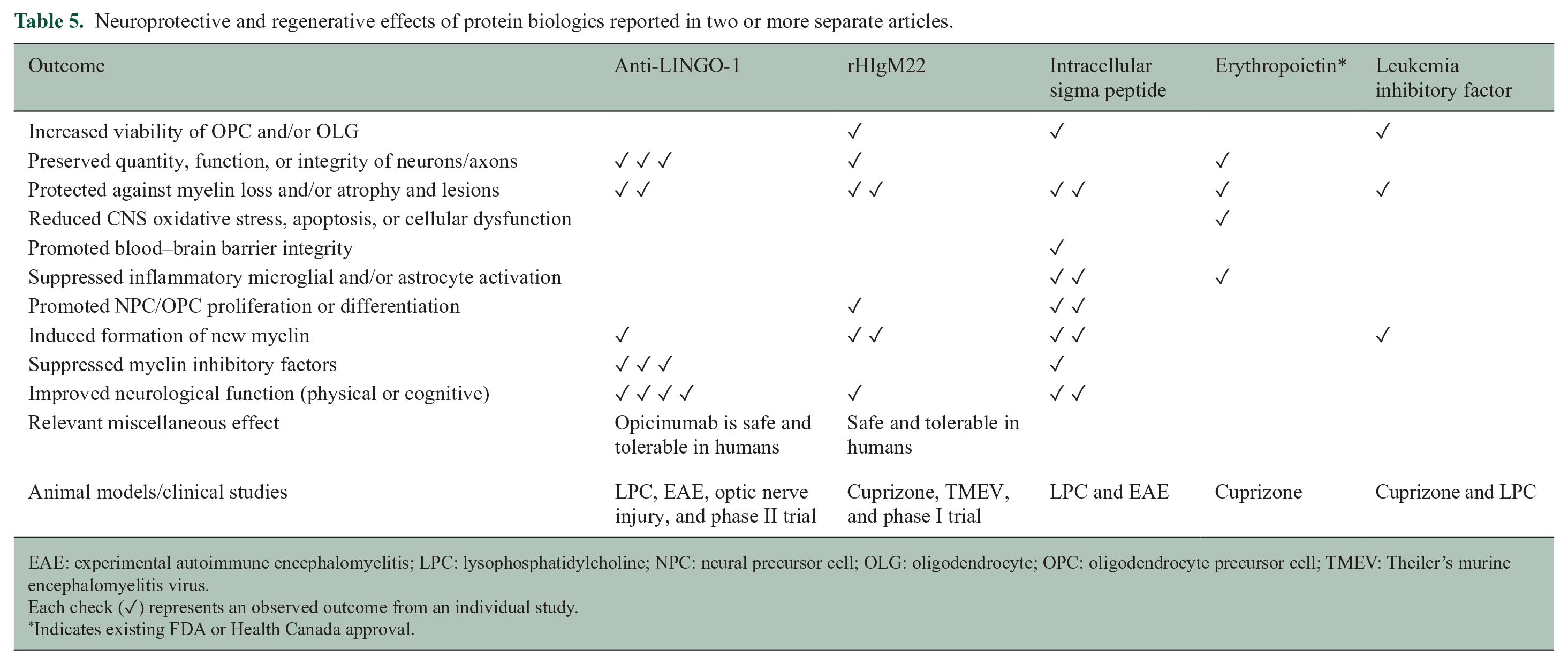
EAE: experimental autoimmune encephalomyelitis; LPC: lysophosphatidylcholine; NPC: neural precursor cell; OLG: oligodendrocyte; OPC: oligodendrocyte precursor cell; TMEV: Theiler’s murine encephalomyelitis virus.
Each check (✓) represents an observed outcome from an individual study.
Indicates existing FDA or Health Canada approval.
Antibodies
Antibody-mediated therapies act by neutralizing, depleting, or functionally blocking target macromolecules. Antibodies designed to target and deplete specific immune cell populations have successfully suppressed the peripheral immune-mediated and neuroinflammatory aspects of MS pathology in clinical practice. 27 In recent years, antibody therapies have also been developed to target neural cells and promote regeneration. Among all included reports from our search, the antibody treatment group contained the greatest proportion of drugs that had advanced to clinical trials (60%). Antibody therapies that have completed at least phase I clinical trials for MS included opicinumab (anti-LINGO-1), recombinant human (rh) IgM22, anti-Nogo-A, anti-semaphorin-4D, elezanumab (anti-RGMa), and temelimab (anti-pHERV-W envelope protein).
Peptide mimetics and decoys
Four peptide mimetic/decoy interventions were reported, including one report of the approved MS immunomodulatory drug glatiramer acetate (GA, Copaxone®). GA was evaluated in an observational human trial that reported null effects of treatment on serum BDNF levels and MRI measures of neuroregeneration in RRMS patients. 28 Two other peptide mimetics were designed to (1) reduce glutamate-induced neuronal excitotoxicity and (2) promote OPC differentiation and migration via semaphorin-3A signaling in EAE and cuprizone studies, respectively.29,30 In EAE and LPC animal models, pharmacological blockade of the chondroitin sulfate proteoglycan (CSPG) receptor, tyrosine-protein phosphatase sigma (PTPσ), by a synthetic domain mimic, intracellular sigma peptide (ISP), reduced gliosis and promoted OPC survival, proliferation, maturation, and axon remyelination31,32 (Table 5). Currently, NVG-291, a close analog of ISP developed by NervGen Pharma, is in preparation for clinical trials in spinal cord injury and MS.31–33
Growth and regulatory factors
Among the reported protein-based interventions, 31.8% investigated the effects of various growth factors and regulatory proteins on neurological outcomes in EAE, cuprizone, and LPC-induced demyelination models. The majority of interventions in this class involved the administration of either hematopoietic or neurotrophic factors, which modulated key signaling pathways regulating immune, neuronal and glial cell activity, and survival. The neuroregulatory effects of erythropoietin and leukemia inhibitory factor were each reported in two separate preclinical studies and are summarized in Table 5.
Inhibitors and proteases
Seven studies reported beneficial effects in preclinical models of MS following treatment with protein inhibitors and proteases. Two of these proteins were derived from animal secretions. Apamin, a neurotoxic peptide isolated from honeybee venom, conferred protection to myelin in the cuprizone model 34 and has completed a phase II trial for Parkinson’s disease (NCT01341431). Ancrod, a thrombin-like serine protease isolated from Malayan pit viper venom, accelerated remyelination in the LPC model. 35 In addition, an engineered selective analogue and inhibitor of soluble tumor necrosis factor, XPro1595, is the focus of an ongoing phase I trial for Alzheimer’s disease (NCT03943264). In the cuprizone model, XPro1595 promoted clearance of myelin debris, which enabled earlier remyelination and ameliorated motor function impairments. 36
Cellular biologics
Twenty-five reports investigated cell-based biologic interventions in EAE and chemical demyelination models, as well as in one human study (Table 6). Three main groups of transplanted cells were identified in our search: mesenchymal stem cells (MSCs, 14 reports), neural or glial precursor cells (NPCs, 10 reports), and embryonic stem cells (1 report). The preclinical studies obtained in our search described numerous neuroprotective and regenerative effects of cellular therapies (summarized in Table 6). These animal data indicate that transplanted MSCs exert beneficial effects partly through their immunomodulatory actions in the periphery when administered systemically and as they infiltrate the CNS. 37 By contrast, the included phase I clinical trial of MSC transplantation in people with RRMS and secondary progressive (SP) MS reported no significant changes in diffusion tensor imaging (DTI) parameters as a result of treatment. 38 Among reported NPC-based therapies, multiple strategies involved the transduction of these cells with neurotrophic genes prior to administration to support engraftment and differentiation to neural lineages.39–41 To date, no NPC therapy has been approved for routine use in MS, but a number of phase I and II trials in progressive MS are ongoing or completed (NCT03269071 and NCT03355365).
Reported neuroprotective and regenerative effects of cellular biologics in animal models of MS.
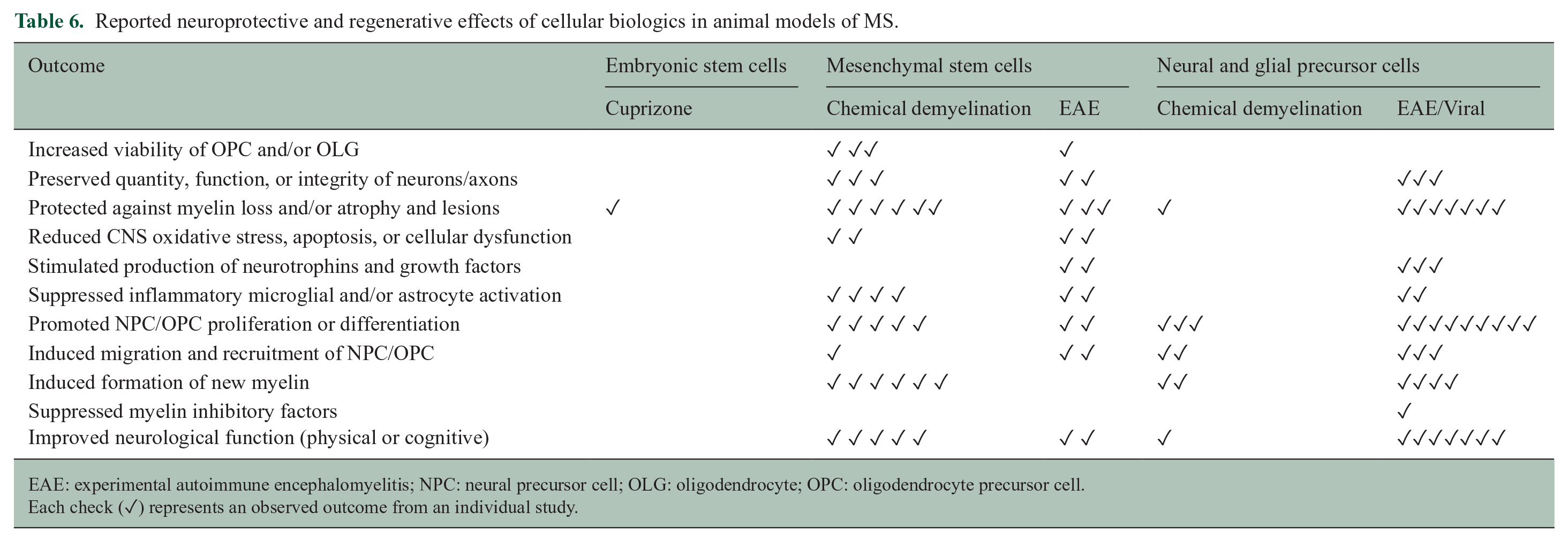
EAE: experimental autoimmune encephalomyelitis; NPC: neural precursor cell; OLG: oligodendrocyte; OPC: oligodendrocyte precursor cell.
Each check (✓) represents an observed outcome from an individual study.
RNA biologics
Five reports described the use of RNA therapies in preclinical models of MS (LPC, EtBr, cuprizone, and EAE), wherein the treatments involved RNA-based approaches to target inhibitors of OPC differentiation and remyelination (Table 7). Four reports described the neuroregenerative effects of targeting LINGO-142,43 and Nogo-A receptor 1 (NgR1)44,45 using gene silencing approaches with small interference RNA (siRNA) and short hairpin RNA (shRNA). An additional report evaluated the impact of administering exogenous microRNA sequence copies in an EAE model. 46 MicroRNA-146a suppresses inhibitory signaling involved in OPC differentiation and, in this preclinical study, supplemental treatment reduced clinical disability, induced M2-like microglial polarization, and promoted OPC differentiation and remyelination. 46
Reported neuroprotective and regenerative effects of RNA and lipid biologics in preclinical studies.
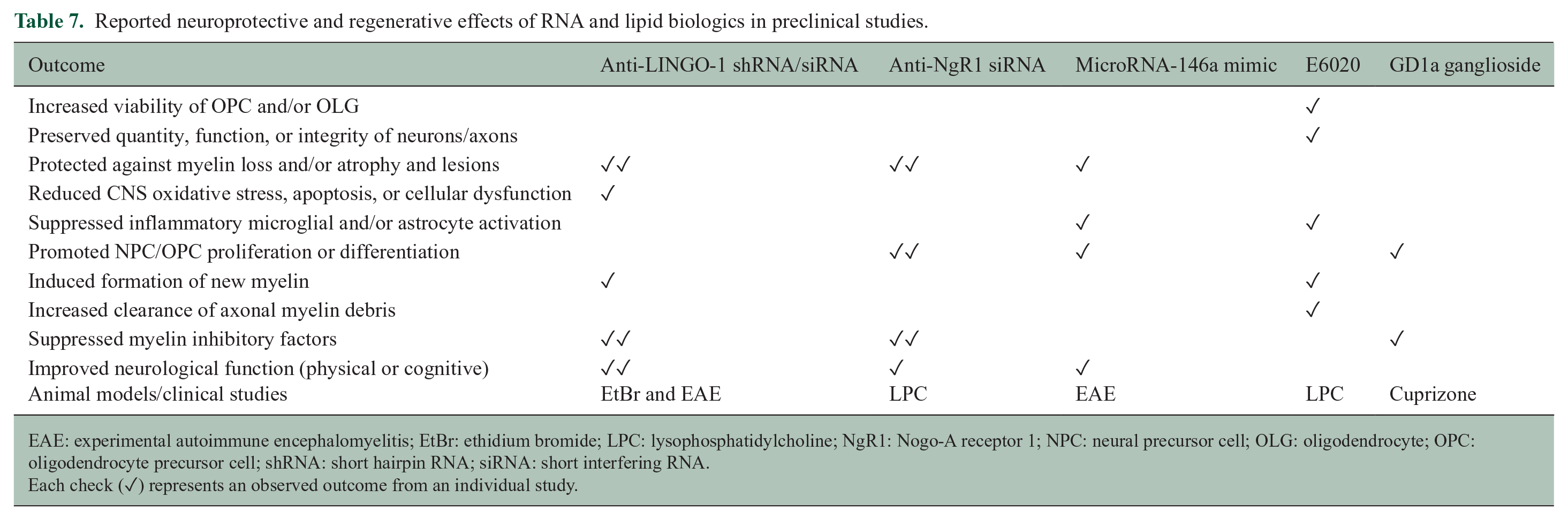
EAE: experimental autoimmune encephalomyelitis; EtBr: ethidium bromide; LPC: lysophosphatidylcholine; NgR1: Nogo-A receptor 1; NPC: neural precursor cell; OLG: oligodendrocyte; OPC: oligodendrocyte precursor cell; shRNA: short hairpin RNA; siRNA: short interfering RNA.
Each check (✓) represents an observed outcome from an individual study.
Lipid biologics
Two reports detailed the neurological effects of lipid-based biologic interventions in preclinical MS models (Table 7). The first study treated LPC-demyelinated animals with the immunomodulatory lipid A mimetic and toll-like receptor 4 agonist E6020. 47 The second treated cuprizone-demyelinated animals with ganglioside GD1a, which promotes OPC maturation by inhibiting fibronectin and integrin interactions. 48
Inorganic compounds
A single report evaluated the therapeutic benefits of lithium carbonate (Li2CO3) in a pilot clinical trial of male and female participants with a progressive form of MS. 49 The study assessed the safety and effects of daily administration of low-dose Li2CO3 (concurrent with DMTs) on disability, lesion volume, parenchymal brain volume, general well-being, and relapse rate over 1–2 years. Li2CO3 treatment was well tolerated and produced a nonsignificant trend toward reduced brain atrophy and stable disability scores but did not impact relapse rates. The authors note that larger follow-up studies are needed to expand upon and confirm these findings.
Dietary interventions
Five studies evaluated the neurological effects of some form of dietary intervention, which was defined as an alteration of the quantity of one or more components of the diet. Two articles investigated the benefits of enriching cuprizone rodent chow with the omega-3 fatty acids docosahexaenoic and eicosapentaenoic acid.50,51 The effects of dietary cholesterol were also studied in EAE, cuprizone, and LPC demyelination models. 52 Two additional reports evaluated the efficacy of intermittent fasting in EAE, EtBr, and cuprizone models,53,54 as well as in a pilot clinical trial assessing feasibility for application in RRMS (NCT01538355). The neuroprotective and regenerative effects of these dietary interventions are presented in Table 8.
Reported neuroprotective and regenerative effects of dietary and physiological interventions in preclinical and clinical studies.
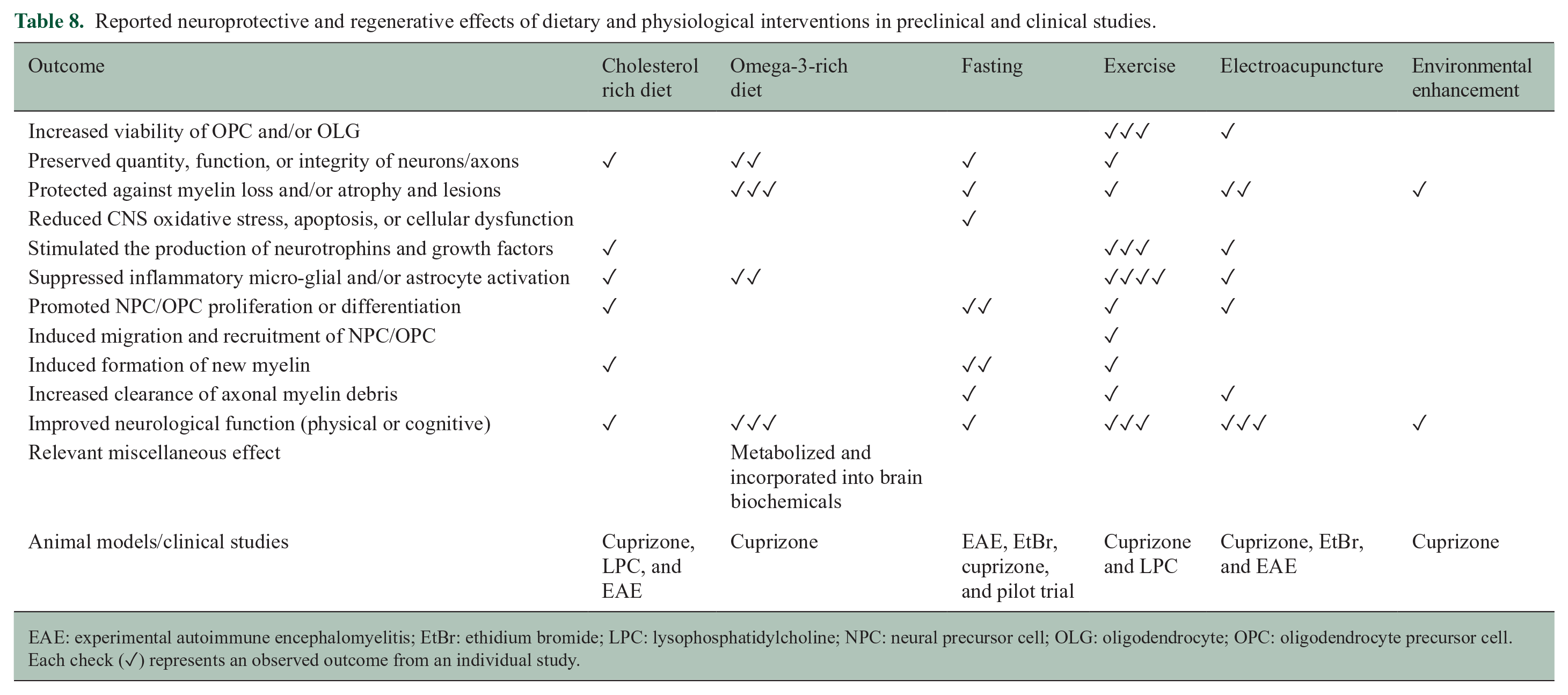
EAE: experimental autoimmune encephalomyelitis; EtBr: ethidium bromide; LPC: lysophosphatidylcholine; NPC: neural precursor cell; OLG: oligodendrocyte; OPC: oligodendrocyte precursor cell.
Each check (✓) represents an observed outcome from an individual study.
Physiological and environmental interventions
Ten reports evaluated the impact of physiological interventions in preclinical models of MS (Table 8). Interventions within this class covered non-pharmacological strategies such as exercise, electrical stimulation, and modification of the environment and social behavior. Voluntary exercise in LPC and cuprizone models was reported to suppress glial inflammation, promote oligodendrogenesis, and improve motor function, among other effects.55–57 The physiological effects of exercise are wide-reaching and, similar to dietary modifications, could be beneficial as an adjunct therapy in MS for disease management and to promote general well-being.
Discussion
The effectiveness of immunomodulatory treatments for MS and, in particular, relapsing forms of MS, has signified the role of neuroinflammation in disease initiation and subsequent neurodegeneration. At present, immunomodulatory small molecule drugs and monoclonal antibodies are the most effective available DMTs for the clinical management of RRMS. 58 The performance of these medications in progressive forms of MS, however, has been underwhelming and inadequate; 59 a reflection of the distinct cellular processes underlying progressive neurodegeneration as compared to inflammatory relapses. 60 Transition to secondary progressive MS over time is a common occurrence for individuals with relapsing MS,58,59 highlighting the need for treatment strategies that both promote CNS remyelination and protect from further immune-mediated demyelination and degeneration. Our systematic review aimed to consolidate findings from the most recent studies that have specifically evaluated strategies devised to promote oligodendrogenesis through recruitment and differentiation of NPCs and OPCs, promote remyelination and/or neuronal and axonal integrity, or that were able to reduce the pro-inflammatory activity of glial cells, expression of inhibitory factors, oxidative stress, cellular dysfunction and/or apoptosis (summarized in Figure 1). Our systematic review of the literature produced 221 articles of relevance that evaluated 262 intervention strategies in preclinical models or clinical trials for MS.
The most highly represented class of treatment strategies comprised small molecule drugs, followed by antibody therapies and stem cell transplantation (Figure 4). Interestingly, 13 of 23 small molecule drugs that were repeatedly evaluated in the included studies are already FDA-approved for MS or other conditions. FDA-approved treatments can be more readily adapted to MS and obviate resource and time-intensive clinical trials, as they have known risk profiles and well-described side effects and counterindications. Among the included FDA-approved small molecules identified in our search, fingolimod was the most frequently reported drug to exert beneficial effects on myelin integrity and repair in several preclinical models of MS (Table 2). As fingolimod is a known immunomodulatory drug, 58 further elucidation is required to distinguish its direct and indirect neuroregenerative properties. Increased knowledge of the mechanisms of action will help determine the optimal timing and dosing of fingolimod to maximize its dual benefits and ascertain its suitability as an adjunct therapy in progressive MS. Many reported FDA approved small molecules that act directly on neurons and axons were adapted from other neurological disorders to investigate their MS-relevant effects, including pregabalin, 4-aminopyridine, lithium, nimodipine, benztropine, phenytoin, and a Sativex-like formula (Tables 2 and 3). The MS drugs dimethyl fumarate and laquinimod both demonstrated neuroprotective effects in cuprizone demyelination models61–64 (Table 2) and, although not yet approved, laquinimod has completed a phase III clinical trial for RRMS (NCT01047319). Multiple studies reported neuroregenerative effects of small molecule drugs that are in current use for other diseases and conditions, such as clobetasol (anti-inflammatory),65,66 clemastine fumarate (anti-allergy),55,67 miconazole (anti-fungal),65,66 and metformin (anti-diabetic).54,68,69 These drugs were all reported to promote remyelination and reduce clinical disability following chemical demyelination in preclinical studies (Tables 2 and 3). A number of reports detailed positive effects of organic compound mixture therapies on neurological outcomes in animal models of MS, though additional investigation will be necessary to validate the neuroprotective and regenerative effects of the individual components before they can be evaluated in clinical trials.
The antibody therapies identified in our search produced multiple favorable effects in both preclinical models and clinical trials by modulating neural and glial targets to promote myelin repair. The recombinant version of a serum-derived human IgM antibody, rhIgM22, which is known to bind to and promote oligodendrocyte process outgrowth (Supplementary Table S5F), was reported to induce remyelination and protect neurons in cuprizone-induced demyelination models70–72 (Table 5). rhIgM22 was likewise safe and tolerable in a phase I trial for RRMS 73 (NCT01803867). Another promising protein therapy is opicinumab, the monoclonal antibody that neutralizes the myelin inhibitory factor LINGO-1. In preclinical models, LINGO-1-targeted antibody therapy conferred protection to axons and enhanced remyelination74–76 (Table 5). Although opicinumab treatment was well tolerated and safe in a phase II clinical trial, it did not improve disability among individuals with an active relapsing form of MS 77 (NCT01864148). However, in a separate trial for individuals with optic neuritis, Opicinumab demonstrated beneficial effects on optic nerve function 78 (NCT01721161). Taken together, the current evidence supports the pursuit of antibody-mediated therapies as neuroprotective and neuroregenerative treatments in MS. However, additional research will be required to confirm the clinical benefits of such strategies.
Cell-based therapies are a promising approach for stimulating repair in neurodegenerative diseases such as MS. Transplantation of mesenchymal and CNS-derived precursor cells has the potential to exert both neuroprotective and neuroregenerative effects through various mechanisms. 79 NPCs have the intrinsic potential to replace damaged oligodendrocytes and promote remyelination, 80 which is particularly important for progressive and advanced forms of MS marked by extensive neurodegeneration. Moreover, transplanted NPCs can promote the repair process in the injured CNS through paracrine effects by secreting a host of growth factors and neurotrophins important for endogenous oligodendrogenesis and remyelination. 80 Despite their potential, the administration route for NPCs has been a limiting factor for translational application in MS. NPCs are most effective at cellular replacement if delivered intra-parenchymally in the vicinity of CNS lesions, which requires targeted surgical intervention. Thus, more attention has been directed to autologous MSC transplantation for the treatment of MS, as these cells can be delivered systemically through intravenous or intrathecal routes.79,81 Overall, cellular biologic therapies are considered a technically complicated approach with a greater risk of adverse effects, thus requiring additional optimization before widespread use in clinical practice. 82
Pharmaceuticals that affect lipid metabolism, and therefore potentially myelin formation, are logical candidates for therapeutic development in MS. Our search identified several such candidates, including sobetirome,66,83 T3 hormone83–85 (Table 4), ellagic acid86,87 (Table 3), the protonophore MP101/201,22,23 and the lipids E6020 47 and GD1a ganglioside 48 (Table 7). Furthermore, the positive effects of some dietary interventions were ascribed at least in part to alterations of metabolism, including vitamin and metabolite supplementation (Table 4), dietary cholesterol 52 and omega-3 fatty acid enrichment,50,51 and the application of intermittent fasting53,54 (Table 8). Studies included in our search that employed dietary or physiological interventions were underrepresented as compared to pharmaceutical-based strategies. Nevertheless, non-pharmacological treatments are being increasingly recognized as valuable adjunct interventions when designing comprehensive neuroregenerative therapies.88,89 Exercise, socialization, and nutritional modifications demonstrated both neuroprotective and regenerative effects in animal models of MS55–57,90,91 (Tables 7 and 8), and the many beneficial effects of plant-derived organic compound formulations24–26,92–95 further supports integrating dietary modifications into MS treatment regimens. Although many non-pharmacological strategies are multifactorial, and are therefore more difficult to evaluate for direct effects on specific outcomes in individuals with MS, their minimal associated risks and practical ease of implementation are attractive features for use in the management of MS. The success of these strategies, however, requires the provision of clear and consistent evidence-based recommendations practiced under the supervision of qualified professionals in order for persons with MS to make therapeutically effective dietary and lifestyle modifications that encourage adherence.96,97 Importantly, non-pharmacological strategies can be less financially burdensome than many standard DMTs. Given that the cost of monoclonal antibody therapies, such as ocrelizumab and natalizumab, is estimated at $30,000 per annum in Canada, 98 the inclusion of non-pharmacological approaches could partly reduce the economic hurdle of achieving therapeutically significant results. As such, socioeconomic considerations informed by the demographic data of individuals with MS should be accounted for in the selection of preclinical strategies for clinical development to provide inclusive access to treatment.
Perhaps, unsurprisingly, the vast majority of data included in our screen was obtained from preclinical animal models, representing over 90% of the study designs (Figure 3). Among the available experimental models for MS, chemical demyelination methods (cuprizone, LPC, and EtBr) were employed in the majority of studies. The advantage of these models is that demyelination and remyelination occur in temporally reproducible patterns with minimal involvement of peripheral immune cells (Supplementary Table S4). Despite their advantages, the pitfalls and applicability of established animal models of MS is an ongoing topic of discussion concerning translation to clinical practice. 99 Reported methods used in the included preclinical studies to dissect mechanism often lacked clear feasibility for translation due to invasive or complicated administration protocols and high doses or frequency of treatments. The lack of reporting of tolerability and potential adverse side effects that are either undetectable in some animal models or that are overlooked in the early stages of drug identification was also concerning. Moreover, there was a consistent risk of bias among preclinical and clinical studies related to the reporting of treatment and outcome blinding and sample size calculations (Table 1). These are critical gaps, in particular, for consistent evaluation of behavioral and clinical outcomes, which are largely subjective and can be prone to unconscious bias. 100 The creation of standardized protocols for randomization, blinding, treatment endpoints, and effective methods for assessing regenerative treatment safety and efficacy in preclinical MS models could substantially reduce variability, ambiguity, and bias in reporting. 101 These preclinical measures would also augment reproducibility and the level of evidence needed to justify advancement to resource-intensive clinical trials. While blinding measures were more thoroughly reported in clinical trial designs, more sensitive and precise imaging techniques are needed to directly monitor and measure the efficacy of remyelinating therapies in individuals with MS over time. 102
In conclusion, the increasing number of studies that have recently evaluated neuroprotective and neuroregenerative interventions in MS underscores the shared impetus of researchers and clinicians to address the unmet need for effective treatments in late-stage and progressive MS. Although there has been considerable progress in this area, the collective data illustrate a skewed representation of the types of strategies that advance from preclinical models to clinical trials that heavily favors antibody and small molecule-based therapies over other intervention types. This may be due to the inherent issues in the administration of other potential therapeutic strategies (e.g. diet and exercise) in a controlled trial design that may lead to difficulties in the interpretation of results. In addition, our findings point to inherent challenges in translating the outcomes of animal studies, as well as to practical barriers to assessing and implementing experimental treatments in clinical settings. Accordingly, further research is required to address the challenges of translating preclinical findings.
Supplemental Material
sj-pdf-1-msj-10.1177_13524585211008760 – Supplemental material for Current status of neuroprotective and neuroregenerative strategies in multiple sclerosis: A systematic review
Supplemental material, sj-pdf-1-msj-10.1177_13524585211008760 for Current status of neuroprotective and neuroregenerative strategies in multiple sclerosis: A systematic review by Jessica R Allanach, John W. Farrell, Miceline Mésidor and Soheila Karimi-Abdolrezaee in Multiple Sclerosis Journal
Footnotes
Author Contributions
M.M. designed the search strategy, composed keyword strings, and identified articles from queried databases. J.F. and J.R.A. served as reviewers for article screening. J.F. composed the background information. M.M., J.F., and J.R.A. performed data extraction. J.R.A. compiled extracted data and summarized results. S.K.-A. conceptualized the review, oversaw manuscript preparation, and interpreted results for discussion.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the endMS Research and Training Network, Scholar Program for Researchers in Training (SPRINT), and the MS Society of Canada. J.R.A. is supported by an endMS Doctoral Studentship Award from the MS Society of Canada. J.F. is supported by the uOttawa/Children’s Hospital of Eastern Ontario Research Institute Collaborative Initiative Postdoctoral Fellowship. M.M. is supported by the Fonds de Recherche du Québec-Santé (FRQS) PhD fellowship. S.K.-A is supported by the MS Society of Canada (EGID-3742) and the Canadian Institute of Health Research (Grant ID 156218).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.