
Abstract
Background:
Autologous haematopoietic stem cell transplantation (AHSCT) is an effective treatment for patients with multiple sclerosis (MS) who have highly active disease, despite the use of standard disease-modifying therapies (DMTs). However, the optimal time for offering AHSCT to patients with ‘aggressive’ MS is yet to be established.
Objectives:
The objective was to explore the safety and efficacy of AHSCT as a first-line DMT in patients with ‘aggressive’ MS.
Methods:
All patients with ‘aggressive’ MS who received AHSCT as a first-line DMT in five European and North American centres were retrospectively evaluated.
Results:
Twenty patients were identified. The median interval between diagnosis and AHSCT was 5 (1–20) months. All had multiple poor prognostic markers with a median pre-transplant Expanded Disability Status Scale (EDSS) score of 5.0 (1.5–9.5). After a median follow-up of 30 (12–118) months, the median EDSS score improved to 2.0 (0–6.5, p < 0.0001). No patient had further relapses. Three had residual magnetic resonance imaging (MRI) disease activities in the first 6 months post-transplant, but no further new or enhancing lesions were observed in subsequent scans.
Conclusion:
AHSCT is safe and effective as a first-line DMT in inducing rapid and sustained remission in patients with ‘aggressive’ MS.
Keywords
Introduction
Multiple sclerosis (MS), a chronic immune-mediated disorder of the central nervous system, is characterised by inflammation, demyelination, oligodendrocyte death and neuronal loss. 1 Its disease course is variable, but most patients present with a relapsing–remitting form. 2 Various natural history studies showed that male gender, late age of onset, shorter interval between first and second relapses, incomplete recovery from the first relapse and frequent relapses in the first 2 years following symptom onset were associated with poor prognosis.3–8 Higher Disability Status Scale (DSS) scores at the second and fifth year from disease onset, denoting early accumulation of disability, has also been associated with worse prognosis.4–8 Therefore, MS seems to set its trajectory early in its course. In addition, clinical and radiological disease activity in the infratentorial region of the brain and in the spinal cord has found to be a poor prognostic factor.9,10
A small proportion of patients with MS have an extremely active disease with early accumulation of fixed disabilities being the hallmark of their disease course. Various terms have been used to describe this phenotype, including ‘aggressive’, ‘malignant’ and ‘fulminant’ MS. These patients do not respond adequately to first-line disease-modifying therapies (DMTs) and should therefore be treated early with one of the higher efficacy DMTs, although a high proportion of them do not respond optimally to these agents.11–16
Autologous haematopoietic stem cell transplantation (AHSCT) has gained considerable interest in recent years as an efficacious therapy for a selected group of patients with MS who have clinically and radiologically active disease, despite the use of standard DMTs. 17 Treatment-related mortality has reduced significantly in the last two decades through better patient selection, optimisation of transplant technique and increased centre experience.18–20 To date, there have been no published studies assessing the safety and efficacy of AHSCT as a first-line therapy in patients with ‘aggressive’ MS, although a Swedish case series of 48 patients included four who were ‘treatment naïve’ before receiving AHSCT. 21 Here, we report the cumulative experience of five international centres using AHSCT as a first-line DMT in patients with ‘aggressive’ MS.
Methods
Subjects and inclusion criteria
This is a retrospective study in which all patients with ‘aggressive’ MS, as deemed by their treating clinicians, who underwent AHSCT as a first-line DMT in Sheffield (United Kingdom), Uppsala (Sweden), Ottawa (Canada), Chicago (United States) and Florence (Italy), were identified and included. The diagnosis of MS was made using the most contemporary version of the McDonald criteria at the time. No pre-defined definition of ‘aggressive’ MS was used, but patients needed to have had clinical and radiological features in keeping with aggressive clinical course with poor prognostic markers which led their clinicians treating them with AHSCT in preference to high-efficacy DMTs. No patient received any standard DMTs before AHSCT, which was therefore considered a first-line treatment. Retrospective review of the medical records was performed to gather demographic details, disease-related characteristics and outcome measurements.
Procedure
Peripheral blood stem cells were mobilised with cyclophosphamide (2–4.5 g/m2) and granulocyte colony-stimulating factor (5–10 µg/kg/day). The following transplantation regimens were used based on centre preference: (1) busulfan, cyclophosphamide 200 mg/kg and rabbit anti-thymocyte globulin 6 mg/kg (Bu-Cy-ATG) with CD34-selected autograft; (2) BCNU (carmustine) 300 mg/m2, etoposide 800 mg/m2, cytosine arabinoside 800 mg/m2, melphalan 140 mg/m2 and rabbit anti-thymocyte globulin 7.5–10 mg/kg (BEAM-ATG) with unmanipulated autograft; or (3) cyclophosphamide 200 mg/kg and rabbit anti-thymocyte globulin 6–7.5 mg/kg (Cy-ATG) with unmanipulated autograft. Detailed descriptions of the transplant procedures had previously been published.21–23
Outcome measurements and statistical analysis
Treatment outcome was assessed using no evidence of disease activity (NEDA), defined as the absence of clinical relapses, confirmed disability progression and magnetic resonance imaging (MRI) disease activity. 24 Relapse was defined as new or worsening symptoms lasting for ⩾24 hours with objective signs confirmed on neurological examination. For the purpose of this analysis, MRI studies which were performed within the first 6 months post-AHSCT were used as re-baseline images. 24 Disability was measured using the Kurtzke Expanded Disability Status Scale (EDSS) score. 25 Confirmed disability progression was defined as an increase in the EDSS score of ⩾1.0 point from the baseline (last EDSS before AHSCT) if the baseline EDSS was ⩽5.5 points, or an increase of ⩾0.5 point if the baseline EDSS was >5.5 points, which persisted over a 12-month period. The Wilcoxon signed-rank test was used to assess statistical difference between the median EDSS score at the baseline and the last follow-up post-AHSCT.
Results
A total of 20 patients with ‘aggressive’ MS who received AHSCT as a first-line DMT were identified from five centres (Table 1). There was an equal proportion of male and female with a median age of 28 (17–47) years at diagnosis and a median interval of 5 (1–20) months between diagnosis and treatment. The median last EDSS score before transplant was 5 (1.5–9.5). All patients had aggressive clinical course with multiple clinical and radiological features suggestive of poor prognosis, including multiple clinical relapses with incomplete recovery, high EDSS scores and numerous new, enlarging or gadolinium-enhancing MRI lesions on multiple occasions particularly in the brainstem, cerebellum and spinal cord (Tables 1 and 2).
Demographic and disease-related characteristics.
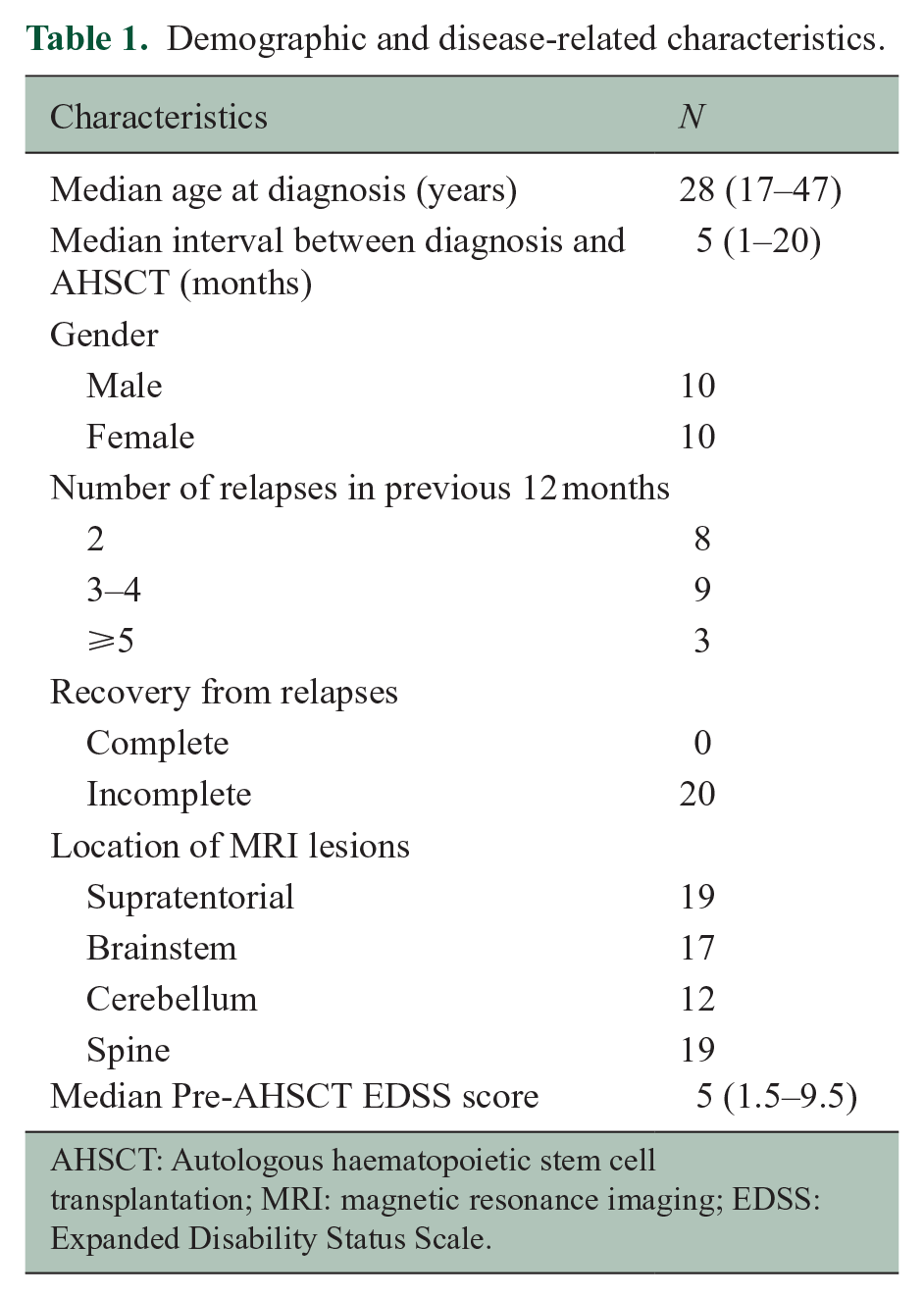
AHSCT: Autologous haematopoietic stem cell transplantation; MRI: magnetic resonance imaging; EDSS: Expanded Disability Status Scale.
Summary of treatment outcomes.
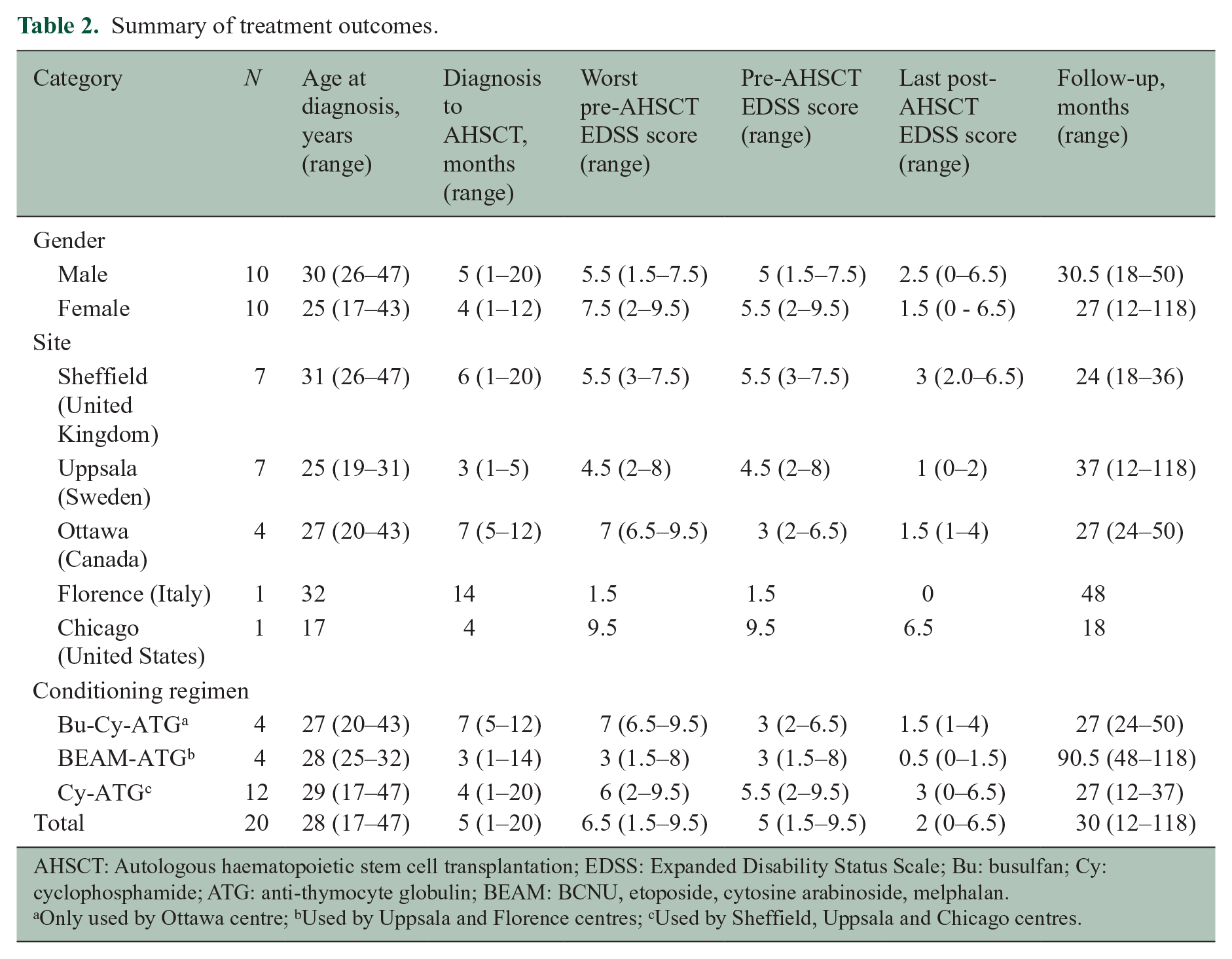
AHSCT: Autologous haematopoietic stem cell transplantation; EDSS: Expanded Disability Status Scale; Bu: busulfan; Cy: cyclophosphamide; ATG: anti-thymocyte globulin; BEAM: BCNU, etoposide, cytosine arabinoside, melphalan.
Only used by Ottawa centre; bUsed by Uppsala and Florence centres; cUsed by Sheffield, Uppsala and Chicago centres.
Three conditioning regimens, Bu-Cy-ATG, BEAM-ATG and Cy-ATG were used in 4, 4 and 12 patients, respectively, reflecting local treatment practices (Table 2). Autologous stem cell re-infusions were unmanipulated in 16 patients, and CD34 selection was performed in the remaining 4 patients. The median follow-up period was 30 (12–118) months. Post-transplant median EDSS score at the last follow-up appointment was 2.0 (0–6.5) (Table 2). The EDSS score of one patient did not change after the treatment. Another patient had a transient increase, despite the overall improvement of their EDSS score following AHSCT. None of these patients experienced confirmed disability progression (Figure 1(a) and (b)). EDSS scores of 13 patients plateaued after the initial 6 months, whereas scores of 5 patients continued to improve beyond this period (Figure 1(a)). Median improvement of the EDSS score was 2.25 (0–6.5), which was statistically significant (p < 0.001, Wilcoxon signed-rank test) (Figure 1(b)). Subgroup analysis showed that this improvement was also statistically significant in males (p = 0.005) and females (p = 0.008), and in patients treated with the Cy-ATG conditioning regimen (p = 0.003) (Table 2).
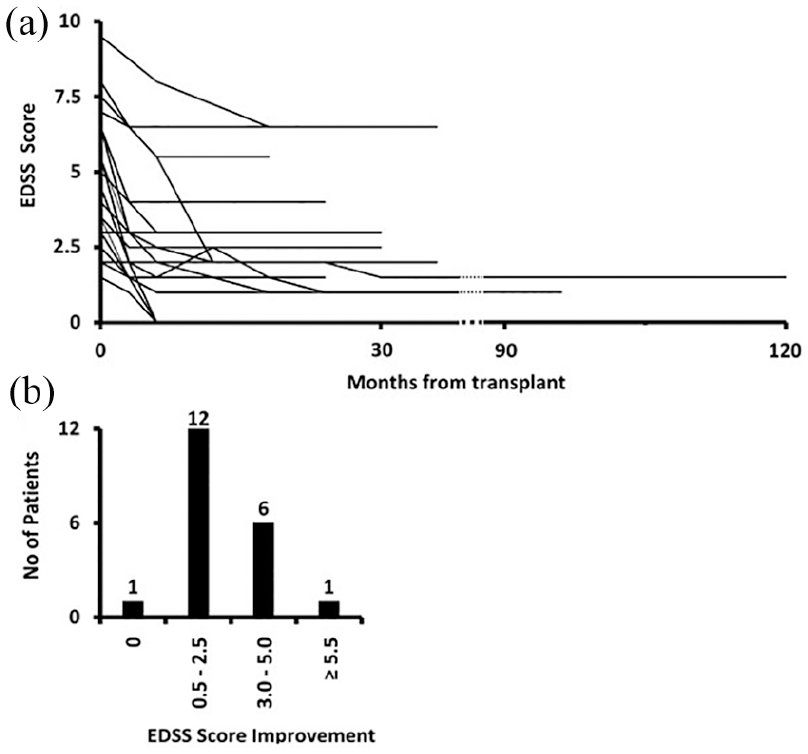
Impact of AHSCT on disability progression. (a) Each line represents change in the EDSS score of one patient during the follow-up period. (b) The improvement of EDSS scores in our cohort.
Seventeen patients had no new, enlarging or gadolinium-enhancing MRI lesions following AHSCT. Three patients had new lesions with or without gadolinium enhancement on their first MRI scans, which were performed within 6 months post-AHSCT; one had two new T2 lesions, one had a new T2 and a new gadolinium-enhancing lesions and one had a single new gadolinium-enhancing lesion. However, serial scans during their subsequent follow-ups (currently 23, 36 and 84 months) did not show any new lesion or gadolinium enhancement. Bu-Cy-ATG, BEAM-ATG and Cy-ATG were used as the conditioning regimen in one patient each. No clinical relapse following treatment with AHSCT was seen in any of these 20 patients. Overall, NEDA was 85% with a median follow-up period of 30 (12–118) months, but 100% after re-baselining MRI disease activities to month 6 post-transplant scans.
Expected transplant-related toxicities were reported, but there were no grade 4 toxicities or treatment-related mortality (Table 3). Thyroid disorders were the only secondary autoimmune conditions that were observed in this cohort. In total, 20% of patients developed hypothyroidism or hyperthyroidism following AHSCT. There was no reported secondary malignancy. One female patient conceived naturally 7 months after AHSCT and gave birth to a healthy baby. Another male patient’s partner conceived 22 months after AHSCT and delivered a healthy baby.
Early and late complications associated with AHSCT.
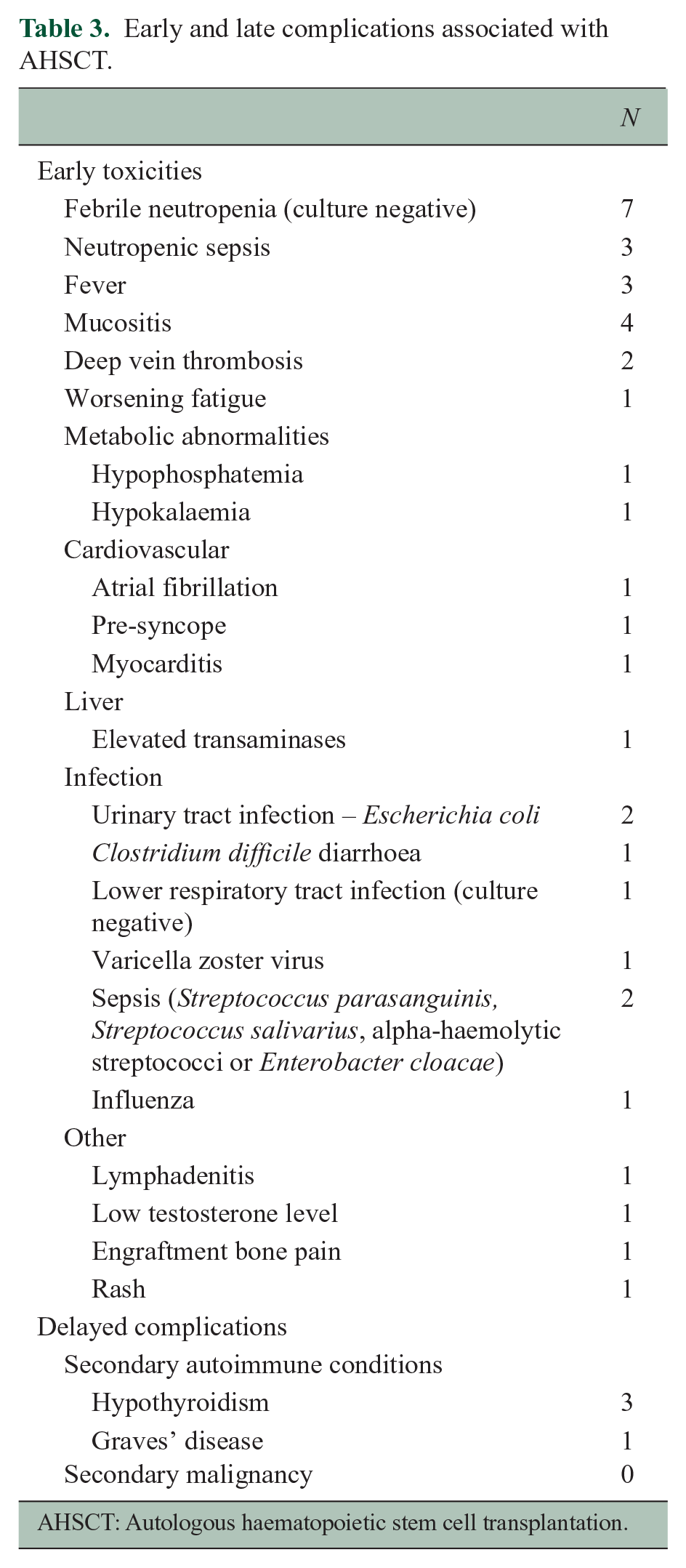
AHSCT: Autologous haematopoietic stem cell transplantation.
Discussion
We present a small cohort of patients with multiple clinical and radiological features predictive of ‘aggressive’ MS who received AHSCT as a first-line DMT. Aggressive clinical course, poor prognostic markers together with the lack of response to multiple courses of corticosteroids and plasma exchanges led their clinicians to treat them with AHSCT in preference to high-efficacy DMTs. All patients were assessed and treated in centres experienced in using AHSCT to treat MS, and balanced therapeutic decisions were made on an individual basis to proceed with this treatment.
There are no universally accepted diagnostic criteria which would allow an early prospective identification of patients with ‘aggressive’ MS. Rush et al. 16 have recently suggested that ‘aggressive’ MS could be defined as relapsing–remitting MS with one or more of the following features: (1) EDSS score of 4 within 5 years of disease onset, (2) two or more relapses with incomplete recovery in the past 12 months, (3) three or more MRI studies showing new or enlarging T2 lesions or gadolinium-enhancing lesions despite treatment and (4) unresponsive to one or more DMTs for up to 1 year. When these criteria were applied to our cohort retrospectively, 18 patients satisfied the definition of ‘aggressive’ MS at the time of their transplant. Although the remaining two patients did not fulfil these criteria, both had multiple poor prognostic markers, including large number of new and gadolinium-enhancing MRI lesions on multiple time points, leading their treating clinicians to offer AHSCT as a first-line therapy. Although a number of other definitions have been proposed for ‘aggressive’ MS, in clinical practice, this diagnosis is often made retrospectively.11,13,26,27 If the diagnosis of this phenotype is only made retrospectively, valuable time would be lost during which unsuccessful and sometimes futile therapeutic attempts would be made using standard DMTs, while disability will progress significantly and become irreversible, potentially compromising the feasibility, safety and efficacy of AHSCT at a later stage.
Although neuroinflammation and neurodegeneration occur concomitantly in MS, the initial relapsing–remitting phase of this illness is thought to be driven by inflammation, whereas the late stage is dominated by neurodegeneration leading to a progressive neurological dysfunction with or without superimposed relapses. 1 Various natural history studies have shown that disability progresses independent of relapses once a critical DSS/EDSS score is reached.4–8 It has been suggested that disability starts to accumulate once the intrinsic reserve capacity of the neural network is completely exhausted resulting in loss of its ability to make spontaneous recovery and improve its function. 28 This disease model permits a ‘therapeutic window’ for treatment, suggesting that an early induction of disease remission would slow down disability accumulation and may even allow the neural network to functionally recover to some extent. As the ‘therapeutic window’ for the ‘aggressive’ MS is significantly narrower, a good case can be made for using AHSCT early in carefully selected patients rather than waiting for the first-line DMTs to fail and the disability to progress. Clearly, the risks of such intensive therapies with inherent potential toxicities need to be considered cautiously, even though such a strategy may pay long-term dividends by potentially delaying the transition into the progressive phase and/or preventing irreversible disability. Given the relentless progression of disease that characterises ‘aggressive’ MS, it is important that there is at least discussion between neurologists and transplant haematologists about the management of such patients at an early stage in the course of their illness.
In this small cohort, overall cumulative NEDA was 85% during a median follow-up period of 30 (12–118) months because three patients had MRI disease activity during the first 6 months post-transplantation before complete remission of the inflammatory process was achieved. Following AHSCT, no patient had clinical relapse or confirmed disability progression. When MRIs were re-baselined at 6 months, the cumulative NEDA rate was 100%, representing a steady-state efficacy unconfounded by short-term disease activity carried over from the baseline. Moreover, AHSCT not only induced rapid remission but also improved EDSS scores in 95% of patients in keeping with an improvement of their functional status. Although high-efficacy DMTs are effective in reducing clinical and radiological disease activities in patients with relapsing–remitting MS, they have a limited impact on disability progression.29–31 Standard DMTs have also found to be less effective in people with high levels of disability.29–31
Our study had a number of limitations. Due to its retrospective nature, the grading of adverse events was challenging, although there were no grade 4 toxicities. However, it is important to note that despite the severe disability experienced by some patients who required intensive care for respiratory support, all tolerated the transplantation procedure and there was no treatment-related mortality. Furthermore, the number of patients included in this study was small, three different conditioning regimens were used and there was no control group. We were therefore unable to compare the safety and efficacy of AHSCT as a first-line therapy with standard DMTs. Although a randomised controlled trial in treatment-naïve patients with ‘aggressive’ MS comparing AHSCT against the best standard of care is needed, this will not be feasible owing to the relatively rare nature of this MS phenotype, and the fact that such patients’ clinical states evolve very rapidly which require timely individualised multidisciplinary team coordinated decision-making. Alternatively, a pragmatic treatment trial or a registry-based study with well-defined criteria for ‘aggressive’ MS could help determining the best treatment approach, including patient selection and transplant technique, for this group of patients.
Conclusion
To the best of our knowledge, this is the largest cohort of patients with ‘aggressive’ MS who received AHSCT as a first-line DMT. The treatment was safe and highly effective in inducing rapid and sustained disease remission with a significant improvement of disability. Further studies are required to confirm these initial findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Joyutpal Das is a Sheffield Biomedical Research Centre (BRC) Clinical Research Fellow and funded by the National Institute for Health Research (NIHR) Sheffield BRC and Haematopoietic Stem Cell Transplantation Charitable Trust Fund. The views expressed are those of the authors and not necessarily those of the National Health Service (NHS), the NIHR or the Department of Health and Social Care.