
Abstract
Cognitive rehabilitation in multiple sclerosis (MS) aims at reducing patients’ cognitive impairments, improving their awareness and ability to take cognitive difficulties into account in their daily living. However, at this moment, more high-quality randomized trials are needed to draw conclusion about the effectiveness of cognitive interventions in MS. Although existing studies provide clear descriptions of intervention key ingredients (e.g. targeted cognitive domain as well as treatment frequency and duration) and the practical details needed to manage these key elements (e.g. restorative approaches, compensatory strategies, or environmental modifications), other crucial aspects received less attention in rehabilitation research. The aim of this topical review is to try to elucidate some critical issues that were only partly addressed and analyzed by the scientific literature: setting (center-based vs home-based) and mode (individual vs group) of the cognitive rehabilitation treatment.
Introduction
Cognitive impairment (CI) is recognized as the most disturbing and debilitating disorder in people with multiple sclerosis (PwMS), negatively affecting many aspects of their life, as level of activity and participation in daily activities, including work and social life, interaction with healthcare providers, and adherence in treatment.1–3 Overall, CI can be present in 43%–70% of adults and 30% of pediatric patients 4 and documented in all MS subtypes.5–9 Information processing speed (IPS), working memory (WM), attention, and executive functions are the major cognitive domains affected.10–13 In view of the widespread and real-world functional implications of impairment, it follows that cognitive abilities are a crucial determinant of a positive response to rehabilitation. 14 For this reason, developing treatments capable of alleviating such deficits should have priority in MS research.
Cognitive rehabilitation (CR) aims at reducing CI, improving PwMS’ awareness of cognitive difficulties and ability to consider them in their daily living while promoting positive neurobiological changes.2,15–17 Although most of the studies on CR in MS involved learning and memory-based interventions,18–24 recently, the focus has moved to other domains as IPS, executive function, and attention15,25–28 with promising evidence for the beneficial effect of intervention. 2 Furthermore, evidence suggests that the positive effects of CR may be more widespread, including quality of life, mood, and fatigue.29–35
However, at this moment, more high-quality randomized trials are needed to draw conclusion about the effectiveness of CR for PwMS.2,8,10,36 To achieve this, precise and complete reports of interventions are strongly recommended to facilitate replication by other researchers and to enable implementation into clinical practice. 37 Although existing studies provide clear descriptions of CR key ingredients (e.g. targeted cognitive domain as well as treatment frequency and duration) and practical strategies to manage those elements (e.g. restorative approaches, compensatory devices, and environmental modifications), other crucial aspects received less attention in rehabilitation research. Access to treatment may not be allowed for many patients due to various and multiple reasons (e.g. traveling cost, physical impairment, and sanitary emergency). Recent data increasingly support the role of technology in improving patients’ functioning and healthcare services efficiency.38,39 Also, given high healthcare costs due to rehabilitation admission, 40 interventions should be developed to try to reduce burden for healthcare services without decreasing the treatment quality and efficiency. Based on research and clinical evidence and organizational and technical considerations, CR might be planned considering preliminarily alternative options of care (i.e. telerehabilitation, group-based intervention) to increase the quality of life for PwMS while reducing the financial burden. This topical review tries to elucidate some critical issues that were only partly addressed and analyzed by the scientific literature: setting (center-based vs home-based) and mode (individual vs group) of CR treatment.
Search strategy
A general search for relevant published literature of the online database PubMed was undertaken. Studies fulfilling our selected criteria and published between 1998 and 2020 were evaluated for possible inclusion in the narrative review. The search combined the following terms: multiple sclerosis (MS), CR, cognitive training, cognitive stimulation matching with home-based, center, individual, or group. The articles have been evaluated according to the title, abstract, and main text. Overall, we reviewed 224 studies. Only clinical trials, randomized controlled trial (RCT), and pilot studies were considered. Then we eliminated articles according to the following exclusion criteria: (1) not cognitive intervention (e.g. pharmacological, aerobic exercise, dual task, psychotherapy, and occupational therapy), (2) other treatment modalities in adjunction to CR (e.g. transcranial direct current stimulation), (3) studies that did not include a neuropsychological assessment to quantify any changes occurred (4) studies that did not include PwMS, (5) studies with pediatric participants, (6) non-English language articles, (7) case reports, and (8) reviews. Thus, 46 articles were identified as research intervention studies of CR in MS suitable for a narrative review.
Table 1 included a summary with selected studies by setting (center/home/mixed), mode (individual/group/mixed), main outcomes, and objective values of intervention effectiveness (i.e. p-value and effect size).
Summary of selected studies by setting (center/home/mixed), mode (individual/group/mixed), main outcomes, and objective values of intervention effectiveness (i.e. p-value and effect size).
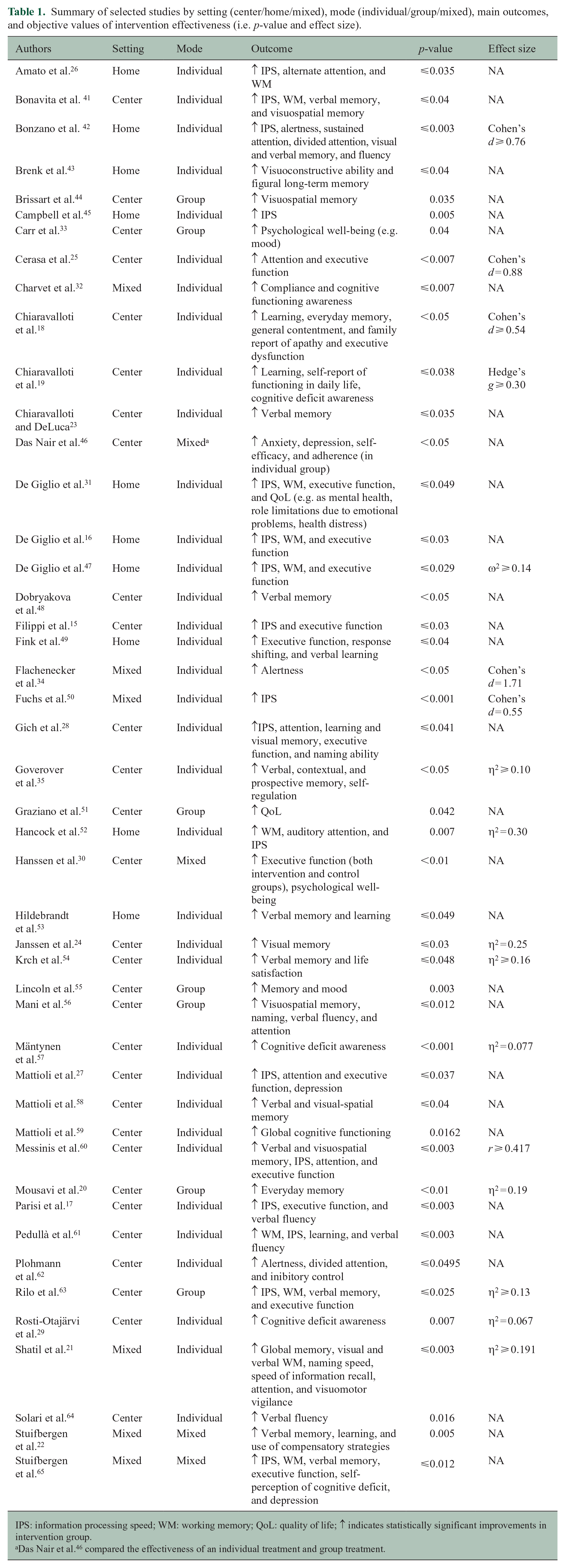
IPS: information processing speed; WM: working memory; QoL: quality of life; ↑ indicates statistically significant improvements in intervention group.
Das Nair et al. 46 compared the effectiveness of an individual treatment and group treatment.
Treatment settings: center-based versus home-based
The majority of the initial studies which provided consistent and promising evidence to the effectiveness of CR in PwMS were performed in center-based setting.19,25–27,41,54,60,62,64 In most of these reports, training sessions were supervised by an experienced neuropsychologist or a clinician who checked for compliance and adherence. 41 Also, the presence of a professional operator was highly recommended when the treatment was manualized so that clinicians had to follow a scripted manual and/or a standardized procedure.19,48,54,58 However, each rehabilitative intervention requires multiple sessions administered across weeks or even months. Moreover, the constraint for traveling to clinical center for training often prevents access to treatment for many patients. 58 The advent of technological advances in healthcare transitioned rehabilitation approaches to personalized online and remote platforms, offering more accessible setting for rehabilitation to individuals who are isolated as a result of different conditions (e.g. physical impairment and sanitary emergency). 66
Recently, CR through self-management programs is rapidly growing, offering the possibility to reach a high number of PwMS whenever a face-to-face treatment is not sought or obtainable and, most of all, providing promising results. For instance, more than one decade ago, several reports indicated the effectiveness of home-based cognitive interventions on various cognitive domains. Hildebrandt et al. 53 explored the benefits of a 6-week home-based cognitive training in PwMS who received a compact disk with memory and working memory (WM) rehabilitation tasks (VILAT-G 1.0). These patients were requested to train for at least 5 days a week for 30 minutes a day. Authors found positive effects on memory, and Brenk et al. 43 examined cognitive training over a 6-week period that took place at participants’ homes. Results indicated significant improvements in visuoconstructive ability and figural long-term memory after training using Gripsgymnastik/Brain-Gym. Also, Fink et al. 49 found that executive function and verbal learning improved significantly more in the group who received home-based cognitive intervention using the reaction capacity module of the RehaCom software (Hasomed, Germany).
Furthermore, in a pilot study by De Giglio et al., 31 PwMS were trained in tasks of memory, attention, visuospatial processing, and calculations using Dr Kawashima’s Brain Training (DKBT; Nintendo, Japan). First instructed by a psychologist on how to use the console and to perform the training, they were required to play 30 minutes per day (5 days per week) following the instructions of the game provided during the training from a virtual guide and to experience all the puzzles proposed. 31 After an 8-week home-based treatment, significant improvements in IPS and executive functions as well in some aspects related to quality of life (e.g. mental health and emotional well-being) were achieved. Furthermore, at neural level, the clinical effectiveness of home-based treatment with video games was supported by thalamic functional connectivity 16 and microstructural changes in corpus callosum 47 that were associated to the maintenance of cognitive function in MS.
In Hancock et al., 52 PwMS completed a 6-week computerized cognitive training at their home specifically aimed to improve IPS and WM. Specifically, participants completed two games that aimed to improve IPS and two games that aimed to improve WM (i.e. 3 days per week engaged in IPS training and 3 days per week engaged in WM training). Tasks continually challenged participants and automatically increased the level of difficulty once the previous level was mastered. Results indicated that the use of Posit Science InSight and Brain Twister Visual N-Back programs supplied by the researchers improved trained functions as indicated by the Paced Auditory Serial Addition Test (PASAT) score.
A significant improvement in attention, IPS, and WM was found by Pedullà et al. 61 after a home-based setting cognitive intervention using COGNI-TRAcK, a user-friendly and personalized treatment on WM, was found to be particularly suitable to deliver intensive, automatically adaptive, and monitored cognitive training. 67 In detail, the adaptive training was structured, so that the exercises’ difficulty level increased by one step every time the user performed a correct exercise. However, the difficulty level decreased by one step if the exercise was incorrect for three times in a row. Results suggested that an adaptive working load was a crucial feature determining the effectiveness of the intervention, allowed a transfer effect to non-trained cognitive domains (new learning and verbal memory, verbal fluency) and ensured a long-term positive effect. 61 This transfer effect was also confirmed by Bonzano et al. 42 who found that, after a WM training delivered with COGNI-TRAcK using the same exercises of, 61 PwMS showed improvements in IPS, sustained attention, and visual memory as well as alertness, divided attention, verbal memory, and fluency. Furthermore, in parallel to cognitive performance improvement, authors found a significant reduction of cortical activity after COGNI-TRAcK treatment (i.e. left cingulate gyrus and the right inferior parietal lobule significantly reduced their activity after the intervention), thus indirectly suggesting a recovery from a possible condition of maladaptive neuroplasticity. 42
Furthermore, Campbell et al. 45 combined neuropsychological assessment and neuroimaging to explore whether a 6-week home-based, computerized CR was an effective means of promoting CR and whether the structural basis for rehabilitation can be better defined. The treatment was delivered using RehaCom software-specific adaptive modules involving WM, visuospatial memory, and divided attention. As in previous works,42,61 the complexity level of tasks was tailored to the PwMS’ performance and increased automatically but only in line with satisfactory progress. A significant improvement in IPS was found following the CR treatment. This was further qualified by alterations in the bilateral prefrontal cortex and right temporoparietal regions during the WM task.
However, there has also been a rise in studies that combine both an at-home training with a periodical and constant supervision by clinicians or technicians. In Shatil et al., 21 a 24-hour technical support by telephone was available to all participants for the entire 12 weeks (three times a week) of cognitive training using CogniFit Personal Coach with an adaptive interactive system that ensured that a subject worked in her or his comfort zone without expiring frustration. Although participants could be called to remind them to carry out training session, almost 60% of PwMS in the training group performed autonomously, without any prompting. This positive trend suggests that the participants were comfortable and felt free to use the program at their discretion in their home settings. The observed cognitive improvements indicate that a combined cognitive training is a practical and valuable tool to improve cognitive skills in PwMS.
Furthermore, the MAPSS-MS22,65 is an interesting tool developed to help the individual acquire the highest level of cognitive functioning and functional independence through compensatory skills, retraining skills, and environmental/lifestyle support. 22 The 8-week intervention includes group sessions (2 hours per week for 8 weeks) focused on building efficacy for the use of cognitive strategies and a home-based computer training program addressing the most common deficits experienced by persons with MS, such as attention, memory, flexibility, and problem-solving (45 minutes, three times per week). During face-to-face session, the facilitator reviewed with participants their progress on cognitive tasks and discussed about strategies and performance difficulties. During home-based training, facilitator was available by e-mail and phone to assist participants if they had questions about the program. In the first explanatory study, MAPSS-MS intervention produced statistically and clinically significant improvements in the use of compensatory strategies and verbal memory. 22 Furthermore, in a recent and larger multisite study, Stuifbergen et al. 65 found that PwMS improved in IPS, verbal, and WM and reported decreased depressive symptoms following MAPSS-MS.
The efficacy of a mixed intervention was also confirmed by Charvet et al. 32 They reported a general improvement across different cognitive functions in PwMS who took part in a 12-week adaptive cognitive intervention targeting attention, WM, and executive function through the visual and auditory domain in home setting using a research version of BrainHQ program (Posit Science Corporation) compared to playing ordinary computer games. Each week, a technician recorded into a database user data from the remote program. With this information as a reference, each participant was then contacted for a weekly check-in call to discuss any concerns or technical problems with their activities. If participants failed to respond and did not show any activities on the remote platform, the study principal investigator contacted them directly to determine the circumstances behind their contact lack and program usage and to provide encouragement for participation, if needed.
In a recent study by Fuchs et al., 50 authors asked participants to complete 12 weeks of training on IPS, using an online adaptive restorative CR software (BrainHQ). Participants were contacted once each week by researchers to be provided with reminds of the study protocols and goals, with technical support as needed, and with mild encouragement. Results indicated that PwMS showed clinically meaningful change in IPS as indicated by Symbol Digit Modalities Test (SDMT).
Treatment modes: individual versus group
Given its intricate relationship between individual qualities (e.g. shyness, extroversion, empathy, self-awareness, etc.), psychosocial issues (e.g. identity formation, cohesion, and therapist–patient alliance) and healthcare costs due to rehabilitation admission, treatment mode (i.e. individual vs group) should be carefully taken into account when planning a CR program.
However, whether a treatment delivered individually25,26,58,59 is more effective than one in a group mode is still under debate.44,51,56,63 As documented by Mhizha-Murira et al., 37 information about treatment mode is often partially reported. Nonetheless, both treatment modes have advantages and disadvantages. For instance, while the level of analysis can be much more intense and comprehensive in individual compared to group treatment, group may offer a safe space for patients to share their concerns, develop and test new skills, and improve confidence. Also, while group-based intervention is usually less expensive than the individual one, it may be inappropriate for certain kind of individuals, who are extremely shy or impulsive.
Comparing the efficacy of both treatment modes on mood and quality of life, Das Nair et al. 46 found that only PwMS who took part in individual treatment show higher improvements in various outcomes as anxiety, depression, and self-efficacy. Furthermore, adherence was better in individual mode compared to group (88% and 55%, respectively). Authors indicated that the success of group intervention depends on cohesion between members, which is often linked to shared identities, ideologies, and interests. 46 Since a high number of PwMS included in the study showed low levels of mood at baseline, this could prevent cohesion and have a negative impact on group treatment adherence. However, this study did not test whether cognitive intervention led to any improvements in cognitive functions, but only in mood and quality of life.
However, several studies evaluated the effectiveness of group memory rehabilitation programs in PwMS. In a pilot study, Carr et al. 33 assessed the feasibility of ReMiND trial, 68 which combined restitution and compensation strategies to improve memory, mood, and independence. Although there was no evidence of an improvement in memory abilities followed by CR, findings showed a significant effect on mood, favoring the intervention group compared to the group who receive usual care. The beneficial effect on mood could be explained considering that participants in the intervention group were less distressed by their memory problems as a result of the memory rehabilitation or due to the social interaction in a group mode. 33
In a multicenter study, Lincoln et al. 55 assessed the clinical effectiveness and cost-effectiveness of a CR program for PwMS compared to a usual care intervention. Although both groups showed no differences in quality of life after one year, those who received CR had fewer memory problems in daily life and reported better mood than those who received only their usual clinical care. Interestingly, participants considered the group positively, reporting a decrease in their CI in daily life. 55 Sharing experiences, giving advice in a group mode, learning that other participants experienced the same problems were deemed as crucial and beneficial aspects. Although the intervention was delivered in a group mode, every effort was made to tailor the training to each participant’s need (e.g. if a participant found the task particularly difficult and stressful, the strategies taught were focused on this problem).
So, one possibility is that clinicians consider a mixed intervention, joining the strengths of both individual (e.g. tailored treatment, strong therapeutic alliance, better adherence, space to discuss in private) and group (e.g. therapeutic effects of the group, possibilities for social interaction and identity formation, sharing of information and experience) delivery modes.
In Stuifbergen et al.,22,65 authors tested the effectiveness of the MAPSS-MS that included both group sessions (2 hours per week for 8 weeks) and a home-based individual computer training program (45 minutes three times per week) with promising results. The group-based sessions of first four sessions were focused on the common cognitive problems experienced with MS (attention and processing speed, memory and language, visuospatial and executive functioning) and the development of relevant compensatory strategies and lifestyle behaviors to support cognitive functioning (e.g. managing fatigue and stress and increasing physical activity).
Hanssen et al. 30 tested the effectiveness of a 4-week CR delivered both in individual and group mode compared to individual usual care program followed by a multidisciplinary team (i.e. neurologist, physiotherapist, social worker, occupational therapist, and nurses). 30 Sessions in the intervention group included lectures, practical exercises, and discussions. The main topic of the first session was cognitive functions and principles of goal setting. The second one included a lecture about executive functions, a group exercise related to planning, and a discussion of strategies for keeping track of appointments and belongings. The third session dealt with how cognitive symptoms can affect communication, how to cope with such challenges, and how to communicate about MS. During the second and third week of the rehabilitation stay, the patients in the intervention group took part in individual sessions, one with a neuropsychologist and one with an occupational therapist. Results indicated that executive functioning improved significantly from baseline to 4 and 7 months in both groups. One possible explanation could be that also PwMS in control group received individual counseling by a multidisciplinary team, which may have motivated them to formulate and implement personal goals for coping with everyday challenges. However, improvements in well-being and psychological aspects of quality of life occurred only in the intervention group.
Furthermore, most participants reported that they felt they gained a better understanding of their cognitive deficits through a group-based intervention. 69 It follows that individuals’ insight and acceptance of cognitive deficits could be an important precursor to improvements. Thus, further studies should investigate the “weight” of group dimension and its consequent psychological effects, as insight and perception of cognitive deficits, and the content of the intervention program on achieved improvements.
Conclusion and future challenges
The ultimate goal of CR is to enable PwMS to function as adequately as possible in their environment. This topical review tried to shed light on some aspects that received less attention, although essential for both the quality of the treatment and the efficiency of healthcare services: setting (center-based vs home-based) and mode (individual vs group) of the CR treatment. We believe that investigating these aspects may provide evidence whether or not those observed improvements after CR persist over time with beneficial effects on PwMS’ daily lives.
Digital and remote technologies are involved in challenges of great interest for the current and future research, such as the improvement of safety, autonomy, and well-being, during daily activities. 39 Considering the high cost of providing healthcare to people with a neurological chronic disease and the increasing technological advancements in rehabilitation field, the time is right to move from traditional standard care center program toward the implementation of new and alternative tools in routine practice with high therapeutic benefits.
Furthermore, the advantages of telehealth over usual care (e.g. participant adherence, quality of care, cost-effectiveness, and access to services) have been further confirmed during health emergency due to COVID-19 in mid-March 2020. Worldwide efforts were made to protect general population and “flatten the curve” of COVID-19 incidence, such as social distancing, self-quarantine, and “stay at home” orders. 70 Thus, the utilization of telehealth has become critical to allow access to medical care during this pandemic, allowing a large number of PwMS access to intervention that otherwise have been stopped due to the virus. 71 In a recent systematic review by Marra et al., 70 several benefits in the use of teleneuropsychology have been proposed, including a general positive feedback from patients and caregivers, a continuing care service provided by the therapist to patients from their home, without the added risk of virus exposure, and a maintained connectedness with patients, many of whom need services and interpersonal contact. However, clinicians and researchers had to keep in mind the possible challenges and drawbacks (e.g. limited access to or familiarity with technological services, reduced opportunities for behavioral observations due to camera angles and the need of a technician to set up and configure the equipment, and necessary test stimuli). 70 The next decade brings new challenges within the new-born science of CR. The first concerns the need to select outcome measures to identify PwMS’ perspective of improvement. Citing Mäntynen et al. 57 who stated that “the main goal for the intervention might not be improvement of cognitive test performances, but learning to cope with the cognitive deficits,” clinicians and researchers have to face with the issue that the amount of change deemed to be significant to a patient’s daily life is unlikely measured by standardized cognitive tests. Beyond the effort to validate sensitive, cost-effective, and reliable screening instruments that can be used in clinical settings to identify the nature of patients’ CI, the future mission could be the development of outcome measures able to catch individuals’ experience and feelings about cognitive difficulties and goals matching them with clinically significant change in randomized trials. In this context, there is a clear need to improve patient engagement and the co-development of meaningful self-reported measures as patient-reported outcomes (PROs) and the drive in meeting this challenge could be health technologies (e-Health) using electronic PROs. 72
The second opportunity is related to the proposal of an integrative rehabilitative treatment. Motor and CIs in MS have been often examined independently, but they can interact with each other, as indicated by PwMS’ difficulties in performing motor and cognitive daily activities simultaneously, for example, talking while walking. 73 The mechanisms through which motor CR could improve cognition in MS are not well understood, although it has been proposed that specific interventions might stimulate neural pathways through neuroplasticity.74,75 Indeed, combining motor and cognitive training could be a likely effective approach in preventing CI through the possibility of transferring rehabilitation-promoted gains from motor to cognitive domains and vice versa by targeting brain areas with overlapped motor and cognitive functions. 74
The success of alternative options of CR might be explained considering also the key factor of self-awareness, an active process of coping with the disease through treatment motivation, self-care, active seeking of information, and emotional balance 76 that play a key role in rehabilitation leading PwMS to develop more awareness about their cognitive deficits and improve adherence as well as the capacity to monitor and correctly self-evaluate their performances.76,77 So when choosing the more suitable intervention strategy to maximize patients’ cognitive gains and adherence, it could be highly recommended to take into account the influence of the active participation and engagement of the participants during the training.
To conclude, although CR in MS is a new-born science, this field of study requires a task force to establish recommendations for future research, highlighting the need for applying a holistic CR approach, where the interlinked cognitive, psychosocial, and physical functioning should be all targeted, as well as the need to get close to individuals’ perspective helping them to detect possible and meaningful effects of interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.