
Abstract
Background:
Evidence for the association between body mass index (BMI) and multiple sclerosis (MS) among men remains mixed.
Objective and methods:
Swedish military conscription and other registers identified MS after age of 20 years and BMI at ages 16–20 years (N = 744,548).
Results:
Each unit (kg/m2) BMI increase was associated with greater MS risk (hazard ratio and 95% confidence interval = 1.034, 1.016–1.053), independent of physical fitness (1.021, 1.001–1.042). Categorised, overweight and obesity were associated with statistically significant raised MS risk compared to normal weight, but not after adjustment for physical fitness.
Conclusion:
MS risk rises with increasing BMI, across the entire BMI range.
Introduction
Multiple sclerosis (MS) has both genetic and environmental risk factors. 1 Higher body mass index (BMI), particularly obesity, before adulthood has been suggested as a risk factor for MS among men. However, a systematic review found mixed evidence. 2 Also, little is known about the MS risk associated with BMI across the entire BMI range.
Here, we examined BMI and MS risk in men using a Swedish register-based cohort with prospectively collected information on height and weight between ages 16 and 20 years. Measured BMI provides greater accuracy than self-reported heights and weights in some other studies. 3 We also address the role of physical fitness, as lower levels of fitness in adolescence have been linked with raised risk for subsequent MS. 4
Methods
Participants
This study used a register-based cohort described in greater detail elsewhere, 5 comprising males born between 1970 and 1992, included in the Swedish Military Conscription Register between ages 16 and 20 years. A total of 896,696 men were identified and 152,148 were excluded due to Swedish personal identification number errors (2166), conscription examination after age of 20 years (6747), an MS diagnosis before age of 20 years (32), death or emigration before age of 20 years (9,443), BMI ⩽ 15 (157), and missing information for age at conscription (58), socioeconomic characteristics (13,719), and height and weight (119,826). Missing BMI is mainly due to exemption from military service for chronic illness or disability, as well as less stringent rules allowing exemption due to lower motivation to participate after 1995. A total of 744,548 men were included and the Swedish personal identification number was used for data linkage.
Measures
BMI (kg/m2) was derived using measured height and weight from the Swedish Military Conscription Register. BMI was categorised as underweight (15 to <18.5), normal weight (18.5 to <25), overweight (25 to <30), and obesity (⩾30). An MS diagnosis after age of 20 years was identified from the Patient Register using International Classification of Diseases (ICD) codes (ICD-8 340, ICD-9 340, ICD-10 G35). To ensure diagnostic accuracy, two MS diagnoses recorded at a minimum of 6 months apart were required. Physical fitness was measured using an electronically braked ergometer and standardised on a 10-point scale (0–9). Highest level of parental occupation nearest to birth date from census data and the Longitudinal Integrated Database for Health Insurance and Labour Market Studies (LISA) was used to derive an approximation of a three-category version of the European Socioeconomic Classification. The Total Population Register provides information on migration and vital status. The Multi-generation Register provides linkage with first-degree relatives.
Statistical analysis
Cox proportional hazards regression was used to examine the association of BMI with time to the first diagnosis of MS. Follow-up was from after age of 20 years until the first diagnosis of MS, death, emigration, or study end (31 December 2014), whichever occurred first. BMI was treated as both continuous (centred at BMI = 22) and categorical. Analyses using fractional polynomials suggested no evidence of a non-linear association between BMI and MS risk. Analyses were adjusted for age at conscription and parental socioeconomic position (an indicator of material and cultural circumstances). Potential covnfounding factors were chosen based on prior research and their availability. No evidence of violation of the proportional hazards assumption was found using Schoenfeld residuals. Physical fitness (continuous) was included in a further adjusted model to test whether the association between BMI and MS was independent of physical fitness. Sensitivity analyses investigated exclusion of men with obesity (BMI ⩾ 30), use of a single MS diagnosis, and multiplicative interaction between BMI and birth period. Analyses were conducted using Stata 16.0 (StataCorp, College Station, TX, USA).
Results
Some 952 men (0.128%) were diagnosed with MS after age of 20 years, at an average age of 31.185 years. Table 1 shows characteristics of the cohort. Higher BMI was linearly associated with increased MS risk (hazard ratio = 1.034, p < 0.001, Table 1 and Figure 1). When categorised, and compared with normal BMI, underweight was associated with reduced MS risk, while overweight and obesity indicated higher risk (p < 0.05, Table 1). The linear association of BMI with MS remained after further adjustment for physical fitness, as did the reduced risk associated with underweight compared with normal BMI, but the associations with overweight and obesity were no longer statistically significant (Table 1). No substantial differences in estimates were observed after excluding BMI ⩾ 30, or including men with only one MS diagnosis. MS risk associated with BMI did not differ notably by birth period.
Characteristics of the birth cohort and hazard ratios for MS risk.
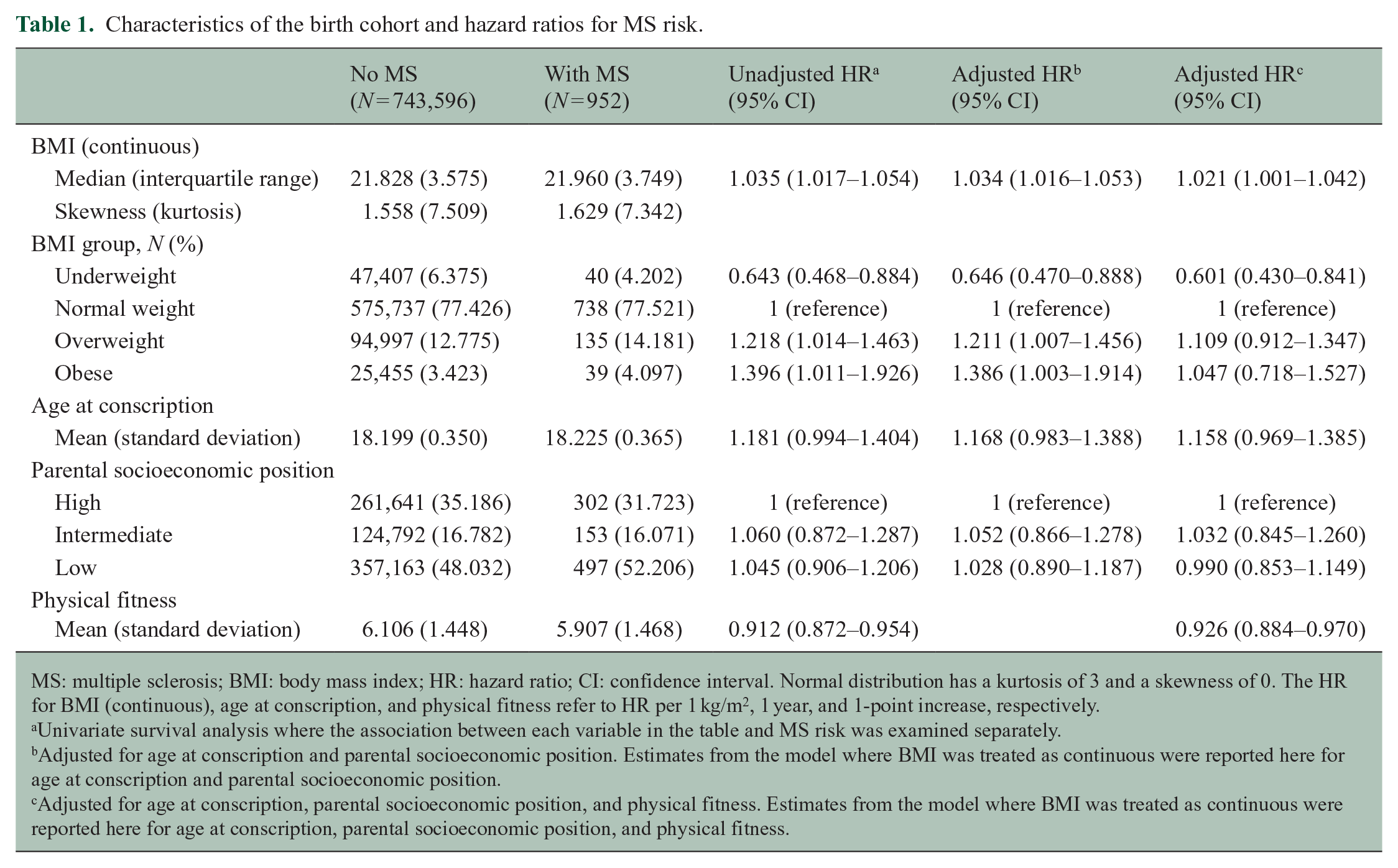
MS: multiple sclerosis; BMI: body mass index; HR: hazard ratio; CI: confidence interval. Normal distribution has a kurtosis of 3 and a skewness of 0. The HR for BMI (continuous), age at conscription, and physical fitness refer to HR per 1 kg/m2, 1 year, and 1-point increase, respectively.
Univariate survival analysis where the association between each variable in the table and MS risk was examined separately.
Adjusted for age at conscription and parental socioeconomic position. Estimates from the model where BMI was treated as continuous were reported here for age at conscription and parental socioeconomic position.
Adjusted for age at conscription, parental socioeconomic position, and physical fitness. Estimates from the model where BMI was treated as continuous were reported here for age at conscription, parental socioeconomic position, and physical fitness.
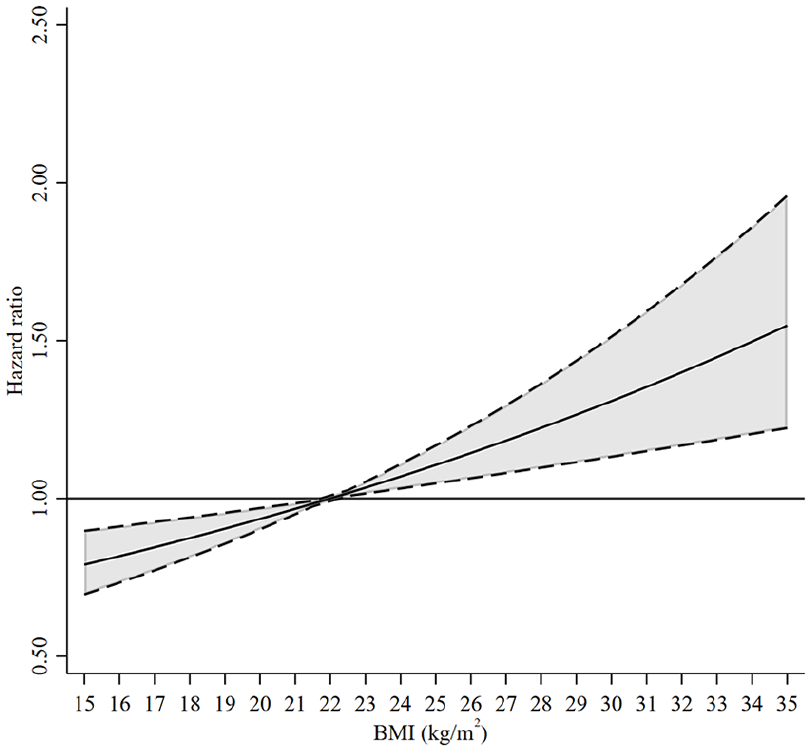
Hazard ratios and 95% confidence interval for MS risk associated with BMI across the entire range.
Discussion
Men with normal weight, overweight, or obesity had an increased MS risk compared with lower BMI. Higher levels of neuroinflammation (leptin, interleukin 6, and C-reactive protein), 6 immune responses (decreasing the number of T regulatory cells), 7 and lower vitamin D levels associated with higher BMI, 8 especially associated with obesity, may not fully explain the results as over 95% of the men had BMI < 30 and we observed associations with MS risk even in those with a BMI < 30. It is possible that early symptoms of MS such as fatigue, poor coordination, and pain affect BMI, but the association of BMI with MS risk seems to be independent of physical fitness as the association persisted over the lower range of BMI after adjustment for physical fitness.
Strengths of this study include standardised objective measurements of BMI, rather than self-report, at a critical MS risk period and a large sample size. However, unlike our previous study, 9 we did not have access to MS Register data, so we could not identify suspected symptomatic MS onset before age of 20 years. MS appears to have a long pre-clinical phase 10 and only exposures before pathogenesis initiation may add notably to MS risk, possibly reducing magnitude of associations. Adjustment for some other factors relevant to MS risk, such as genetic factors, smoking, and vitamin D, was also not possible as these measures were not available in this cohort.
In conclusion, higher BMI at ages of 16–20 years was associated with higher subsequent MS risk among men across the entire BMI range (a dose-dependent effect not only limited to overweight or obesity) although with modest effect size. BMI-associated risks for MS do not seem to be entirely due to metabolic changes associated with obesity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.M. has received research funding from Novartis, Roche and AstraZeneca, as well as serving on an advisory board for IQVIA. T.O. has received honoraria for advisory boards and unrestricted MS research grants from Biogen, Novartis, Merck, Sanofi, and Roche.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the UK Economic and Social Research Council (ESRC) to the International Centre for Life Course Studies (grants RES-596-28-0001 and ES/JO19119/1), Nyckelfonden, the Swedish Research Council and the Swedish Brain Foundation.
Ethical approval
The study was approved by the Swedish National Ethics Authority (2019-04143) and the Uppsala Regional Ethics Committee (2014/022).