
Abstract
Background:
Inpatient multidisciplinary rehabilitation (MDR) can improve health-related quality of life (HRQoL) in multiple sclerosis (MS) patients. However, the evidence of a long-term benefit is limited.
Objectives:
To investigate the long-term effectiveness of inpatient MDR on HRQoL in MS patients.
Methods:
We conducted a randomized controlled partial crossover trial with 427 MS patients.
Results:
Statistical significant long-term improvements in HRQoL were found in three of the six outcome measures at 12-month follow-up. Three in four suggested minimal clinically important differences (MCIDs) were unmet.
Conclusion:
These results indicate that the administration of inpatient MDR may lead to long-lasting improvements in HRQoL in MS patients.
Introduction
Multiple sclerosis (MS) has a significant impact on functional status and health-related quality of life (HRQoL). Inpatient multidisciplinary rehabilitation (MDR) has been shown to improve HRQoL in MS patients,1–3 and thus, MDR should be included as an integral priority in the future directions of the total management of MS. 4 However, the evidence of the long-term effects are limited.1,3 In continuation of our first report 2 from the Danish MS Hospitals Rehabilitation Study, this paper presents the results on HRQoL from 12-month follow-up (MFU), including a reanalysis of the previously reported 6-month data with increased statistical power.
Study design and methods
The study was designed as a pragmatic partial crossover trial 5 with MS patients randomized to one of the two groups with different treatment sequences: A or B, as illustrated in Supplemental Figure 1 (see Supplemental Appendix 1). We pooled the treated patients from group A and group B, to double the number of patients treated in the reanalysis of 6-month data. 2 All patients submitted written informed consent. The study was approved by the Danish Research Ethics Committee (ref. no. 1-01-83-0002-07), and it was registered at www.controlled-trials.com (ISRCTN05245917). For an in-depth description of our study design, statistical modelling and analyses, please see Supplemental Appendix 2 and the first report. 2
Referral and admission criteria
The referrals, with attached medical records, were a priori evaluated by an MS nurse and an experienced neurologist, and if necessary, with clarifying telephone conversation or a home visit. Patients suitable for inpatient MDR management were found eligible on the basis of functional health statuses, a detailed questionnaire focusing on demographic data, disease characteristics, limitations in the functional activities of daily living, community-based options, care intensity measurements and the patients’ self-perceived and prioritized focus areas. 6 The criteria for admission were patients with obvious impairments/disabilities and rehabilitation potentials to benefit from the integrated input of at least two disciplines beyond the neurologist and the MS nursing staff and patients who had the potential to actively participate in an intensive, goal-orientated MDR programme. 7
Results
Of the included 413 patients, 2 we admitted 402 patients with a median length of stay of 20 days (range: 7–20 days). Baseline statistics are presented in Table 1. In total, 180 patients in group A and 175 patients in group B completed the study. Supplemental Figure 2 depicts the trial flowchart (see Supplemental Appendix 3). Changes in HRQoL, Expanded Disability Status Scale (EDSS) and use of immunotherapy during the study period are presented in Table 2. There was no overall progression in the EDSS in any of the two groups during the 1-year follow-up.
Baseline statistics.
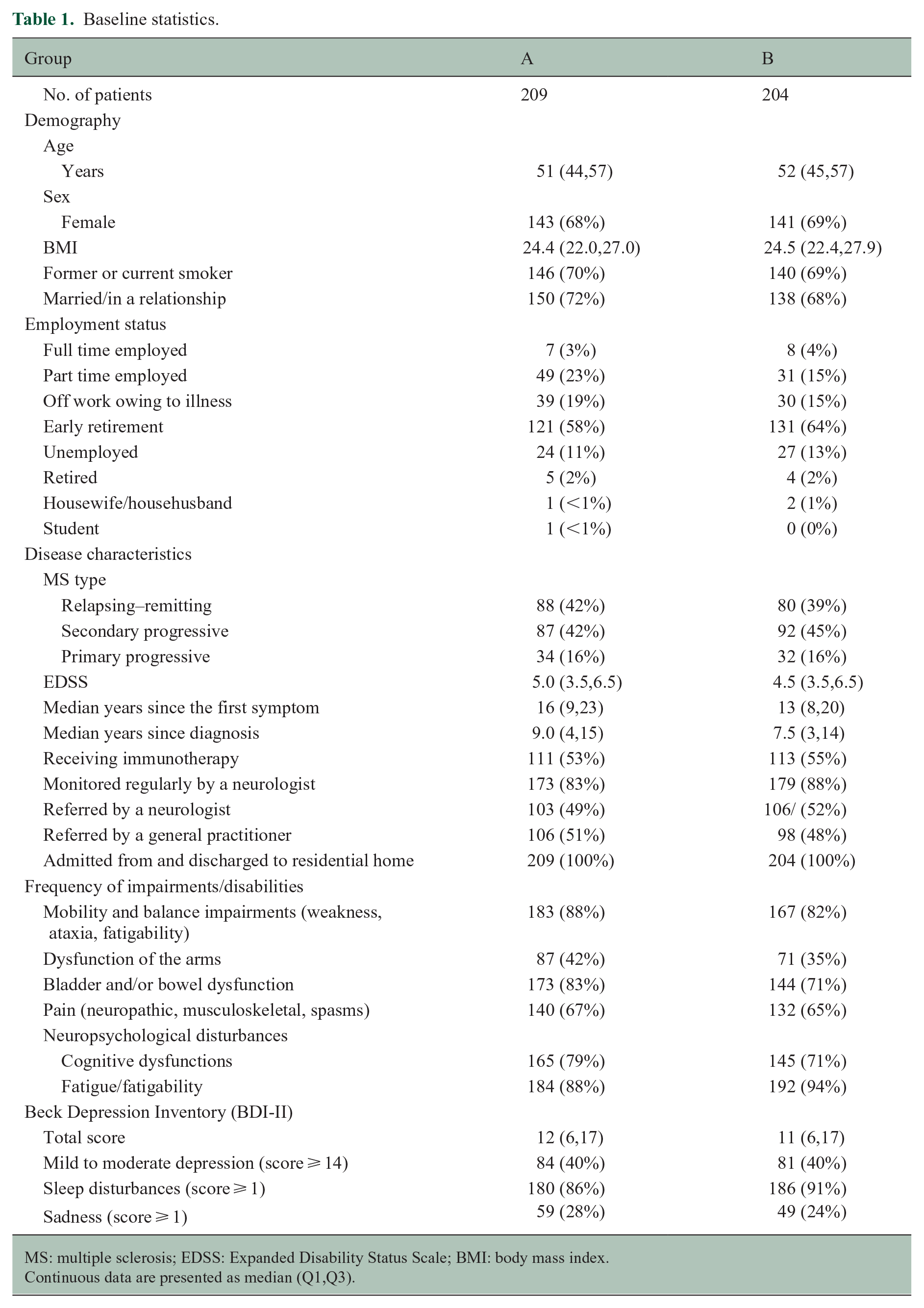
MS: multiple sclerosis; EDSS: Expanded Disability Status Scale; BMI: body mass index.
Continuous data are presented as median (Q1,Q3).
Changes and results.
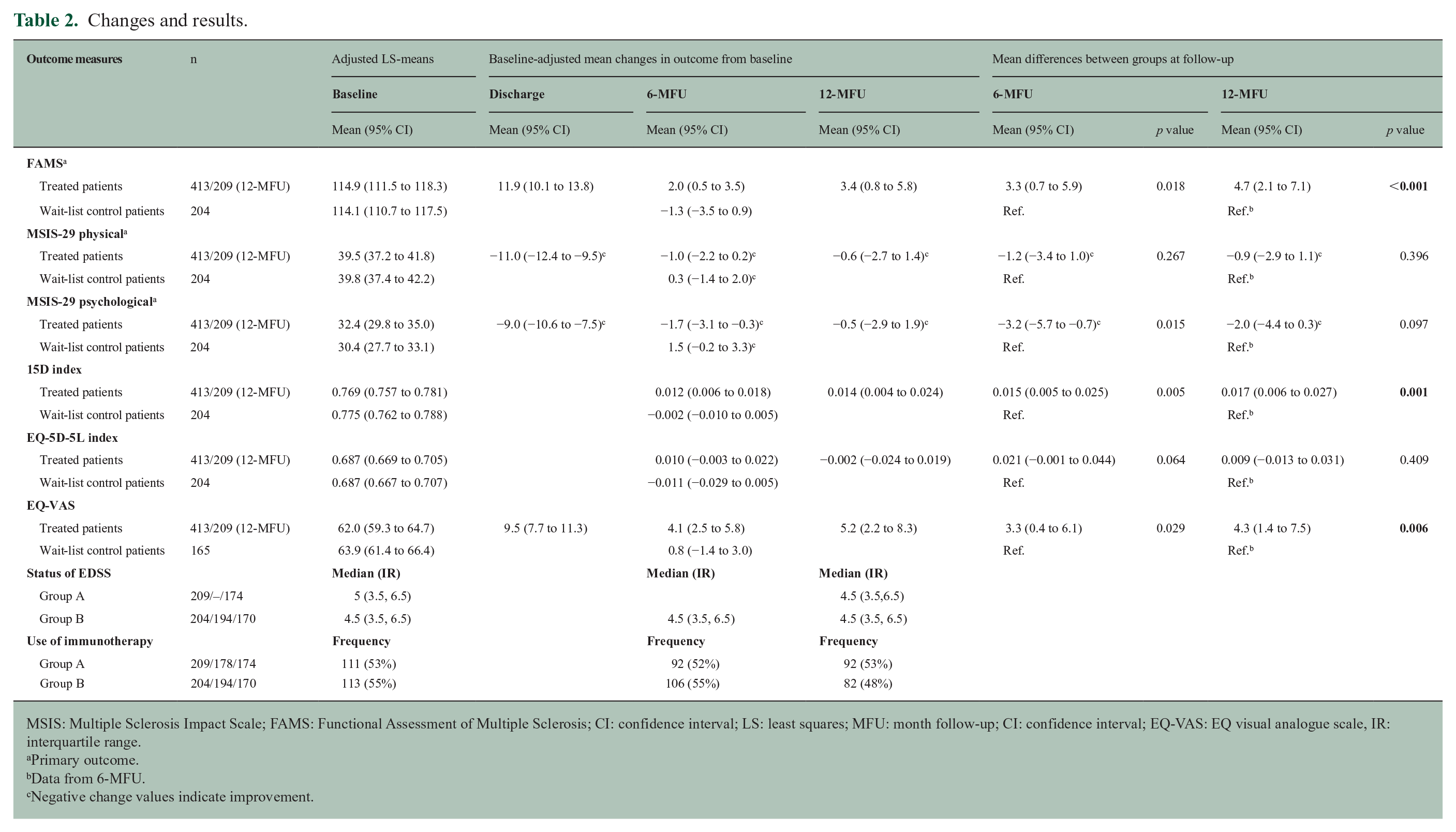
MSIS: Multiple Sclerosis Impact Scale; FAMS: Functional Assessment of Multiple Sclerosis; CI: confidence interval; LS: least squares; MFU: month follow-up; CI: confidence interval; EQ-VAS: EQ visual analogue scale, IR: interquartile range.
Primary outcome.
Data from 6-MFU.
Negative change values indicate improvement.
DiscussionWhile a clear decline followed discharge, continued statistically significant improvements in HRQoL were found at 12-MFU in three (functional assessments of multiple sclerosis (FAMS), 15D and EQ visual analogue scale (EQ-VAS)) of the six outcome measures. To our knowledge, this is the first study to demonstrate controlled long-term benefits on HRQoL from inpatient MDR, supporting the findings of Freeman et al. 1
While the estimated improvement in 15D exceeded the suggested minimal clinically important difference (MCID) and the improvement in EQ-VAS tended, estimates for the Multiple Sclerosis Impact Scale (MSIS)-29 physical and EQ-index did not. Unfortunately, neither FAMS nor MSIS-29 psychological has a suggested MCID, and even though an explorative post hoc analysis that found a 3-point change in FAMS may represent an MCID in MS patients, 8 the evidence is sparse. These circumstances make it more challenging to interpret the results, and therefore, appraising the clinical importance of our long-term findings will, to some extent, be a matter of opinion.
Focusing on FAMS, the average improvement of 4.7 units was close to our prespecified difference of interest of 5 points. 9 We assumed it would indicate a clinically important difference since every single item in FAMS represents a specific function in the patient overall functional status of their daily lives. Clinical importance of the improvement in FAMS might be exemplified and qualified by looking at certain FAMS anchor questions, as proxy indicators for overall status of functioning and HRQoL; for example, question 25: ‘I am content with the quality of my life right now’ and question 52: ‘I worry that my condition will get worse’, one of the most disabling concerns. At 12-MFU, 31% of the study patients reported an improvement in question 25 with a mean value of +1.52, moving from an average of 1.60 (between ‘a little bit’ and ‘some what’) to 3.12 (‘quite a bit’). Forty-eight percent maintained their baseline level. In question 52, 34% of the study patients reported an improvement of a mean value of +1.53, from an average of 1.28 to 2.81, and 44% maintained their baseline level. Also, previous studies found that relatively modest improvements in global HRQoL scores have significant value to patients. 10 Therefore, based upon our clinical experiences, improving close to a mean of 5 units in FAMS, distributed on two or more items (functions), could be of great importance to the patients and their relatives.
Having said that, our experiences with FAMS, which we use on a regular basis in our clinic, are that it underestimates the benefits of MDR and that could also be the case for the other outcome measures as well. Although being a highly reputable instrument, FAMS suffers from insufficient responsiveness to changes in function and ceiling effect. The risk of ceiling effect was evident in the fact that 56% of the study patients scored maximum on at least 25% of the questions at baseline, of which many deal with functions that MDR may improve.
A more thorough evaluation of long-term clinical relevance must, however, await a careful item and dimension analysis taking into account that individualized MDR seeks to improve aspects of HRQoL which match a patient’s major challenges. In fact, this may blur clinically important improvements when evaluated across a heterogeneous patient group.
Despite the study limitations, most obviously the lack of 12-MFU for the wait-list control patients (due to the trial design), the long-term results are reliable, as the partial crossover design facilitated an efficient 12-MFU comparison of treatment versus control. 5 Additional limitations of this study have been discussed in our first report. 2
In summary, our findings suggest that the administration of inpatient MDR may provide a foundation for a long-lasting improvement in HRQoL in MS patients.
Supplemental Material
MSJ884244_Appendix_1 – Supplemental material for Can inpatient multidisciplinary rehabilitation improve health-related quality of life in MS patients on the long term – The Danish MS Hospitals Rehabilitation Study
Supplemental material, MSJ884244_Appendix_1 for Can inpatient multidisciplinary rehabilitation improve health-related quality of life in MS patients on the long term – The Danish MS Hospitals Rehabilitation Study by Finn Boesen, Michael Nørgaard, Anders Guldhammer Skjerbæk, Peter Vestergaard Rasmussen, Thor Petersen, Brita Løvendahl and Philipp Trénel in Multiple Sclerosis Journal
Supplemental Material
MSJ884244_Appendix_2 – Supplemental material for Can inpatient multidisciplinary rehabilitation improve health-related quality of life in MS patients on the long term – The Danish MS Hospitals Rehabilitation Study
Supplemental material, MSJ884244_Appendix_2 for Can inpatient multidisciplinary rehabilitation improve health-related quality of life in MS patients on the long term – The Danish MS Hospitals Rehabilitation Study by Finn Boesen, Michael Nørgaard, Anders Guldhammer Skjerbæk, Peter Vestergaard Rasmussen, Thor Petersen, Brita Løvendahl and Philipp Trénel in Multiple Sclerosis Journal
Supplemental Material
MSJ884244_Appendix_3 – Supplemental material for Can inpatient multidisciplinary rehabilitation improve health-related quality of life in MS patients on the long term – The Danish MS Hospitals Rehabilitation Study
Supplemental material, MSJ884244_Appendix_3 for Can inpatient multidisciplinary rehabilitation improve health-related quality of life in MS patients on the long term – The Danish MS Hospitals Rehabilitation Study by Finn Boesen, Michael Nørgaard, Anders Guldhammer Skjerbæk, Peter Vestergaard Rasmussen, Thor Petersen, Brita Løvendahl and Philipp Trénel in Multiple Sclerosis Journal
Footnotes
Acknowledgements
This study was made possible through a non-earmarked inheritance from Maja and Johan Jørgensen to the Danish MS Hospitals. We thank all the patients and the staff who participated in this study, as well as the volunteers from the MS Society. Their contributions are gratefully acknowledged.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.