
Abstract
Objective:
The objective of the study was to determine whether early infratentorial and/or spinal cord lesions are long-term cumulative predictors of disability progression in multiple sclerosis (MS).
Methods:
We selected 153 MS patients from the longitudinal Amsterdam MS cohort. Lesion analysis was performed at baseline and year 2. Disability progression after 6 and 11 years was measured using the Expanded Disability Status Scale (EDSS) and EDSS-plus (including 25-foot walk and 9-hole peg test). Patients with spinal cord or infratentorial lesions were compared for the risk of 6- and 11-year disability progression to patients without spinal cord or infratentorial lesions, respectively. Subsequently, patients with lesions on both locations were compared to patients with only spinal cord or only infratentorial lesions.
Results:
Baseline spinal cord lesions show a higher risk of 6-year EDSS progression (odds ratio (OR): 3.6, p = 0.007) and EDSS-plus progression (OR: 2.5, p = 0.028) and 11-year EDSS progression (OR: 2.8, p = 0.047). Patients with both infratentorial and spinal cord lesions did not have a higher risk of 6-year disability progression than patients with only infratentorial or only spinal cord lesions.
Conclusion:
The presence of early spinal cord lesions seems to be a dominant risk factor of disability progression. Simultaneous presence of early infratentorial and spinal cord lesions did not undisputedly predict disability progression.
Introduction
Multiple sclerosis (MS) is the most frequent inflammatory, demyelinating disease of the central nervous system (CNS) in young adults, leading to long-term disability. 1 In addition to the clinical presentation and neurological assessment, magnetic resonance imaging (MRI) of the brain and spinal cord plays a pivotal role both in the diagnosis and monitoring of disease activity.2–4 Recommended MRI outcome measures for daily clinical practice include active (new or enlarging) T2-hyperintense and T1-gadolinium-enhancing lesions.3–7 Although the correlation between T2 lesion burden and clinical outcome measures is moderate at best, expressed in the term “clinico-radiological paradox,”8–10 it has been conclusively demonstrated that T2 lesions are related to the risk of conversion to clinically definite multiple sclerosis (CDMS)11,12 and increased disability.12,13
Previous research demonstrated that not only the presence of lesions but also lesion location is relevant for the prediction of future disability.14–17 In particular, lesions in the spinal cord and posterior cranial fossa are located in clinical eloquent areas with less compensatory possibilities, resulting in an increased risk of developing disability or conversion to CDMS.16–22 Infratentorial lesions are important predictors for long-term disability,20,22 especially brainstem lesions. 22 In addition, there is considerable evidence that spinal cord lesions demonstrate an increased risk of developing disability or conversion to CDMS.18,19,21 Moreover, there are indications that patients with a combination of both spinal cord and infratentorial lesions have a higher chance of disability or conversion to CDMS.16,17 However, so far the cumulative value of early spinal cord and infratentorial lesions on disability progression measured by the Expanded Disability Status Scale (EDSS) and EDSS-plus has not been determined.
We hypothesize that the presence of both infratentorial and spinal cord lesions early on in the disease course might be a stronger predictor for future disability than the sole presence of lesions in one of these locations. Furthermore, we hypothesize that the combination of new infratentorial and spinal cord lesions early in the disease is a better predictor than new lesions on these locations alone. Hence, the aim of this study was to determine whether early infratentorial and spinal cord lesions are cumulative predictors for disability progression after both 6 and 11 years measured by the EDSS and EDSS-plus. This could contribute to a better risk profile for patients with a higher risk of disability progression.
Methods
Patient selection
This observational cohort study prospectively included patients from the Amsterdam MS Cohort. The study design is illustrated in Figure 1.
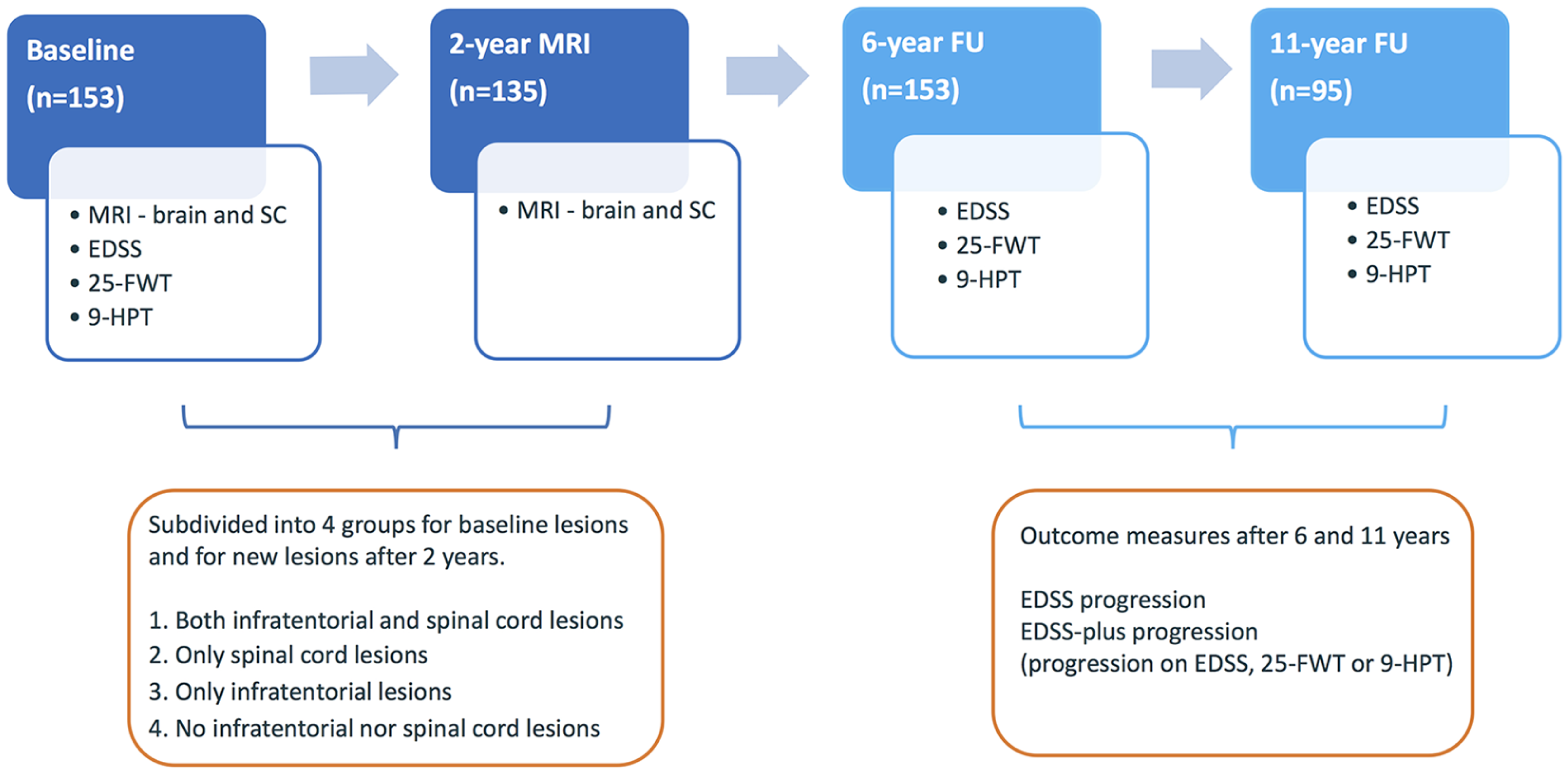
Study design.
A total of 319 MS patients were recruited from December 2000 until September 2007. Inclusion criteria were as follows: age between 18 and 60 years at onset of first symptoms (n = 315), relapsing onset (n = 289), baseline visit within 12 months from onset (n = 208), brain and spinal cord imaging (including post-contrast series) available at baseline or within 3 months (n = 188), clinical and radiological follow-up (FU) after 2 years (n = 173), and clinical FU around 6 years after baseline (n = 153).
The institutional ethics review board of the Amsterdam UMC—location VU University Medical Center approved this study and all subjects gave written informed consent prior to participation.
Clinical assessments
At baseline and FU visits, clinical assessments included the EDSS, 23 timed 25-foot walk test (25-FWT), and 9-hole peg test (9-HPT). Telephone EDSS was used in case of a missing FU visit (4.5% of total EDSS scores used). Prescribed disease-modifying therapy (DMT) and relapses were noted for all patients.
Neuroimaging
The neuroimaging and image analysis protocol of the Amsterdam MS cohort has been described previously. 21 Brain and spinal cord MRI were performed preferable on the visit date or within 3 months prior or after the baseline clinical assessments. Brain and spinal cord MRI were performed on a 1.0- or 1.5-Tesla whole-body MR system (Siemens Magnetom Impact Expert, Siemens Vision, and Siemens Sonata; Siemens AG, Erlangen, Germany). Brain MRI protocol included axial two-dimensional (2D) dual-echo, spin-echo (proton-density and late echo T2-weighted) images (repetition time (TR): 2200–3000 ms; echo-time (TE): 20–30 and 80–100 ms) and axial T1-weighted spin-echo images after single-dose gadolinium administration (TR: 500–600ms; TE: 20 ms). The spatial resolution of the 2D sequences consisted of slice thicknesses of 3–5 mm, with a 10% gap and in-plane resolution of 1 × 1 mm2. Spinal cord imaging covered the total length of the spinal cord and included proton-density and T2-weighted, dual-echo, spin-echo sequences (TR: 2500–3000 ms; TE: 20–30 and 80–100ms), a 0.3-mm gap between slices and resolution of 1 × 1 mm2. T2-hyperintense and T1-contrast-enhancing lesions were identified by an experienced rater (>10 years of experience) blinded to the clinical and paraclinical data of the patient.
Baseline lesion counts included the total number of T2-hyperintense and T1-contrast-enhancing lesions at that moment. New lesions were counted on the 2-year MRI (n = 135). T2 lesions were categorized as supratentorial (juxtacortical, periventricular, deep white matter, corpus callosum, basal ganglia, internal capsule), infratentorial (brainstem and cerebellum), or spinal cord.
Clinical endpoints
Disability progression at 6- and 11-year FU was determined using the EDSS 23 and EDSS-plus. 24 EDSS progression was defined as used in clinical trials with an increase in EDSS of 1.5, 1, or 0.5 in case of a reference EDSS of 0, 1–5.5, or ⩾6.0, respectively. 25 The EDSS-plus is a more extensive assessment for disability progression, defined as progression on EDSS as described above or a 20% increase at FU on the 25-FWT or 9-HPT. 24
Statistical analysis
Normality of variables was checked by visual inspection of histograms. Statistics were performed using parametric and non-parametric tests. Risk of disability progression was determined using logistic regression models.
We first explored the risk of disability progression for patients with spinal cord lesions versus patients without spinal cord lesions and also for patients with infratentorial lesions versus patients without infratentorial lesions at baseline. Second, we determined the number of patients with cervical spinal cord and thoracic spinal cord lesions and determined their risk of disability progression. For the infratentorial lesions, we distinguished brainstem and cerebellar lesions to determine their individual risk of disability progression.
Subsequently, we subdivided patients into four categories according to the presence of spinal cord and/or infratentorial lesions on baseline MRI (regardless of the presence of supratentorial lesions), respectively: (1) both infratentorial and spinal cord lesions, (2) only spinal cord lesions, (3) only infratentorial lesions, and (4) no spinal cord nor infratentorial lesions (see Figure 2). We additionally analyzed the risk of 6- and 11-year disability progression comparing groups based on the development of new infratentorial and/or spinal cord lesions after 2 years.
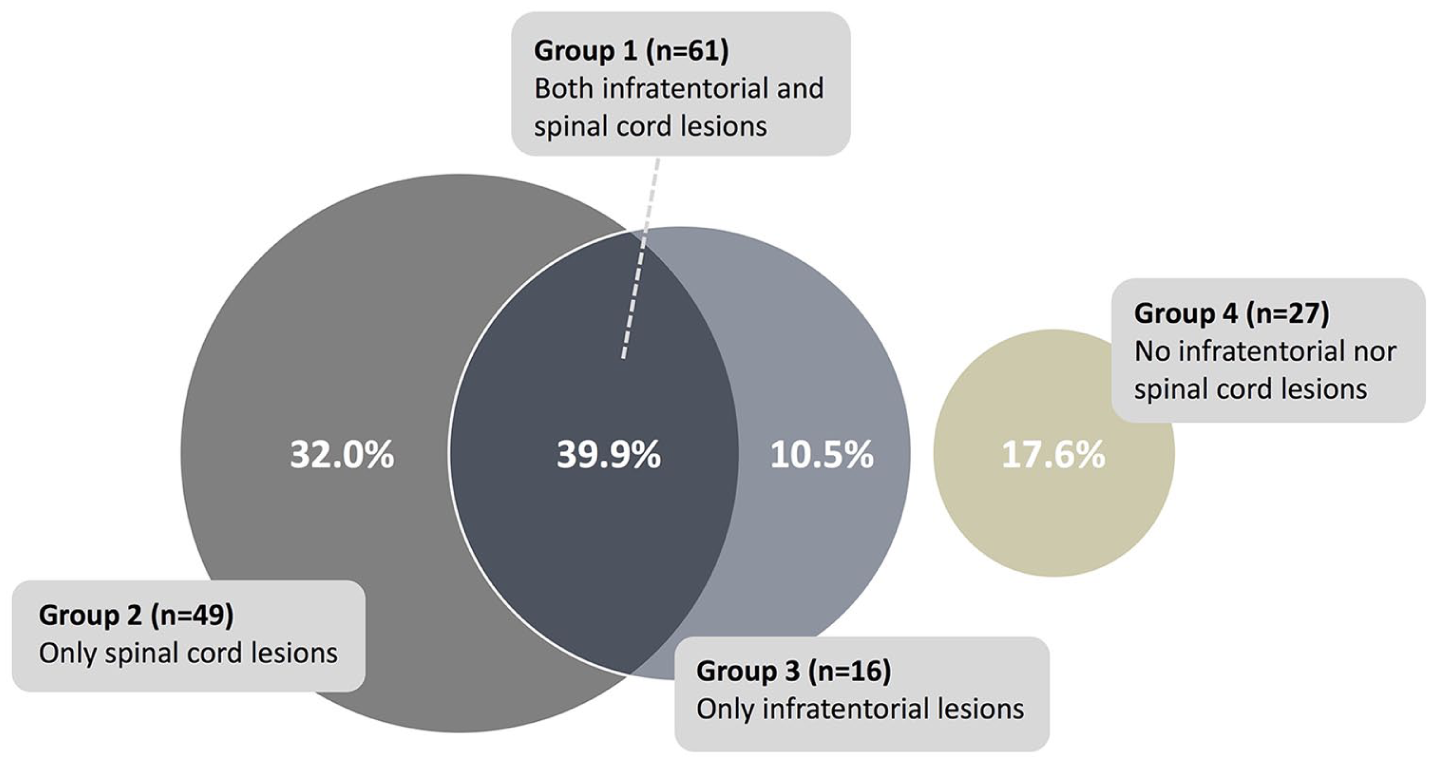
Presence of infratentorial and spinal cord lesions at baseline (n = 153), only shown for patients with 6 years of FU.
Logistic regression models were used to identify whether the presence of both infratentorial and spinal cord lesions at baseline results in a higher risk of EDSS progression or EDSS-plus progression after 6 and 11 years of FU, than the presence of infratentorial or spinal cord lesions in isolation.
Disease duration, age at baseline, baseline supratentorial T2-hyperintense and T1-contrast-enhancing lesion counts, sex, EDSS at baseline and DMT use during FU were analyzed to identify potential confounders. DMT use during FU and supratentorial T2-hyperintense lesions were confounders and all models were corrected for DMT use during FU and supratentorial T2-hyperintense lesion count at baseline or after 2 years, accordingly. Level of significance was set at p < 0.05. SPSS 22.0 was used for statistical analyses (IBM, SPSS, Chicago, IL, USA).
Results
Patients were followed for 6 years (153 patients) and 11 years (95 patients) and were classified according to the presence of infratentorial and spinal cord lesions at baseline and separately on the development of new lesions in the first 2 years.
Demographics for lesion distribution at baseline
Of the 153 patients with a 6-year FU, 110 patients (71.9%) had spinal cord lesions (59 with both cervical and thoracic lesions, 32 only cervical, and 19 only thoracic spinal cord lesions). Baseline infratentorial lesions were seen in 77 patients (50.3%), of which 21 patients presented with both brainstem and cerebellar lesions, 30 patients had brainstem lesions only, and 26 patients had cerebellar lesions only.
In total, 95 patients had an 11-year FU, of which 67 (70.5%) had spinal cord lesions (35 patients had both cervical and thoracic lesions, 20 patients only cervical, and 12 patients only thoracic spinal cord lesions). Baseline infratentorial lesions were present in 51 (53.7%) patients (12 patients had both brainstem and cerebellar lesions, 20 patients only brainstem, and 19 patients only cerebellar lesions).
Subsequently, patients were subdivided into four groups based on the presence of infratentorial and/or spinal cord lesions at baseline. Of the 153 patients with a 6-year FU, 61 patients (39.9%) had both spinal cord and infratentorial lesions, 49 (32.0%) only spinal cord lesions, 16 (10.5%) only infratentorial lesions, and 27 (17.6%) no spinal cord nor infratentorial lesions. Figure 2 shows the distribution of patients according to lesion location at baseline. Baseline and FU characteristics are summarized in Table 1.
Demographic, clinical, and MRI data of patients with 6- and 11-year follow-up.
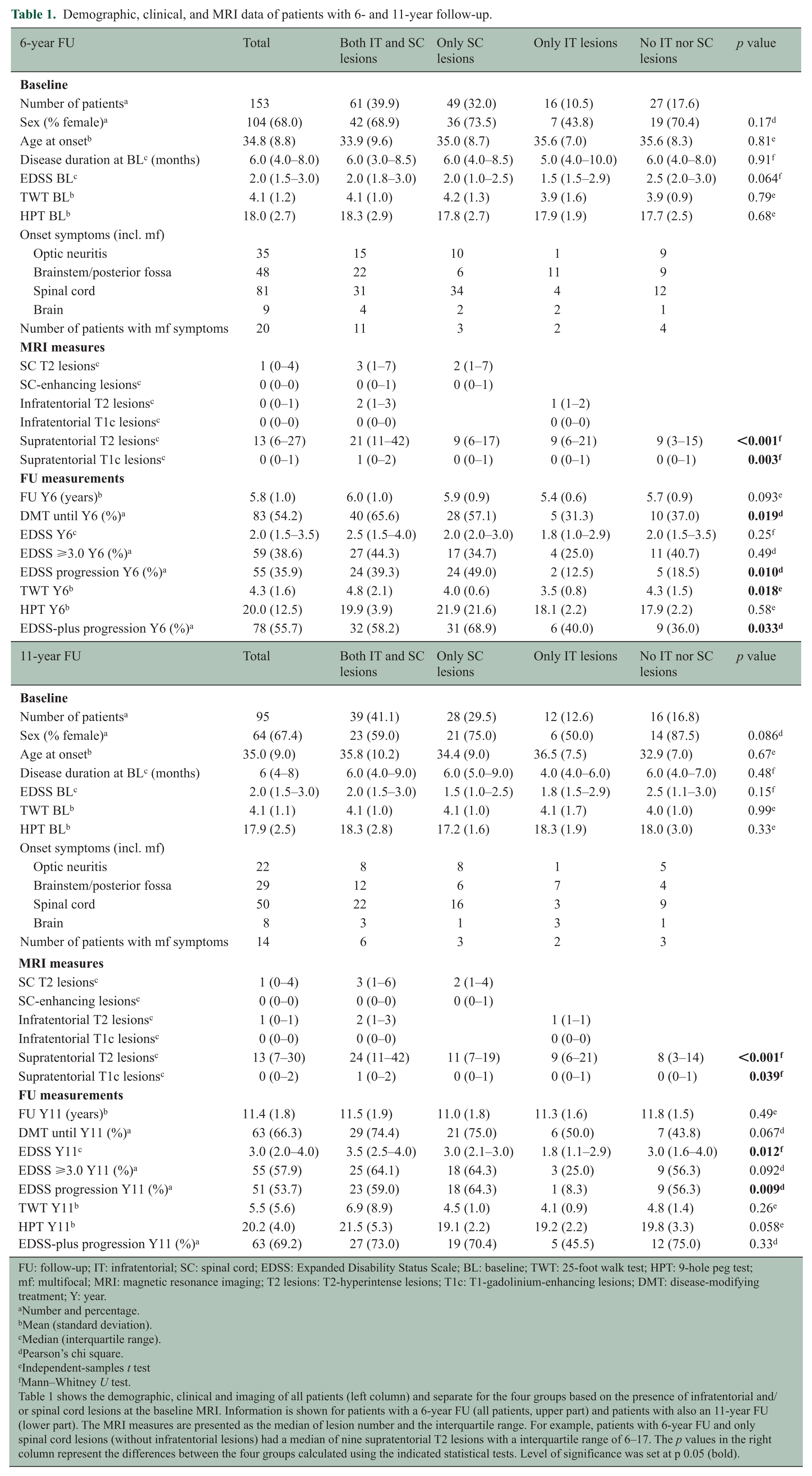
FU: follow-up; IT: infratentorial; SC: spinal cord; EDSS: Expanded Disability Status Scale; BL: baseline; TWT: 25-foot walk test; HPT: 9-hole peg test; mf: multifocal; MRI: magnetic resonance imaging; T2 lesions: T2-hyperintense lesions; T1c: T1-gadolinium-enhancing lesions; DMT: disease-modifying treatment; Y: year.
Number and percentage.
Mean (standard deviation).
Median (interquartile range).
Pearson’s chi square.
Independent-samples t test
Mann–Whitney U test.
Table 1 shows the demographic, clinical and imaging of all patients (left column) and separate for the four groups based on the presence of infratentorial and/or spinal cord lesions at the baseline MRI. Information is shown for patients with a 6-year FU (all patients, upper part) and patients with also an 11-year FU (lower part). The MRI measures are presented as the median of lesion number and the interquartile range. For example, patients with 6-year FU and only spinal cord lesions (without infratentorial lesions) had a median of nine supratentorial T2 lesions with a interquartile range of 6–17. The p values in the right column represent the differences between the four groups calculated using the indicated statistical tests. Level of significance was set at p 0.05 (bold).
Regression models using lesion distribution at baseline
First we analyzed the risk of disability progression comparing patients with spinal cord lesions to patients without spinal cord lesions (regardless of infratentorial lesions) and patients with infratentorial lesions to patients without infratentorial lesions (regardless of spinal cord lesions). Subsequently, we analyzed the risk of disability for patients with both infratentorial and cerebellar lesions compared to patients with only infratentorial or only spinal cord lesions. All models are adjusted for DMT use during the FU period and T2-supratentorial lesions.
Patients with baseline spinal cord lesions (regardless of infratentorial lesions) had a higher risk to show EDSS progression (OR: 3.6; confidence interval (CI): 1.42–9.03, p = 0.007) and EDSS-plus progression (OR: 2.5; CI: 1.10–5.47, p = 0.028) after 6 years and EDSS progression after 11 years (OR: 2.8; CI: 1.02–7.51, p = 0.047) (Table 2), compared to patients without baseline spinal cord lesions. Patients with cervical spinal cord lesions did not have a higher risk of disability progression than patients without cervical spinal cord lesions, and patients with thoracic spinal cord lesions did not have a higher risk of disability progression than patients without thoracic spinal cord lesions.
Risk of 6- and 11-year disability progression.
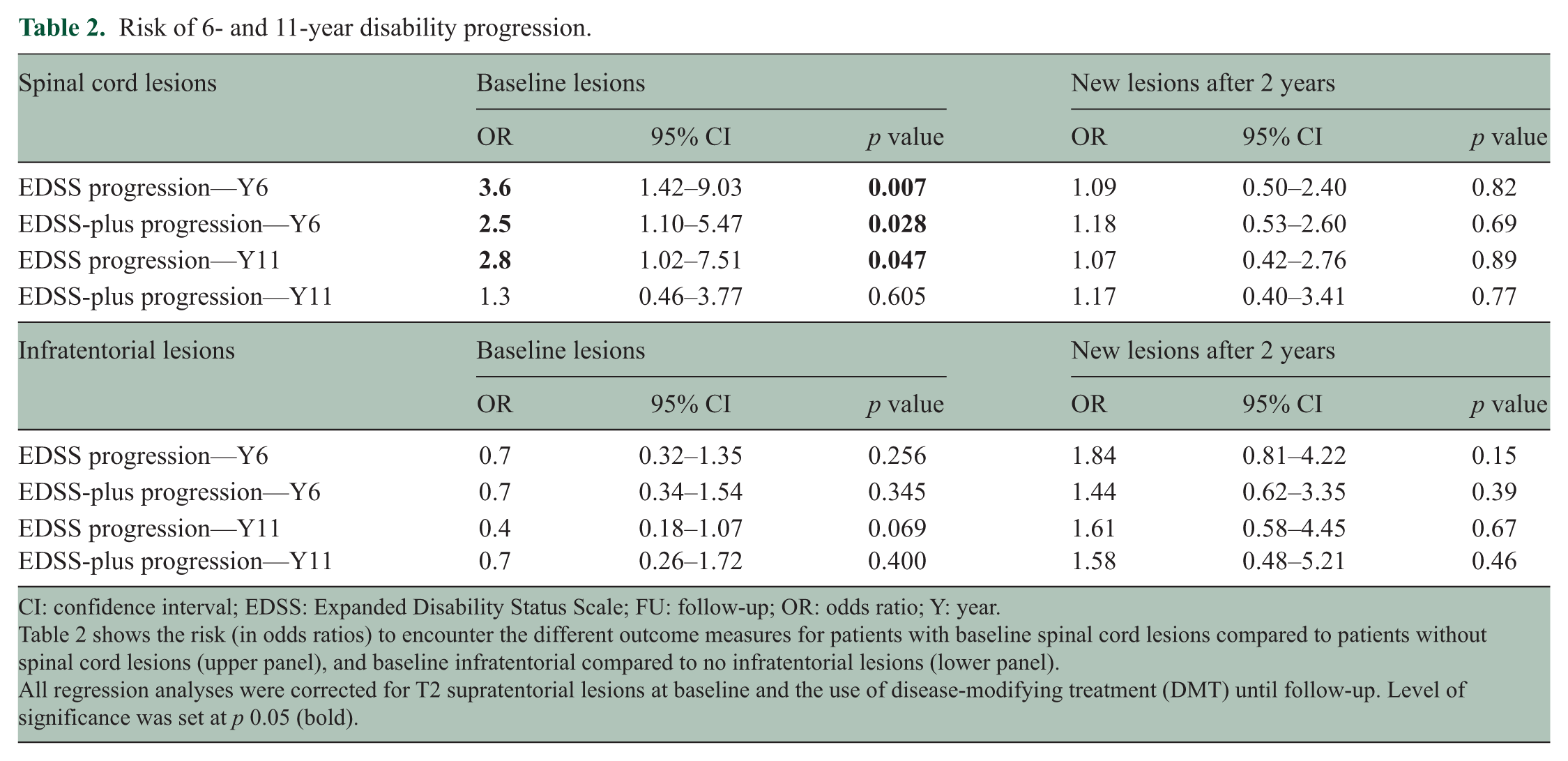
CI: confidence interval; EDSS: Expanded Disability Status Scale; FU: follow-up; OR: odds ratio; Y: year.
Table 2 shows the risk (in odds ratios) to encounter the different outcome measures for patients with baseline spinal cord lesions compared to patients without spinal cord lesions (upper panel), and baseline infratentorial compared to no infratentorial lesions (lower panel).
All regression analyses were corrected for T2 supratentorial lesions at baseline and the use of disease-modifying treatment (DMT) until follow-up. Level of significance was set at p 0.05 (bold).
Patients with baseline infratentorial lesions (regardless of spinal cord lesions) showed a trend towards a lower risk of EDSS progression after 11 years (Table 2) than patients without baseline infratentorial lesions. Patients with brainstem lesions did not show a higher risk of disability progression compared to patients without brainstem lesions. In addition, patients with cerebellar lesions did not show a higher risk of disability progression compared to patients without lesions in the cerebellum.
Patients with both spinal cord and infratentorial lesions did not differ with respect to the risk of EDSS or EDSS-plus progression after 6 or 11 years compared to patients with only spinal cord lesions, but showed a higher risk of 11-year EDSS progression than patients with only infratentorial lesions(OR: 17.6; CI: 1.8–176.0, p = 0.015) (Table 3).
Risk of 6- and 11-year disability progression for combination of infratentorial and spinal cord lesions.
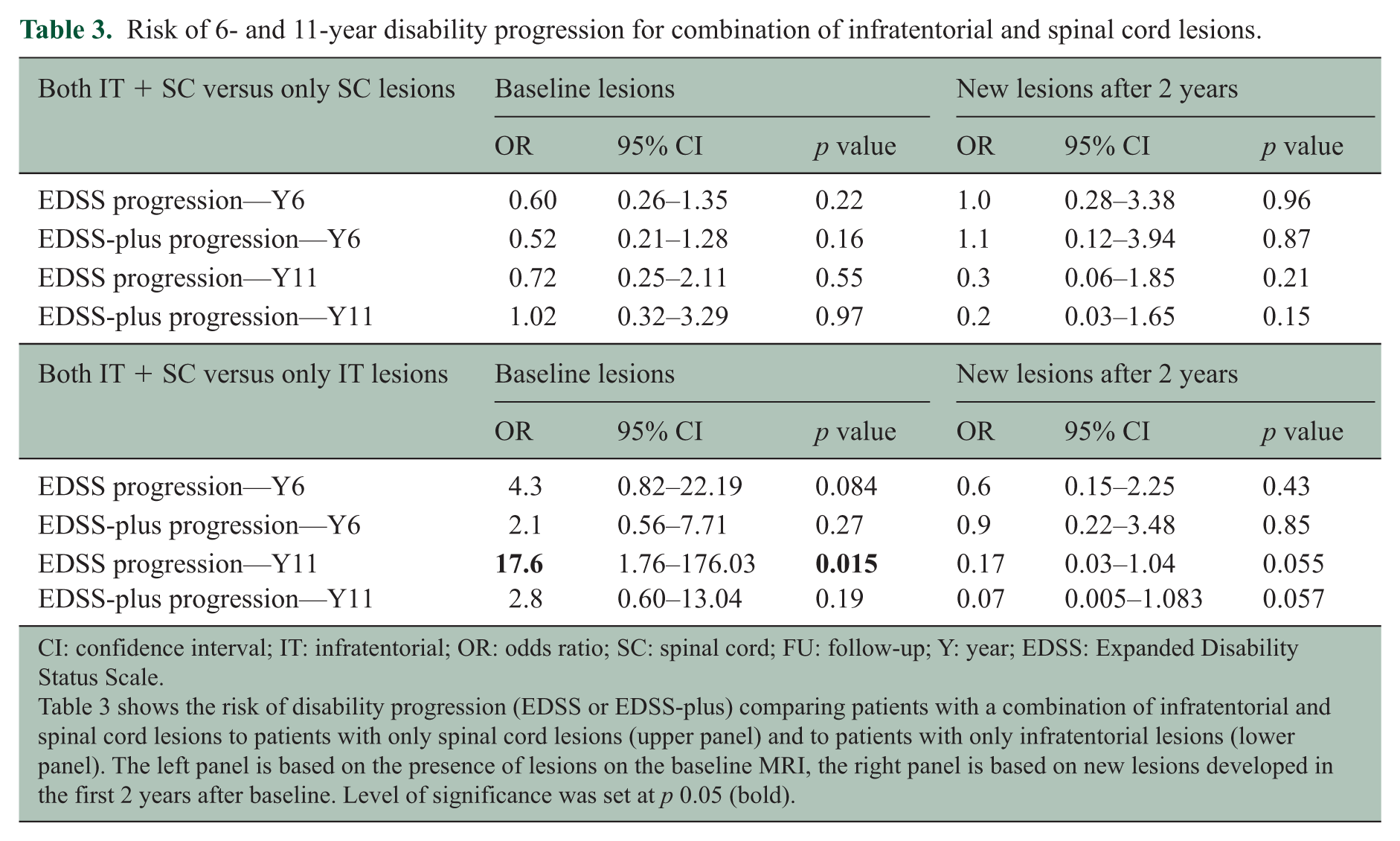
CI: confidence interval; IT: infratentorial; OR: odds ratio; SC: spinal cord; FU: follow-up; Y: year; EDSS: Expanded Disability Status Scale.
Table 3 shows the risk of disability progression (EDSS or EDSS-plus) comparing patients with a combination of infratentorial and spinal cord lesions to patients with only spinal cord lesions (upper panel) and to patients with only infratentorial lesions (lower panel). The left panel is based on the presence of lesions on the baseline MRI, the right panel is based on new lesions developed in the first 2 years after baseline. Level of significance was set at p 0.05 (bold).
In case the reference group was the group without infratentorial nor spinal cord lesions, only the group with solely spinal cord lesions had a significant higher risk of disability after 6 (OR: 3.9; CI: 1.27–12.15, p = 0.018) and 11 years (OR: 3.6; CI: 1.26–10.15, p = 0.017). The group with only infratentorial lesions showed a lower risk of EDSS progression after 11 years (OR: 0.07; CI: 0.01–0.65, p = 0.020) (see Supplementary Table 1, middle panel with baseline data).
New disease activity in the first 2 years after baseline
The year 2 MRI scan and 6-year FU were completed by 135 patients, 45 patients (33.3%) had new spinal cord lesions and 37 patients (27.4%) had new infratentorial lesions, 18 (11.6%) of these patients had a combination of new infratentorial and new spinal cord lesions, 27 (17.4%) only new spinal cord lesions, and 20 (12.9%) only new infratentorial lesions. Most patients with new infratentorial or new spinal cord lesions already had infratentorial and/or spinal cord lesions at baseline. Of the 45 patients with new spinal cord lesions, 23 patients had both infratentorial and spinal cord lesions at baseline, 17 patients had only spinal cord lesions at baseline, 1 patient only had baseline infratentorial lesions, and 4 patients had no infratentorial nor spinal cord lesions at baseline and. Of the 37 patients with new infratentorial lesions, 21 patients had a combination of baseline infratentorial and spinal cord lesions, 3 patients had only infratentorial lesions at baseline, 10 patients had baseline spinal cord lesions only, and 3 patients did not have baseline infratentorial or spinal cord lesions.
Patients with both new infratentorial and new spinal cord lesions did not differ regarding the risk of disability progression compared to patients with only spinal cord lesions (Table 3) but showed a trend toward a lower risk of disability progression after 11 years compared to patients with only new infratentorial lesions. Also, having patients without new infratentorial nor new spinal cord lesions as a reference, only patients with solely new infratentorial lesions had a (trend towards a) higher risk of disability progression (Supplementary Table 1).
Discussion
Infratentorial and spinal cord lesions are important to diagnose MS 7 and play an essential role in predicting disability outcome.16–22 In this longitudinal cohort study, we determined whether the presence of infratentorial and spinal cord lesions are a cumulative predictor for disability progression (measured by EDSS and EDSS-plus) after 6 and 11 years, which has not been explored before.
Although we hypothesized that infratentorial and spinal cord lesions would be cumulative predictors for disability progression, surprisingly, the combination of lesions in both locations did not unquestionably reveal to be a better predictor of disability progression than spinal cord lesions or infratentorial lesions alone. However, the presence of early spinal cord lesions was an important risk of disability progression. In contrast, the presence of early infratentorial lesions did not predict disability progression, but for patients with new infratentorial lesions after 2 years, a trend was seen for higher risk of disability progression compared to patients with a combination of new infratentorial and new spinal cord lesions or patients without new infratentorial and spinal cord lesions.
The risk of disability progression for spinal cord and infratentorial lesions was analyzed individually and in combination. Patients with baseline spinal cord lesions, regardless of the presence of infratentorial lesions, had a higher risk of disability progression than patients without spinal cord lesions, which is also the case for patients with only spinal cord lesions (without infratentorial lesions) compared to patients without infratentorial nor spinal cord lesions. In general, studies determining the predictive value of spinal cord lesions on disability show that patients with spinal cord lesions have a higher risk of disability progression than patients without spinal cord lesions.16–19,21,26 In clinically isolated syndrome (CIS) patients, from the same cohort as this study, patients with spinal cord lesions converted significantly earlier to CDMS than patients without spinal cord lesions, 21 and patients with optic neuritis with both infratentorial and spinal cord lesions also showed a higher risk of disability progression. Considering cervical or thoracic spinal cord lesions separately, this did not result in a difference in risk of disability compared to patients without cervical or thoracic spinal cord lesions, respectively. Besides the relevance for diagnosis, 3 these results also underscore the importance of (full-length) spinal cord imaging for the development of future disability.
Nonetheless, new spinal cord lesions developing in the first 2 years were not a predictor for disability progression, most likely because many patients with spinal cord lesions at baseline did not develop new spinal cord lesions during the first 2 years. However, these patients were part of the reference group and were shown to have a higher risk of disability progression already from baseline on. New spinal cord lesions provide unclear prognostic relevance of obtaining a new spinal cord MRI in absence of symptoms. This is in line with recent expert panel guidelines stating that current scientific data do not justify FU spinal cord MRI on regular basis for prognostic and monitoring purposes.3,4
Surprisingly, baseline infratentorial lesions were not a clear predictor for disability progression and the presence of infratentorial lesions even indicated a lower risk of 11-year EDSS progression. In contrast to the unexpected findings regarding baseline infratentorial lesions, new infratentorial lesions after 2 years showed a trend for an increased risk of disability progression on both EDSS and EDSS-plus after 11 years compared to patients without new lesions (Supplementary Table) or a combination of new infratentorial and spinal cord lesions (Table 3). Considering previous studies, one would expect that baseline infratentorial lesions would be found as predictors for disability 20,22,27 or disability progression. 17 However, the low number of patients with only infratentorial lesions possibly explains the contrary findings in our study. Perhaps, new infratentorial lesions could overrule compensatory mechanisms that were initially strong enough to mask clinical symptoms. Another plausible explanation could be that spinal cord lesions are the dominant factor in determining the risk of disability. Due to the salience of the spinal cord tracts, one might imagine that lesions herein will more easily affect important pathways without compensatory possibilities of neighboring areas than infratentorial lesions; imaginably, spinal cord lesions early in the disease might reflect a more direct risk of disability, while infratentorial lesions after 2 years raise this risk of disability progression.
Lesion location within the infratentorial area (brainstem or cerebellum) did not show differences in the risk of disability progression in our study but has been shown to be of distinctive predictive relevance of disability outcome in a previous study, with brainstem lesions resulting in a higher risk of disability progression than lesions in the cerebellum. 22 A possible explanation for the different results in our study compared to previous studies could have been patient selection, for example, patients with optic neuritis as initial presenting symptom 17 who are thought to have a more favorable disease course. 28 Differences in outcome could also be attributed to lower field strengths at the time, in combination with a low number of patients. 20
The combination of infratentorial and spinal cord lesions at baseline did not seem to be a better predictor than spinal cord lesions alone, possibly because spinal cord lesions in itself were already good predictors of disability progression. The combination of infratentorial and spinal cord lesions showed a higher risk of 11-year disability progression compared to only infratentorial lesions, but the value of these results is debatable. This result could be an effect of the low risk of disability progression seen in the individual analysis for infratentorial lesions combined with the strong predictive value of the spinal cord lesions separately. Moreover, the low number of patients showing disability progression after 11 years in the group with only infratentorial lesions make these results debatable as well. Besides, a combination of new infratentorial and spinal cord lesions even resulted in a lower risk of long-term disability progression than patients with only infratentorial lesions. This suggests that the development of new lesions in this area, even more than lesions at baseline, is important in respect to future disability, while spinal cord lesions at baseline were more important predictors than new developing spinal cord lesions.
Although the combination of infratentorial and spinal cord lesions was not compared to these locations individually before, two other studies evaluated infratentorial as well as spinal cord lesions in isolation, but not their cumulative value.16,17 Despite the differences in terms of study design and patient selection, in these studies, new infratentorial or spinal cord lesions resulted in a higher risk of medium-term disability.16,17 Moreover, the presence of baseline spinal cord lesions only predicted medium-term disability progression in the optic neuritis cohort. 17
Despite a long FU and a well-documented cohort, some limitations should be mentioned. The unexpected trend toward a lower risk of 11-year disability for patients with infratentorial lesions could be due to loosing FU of patients with higher disability, although the patients who were lost during FU did not differ on baseline characters. Subsequently, subdivision of patients into four smaller groups might have resulted in a loss of power to find statistical differences; moreover, the patients without spinal cord lesions nor infratentorial lesions have a high baseline EDSS and high percentage showed disability progression. Larger cohort studies with long(er) FU are necessary to further explore the role of early infratentorial and spinal cord lesions on disability progression, especially long-term disability progression. Also, connectivity and atrophy of cerebellum, brainstem,29,30 and spinal cord19,31 might have been interesting to examine in relation to disability progression, but unfortunately this was not possible using data from this cohort.
Conclusion
The presence of spinal cord lesions close to symptom onset appears to be a dominant predictor of disability progression, and new developing infratentorial lesions showed a trend to higher risk of long-term disability progression. The presence of simultaneous infratentorial and spinal cord lesions does not seem to result in an undisputedly worse outcome on disability progression compared to patients with only infratentorial lesions or only spinal cord lesions.
Supplemental Material
MSJ864933_supplemental_table – Supplemental material for Infratentorial and spinal cord lesions: Cumulative predictors of long-term disability?
Supplemental material, MSJ864933_supplemental_table for Infratentorial and spinal cord lesions: Cumulative predictors of long-term disability? by Iris Dekker, Madeleine H Sombekke, Lisanne J Balk, Bastiaan Moraal, Jeroen JG Geurts, Frederik Barkhof, Bernard MJ Uitdehaag, Joep Killestein and Mike P Wattjes in Multiple Sclerosis Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: I.D. received speaking honoraria from Roche, outside the submitted work; M.H.S., L.J.B., and B.M. have nothing to disclose. F.B. serves as editorial board member of Brain, European Radiology, Neurology, Multiple Sclerosis Journal, and Radiology. He has accepted consulting fees from Bayer-Schering Pharma, Biogen-Idec, Teva, Merck Serono, Novartis, Roche, Janssen Research, Genzyme-Sanofi, IXICO Ltd, GeNEuro, Apitope Ltd and speaker fees from Biogen-Idec and IXICO. Has received grants from AMYPAD(IMI), EuroPOND (H2020), UK MS Society, Dutch MS Society, PICTURE (IMDI-NWO), NIHR UCLH Biomedical Research Center (BRC), and ECTRIMS-MAGNIMS. F.B. is supported by the NIHR UCLH Biomedical Research Center. J.J.G.G. reports research projects funded by Novartis, Biogen, and Genzyme. B.M.J.U. reports personal fees from Genzyme, Biogen Idec, Teva, Merck Serono, and Roche, outside the submitted work. J.K. reports grants and personal fees from Biogen Idec, Novartis, Merck Serono, Teva, Genzyme, and Roche, outside the submitted work. M.P.W. reports personal consultancy and speaking fees from Biogen, Novartis, Janssen, Roche, Celgene, IXICO, Sanofi Genzyme, Bayer Healthcare, Biologix, Genilac, and Merck Serono.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by Dutch MS Research Foundation, grants 02-358b, 05-358c, 09-358d, and 14-358e.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.