
Abstract
This retrospective cohort study assessed the timing of infusion-related adverse events (IAEs) during natalizumab (NTZ) administration in well-documented relapsing-remitting multiple sclerosis (RRMS) patients who had received NTZ infusions in our centre between 2006 and 2018. In 225 RRMS patients (14,174 NTZ infusions), 276 IAEs (1.95%) occurred in 60 patients. All documented severe IAE occurred during infusion. Of the 19 moderate adverse events, 17 were during infusion. None of the reactions that occurred after the infusion required intervention. These results suggest that post-infusion monitoring is not necessary in patients who do not have an adverse event during infusion.
Introduction
Despite substantial efficacy, natalizumab (NTZ) is a time-consuming therapy for relapsing remitting multiple sclerosis (RRMS) patients due to monthly administration and the need for monitoring. According to the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA), NTZ must be administered for over 1 hour and patients must be monitored during the infusion and for 1 hour afterwards, since NTZ can trigger infusion-related reactions.1,2
The two main types of infusion-related adverse events (IAEs) described during NTZ treatment are non-antibody-mediated infusion reactions and hypersensitivity reactions. The incidence of hypersensitivity reactions reported in the large AFFIRM and SENTINEL trials as well as other studies ranged from 1.3% to 6.3%, most often reported during the second infusion and with moderate severity.3–9 The occurrence of anti-drug antibodies is associated with a higher incidence of IAEs. 10 There is no evidence available about the timing of the immediate IAEs.
The objective of this retrospective cohort study is to assess the timing of IAEs, the nature of the specific reaction and the need for intervention.
Methods
All patients who had received NTZ treatment at our centre between January 2006 and May 2018, with a minimum age of 18 years at the time of treatment onset, were included. For each infusion, both specially trained multiple sclerosis (MS) nurses and doctors have entered details in the patients’ medical records on the IAE and intervention, if applicable. Medical records of all patients were scrutinised by the same investigator (F.C.L.) for retrospective data collection. Data were extracted on demographics (age, sex), NTZ treatment (start date of first NTZ infusion, date of reinitiation of NTZ if applicable, number of infusions) and on adverse events (type of adverse event, time of occurrence, number of infusions and intervention).
All reactions were categorised according to severity, using the Common terminology criteria for adverse events (CTCAE) scale. 11 Anti-NTZ antibodies were determined in all patients for whom the reaction was classified as severe. 12 Results are presented using descriptive statistics.
Results
Study population
The study population consisted of 225 RRMS patients, of whom 66 were male and 159 female, with an average age of 44.4 years (standard deviation (SD) = 10.2 years). Eighty patients were repeatedly tested JCV seronegative until May 2018 or until NTZ discontinuation; data on JCV status were missing in 16 patients. The total number of infusions was 14,174, with the number of infusions per patient ranging from 2 to 155 (median = 59). In 39 patients, NTZ infusions were reinitiated at least once after termination of the treatment due to pregnancy, raised JCV titre, side effects, advanced disease progression or their own initiative. The number of patients experiencing at least one infusion-related event was 60 (26.7%), in whom 276 IAEs occurred resulting in an overall IAE rate of 1.95% (276/14,174).
Severe IAE
A total of 11 severe IAE (4.0% of all IAEs) were observed in nine patients (4% of all patients), a summary is presented in Table 1. Except for one patient, for whom no complete information was available about the timing of the event, all severe IAEs started during the infusion. In total, seven out of the nine patients required withdrawal from NTZ. None of the severe reactions were considered as serious events or required medication other than clemastine intravenously (IV) or orally. All patients recovered without sequelae. In addition, in case 6, 8 and 9, a positive skin prick test against NTZ was found. Allergy to nickel or cobalt was the only common allergies (five out of the nine patients); two patients had no registered allergies. The majority of patients (six out of the nine) presenting with a severe IAE had detectable antibodies against NTZ (see Table 1). Remarkably, 7.75 years after cessation of NTZ a very high antibody titre was found in case 2.
Timing and characteristics of severe infusion-related events.
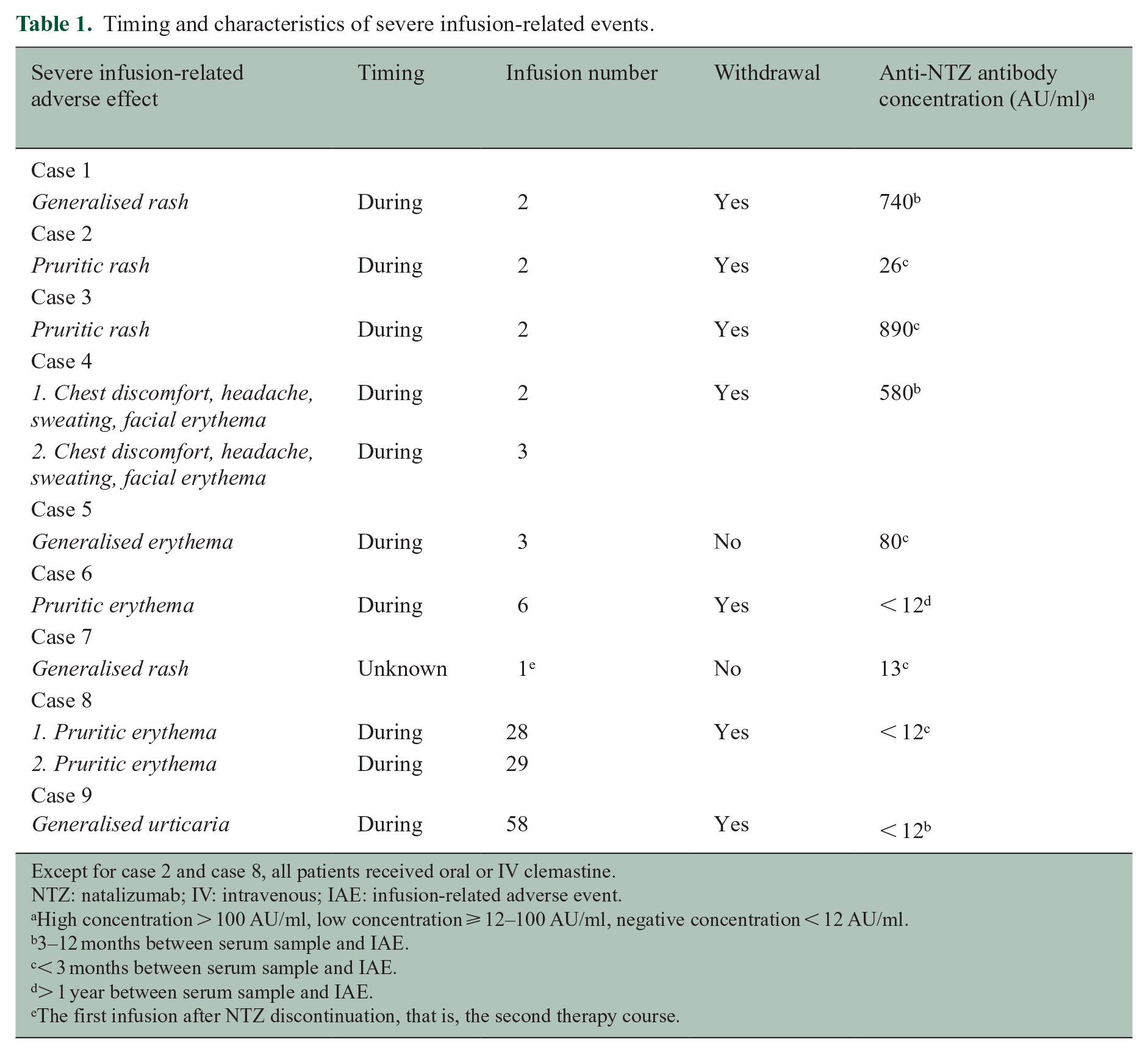
Except for case 2 and case 8, all patients received oral or IV clemastine.
NTZ: natalizumab; IV: intravenous; IAE: infusion-related adverse event.
High concentration > 100 AU/ml, low concentration ⩾ 12–100 AU/ml, negative concentration < 12 AU/ml.
3–12 months between serum sample and IAE.
< 3 months between serum sample and IAE.
> 1 year between serum sample and IAE.
The first infusion after NTZ discontinuation, that is, the second therapy course.
Moderate and mild IAE
The majority of IAEs were mild to moderate and were successfully managed without withdrawal of NTZ therapy. Details on the timing are presented in Table 2. Since the focus of this article is on the immediate reactions and delayed reactions by definition occur after the post-infusion monitoring period, these reactions were not included in the analyses. Fifteen patients experienced 19 moderate IAEs; 17 of the 19 moderate IAEs occurred during the infusion. Two reactions that occurred after the infusion did not require intervention. Almost all interventions consisted of symptomatic treatment, except a discontinuation of the infusion in three patients and one adjustment of the infusion rate.
Timing of moderate and mild infusion-related adverse events.
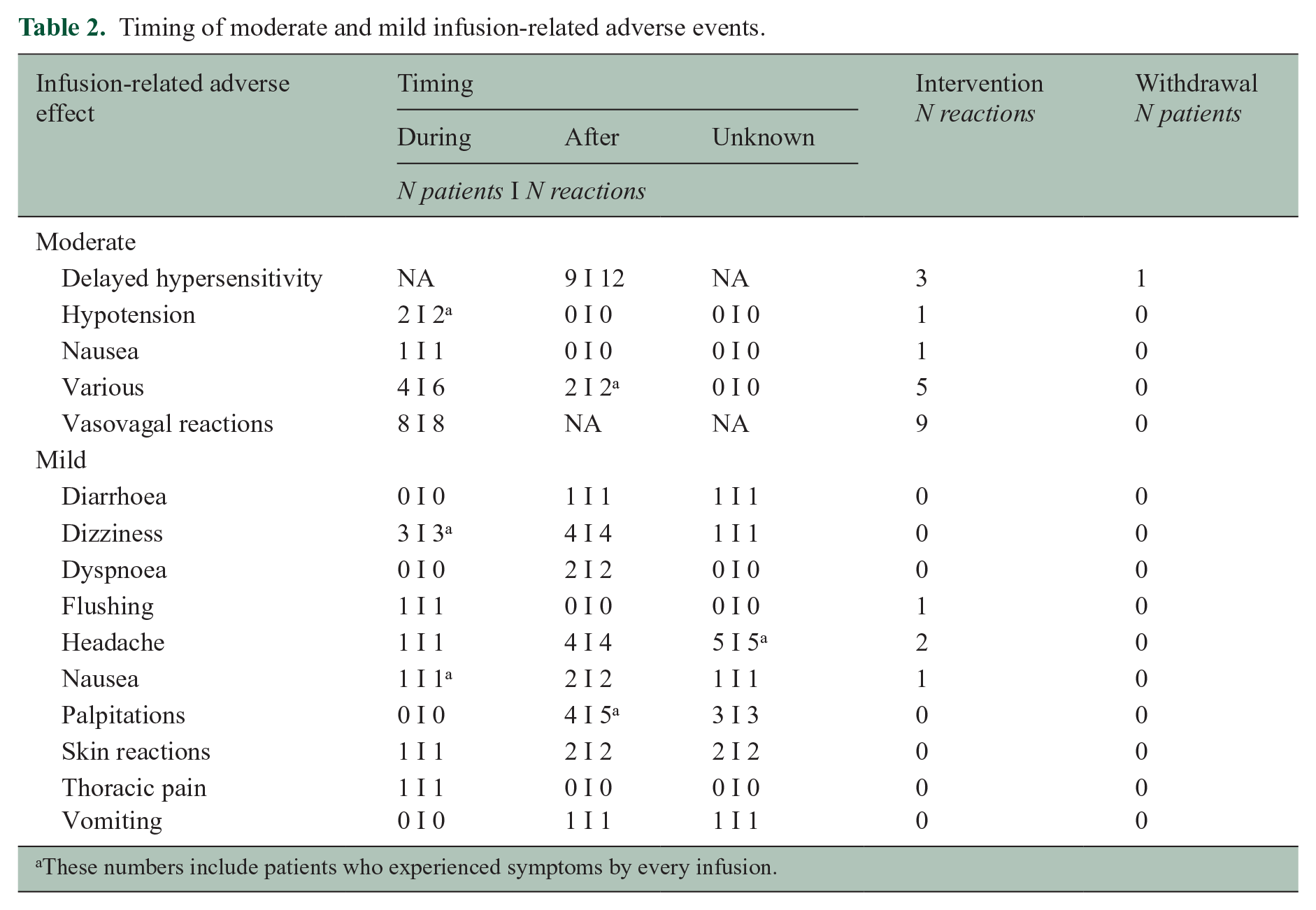
These numbers include patients who experienced symptoms by every infusion.
Forty-three IAEs occurred in the mild category. Four patients required precautions for the following infusion, such as slowing the infusion rate or prophylactic medication. Of the 16 patients with more than one IAE, six patients had the following allergies: nitrofurantoin, diclofenac, atopic eczema, aspergillus, ibuprofen and penicillins. The remaining 10 patients had no (known) allergies.
Discussion
We aimed to identify the timing of IAEs to assess the need for post-infusion monitoring and reviewed a total of 14,174 infusions over a follow-up period of 12 years. All documented severe reactions and all clinically relevant moderate reactions occurred during NTZ administration. Patients, who have not had any symptoms of an IAE during the infusion, did not develop a clinically relevant moderate or severe reaction after NTZ administration. Thus, the need for post-infusion observation will depend on the patients’ clinical status during the infusion. Consequently, our data suggest that patients who do not have an IAE while receiving NTZ treatment do not need to stay in the hospital for an additional observation hour.
The majority of patients presenting with a severe IAE had detectable antibodies against NTZ. The association between anti-drug antibodies and the occurrence of IAE is well recognised. 10 In line with previous research, our results confirm that NTZ antibodies develop early during treatment.10,12 Therefore, special caution is recommended during administration of infusion number 2 and 3. However, our data suggest that even in early treatment post-infusion monitoring is unnecessary if no IAE occur during infusion.
Although the prospective nature of the data collection of this NTZ cohort can be considered as a significant advantage, specific data on the timing of IAE has been collected retrospectively, which has possible limitations. However, we have been able to review a large number of infusions with an accurate description of the timing and comprehensive information about the nature of the side effects in the large majority of events.
If confirmed in other cohorts, post-infusion monitoring during NTZ treatment could safely be omitted from clinical protocols and regulatory recommendations. This will result in improved patient care in terms of efficiency and patient satisfaction, and reduce health care costs, without jeopardising patient safety.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: F.C.L., J.A.v.R. and Z.L.E.v.K. do not report any competing interests. T.R. has received grant support from Genmab, other from Regeneron, other from AbbVie, other from Pfizer, during the conduct of the study. B.M.J.U. reports personal fees from Genzyme, Biogen Idec, TEVA, Merck Serono and Roche outside the submitted work. J.K. has accepted speaker and consulting fees from Merck-Serono, Biogen, Roche, Teva, Genzyme and Novartis.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.