
Abstract
Objectives:
The impact of physical disability in multiple sclerosis on employment is well documented but the effect of neurological symptoms has been less well studied. We investigated the independent effect of self-reported fatigue and cognitive difficulties on work.
Methods:
In a large European cost of illness survey, self-reported fatigue, subjective cognitive impairment (SCI), and productivity at work were assessed with visual analogue scales (VAS 0–10). The analysis controlled for country, age, age at diagnosis, gender, education, and physical disability.
Results:
A total of 13,796 patients were of working age and 6,598 were working. Physical disability had a powerful impact on the probability of working, as did education. The probability of working was reduced by 8.7% and 4.4% for each point increase on the VAS for SCI and fatigue, respectively (p < 0.0001). Regular work hours decreased linearly with increasing severity of fatigue and cognitive problems, while sick leave during the 3 months preceding the assessment increased. Finally, the severity of both symptoms was associated with the level at which productivity at work was affected (p < 0.0001).
Conclusion:
Our results confirm the independent contribution of self-reported fatigue and SCI on work capacity and highlight the importance of assessment in clinical practice.
Background
The past few decades have witnessed a growing public interest in the impact of diseases on employment and work impairment. There is an ongoing debate regarding the role of production losses in decisions about public funding of treatments,1,2 but few funders include them formally in their decision-making. However, particularly in disabling diseases such as multiple sclerosis (MS), the impact on work capacity is not only substantial3,4 but also very relevant for any economic assessment. 5 Unemployment poses a large burden on individuals and their family, in terms of financial loss, social withdrawal, reduced physical activity, and more formally, psychiatric morbidity. Reduced work capacity has major economic implications for society when individuals no longer participate in productive activities.
MS is the most common non-traumatic disabling condition that affects young adults 6 and over time causes physical disability in the majority of people with MS, 7 with a limited impact on mortality. 8 As a result, the socioeconomic impact of MS is high 5 and studies have consistently shown that the probability of working with MS is lower than for the general population. 3 Shorter working hours, sick leave, poor work performance, and early retirement are common. 4 Most large studies on employment in MS have focused on physical disability as the cause for reduced work capacity.3,4 The role of more “invisible symptoms” such as subjective cognitive impairment (SCI) and fatigue is less clear and lack of awareness of these symptoms may lead to unnecessary loss of work. 9
Disability is generally measured with the Expanded Disability Status Scale (EDSS) 10 which focuses predominantly on ambulation. EDSS has been shown to be a strong predictor of workforce participation. 4 However, even at low EDSS, when minimal physical disability is present, workforce participation is significantly affected. In the most recent large survey in 16 countries in Europe, 54% of people with MS at or below EDSS 3 were not working. 4 This indicates that the EDSS does not capture prominent non-physical symptoms, such as fatigue and cognitive impairment, that may play a role in the decision to reduce or abandon employment. In MS patients with EDSS ⩽ 4, objective cognitive impairment is missed by clinicians in 25% of patients. 11 Fatigue and SCI have also been linked to workplace accidents, when physical disability was not. 12 MS patients often describe fatigue as their main problem.13,14 There is also an indirect effect: fatigue and objective cognition have been shown to mediate the role of physical disability in employment. 15
The presence of fatigue in MS has been well studied and estimated at 50%–90% in different studies, with the range explained by differences in study populations and assessment methods.4,13,16,17 The latter range from lengthy psychometric instruments (Fatigue Severity Scale, FSS; 18 Multidimensional Fatigue Inventory, MFI 19 ) to a simple yes/no question followed by an enquiry about the degree of severity (visual analogue scale, VAS4). Self-reported fatigue was investigated in a large registry study in the United States and was linked to unemployment. 20 Fatigue has been conceptualized either as a direct primary consequence of the MS pathology or as secondary to other factors such as socio-demographic conditions, pain, and psychiatric comorbidities that are all more common in individuals with fatigue.21,22 The former may partly explain the fact that fatigue increases with time and with impaired mobility, the latter that substantial fatigue is present at all stages of disability. 23
Cognitive impairment is present in 40%–65% of people with MS.24,25 This is also reflected in a recent European cost of illness survey where two thirds of participants reported some level of cognitive impairment. 4 Symptoms include deficits in complex attention, efficiency of information processing, executive functioning, processing speed, and long-term memory. 26 Although cognitive impairment in MS has long been observed, it has received focus only in recent years. 24 Until recently, formal cognitive assessment was at best available in university centers, but a new brief instrument with international validation is becoming established and linked to everyday task performance, including employment.27–29 Self-report data on SCI have been collected in small studies and large surveys.30,31
A number of studies in MS have explored the effect of fatigue and/or cognitive impairment on employment.32–36 However, most studies were based on small, geographically delimited samples. We used a large survey on the burden of MS in Europe to further investigate work impairment associated with the presence of fatigue or SCI. 4
Methods
Data
The European cost of illness survey included a total of 16,808 patients from 16 countries, recruited with the help of local MS societies. 4 The cross-sectional study was approved by local ethics committees, and the data were collected with a standard questionnaire that people with MS could complete either online or on paper. Questions related to demographics (age, gender, education, work situation), disease manifestations (self-assessed EDSS, relapses, fatigue, SCI), health-related quality of life (HRQoL), inpatient and outpatient care, equipment and investments, community, and family assistance. As both HRQoL and costs have been shown to be correlated with EDSS, the aim was to obtain country samples where all levels of physical disability were well represented (n = 400–500). The samples therefore do not reflect the prevalence of the type and severity of the MS population in the countries. The sample from Russia (n = 208) was excluded from the analysis due to its limited size and also the fact that participants were not recruited by the patient association as in all other countries but in a single specialized clinic in Moscow.
For people in employment or self-employment, the information included the number of weekly working hours, the reason for not working full-time (if applicable), and the number of days of sick leave during the past 3 months; for those not in employment, it included the reasons for not working or having left the workforce. In economic surveys, the impact of diseases on work productivity is most often assessed with the Work Productivity and Activity Impairment (WPAI) questionnaire. 37 The instrument assesses the overall impact while at work with a VAS and this VAS was included in the survey.
In view of the objective to assess the impact of fatigue and SCI on work capacity, not fatigue and cognition per se, these were self-assessed using VAS ranging from 0 (no fatigue, no cognitive difficulties) to 10 (severe fatigue, severe SCI), preceded by a yes/no question. In addition, a description of difficulties in cognition was provided. 26
Analysis
Demographics are presented for the total study population. For the analysis of work impairment, only participants of working age at the time of the survey were included (18–65 years). As both the legal retirement age and the effective retirement age among the countries vary considerably, we chose an average upper limit at 65 years; the lower limit was given by the study protocol that excluded participation below 18 years.
To obtain a representative sample of European MS patients, each observation was assigned a weight proportional to the share of the European MS population estimated to be living in each country 38 divided by the share of the study sample derived from that country (see Table 1). Binary outcome variables (employment status) were analyzed with logistic regression, while continuous and count data (hours worked, sick leave days, work tasks affected) were analyzed with ordinary least squares linear regression. In regression equations, symptom scores (self-reported fatigue and SCI) and age were included as continuous explanatory variables, while all other regressors were represented by dummy variables. The 95% confidence intervals around mean values for continuous outcomes were constructed based on standard normal approximation.
Subject count per country.
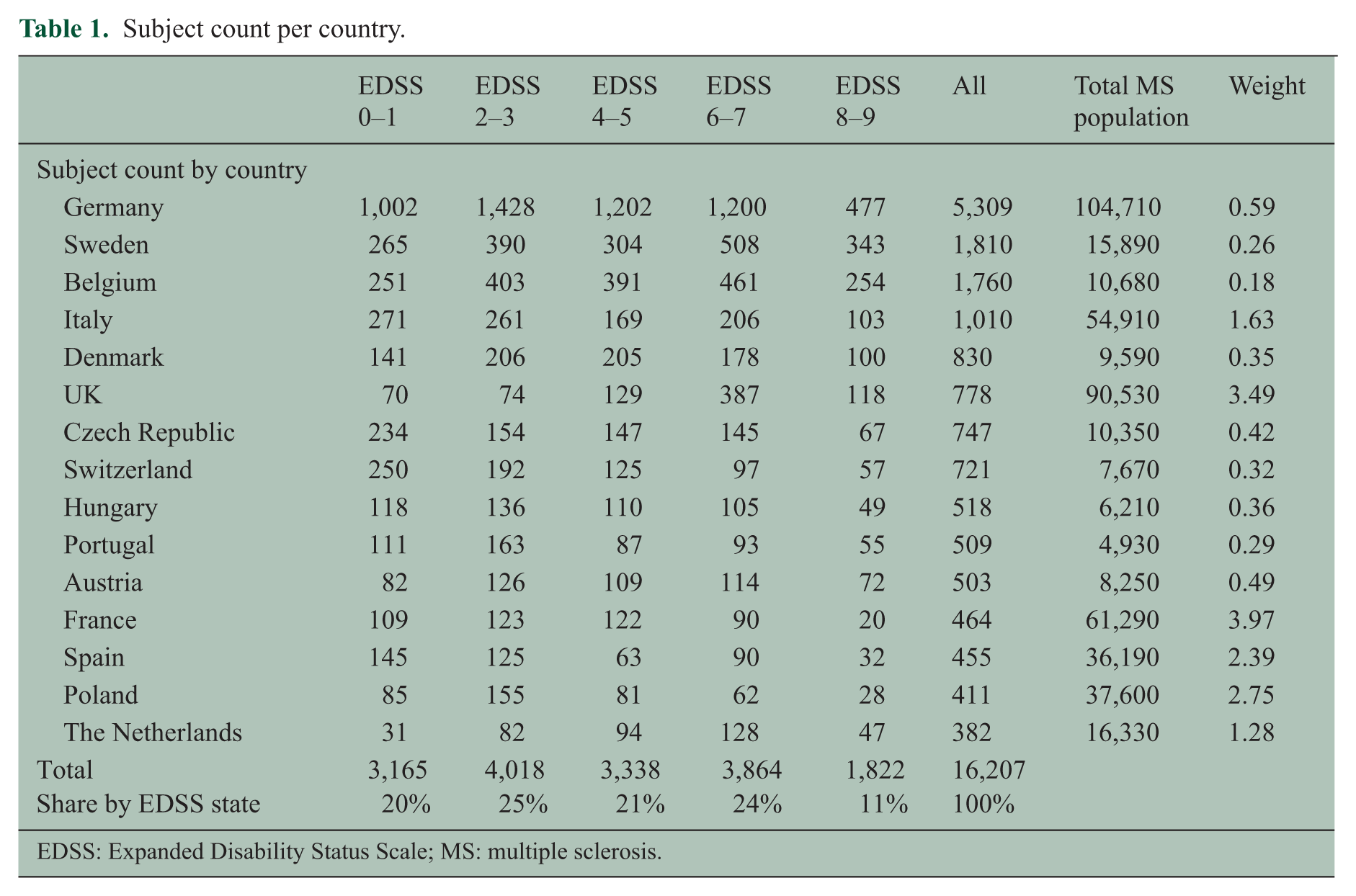
EDSS: Expanded Disability Status Scale; MS: multiple sclerosis.
Results
A total of 16,207 subjects with available EDSS scores (2.4% missing) were included in the study. The country samples were not proportional to the prevalence of MS in the different countries; for instance, recruitment in Sweden, Belgium, and Portugal was proportionally higher than the recruitment in France, Czech Republic, and Poland, in relation to the overall MS population in each country. 38 Almost a third of participants came from Germany. Also, the distribution across disease severity does not represent prevalence, as the study aimed at enrolling equal numbers at all EDSS levels in order to analyze resource use data by severity. However, there were fewer patients at EDSS 0 and EDSS 9, and in order to obtain an even distribution in this analysis, we present the analysis for five severity groups. Table 1 shows the distribution of the sample across EDSS levels.
Table 2 presents demographics, self-assessed symptoms (fatigue, SCI), and work capacity by EDSS level as well as the details on the number of hours worked. Participants were on average 51 years of age at the time of the survey, 26% were male. On average, they first experienced symptoms of MS at age 30 and were diagnosed 6 years later. For subjects with a more recent diagnosis, the time to confirmed diagnosis was shorter as a likely consequence of both revised diagnosis criteria 39 and more focus on early diagnosis. 40 Educational levels were high, possibly due to the fact that the survey was primarily completed electronically. Employment declined rapidly with advancing EDSS. Overall working hours in the sample were reduced at all levels of disease severity.
Demographics, all subjects (n = 16,207).
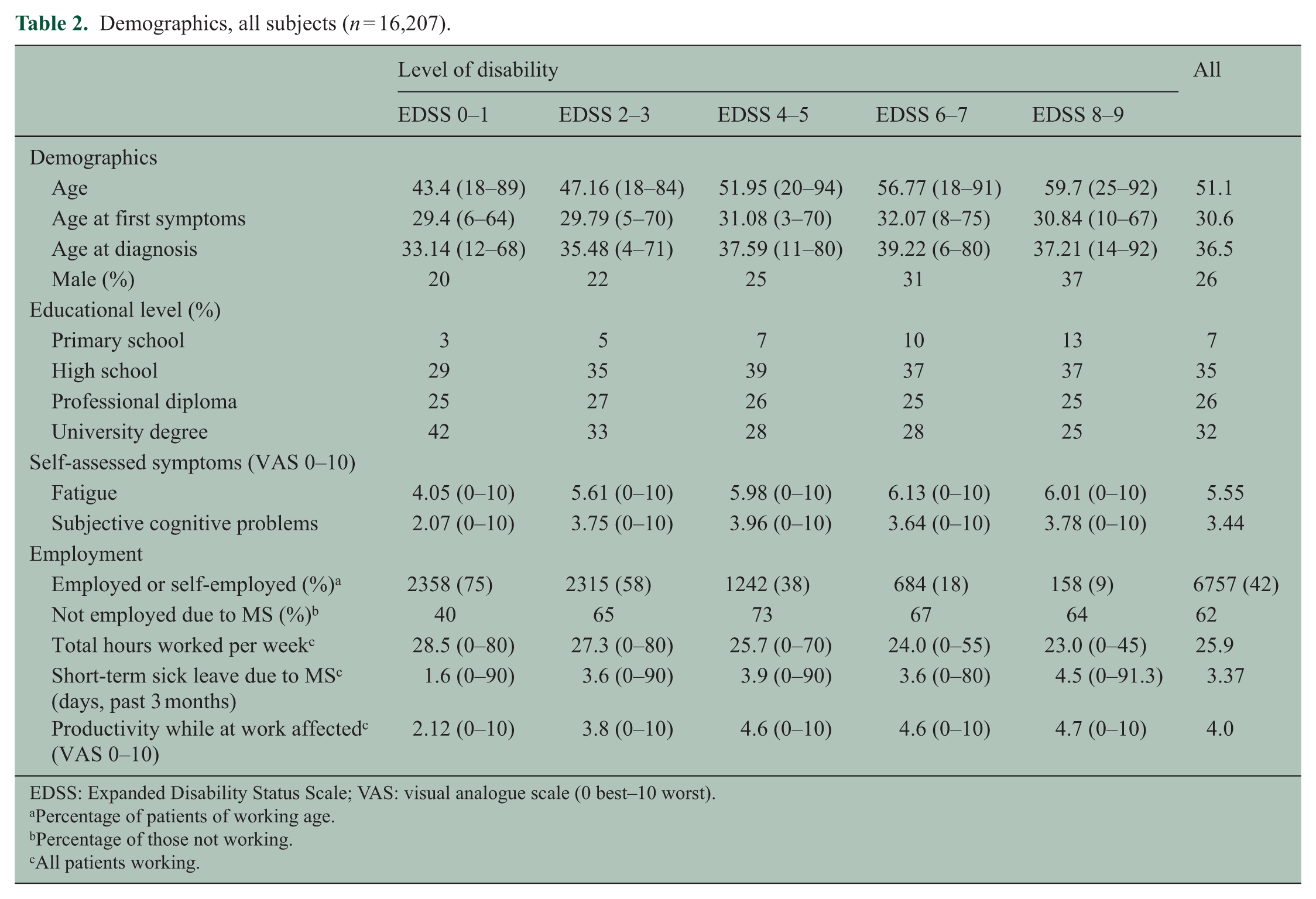
EDSS: Expanded Disability Status Scale; VAS: visual analogue scale (0 best–10 worst).
Percentage of patients of working age.
Percentage of those not working.
All patients working.
Probability of employment
Table 3 presents results from a fixed-effects logistic regression where country, demographics, and symptom scores explain the probability of being employed/self-employed. A total of 13,796 subjects at working age (18–65 years) and with available data on work capacity and symptoms were included in this analysis. Among these, 6,598 (48%) were gainfully employed or self-employed.
Logistic regression on probability of being employed or self-employed.
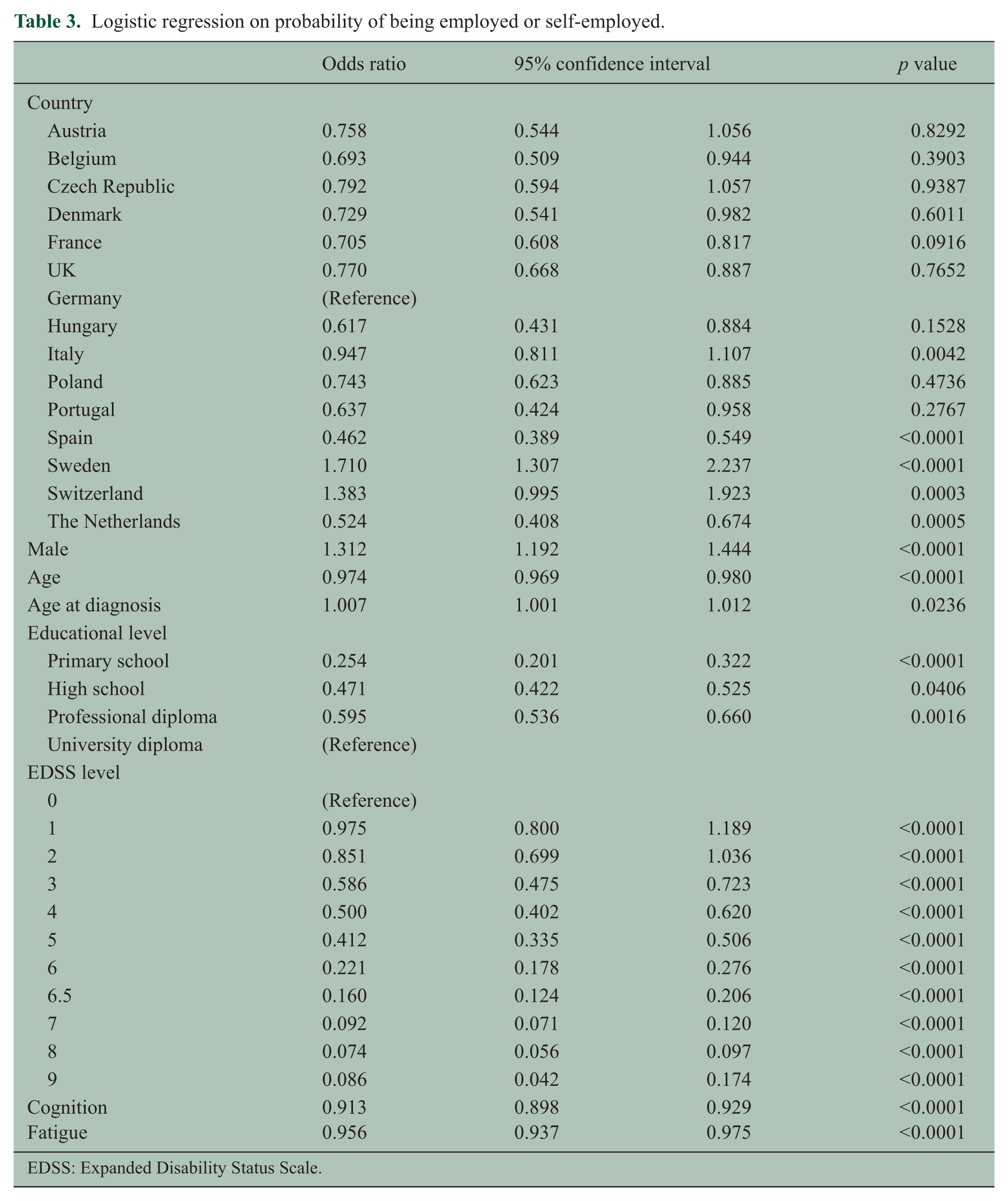
EDSS: Expanded Disability Status Scale.
Participation in the workforce is affected by a number of factors not specific to the individual patient, such as geographic location, local socioeconomic and cultural circumstances. Patients in Sweden and Switzerland were more likely to work, while the probability of working was lower in Spain, Italy, and the Netherlands. Men and those with higher educational levels were more likely to be working.
However, the degree of physical disability and the severity of symptoms (fatigue, SCI) all had an independent impact on the probability of working. Patients with EDSS scores of 7 or above were more than 10 times more likely not to be working than those with no disability. The probability of working was reduced by 8.7% and 4.4% for each point increase on the 10-point VAS of SCI and fatigue, respectively.
Working hours related to SCI and fatigue
Among the 6,598 subjects who were employed or self-employed at the time of the survey, many worked reduced hours due to MS or for other reasons. Figure 1 presents the average number of hours worked per week in relation to the severity of SCI and fatigue.
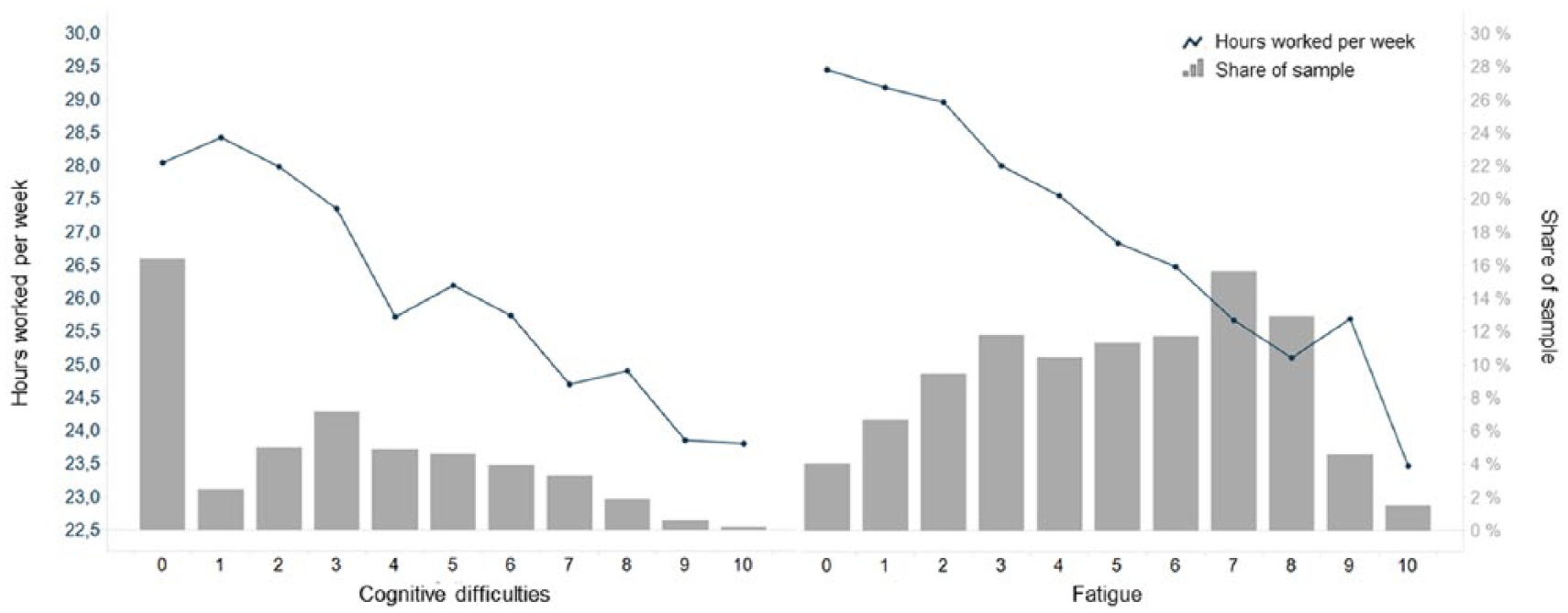
Hours worked per week in relation to self-reported cognitive function and fatigue: The average number of hours worked per week in relation to the severity of cognitive symptoms (line in left pane) and fatigue (line in right pane), respectively. Bars represent the share of the sample within each category of symptom severity. Cognitive symptoms and fatigue were self-assessed on a visual analogue scale where 0 indicates no symptoms and 10 severe symptoms. The analyses controlled for country, gender, age, disease duration, educational level, and physical disability (EDSS score).
A third of patients had no subjective SCI, while only 4% of patients reported no fatigue. The number of hours worked per week decreases linearly with the degree of SCI as well as with the degree of fatigue. In a multivariate linear regression controlling for age, gender, country, education, and EDSS, a 1-point change in SCI was associated with 0.19 hours less worked per week (p < 0.0001). The change in work hours associated with a point increase in fatigue was not statistically significant (0.047, p = 0.37).
Short-term leave of absence related to SCI and fatigue
Among those working and not on long-term sick leave, 1,336 patients (20.2%) had been on sick leave in the past 3 months. Figure 2 presents the average number of days of sick leave in the past 3 months in relation to SCI and fatigue. The number of sick leave days was positively related both with SCI and fatigue. Confidence intervals were wide, in particular, in groups with higher level of symptom severity due to the small number of subjects. Each point increase in symptom severity (cognitive function or fatigue) was associated with an additional 0.2 sick days per 3 months in a linear regression model controlling for country, gender, age, age at symptom debut and diagnosis, educational level, and EDSS score.
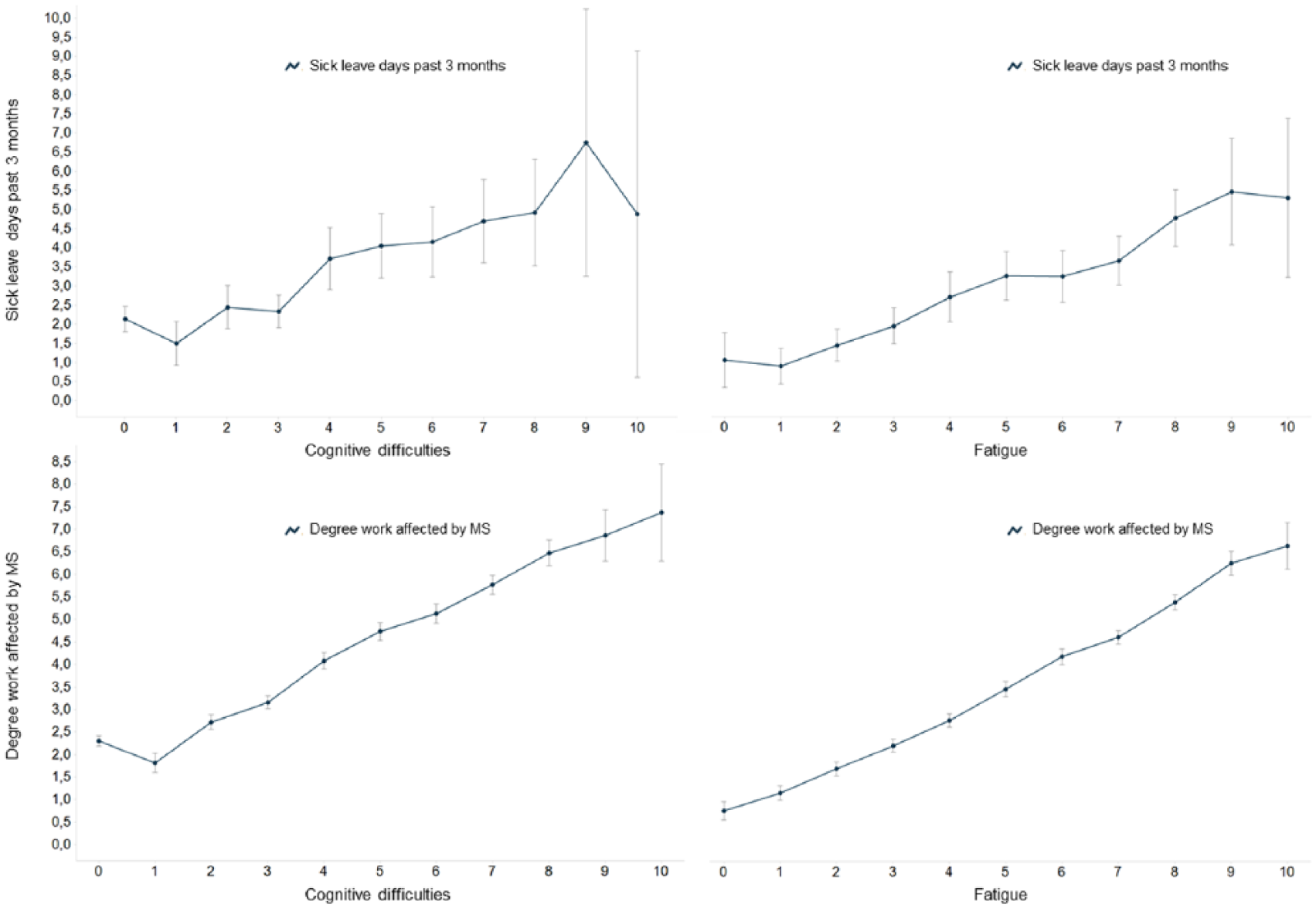
Sick leave days and degree work affected in relation to cognitive difficulties and fatigue: The average number of days of sick leave in the past 3 months, and the effect of MS on the ability to complete work tasks, in relation to subjective cognitive problems (left pane) and fatigue (right pane). Cognitive symptoms, fatigue, and the impact on productivity while at work were self-assessed on visual analogue scales, where 0 indicates no symptoms/impact and 10 severe symptoms/impact. The analyses controlled for country, gender, age, disease duration, educational level, and physical disability (EDSS score).
Effect of MS on work tasks while working
MS affected patients’ ability to complete their tasks while at work. The degree of SCI and fatigue, respectively, both measured on a 0–10 scale, has an almost linear association with how much patients were affected in their work (Figure 2). Confidence intervals are narrow except for in the most severe symptom categories with few individuals. Controlling for country, gender, age, age at symptom debut and diagnosis, educational level, and EDSS score, a 1-point increase in SCI and fatigue, respectively, was associated with 0.41- and 0.28-point increase on the 10-point VAS measuring how work is affected by MS (p < 0.0001 for both).
Discussion
Advancing physical disability as measured by the EDSS has been shown in many studies to negatively impact workforce participation of people with MS.3,4 However, employment is affected by MS very early in the disease, at low EDSS levels where virtually no physical disability is present. 4 In our study, 25% of participants with an EDSS of 0-1 (mean age 43 years) were not working, and some of them had already obtained invalidity pensions. Clearly, disease manifestations other than ambulation have an impact as well. Employment is, however, also affected by personal and external factors not related to the disease, such as age, gender, education, socioeconomic conditions, as well as the country of residence and its economic performance.
Our analysis shows that fatigue and SCI, as judged by the patients themselves on a 10-point VAS, directly and independently affect employment regardless of physical disability, age, gender, education, and country of residence (Table 2). They also affect the number of hours regularly worked (Figure 1) and the number of days of sick leave (Figure 2). Finally, the correlation with symptom severity and the negative effect on productivity while working is almost linear.
This is the largest study so far to investigate how these symptoms relate to work capacity, and the size of our sample allowed many of the factors that are important for employment (age, education, gender, country, disease duration, EDSS) to be controlled for, thus isolating the effect of SCI and fatigue. While other studies have addressed the same question, sample sizes were often too small to control for the large number of factors affecting employment and their interrelation.
There are a number of issues in our study that require discussion. Fatigue and SCI are present not only in people with MS but also in the general population. In an ideal world, we would have included a control group to exclude symptoms unrelated to MS. However, such data are not readily available as population registries will not include the symptoms, and collecting data from a matched sample was unrealistic in terms of time and resource demands. Fatigue and SCI are much more prevalent in the MS population.
We have assessed the presence of SCI and fatigue, as well as their severity, with a binary question followed by a 10-point VAS on the severity of the symptoms. Ordinal scales have been shown to be useful for evaluating other subjective symptoms, including cognition, as the obtained scores can be readily analyzed using standard statistical tests. 41 In our study, the use of simple questions is justified by the length of the survey questionnaire, the large sample and the complete anonymity of the participants, and thus the uncontrolled conditions during which patients completed the survey. Most importantly, however, our purpose was to investigate how the respondents judged these problems and their impact on their employment, not to clinically assess fatigue and cognition.
Self-assessment has been used in registry studies for assessing fatigue, 20 and our results for SCI across all physical impairment categories are in line with other large surveys. 31 Some studies have shown that the correlation between self-reported and objective assessment of cognition was weak. 42 Despite this, a more recent study found that both MS patients’ self-reported and objective cognitive performance predicted both employment and working hours. 43 It is also important to note that SCI in MS has been linked to mood, depression, and other psychosocial factors. 23 We cannot exclude that at least some of the reports of poor cognition and high fatigue are the result of low mood, and that depression is affecting productivity at work and employment. However, a previous study demonstrated that while depression was related to shorter working hours, it did not explain the relationship between perceived cognitive difficulties and the work outcomes. 43 Also, depression was shown to have no individual contribution to employment status, whereas fatigue and objective cognitive status did. 15 Finally, while we cannot rule out that some people wrongly attributed a poor work record to diminished cognition, rather than actual diminished cognition being the cause of their employment difficulties, this is unlikely to have an effect in such a large sample. Also, there is now convincing evidence linking objectively poor cognitive performance to employment performance. 25
Conclusion
How people feel affects their daily activities, family life, and employment. People with MS have to cope with many “hidden” symptoms, often unnoticed in the context of overwhelming physical handicap. In recent years, there has been an increased focus on these symptoms and studies are performed to assess them objectively. Our purpose was to investigate whether fatigue and SCI reported by patients could be linked to reduced work capacity. While our results unsurprisingly confirm that EDSS is highly correlated with reduced employment, SCI and fatigue had an independent link not only to employment itself but also to more subtle work performance issues such as work hours, sick leave, and productivity while working. Our data set did not, however, allow us to assess their effects on other activities of daily living, and more research into this aspect is certainly warranted.
Our results support the call for incorporating assessment of these symptoms in routine clinical practice to detect changes 27 and developing strategies for treatment adapted to individual patients. 44 Regular assessments could predict some of the work difficulties MS patients may encounter, and, conversely, patients who experience challenges at work or receive poor employment appraisals should be assessed for fatigue and cognitive impairment. 30 Other authors have suggested that MS patients with known fatigue or cognitive impairment should be offered support at work, including employer liaison.45,46
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: G.K. has provided consulting and speaking services to from Almirall, Bayer, Biogen, Merck Serono, Novartis, Oxford PharmaGenesis, Roche, Sanofi Genzyme, and Teva. D.L. has participated in speaker bureaus for Bayer, Merck, Almirall, Execemed, Teva, Roche, Novartis, Biogen, and Sanofi; has consulted with Novartis, Bayer, Merck, Biogen, Teva, and Sanofi; has had research grants from Bayer, Merck, Novartis, and Biogen. All fees are paid into her institution. L.J. is employed by H. Lundbeck and has provided consulting and advisory services to Ipsen, Pfizer, Merck, Sanofi, and Biogen.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by an independent grant from Biogen who had also provided financial support for the original collection of data used. The sponsor has in no way interfered with or influenced the analysis and the manuscript.