
Abstract
Imaging markers that are reliable, reproducible and sensitive to neurodegenerative changes in progressive multiple sclerosis (MS) can enhance the development of new medications with a neuroprotective mode-of-action. Accordingly, in recent years, a considerable number of imaging biomarkers have been included in phase 2 and 3 clinical trials in primary and secondary progressive MS. Brain lesion count and volume are markers of inflammation and demyelination and are important outcomes even in progressive MS trials. Brain and, more recently, spinal cord atrophy are gaining relevance, considering their strong association with disability accrual; ongoing improvements in analysis methods will enhance their applicability in clinical trials, especially for cord atrophy. Advanced magnetic resonance imaging (MRI) techniques (e.g. magnetization transfer ratio (MTR), diffusion tensor imaging (DTI), spectroscopy) have been included in few trials so far and hold promise for the future, as they can reflect specific pathological changes targeted by neuroprotective treatments. Position emission tomography (PET) and optical coherence tomography have yet to be included. Applications, limitations and future perspectives of these techniques in clinical trials in progressive MS are discussed, with emphasis on measurement sensitivity, reliability and sample size calculation.
Introduction
During the last 20 years, over a dozen of disease-modifying treatments (DMTs) received the approval for the treatment of relapsing–remitting multiple sclerosis (RRMS), being facilitated by screening the anti-inflammatory activity of putative treatments using active magnetic resonance imaging (MRI) lesions as outcomes in phase 2 trials. On the contrary, the paucity of active medications for both primary progressive multiple sclerosis (PPMS) and secondary progressive multiple sclerosis (SPMS) is striking. In view of this, the Progressive MS Alliance recently suggested to develop and to validate biomarkers of progression that could make clinical trials for progressive multiple sclerosis (MS) less time- and resource-consuming, when compared with conventional clinical measures. 1 This could be achieved with the identification of reliable, reproducible and sensitive-to-change imaging outcomes.
Several MRI measures reflect the neurodegenerative pathology of progressive MS and hold promise for clinical trial applications in this population. Along with the use of conventional MRI metrics (e.g. brain volume, lesion count and volume), advanced MRI techniques and optical coherence tomography (OCT) are also emerging as candidate imaging outcomes of MS progression. Indeed, the number of imaging outcomes included in clinical trials for progressive MS has almost doubled from 2.3 ± 1.5, in the decade 1996–2006, to 4.1 ± 2.6 in most recent years (2007 to current) (Figure 1).
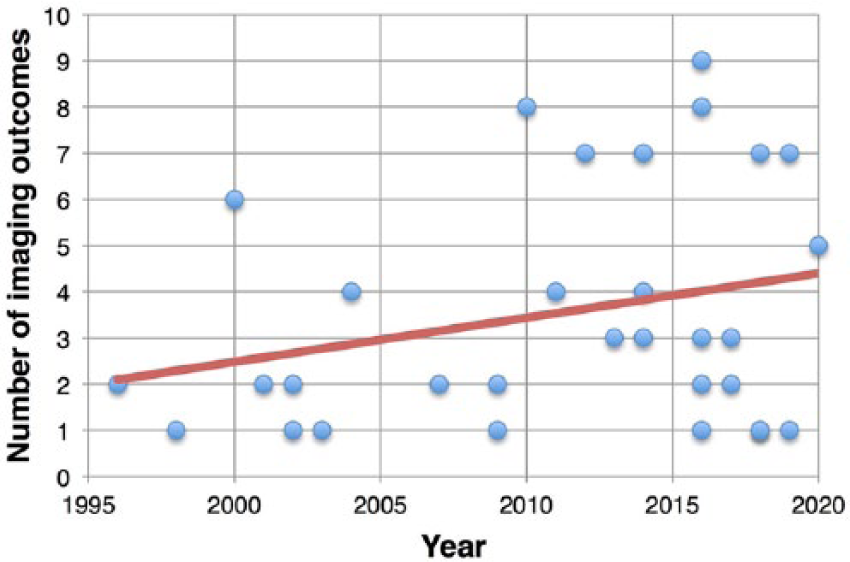
Clinical trials and imaging outcomes. Scatter plot shows the number of imaging outcomes used in clinical trials conducted from 1996 up to recent years (the expected conclusion date has been used for ongoing clinical trials).
In this review, we will discuss imaging biomarkers, which have been included in phase 2 and 3 clinical trials for progressive MS and those emerging for the future. Methodological and statistical drawbacks will be also discussed.
Brain lesion count and volume
Lesion counts were the first MRI-derived outcome for MS clinical trials and include the number of gadolinium-enhancing and new/enlarging T2 lesions, and their related volumes. Lesion measures are the best biomarker of active inflammation in MS, allowing the screen for early disease activity in phase 2 clinical trials in RRMS. 2 On the contrary lesion-derived measures play a secondary – but not negligible – role in the study of progressive MS. In PPMS, the burden of T2-visible lesion load and of gadolinium-enhancing lesions is low, despite clinical severity 3 and seems to have only a minimal impact on the disability accrual over time. 4
MRI measures of focal brain lesions are the most common imaging metric in phase 2 and 3 clinical trials in progressive MS.5–30
Future clinical trials on progressive MS might include these outcomes if the presence of inflammation is expected and targeted. Indeed, trials might pick populations with relatively high inflammatory activity, depending on inclusion/exclusion criteria (e.g. 24.7%–27.5% of PPMS patients presented with Gd-enhancing lesions at baseline visit of the ORATORIO trial). 7 However, clinical outcomes might be difficult to predict based on results on lesion measures. Indeed, the use of DMTs specifically designed for RRMS in clinical trials in progressive MS can result in a positive effect on lesion count and volume measures but not on neurodegenerative clinical (e.g. disability progression) and imaging outcomes (e.g. brain and spinal cord (SC) atrophy), as occurred in the INFORMS trial.5,31 Similarly, use of interferon-beta in SPMS was associated with fewer active lesions, but no effect was established on clinical disability. 32
Global and regional brain atrophy
Brain atrophy is detectable on MRI scans from the earliest clinical stages of MS and is a biomarker of irreversible neurodegenerative processes. 33 Global brain atrophy has been associated with the degree of disability in large cohorts of both RR and progressive MS.34,35 Besides, improvements in MRI post-processing have allowed to segment white matter (WM) and grey matter (GM) (both cortical and deep) separately, allowing refinement of association with clinical features.36,37 Regional volumes might show a greater change over time, 12 resulting in higher sensitivity and smaller sample size when compared with global measures. 38
Intriguingly, brain atrophy has not been associated with relapse risk in RRMS, suggesting that atrophy is probably driven more by (possibly independent) neurodegenerative changes than inflammatory lesions, which further support the use of this measure in progressive MS. 33
There are several methods to quantify whole-brain atrophy. In general, brain tissue volume needs to be normalized for head size, and longitudinal changes can be detected using registration- and segmentation-based techniques. Registration-based methods compare longitudinally acquired images and measure changes in brain surface; structural image evaluation using normalization of atrophy (SIENA) is the most popular example. Segmentation-based techniques measure brain volume on a single scan and then determine change over time indirectly and include brain parenchymal fraction (BPF) (which is the ratio of brain parenchymal volume to the total volume within the brain surface contour).33,39 In comparative analyses, brain atrophy measured with registration-based techniques showed better reproducibility 40 and higher power to detect treatment effect, when compared with segmentation-based.41,42
Whole-brain atrophy has been included in several phase 2 and 3 clinical trials in progressive MS as primary8,9,12,15,43–46 or secondary outcome (Table 1).5–7,11,13,14,16–18,21–24,26,30,50–52
Clinical trials in progressive MS using imaging outcomes.
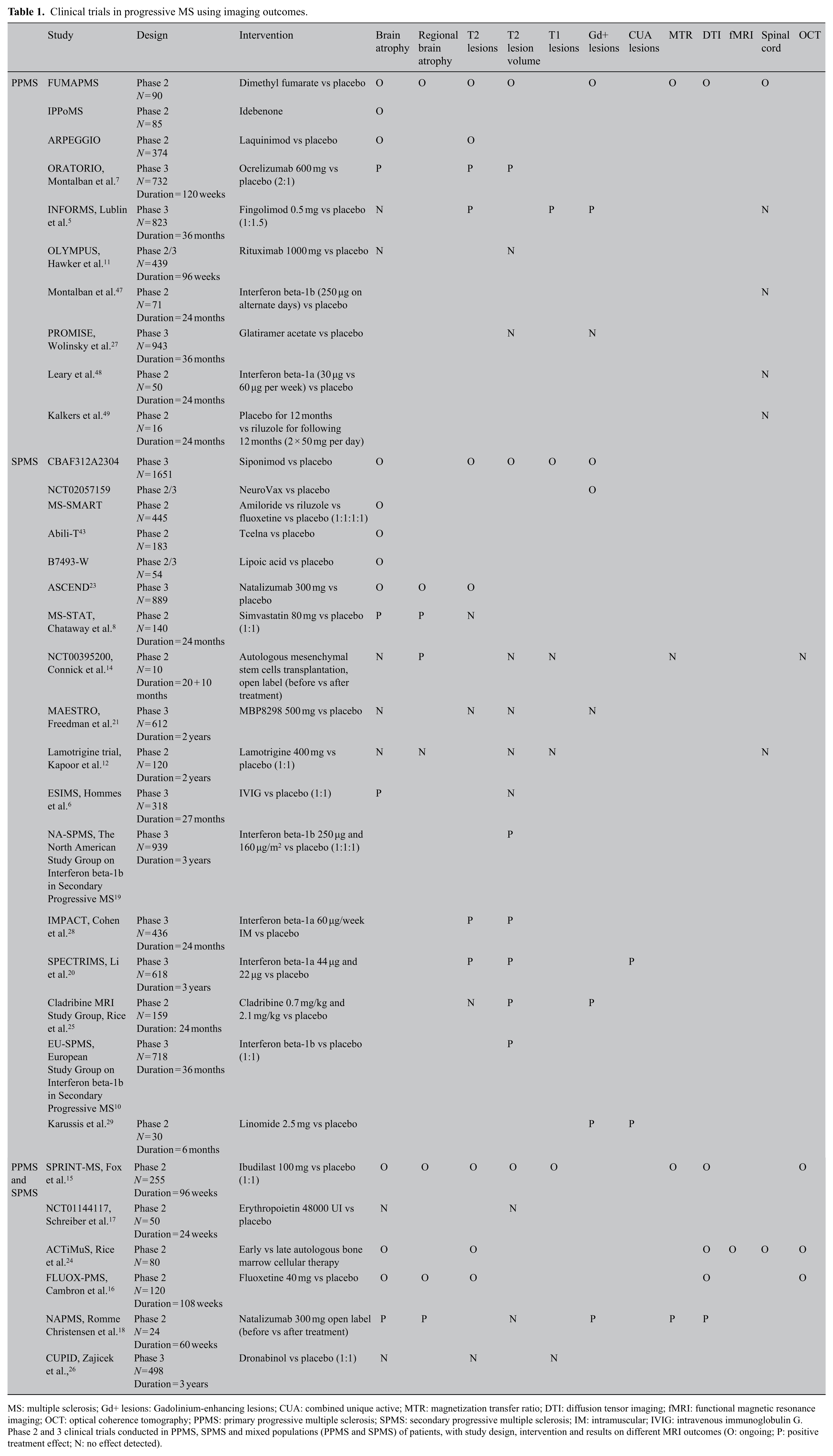
MS: multiple sclerosis; Gd+ lesions: Gadolinium-enhancing lesions; CUA: combined unique active; MTR: magnetization transfer ratio; DTI: diffusion tensor imaging; fMRI: functional magnetic resonance imaging; OCT: optical coherence tomography; PPMS: primary progressive multiple sclerosis; SPMS: secondary progressive multiple sclerosis; IM: intramuscular; IVIG: intravenous immunoglobulin G.
Phase 2 and 3 clinical trials conducted in PPMS, SPMS and mixed populations (PPMS and SPMS) of patients, with study design, intervention and results on different MRI outcomes (O: ongoing; P: positive treatment effect; N: no effect detected).
The first trial demonstrating a beneficial effect on global brain atrophy (using simvastatin) was a phase 2 trial study in SPMS. 8 Positive results have been reported also in the phase 3 ORATORIO study in PPMS. 7 A number of ongoing trials are measuring global brain atrophy, and their results should become available over the next several years (Table 2).
Phase 3 clinical trials in progressive MS evaluating brain atrophy.
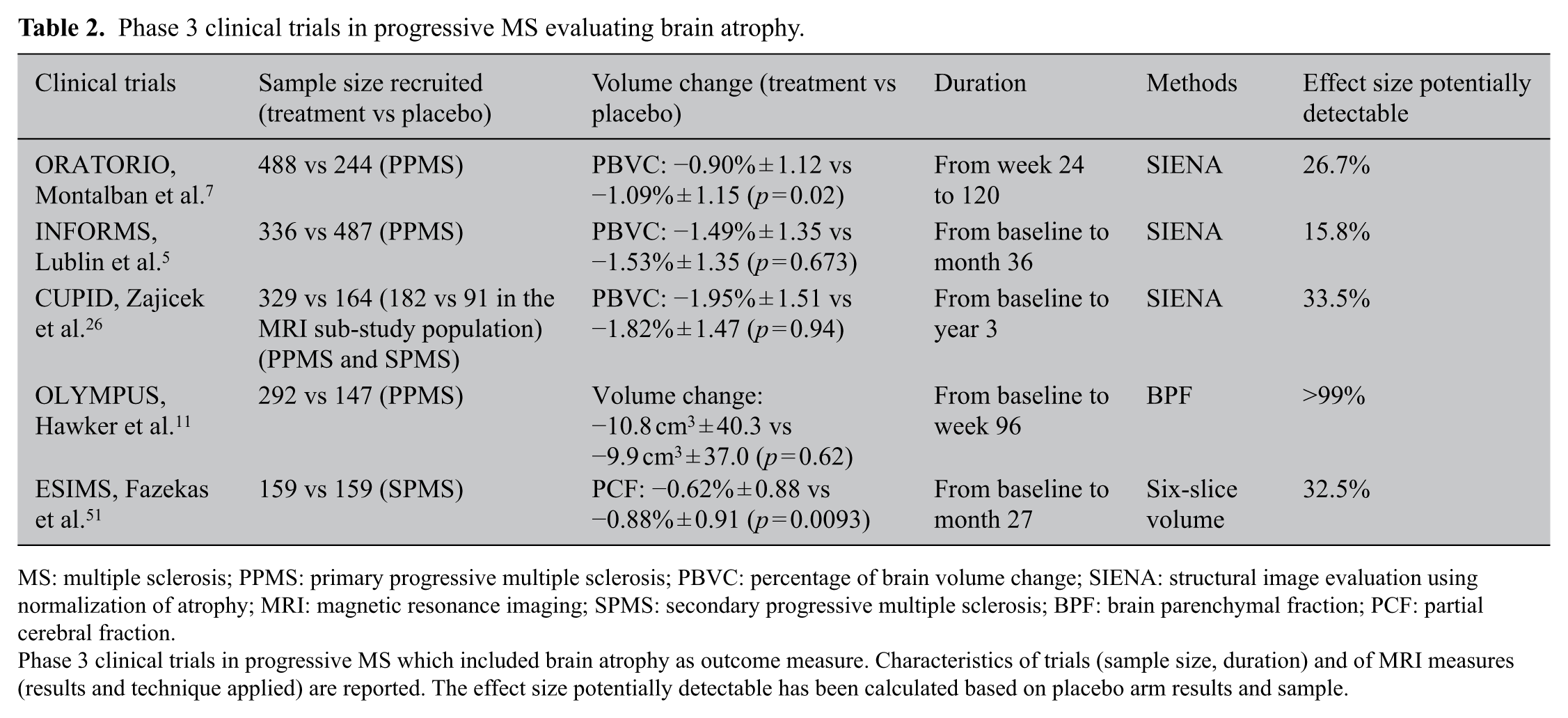
MS: multiple sclerosis; PPMS: primary progressive multiple sclerosis; PBVC: percentage of brain volume change; SIENA: structural image evaluation using normalization of atrophy; MRI: magnetic resonance imaging; SPMS: secondary progressive multiple sclerosis; BPF: brain parenchymal fraction; PCF: partial cerebral fraction.
Phase 3 clinical trials in progressive MS which included brain atrophy as outcome measure. Characteristics of trials (sample size, duration) and of MRI measures (results and technique applied) are reported. The effect size potentially detectable has been calculated based on placebo arm results and sample.
Regional brain atrophy has been used as secondary outcome in a few trials, where measures were obtained from GM, WM, 12 putamen, thalamus and optic nerve. 14 Considering that MS does not affect the brain uniformly, the detection of regional pathology might be predictive of more specific clinical features, when compared with whole-brain measures. 53 However, standardization of software for analysis is needed to make widespread application in clinical trials possible. 54
Overall, measures of global and regional brain atrophy are gaining relevance in clinical trials on progressive MS, reflective of improvements in measurement techniques allowing good reproducibility and sensitivity to change. Nevertheless, there are several possible limitations, including changes in magnet, gradients, coils, distortion corrections and image-contrast changes. Patients treated with anti-inflammatory treatments have a slight decrease in the brain volume in the first 6–12 months (pseudoatrophy), compared with placebo, due to the resolution of inflammation and oedema.55,56 A possible solution is to re-baseline subjects after 6 months,57,58 although longer periods may be required for more toxic types of treatment (e.g. chemotherapy during bone marrow transplantation). 59 However, rebaselining carries the risk of losing power because of reduced time of observation on treatment. In the OPERA II trial (one of the two phase 3 trials for ocrelizumab in RRMS), statistical significance in brain volume change was lost when analysing data from week 24 to 96, instead of baseline to week 96. 60
A reversible fluctuation of brain volumes can also occur because of variations in dehydration status. 61
Advanced MRI techniques
Conventional neuroimaging techniques lack specificity with regard to different pathophysiological substrates of MS and are not able to explain the heterogeneous and long-term clinical evolution of the disease.58,62–64 Advanced MRI techniques, such as magnetization transfer ratio (MTR), diffusion tensor imaging (DTI) and magnetic resonance spectroscopy (MRS), may provide higher pathological specificity for the more destructive aspects of the disease (i.e. demyelination and neuroaxonal loss) and be more closely associated with clinical correlates.55,65 Moreover, functional magnetic resonance imaging (fMRI) is contributing to the definition of the role of cortical reorganization after MS tissue damage. 37
MTR values reflect the efficiency of the magnetization exchange between mobile protons in tissue water and those bound to the macromolecules, such as myelin. MTR has been associated with disease progression in PPMS.35,66 In view of this, MTR has been included in several clinical trials in progressive MS and has been measured in GM, WM, T2 lesions, putamen, thalamus and optic nerve.13–15,18
DTI measures brain tissue microstructure by the exploitation of the properties of water diffusion. From the tensor, it is possible to calculate the magnitude of diffusion, reflected by mean diffusivity (MD), and diffusion anisotropy, which is a measure of tissue organization, generally expressed as fractional anisotropy (FA). In line with this, MD is increased and FA is decreased in T2 lesions, WM and GM from MS patients.67,68 DTI has been assessed across multiple scanners/platforms and is suitable for multi-centre studies.69,70 DTI is the most frequently used advanced MRI metric in phase 2 and 3 clinical trials in progressive MS, and is able to detect significant variations in brain microstructure during typical trial duration. 18 MD and FA have been measured in pyramidal tracts, WM, GM and lesions in different trials in progressive MS.13,15,16,18,24 More specific measures such as axial and radial diffusivity can be calculated as measures of the mobility of water along and perpendicular to axons (reflecting axonal density and demyelination, respectively); 65 however, they have not been included in clinical trials in progressive MS so far.
fMRI provides signal related to brain activation based on blood oxygen consumption and blood flow in the brain and has only been included in a single clinical trial on progressive MS. 24
MRS can measure brain levels of several metabolites.71,72 The most commonly measured is total N-acetyl-asparate (NAA), a marker of axonal loss and metabolic dysfunction. 73 NAA has been included in a few clinical trials in RRMS 74 and one in PPMS. 75
Spinal cord atrophy
SC atrophy is a common and clinically relevant aspect of progressive MS. A reduction in the cross-sectional area (CSA) of the SC over time is thought to reflect the development of atrophy (i.e. demyelination and neuronal/axonal loss).76,77
In clinically definite MS, the rate of cord atrophy has been reported to vary between 1% and 5% per year.77–81 Higher rates were found in progressive patients.77,82 Development of cord atrophy is considered to be one of the main substrates of disability accumulation. It can account for 77% of disability progression after 5 years.83–85
A few clinical trials in progressive MS have included SC atrophy as outcome measure (Table 1).12,13,24,31,47–49 Its more widespread use has been hampered by challenges to obtain high reproducibility and responsiveness to changes when measuring such a small structure. Small absolute changes in SC area are difficult to detect in a multi-centre setting, where there may be a great variability of imaging protocols and scanners. 40 The acquisition of high-quality SC MRI can be affected by artefacts (e.g. breathing, pulsation of blood and cerebrospinal fluid (CSF)), and this may limit the precision of SC atrophy measurements. As a consequence, sample size estimates obtained for current measurement techniques are fairly large and generally prohibitive, when compared with brain atrophy. Development of registration-based techniques to measure SC atrophy may address this concern as will be discussed below. 86
Position emission tomography
Position emission tomography (PET) is a quantitative imaging technique, which investigates cellular and molecular processes in vivo using positron-emitting molecules, ideally binding a selective target.72,87,88 As MS is a complex and multifactorial disease, various radioligands have been tested. Amyloid tracers, measuring myelin loss and repair, and 11 C-flumazenil, reflecting neuronal integrity, might be of interest for clinical trials on neuroprotective compounds.63,88–91
To date, no large MS clinical trials have included PET, reflecting its invasive nature and high costs. In the future, the development of standardized and less-expensive procedures might represent a trigger for the application of this technique in small phase 1 and 2a clinical trials. 6
OCT
OCT is a non-invasive method to obtain high spatial resolution images of the retina, measuring retinal nerve fibre layer (RNFL) thickness and macular volume.
RNFL is thinner in patients with MS than in healthy controls, even in patients with MS who have not experienced episodes of optic neuritis. 92 Therefore, OCT measures a more diffuse pathological process which better corresponds to overall central nervous system damage.93,94
RNFL and macular volume have been included in a few clinical trials on progressive MS (Table 1),14–16,24 so far without demonstrable neuroprotective effects.
OCT is a fast, non-invasive, easy-to-use imaging method producing quantitative measures reliably, with great potential in MS for testing neuroprotective strategies over a short time frame. 33 Like brain volume, RNFL is sensitive to biological variations. However, there is the need for high-quality acquisitions and appropriate image processing, performed by trained examiners following specific consensus criteria.
Design issues
Measurement sensitivity
Quantitative MRI measures are strongly dependent not only on acquisition parameters but also on processing methods, presenting with different sensitivity to change, reproducibility and measurement error.
Clinical trials results can be affected by the analysis. 41 For instance, in a clinical trial of teriflunomide in RRMS, changes were measured by BPF, a segmentation-based technique, and no significant effect was found initially. 95 However, in a post hoc analysis, the use of a registration-based automated technique (SIENA) revealed that teriflunomide was associated with significant reductions in brain volume loss. 96
Similarly, the conventional way of estimating SC atrophy is using segmentation-based methods, such as the cervical cord CSA97,98 and the upper cervical cord area (UCCA), 99 that are measured at each time point with subsequent calculation of percentage change between time points. More recently, GBSI (generalized boundary shift integral) has been suggested as a novel registration-based method to estimate cervical SC atrophy directly between scans, possibly reducing sample sizes. 86
The number of observations over time can increase sensitivity to change. However, at least for brain atrophy, the effect of increasing the number of observations is modest, when compared with the effect of increasing the duration of follow-up. 100
Sample size
Sample size calculation is a pivotal aspect of planning clinical trials and is based on the primary outcome of the study, generally being imaging for phase 2 and clinical for phase 3 trials.101,102 Imaging outcome measures are often included as secondary or exploratory variables in all patients in phase 3 clinical trials, even though they might require a smaller sample size to detect significant difference. A caveat though is that the size of the treatment effect may differ between clinical and imaging outcomes; that is, 30% reduction in rate of brain volume may not equate in 30% reduction in disability progression.
In order to further explore this issue, we estimated the treatment effect on brain atrophy which could have been detected in populations recruited in phase 3 clinical trials in progressive MS (Table 2), based on the actual sample size and the measured rates of brain atrophy in the placebo arm (we accepted a power of 80% and the α error was set at 0.05). Most recent studies would have been able to detect 15%–30% treatment effects on brain atrophy,5,7,26 in line with actual detected statistical effect (17.5% relative difference in the ORATORIO trial).
Inclusion criteria can also impact sample size. For instance, in RRMS populations, the rate of inflammatory activity is high, and measures of inflammatory activity (new or enlarging T2 lesions, new T1 lesions and Gd-enhancing lesions) can lead towards relatively lower sample sizes, compared with progressive MS.103,104 For instance, when considering the number of enhancing lesions, the detection of 50% treatment effect for interferon-beta treatment requires about 120 patients per arm in RRMS trials and a threefold number in SPMS. 105 By contrast, use of imaging markers more specific for progressive features (e.g. brain atrophy) will reduce the sample size needed in clinical trials in PPMS and SPMS. Advanced MRI techniques, such as MTR, might also require smaller sample sizes,106,107 in particular when trials with neuroprotective agents are conducted in selected populations.
Sample size can be affected also by variability of imaging outcomes. For instance, BPF measurement can have up to 0.00283% variance due to patient repositioning, physiological variations and inflammatory lesion occurrence. 108 Measurement precision can affect the standard deviation of the measure which is a major determinant of the sample size. 42 Increasing the number of scans performed in clinical trials and improving imaging analysis techniques (e.g. registration vs segmentation) can reduce these sources of variability and, accordingly, sample size.
Overall, DMTs can have a specific effect on each MRI outcome and thus the sample size should be estimated depending on the expected efficacy profile in the selected population. As such, MRI may be particularly useful in early-phase clinical studies on novel therapeutic agents, where drugs can be easily screened before they are taken forward to larger scale studies, 109 as is common practice for anti-inflammatory drugs in phase 2 RRMS studies.
Conclusion and future perspectives
Progressive MS represents a unique opportunity for studying imaging markers of neurodegeneration, with equal bearing on relapsing forms of the disease. Several imaging candidates hold promise for filling the unmet need of biomarkers in progressive MS, by capturing the effect on neurodegeneration, although inflammatory markers remain important in this stage of the disease. Brain volume loss is the best examined and most robust outcome with attainable sample sizes and first positive results, though treatment effects tend to be more modest than those seen for inflammatory MRI markers. Brain volume is already being applied as primary outcome measure in phase 2 trials and as secondary exploratory measure in phase 3 trials in progressive MS. Results from these trials will help establish the importance of brain atrophy in tracking MS progression. 46 SC MRI holds great promise for future trials due to higher rates of atrophy and better sensitivity to change compared with brain volume changes. However, robust application in clinical trials requires implementation of techniques with lower measurement noise, such as registration-based methods; in part, these can be validated using historical data sets. Advanced MRI measures (such as MTR, DTI and fMRI), due to their greater specificity, might shed light on mechanisms of action of new medications and should be included when clinical trials aim at exploring drug potentials for neuroprotection and tissue repair. In clinical trial design, the inclusion/exclusion of patients with specific MRI characteristics might help in identifying groups who are more likely to respond to a given medication and, so, in further reducing the sample size needed.
Footnotes
Acknowledgements
The authors are grateful to Professors Olga Ciccarelli, Robert J Fox, Alex Rovira and Bruno Stankoff for sharing their slides presented at the ECTRIMS Focused Workshop ‘Advancing Trial Design in Progressive Multiple Sclerosis’, for the preparation of the present manuscript. This review is part of a special issue derived from the 5th Focused ECTRIMS Workshop, ‘Advancing Trial Design in Progressive Multiple Sclerosis’, held in Rome, Italy, on 9–10 March 2017. The authors acknowledge the contributions of workshop attendees. F.B. is supported by the NIHR Biomedical Research Centre at UCLH.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.