
Abstract
Previous studies have demonstrated that the chimeric monoclonal antibody rituximab significantly reduces clinical and radiological disease activity in relapsing-remitting multiple sclerosis as early as 4 weeks after the first administration. The exact mechanisms leading to this rapid effect have not yet been clarified. The aim of this positron emission tomography study was to assess central nervous system penetration as a possible explanation, using zirconium-89-labelled rituximab. No evidence was found for cerebral penetration of [89Zr]rituximab.
Keywords
Introduction
Previous studies have suggested that rituximab, a chimeric monoclonal antibody (mAb) against the CD20 antigen on mature B-lymphocytes, significantly reduces the number of active inflammatory lesions and clinical relapses in multiple sclerosis (MS) patients. 1 Remarkably, this effect can be seen as early as 4 weeks after the first dose. 1 The exact mechanism underlying this rapid reduction of disease activity is not fully understood. Penetration into the central nervous system (CNS) could be an explanation for the fast effect of rituximab on disease activity. It is not clear, however, whether rituximab actually is able to enter the brain given its high molecular weight of 150 kDa. As such, brain penetration can only be expected in MS lesions, where the blood–brain barrier is disrupted. The purpose of this pilot study was to assess whether zirconium-89-labelled rituximab is able to detect these active CD20-positive lesions in patients with active relapsing-remitting multiple sclerosis (RRMS).
Methods
89Zr (half-life 78.4 hours) was produced and labelled to rituximab according to the procedures described by Verel et al. 2 and quality tests were performed according to the procedures described by Muylle et al. 3
Patients diagnosed with RRMS according to the McDonald criteria, with both a maximum Expanded Disability Status Scale (EDSS) of 5.0 and documented disease activity, were included. Active disease was classified as ⩾1 MS attack in the year prior to screening, with objective neurological signs confirmed by a physician, and a magnetic resonance imaging (MRI) scan within 3 months prior to screening demonstrating ⩾2 gadolinium-enhancing lesions of at least 3 mm in any axis. A baseline brain MRI (Siemens Sonata 1.5T) was performed within 7 days prior to administration of rituximab. Patients received a standard therapeutic dose of 1000 mg intravenous rituximab on study days 1 and 15. Only the first dose contained 10 mg rituximab labelled with 37 MBq 89Zr, which was injected within 2 hours after the unlabelled rituximab. Positron emission tomography (PET) scans (Philips Gemini TF PET/CT) were acquired on days 1, 3 and 6 after injection. Prior to each scan, venous blood samples were taken to analyse whole blood [89Zr]rituximab concentrations, and lymphocyte count and phenotype.
Regions of interest (ROIs) were drawn manually on MS lesions, normal-appearing white matter (NAWM), normal-appearing grey matter (NAGM) and the cerebral spinal fluid (CSF) in the lateral ventricles. These ROIs were defined on T2-weighted fluid-attenuated inversion recovery (FLAIR) MRI images, which had been co-registered with the PET data. Radioactivity concentrations in all ROIs were derived for each time point.
The study was approved by the Medical Ethics Review Committee of the VU University Medical Center, and all subjects gave informed consent in writing.
Results
In this pilot study, three clinically and radiologically active RRMS patients were included with two completing the entire study protocol. No significant adverse events occurred upon administration of [89Zr]rituximab.
In all three patients, a profound peripheral B-cell depletion was observed during the first days after injection.
At all three time points, radioactivity levels in the MS lesions were equal to those in comparable areas of NAWM (Figure 1). Tissue concentrations in lesions and NAWM were 1.8%–2.6% of the activity measured in the venous blood samples. For NAGM, this was 3.7%–5.4% (Supplemental Table 1).
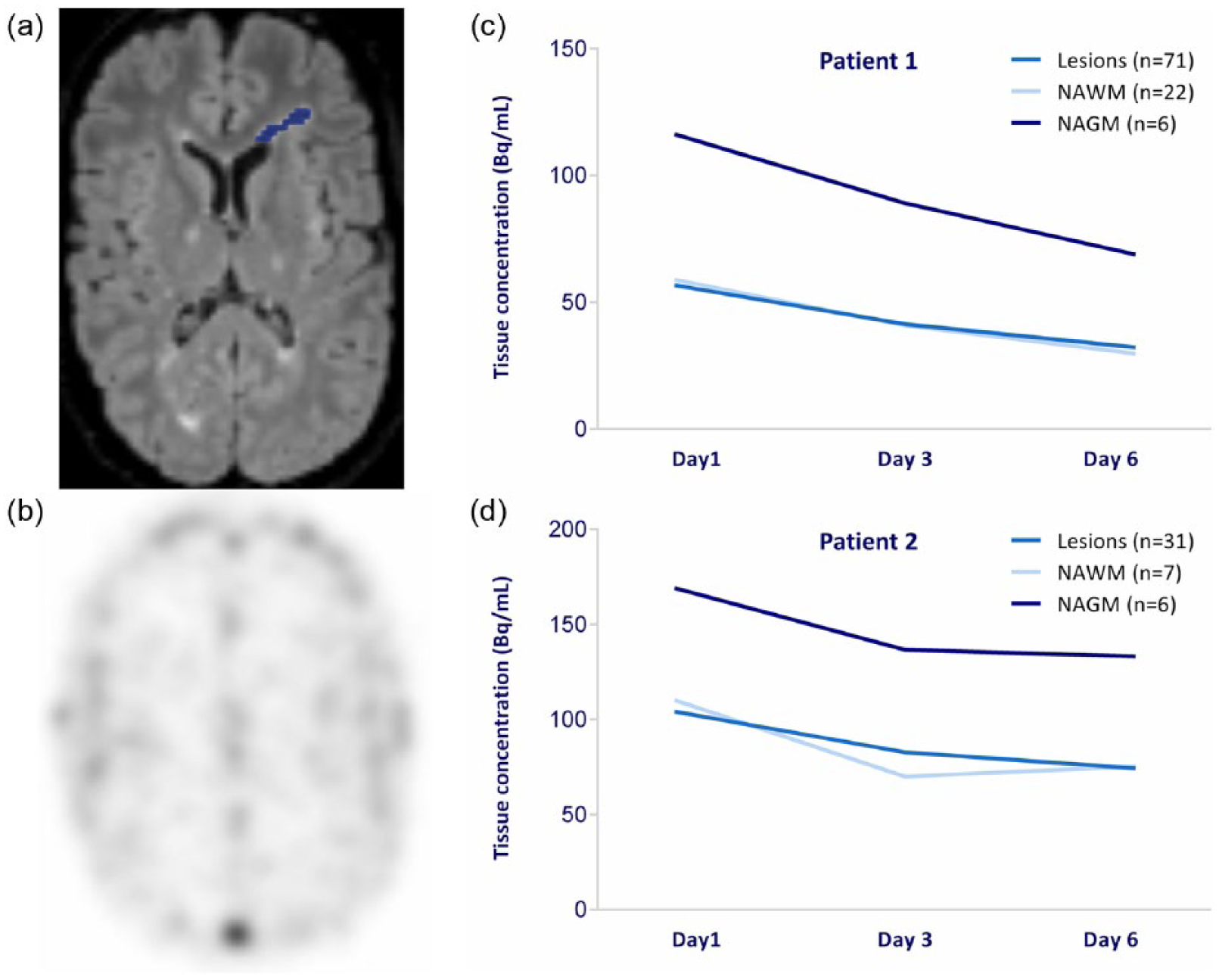
Radioactivity measured in the different regions of interest. (a) MRI scan of patient 1 with one region of interest marked in blue and (b) corresponding [89Zr]rituximab PET scan on day 6. (c, d) Mean decay corrected tissue concentrations measured on day 1, 3 and 6 in T2 MS lesions, normal-appearing white matter (NAWM) and normal-appearing grey matter (NAGM) for both patients.
Discussion
This pilot study demonstrates that PET imaging of radiolabelled mAbs can be used to obtain insights into the mechanisms of action of mAbs currently in use or in development for the treatment of MS.
Tissue concentrations measured in lesions and NAWM were very similar and corresponded to an estimated average blood volume fraction for white matter of 2.7% ± 0.6%. 4 Tissue concentrations in NAGM also corresponded with estimated average blood volume fractions for grey matter of 5.2% ± 1.4%. 4 This suggests that the measured signals were primarily, if not completely, due to intravascular activity. As such, no evidence was found for cerebral penetration of [89Zr]rituximab.
Additionally, we estimated the radioactivity in the CSF in the lateral ventricles, which was similar to the NAWM at all three time points (Supplemental Table 1). The signal seems to be non-specific and not highly reliable due to inaccurate scatter correction at the location.
It should be noted that [89Zr]rituximab was administered after a therapeutic dose of unlabelled rituximab in order to block peripheral binding sites with the cold rituximab. Therefore, at least in theory, it is possible that lack of [89Zr]rituximab uptake was due to saturation of binding sites in the brain by unlabelled rituximab. However, as measured concentrations could be explained entirely by the signal expected from intravascular activity at all three time points, there is no evidence for any free [89Zr]rituximab in the brain parenchyma at those time points.
Furthermore, while this study shows no CNS penetration of zirconium-89-labelled rituximab at the level of PET, we cannot exclude that rituximab itself can enter the brain parenchyma at very low penetrance, which could still have immunological effects.
Further studies are needed to confirm that CNS penetration of rituximab is indeed negligible.
The peripheral and intrathecal effects of this anti-CD20 mAb on complement-mediated B-cell lysis, B-cell antigen presentation, and cytokine and chemokine production in MS have been documented extensively. 5 Moreover, a recent study suggested that CD20-expressing T cells could also play a role in the therapeutic effects of rituximab. 6 Nevertheless, early therapeutic effects of rituximab in MS are not fully explained by currently known B and T cell pathology. Further insights remain highly relevant in the light of recently reported positive results of the phase III ocrelizumab trials in MS. 7
Footnotes
Acknowledgements
This research has been executed within the VUmc MS Center, Amsterdam. Roche kindly donated rituximab for this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: M.H.J.H. reports no disclosures. J.K. has accepted speaker and consulting fees from Merck Serono, Biogen, Teva, Genzyme, Roche and Novartis. M.M.Y. reports no disclosures. G.A.M.S.v.D. reports no disclosures. A.A.L. reports no disclosures. F.B. serves as a consultant for Bayer Schering Pharma, Sanofi-Aventis, Genzyme, Biogen-Idec, Teva, Novartis, Roche, Synthon BV and Jansen Research. B.N.M.v.B. reports no disclosures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: VUmc MS Center Amsterdam has received financial support for research activities from Bayer Schering Pharma, Biogen, Roche, GlaxoSmithKline, Merck Serono, Novartis and Teva.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.