
Abstract
Cognitive and motor performance measures are commonly employed in multiple sclerosis (MS) research, particularly when the purpose is to determine the efficacy of treatment. The increasing focus of new therapies on slowing progression or reversing neurological disability makes the utilization of sensitive, reproducible, and valid measures essential. Processing speed is a basic elemental cognitive function that likely influences downstream processes such as memory. The Multiple Sclerosis Outcome Assessments Consortium (MSOAC) includes representatives from advocacy organizations, Food and Drug Administration (FDA), European Medicines Agency (EMA), National Institute of Neurological Disorders and Stroke (NINDS), academic institutions, and industry partners along with persons living with MS. Among the MSOAC goals is acceptance and qualification by regulators of performance outcomes that are highly reliable and valid, practical, cost-effective, and meaningful to persons with MS. A critical step for these neuroperformance metrics is elucidation of clinically relevant benchmarks, well-defined degrees of disability, and gradients of change that are deemed clinically meaningful. This topical review provides an overview of research on one particular cognitive measure, the Symbol Digit Modalities Test (SDMT), recognized as being particularly sensitive to slowed processing of information that is commonly seen in MS. The research in MS clearly supports the reliability and validity of this test and recently has supported a responder definition of SDMT change approximating 4 points or 10% in magnitude.
Keywords
Overview and historical perspective
Slowed cognitive processing was identified as a core symptom of multiple sclerosis (MS) in 1877 by Charcot 1 who presciently observed that in many patients, “conceptions are formed slowly and the intellectual and emotional faculties are blunted in their totality.” It would take a century for psychometric methods to be rigorously applied to this population, confirming Charcot’s hypothesis that bradyphrenia is a core MS deficit. Beginning with the work of Stephen Rao in the 1980s,2–4 cognitive processing speed (CPS) was formally quantified using primarily two neuropsychological tests, the Paced Auditory Serial Addition Test (PASAT) 5 and the Symbol Digit Modalities Test (SDMT). 6 When other, more complicated, timed executive function tests were applied to MS samples, more often than not the processing speed component accounted for the test’s sensitivity.7–8 Subsequently, due to its ease of administration and other factors (e.g. reliability and validity, predictive validity, sensitivity, and specificity), the SDMT has risen to the forefront of neuropsychological evaluation in MS. Over the last 5 years, it has become the most commonly used neuropsychological test of processing speed in MS. 10
While the SDMT was first published as a commercially available test in 1982, 6 the idea of measuring information processing speed and efficiency using a symbol/digit substitution task dates to the early 20th century. In 1913, a symbol digit substitution task was described in a manual of psychometric scales for the examination of school children (Figure 1(a)). 11 Writing in 1927, Lemmon 12 credited both Guy Montrose Whipple 13 and William Henry Pyle 11 for developing this procedure. By then, the task had been adopted by the United States Army in their efforts to screen incoming recruits for mental deficiency (Figure 1(b)). 14 However, the stimulus/response pairing had shifted from the reporting of numbers associated with the correct symbol to that of writing symbols in accordance with the target numbers. This form would evolve into the digit symbol coding (aka digit symbol substitution test) test co-opted by the Wechsler adult and children intelligence tests, in the 1930s 15 and 1940s. 16 The Coding Test Version, wherein the participant writes symbols corresponding to the target key at the top of the page, is a core test of processing speed in current versions of the Wechsler intelligence scales. It seems that the original number response method lay quiescent for decades until the 1960s when Smith and colleagues began to pilot their SDMT method in studies of cognitive aging and neuropsychology.17–19
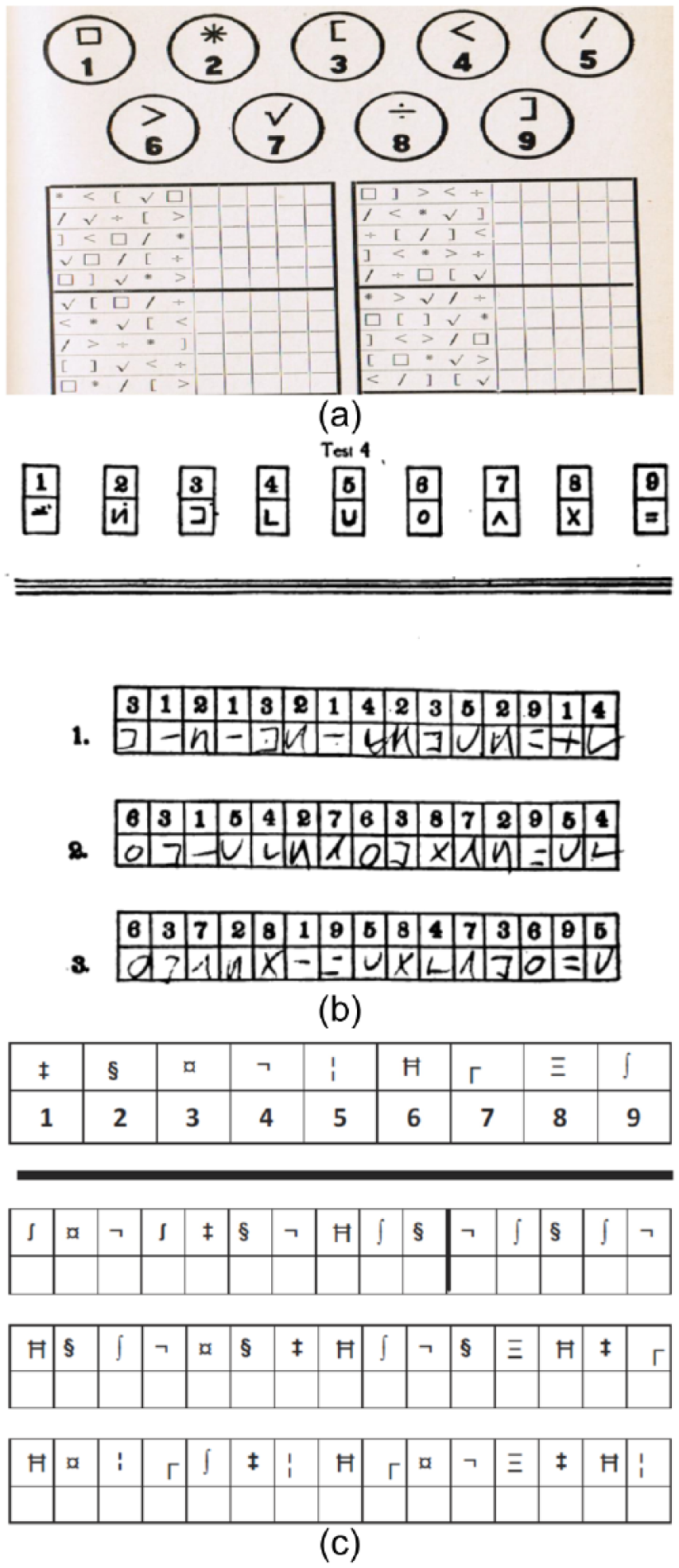
(a) The Symbol Digit Modalities Test as originally developed by Whipple 13 and Pyle 11 in the early 20th century. This is the earliest description of a symbol/number coding task we are able to locate, and neither source refers to a prior version of the task. (b) A scored version of the Digit Symbol Substitution Test as developed for the US Army in the early 1920s, subsequently adapted by the Wechsler intelligence scales. (c) A faux version of the Symbol Digit Modalities Test (SDMT) as presented in an earlier publication on the Brief International Cognitive Assessment for MS (BICAMS).
The SDMT is presently owned by Western Psychological Services and to protect the copyright and conform with ethical principles, we present a faux rendering 20 of the test in Figure 1(c). The subject is presented with a page headed by a key that pairs the single digits 1–9 with nine symbols. Rows below contain only symbols, the subject’s task is to write or orally report the correct number in the spaces below. After completing the first 10 items with guidance, the subject is timed to determine how many responses can be made in 90 seconds. In the standard administration of the SDMT, the written response task is conducted first, followed by an oral response task, using the same stimuli. However, the vast majority of MS studies skip the written response administration and only utilize the oral version, to diminish the sensory motor impact of using the written version. Thus, the examiner uses a scorer form on which he or she records the subject’s voiced responses. The correct answers appear on the examiner’s form making scoring quick, with minimal chance for error. In total, the test requires no more than 5 minutes to complete.
Recognizing the importance of the processing speed domain for MS research, Rao and colleagues included both the PASAT and SDMT in the Brief Repeatable Battery of Neuropsychological Tests (BRB), 21 and for the past 25 years, the vast majority of studies have utilized either or both of these measures. Both tests are included in the Minimal Assessment of Cognitive Function in MS (MACFIMS), 22 a consensus opinion battery developed in 2002. The PASAT gained considerable favor after its inclusion in the Multiple Sclerosis Functional Composite (MSFC).23,24 However, in the early 2000s, we and others began to take note of what seemed to be superior reliability and sensitivity of the SDMT as well as greater patient acceptance, suggesting that it may be a superior test due to better psychometric validity and ease of administration. Consequently, as shown in Table 1, the SDMT is the single test common to all recommended cognitive batteries for MS patients, including the BRB, MACFIMS, NINDS Common Data Elements, 25 MS-Cog, 26 and the Brief International Cognitive Assessment for MS (BICAMS).27,28
Review objective
The SDMT was selected for this review due to its prominent role in discussions emanating from the Multiple Sclerosis Outcome Assessments Consortium (MSOAC). This effort to adopt a clinical outcome assessment tool for clinical trials to better capture MS-related disability was born out of a consensus paper by the International Advisory Committee on Clinical Trials in Multiple Sclerosis. 29 The MSOAC includes representatives from the National MS Society as well as 6 other MS advocacy organizations, Food and Drug Administration (FDA), European Medicines Agency (EMA), National Institute of Neurological Disorders and Stroke (NINDS), 21 academic institutions, and 9 industry partners, along with persons living with MS. The goals of the consortium are acceptance and qualification by regulators of performance outcomes that reflect core MS impairments that are highly reliable and valid, practical, cost-effective, and meaningful to persons with MS. This review benefitted from a formal MSOAC sponsored literature search, conducted in Embase, Medline, PsycINFO, and Cumulative Index of Nursing and Allied Health Literature, followed by an enrichment technique (key papers identified by MSOAC members added and informed search criteria) including work identified from prior reviews. Like the companion reviews in this issue of the Timed 25-Foot Walk, Nine-Hole Peg Test, and Low-Contrast Letter Acuity, this article begins with psychometric characteristics and concludes with an appraisal of the clinical meaningfulness of the measure.
Psychometric validity
Reliability
The SDMT manual reports that in a healthy sample, the test–retest reliability coefficient is 0.76 for the oral response version. The r was considerably higher, 0.97, in a sample of 34 MS patients tested over 2 weeks. 30 Satisfactory reliability was maintained at 1-month 31 and 2-year intervals (an epoch that encompasses both reliability and maturation effects). 32 Through the BICAMS27,28 initiative, the reliability of SDMT remains good to excellent at short intervals following translation of the test instructions into Persian (0.79), 33 Portuguese (0.86), 34 and Spanish (0.95). 35
Alternate forms were developed by a National MS Society Cognitive Function Study Group, 21 but subsequently, these forms were found to be non-equivalent. 36 For these alternate forms, the same symbols were employed, but the alternative forms used different symbol–digit pairings. On the standard SDMT, however, the first 26 items utilize only the first six symbols in the key, a subtlety apparently missed when alternate forms were first developed. Accommodating this idiosyncrasy while generating new forms resulted in alternate versions that yield data nearly identical with the standard form, 37 while maintaining good test–retest reliability in healthy controls (HCs) with r varying from 0.84 to 0.90. Drake et al. 32 reported that the test–retest reliability of the SDMT in 115 MS patients over 2 years is r = 0.74.
Construct and predictive validity
The construct validity of SDMT was investigated in 278 MS patients. 38 The MACFIMS was administered in total. SDMT loaded on a general processing factor in the relapsing–remitting multiple sclerosis (RRMS) analysis and showed a split loading in the secondary-progressive multiple sclerosis (SPMS) group, loading on a speed/executive function factor and a memory factor. This latter observation is important. The SDMT was originally developed11–13 as a learning and processing efficiency test, under the assumption that as the test proceeds, individuals will tend to learn the symbol/digit associations. Subsequent research showed that symbol search coding tests in general load on a processing speed factor.15,39 Nevertheless, there is likely some degree of learning involved, and this multimodal aspect of the SDMT may account for its very high sensitivity to cognitive impairment. Within a brief battery of cognitive tests, the SDMT was found to be the test that best predicted future cognitive decline. 40
Discriminative validity
An oft-repeated observation is that the SDMT frequently discriminates MS and control groups as well as, if not better than, other neuropsychological tests.32,38,41–49 In a study using an extended battery of tests, 41 SDMT loaded first in regression models discriminating MS patients and HCs. 38 While all MACFIMS tests significantly discriminated these groups, the effect size was largest for SDMT (d = 1.3). In Figure 2, the mean effect size d and the range of smallest to largest effects sizes are depicted. The analysis is derived from 15 studies26,33,38,41,44,46,50–57 that compared MS patients and HCs and included the SDMT, PASAT, a consensus opinion memory test, and the Controlled Oral Word Association Test.
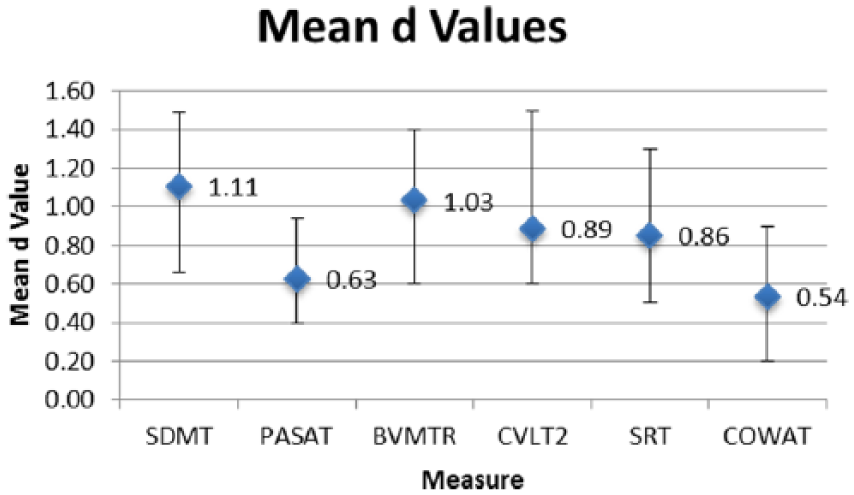
Mean effect sizes and ranges for each of the more commonly used neuropsychological tests in consensus standard batteries. Figure shows the mean effect size as calculated by the Cohen d method where d is the difference between group means divided by the average SD. All d values reflect MS and healthy control group comparisons. SDMT has a larger mean effect size as compared to others depicted.
Criterion validity, correlation with brain MRI
Neuropsychological testing is frequently employed as a clinical benchmark for interpreting the meaningfulness of MRI abnormalities. In MS, early work in the late 1980s showed that cognitive impairment is correlated with lesion burden and ventricle enlargement.58,59 The next decade witnessed the advent of many MRI metrics including spectroscopy, diffusion, whole brain atrophy, and gray versus white matter volume. Two early studies44,60 used linear regression with multiple MRI measures to determine the most robust predictor of cognitive impairment and in both studies MRI accounted for most variance in SDMT, the strongest predictor being central atrophy (r = 0.70 or 0.71), as measured by ventricle enlargement. Compared to other MACFIMS cognitive tests, SDMT accounted for more variance in gray matter volume, 61 whole brain diffusion abnormalities, 62 and lesion burden at both 1.5 and 3.0 T. 63 Consequently, SDMT has become a standard for measuring cognition in recent efforts to understand clinical correlations of regional gray matter atrophy, within-structure diffusivity, and connectivity.55,64–67 In a recent meta-analysis, the SDMT was found to have the strongest relationship with various MRI metrics among tests of processing speed. 68
Summary
The SDMT has proven to be quite useful in neuropsychological MS research. It has excellent test–retest reliability, and alternate forms have been developed that are equivalent in difficulty. When the alternate forms are used, reliability is maintained. Validity research shows that SDMT is a good measure of processing speed or efficiency. SDMT is the neuropsychological test most sensitive to MS cognitive disorder and correlates very well with MRI measures of atrophy, lesion burden, and microstructural pathology. The test very effectively represents the core neuropsychological domain of processing speed. Thus, it is no surprise that the SDMT is the only neuropsychological test included in all MS cognitive test batteries developed in recent years (Table 1).21,22,25,26,28
Neuropsychological tests used in common consensus standard assessment batteries, by cognitive domain.
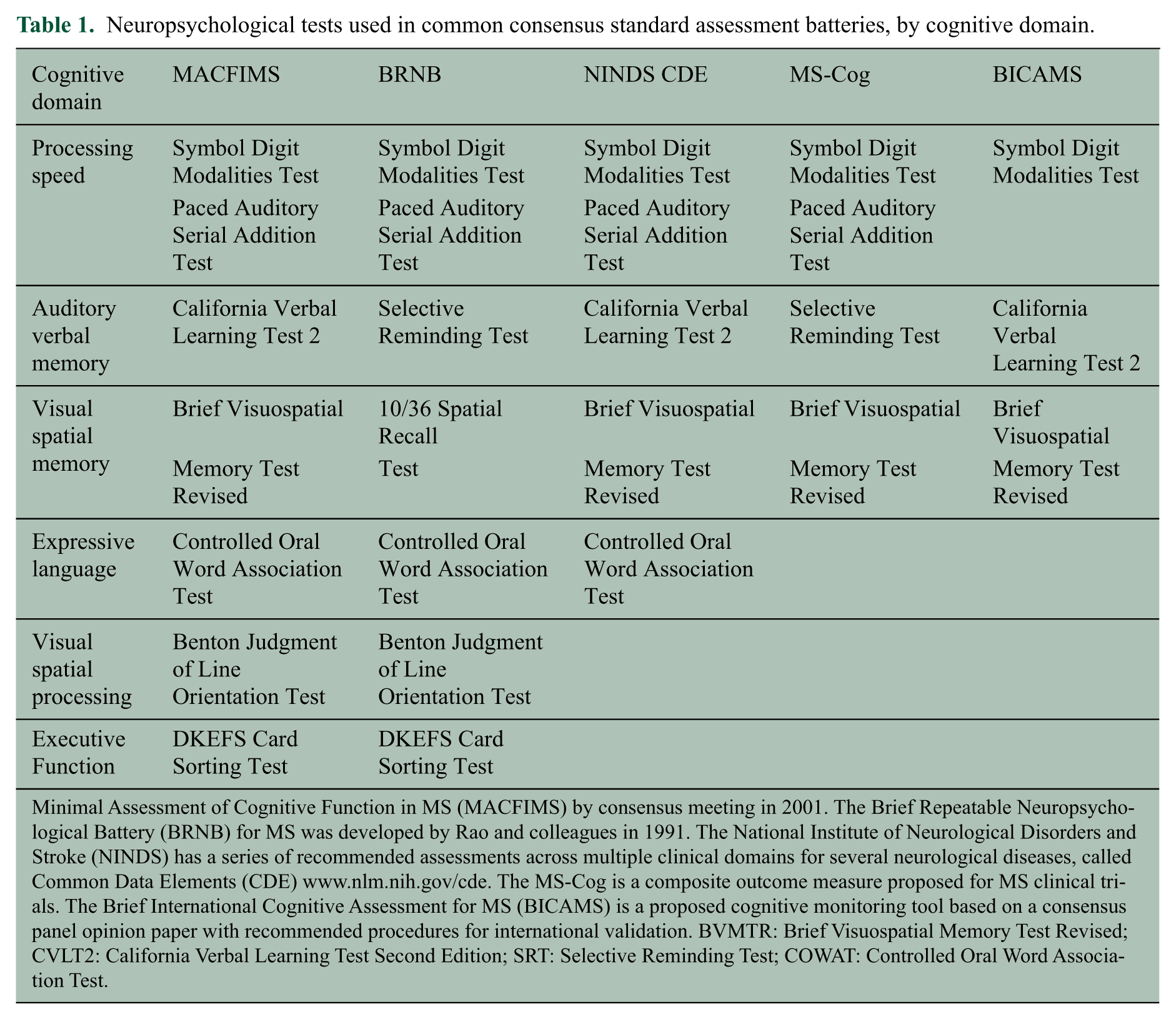
Minimal Assessment of Cognitive Function in MS (MACFIMS) by consensus meeting in 2001. The Brief Repeatable Neuropsychological Battery (BRNB) for MS was developed by Rao and colleagues in 1991. The National Institute of Neurological Disorders and Stroke (NINDS) has a series of recommended assessments across multiple clinical domains for several neurological diseases, called Common Data Elements (CDE) www.nlm.nih.gov/cde. The MS-Cog is a composite outcome measure proposed for MS clinical trials. The Brief International Cognitive Assessment for MS (BICAMS) is a proposed cognitive monitoring tool based on a consensus panel opinion paper with recommended procedures for international validation. BVMTR: Brief Visuospatial Memory Test Revised; CVLT2: California Verbal Learning Test Second Edition; SRT: Selective Reminding Test; COWAT: Controlled Oral Word Association Test.
Clinical relevance of the SDMT
How well does the SDMT reflect neurocognitive capacities that are related to activities of daily life important to patients? On the surface, the test may not seem to be very relevant. Unlike the T25FW, for example, patients are not asked to perform a task ordinarily undertaken in daily life. In fact, when a person takes the test for the first time, the chances are there that he or she has never seen anything like it before. One may have some appreciation for the observation that a person who used to walk 25 feet in 4 seconds and now requires 6 seconds to cover the same distance is affected or in some way meaningfully compromised. In contrast, there is little inherent meaning in a SDMT raw score change of 60 to 45. Why then should a relative deficit on the SDMT compared to a healthy person, or SDMT decline over time, be of concern to patients or clinicians?
Group studies
Slower performance on the SDMT is correlated, at the group level, with activities of daily living (ADLs) and employment status. Some research 69 suggests that cognition is the most important domain for employability, although a recent study found that the T25FW is just as closely linked to this particular limitation of daily functioning. 70
Strober et al. 71 assessed cognition and Expanded Disability Status Scale (EDSS) in 101 patients and defined employment as employed/volunteer, disabled, or retired. Disease duration, MS course, EDSS, and cognitive performance all distinguished the groups, and a regression analysis retained EDSS, SDMT, and the personality trait of persistence as the strongest predictors. In this, and a subsequent study carried out with an independent sample, 72 SDMT was the most robust neuropsychological predictor of employment from a comprehensive test battery. The effect size was large, on the order of d = 0.80–0.90. This effect size was recently replicated by an independent group in Australia. 73
SDMT is similarly related to other daily activities, even when measured in controlled or relatively standardized conditions. All of the cognitive outcomes in the BICAMS 28 battery were correlated with errors when patients were asked to use a desktop computer to access the Internet and purchase an airplane ticket or food. 74 The correlation between performance errors and SDMT was r = −0.48, slightly lower than with the Brief Visuospatial Memory Test—Revised (BVMT-R) 75 (r = −0.59). In a similar setting, MS patients were asked to prepare a dish from a standard recipe. 76 Across a comprehensive test battery, SDMT showed the largest, albeit modest, correlation with cooking efficiency (r = 0.29). Furthermore, the SDMT was the only neuropsychological test which predicted impaired money management in MS patients. 77
Benchmarks for clinically relevant levels of SDMT performance
Group studies showing significant positive correlations between SDMT and employment status and various ADLs support the test’s ecological validity. MS patients performing poorly on the SDMT are more likely to lose employment and struggle while carrying out ADLs. However, within-sample correlations do not determine when SDMT performance becomes relevant for a particular patient—we do not know how any specific score corresponds to a patient’s adaptive functioning.
Unfortunately, as is the case for neuropsychological performance in general, the correlation between SDMT and self-reported cognitive difficulty is poor.43,78–83 Largely subjective symptoms, such as depression, pain, and fatigue, tend to correlate with one another and with quality of life measures. In contrast, cognitive performance tests tend to correlate poorly with such symptoms but are robustly related to ADLs and employability. Therefore, it is within these functional domains that we must search for benchmarks to aid in the interpretation of SDMT scores.
Following the work of Goldman et al., 84 multiple employment-related anchors were recently captured to compare with SDMT performance. SDMT scores were obtained from MS adults who were fully employed and free of work problems, employed but work-challenged, or unemployed due to disease-related factors. 70 The analysis established benchmark SDMT scores associated with these varying levels of vocational disability. Of the tests under study, T25FW and SDMT were most discriminating of these groups, and the SDMT benchmarks (MS work disabled = 45, MS employed but work challenged = 55, MS employed and stable = 63) were offered to complement previously established, meaningful levels of slowed ambulation. 84
Clinically meaningful change
In an effort to correlate discrete changes in SDMT with functional status, Morrow et al. 85 examined a sample of persons with MS who were all employed full time 3.5 years earlier. Those persons who had declined in status over the interim were compared on the MACFIMS with those maintaining employment. SDMT maximally discriminated the groups. Depending on how work disability was defined, conservatively or liberally, SDMT raw score decline of 3 or 4 points maximally separated the employment status groups.
Another way of documenting clinically meaningful change is to consider how the test reflects a clearly discernible change in clinical condition apparent to the person with MS, caregiver, and/or a clinician observer. If the test declines during an acute neurologic episode, that is, a relapse, and then recovers, the degree of change that is observed could be construed as clinically meaningful.
The STRATA study 86 was a long-term observational safety study of natalizumab (Tysabri) for relapsing MS. STRATA provided a unique opportunity to study SDMT in a large cohort of patients undergoing monthly screenings (SDMT, Beck Depression Inventory Fast Screen for Medical Patients, 87 MS Neuropsychological Screening Questionnaire (MSNQ) 43 ) for progressive multifocal leukoencephalopathy (PML). The SDMT was reliable over the course of the investigation, showing an anticipated learning or treatment effect, as scores improved. While no PML was observed, the evaluation of patients undergoing relapse provided the opportunity to isolate the effects of such an overt clinical state on SDMT performance. This analysis 88 revealed that in comparison with the scores in non-relapsing patients where improvement was observed, those in relapse declined by roughly 2–3 points, followed by recovery to nearly the level of the control group.
MS relapses involve a range of sensory/motor deficits that could compromise SDMT performance. In a prospective study, 89 these factors were controlled in a comparison of 24 relapsing and 24 non-relapsing MS patients. All participants had a retrospective baseline evaluation and were examined again prospectively at the time of relapse, before steroid treatment, and again 3 months later. Importantly, all patients enrolled in the relapse group either reported or were suspected of cognitive impairment on the basis of clinician or observer impression. At relapse, the groups differed on SDMT by 5 points, and at 3 months, the difference had been reduced to roughly 3.
These SDMT findings suggest that it may be possible to identify MS patients experiencing cognitive changes as part of a relapse, independent of other factors. Pardini et al. 90 attempted to validate the concept by examining patients free of relapse, and having no clinical change by EDSS, but based on prior work 85 showing at least a 4-point decline on SDMT from baseline. Of 99 patients, 17 were so identified and labeled as having an “isolated cognitive relapse” with a stable EDSS. This group evidenced positive gadolinium enhancement on MRI concordant with the SDMT decline and showed only a partial recovery of function at 6 months and 1 year follow-up.
These findings have a bearing not only on the issue of benchmarks for clinically meaningful change but also on the MS disease activity in general. It has recently been shown that the frequency of “no evidence of disease activity” or NEDA is significantly reduced when cognitive function is monitored. 91 Were SDMT or similar tests employed on a routine basis, 92 transient deficits may explain, in part, some of the discrepancy between MRI disease activity and clinical activity, which is typically defined as positive findings on a traditional neurologic exam, which heavily emphasizes motor and sensory testing.
Summary
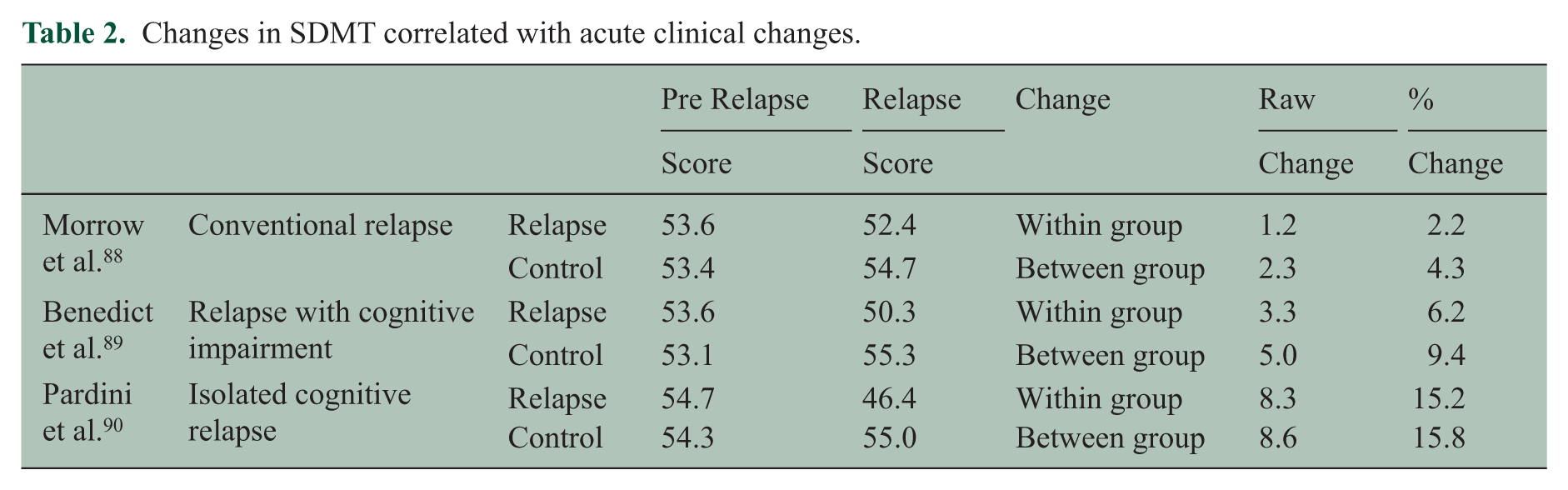
SDMT, a valid measure of cognitive processing speed (CPS), is robustly correlated with instrumental ADLs in MS patients. In studies including multiple cognitive or motor performance tests, it stands out as among the best or the single most robust predictor of employability and overall ADLs. One retrospective, longitudinal study comparing work-stable versus work-disabled patients showed that a 3- or 4-point decline over 42 months maximally separated the groups. There are now three controlled studies revealing changes in SDMT that are associated with functional decrements during relapses or acute disease activity, as a proxy for readily observable decline in clinical status (Table 2). The percentage of change relative to controls ranges from 4% to 16%. A general interpretation of the data suggests that a raw score change of 4 points, or a 10% change, is clinically meaningful.
Changes in SDMT correlated with acute clinical changes.
Conclusion and future directions
A century ago, psychologists in the United States developed a cognitive test requiring subjects to process symbol/digit associations as rapidly as possible, believing the task to be related to processing speed and efficiency. Work in MS dates to the early 1990s when Smith’s SDMT was incorporated in the Rao Brief Repeatable Neuropsychological Battery. In the early 2000s, researchers began to take note22,43,44,60 of the repeated observation that the SDMT is the most reliable and sensitive neuropsychological test, leading to the idea that it may serve as a screen for neuropsychological impairment. 42 In 2008, Brochet et al. 46 questioned whether the SDMT should replace the PASAT as the cognitive component of the MSFC, compelling Drake et al. to publish z score calculation tables for the SDMT versions of the MSFC.29,32,46 This work was paralleled by experimental neuropsychological research reinforcing the core contributions of processing speed in MS.93–95 The SDMT is now the leading cognitive test candidate for the more recent MSOAC effort to qualify performance scales for MS clinical trials with the FDA and EMA. 29
One should bear in mind that while the SDMT is a published psychometric test protected by copyright, the task, in general, comes in many administration formats and dates to the early 20th century. There are many similar tasks in the psychological and medical literature, and virtually any computer-based test found on the Internet includes a variant of the original digit/symbol substitution test. The MATRICS Consensus Cognitive Battery,96–98 endorsed by the FDA for labeling in cognitive impairment associated with schizophrenia, includes the Brief Assessment of Cognition in Schizophrenia (BACS) Symbol Coding Test. An adaptation of the SDMT has been used in professional sports concussion management for years.99,100 An iPad version of the MSFC 101 will likely include the Processing Speed Test, a digit symbol task wherein the participant presses a button corresponding to the correct number for each stimulus. It remains to be seen how important it is to use the same task across studies and if there are any differences in reliability, sensitivity, and validity across many versions of the test.
In our opinion, the SDMT is the best psychometric measure available for assessing CPS in MS patients. That said, the test is not without its problems and limitations. There are very little longitudinal data that would permit us to draw conclusions about how sensitive SDMT is to changes in cerebral function over time. Interestingly, even though decline in SDMT over 3 years was associated with morphological abnormalities in the thalamus; 102 as a group, MS patients were stable on the test compared to HCs.103,104 Most notably, the SDMT is not a pure test of processing speed. SDMT performance can be influenced by visual acuity and ocular motor functions,10,105 and while SDMT is correlated with other processing speed tests, there is undoubtedly some incidental learning of symbol–digit associations, and hence the need for alternate forms. 106 Although not likely the major contributor to measuring processing speed, these factors should be taken into account when interpreting SDMT performance.
Processing speed is a basic elemental cognitive function required by, and therefore influencing downstream processes such as learning, memory, word retrieval, and executive function. 10 In MS, processing speed has been shown to account for impairments in working memory, executive functions, and learning and memory.107–111 As such, higher cognitive processes in MS can be influenced by impaired processing speed and may be the primary reason that impaired performance on tests of higher cortical function may be compromised. This has significant implications as the choice of treatment may influence the effectiveness of the cognitive intervention. For example, MS patients with impaired learning and memory and a co-morbid deficit in processing speed may not benefit from memory retraining compared to those without impaired processing speed.
As noted in a prior topical review, 112 cognitive performance is not reliably correlated with patient self-reports of cognitive symptoms. Patient self-reports of cognitive functioning (cognition patient-reported outcomes (PROs)) are less related to actual cognitive performance than to other subjective symptoms such as depression and fatigue.81,113,114 While the linear relationship between SDMT and real-life activities within groups is well established, identifying definitive anchors has been challenging. This and the earlier review identify two potential anchors, unwanted job loss and employment problems, and mental status changes during relapses. In general, the available work suggests that a 10% change in SDMT is clinically relevant. Others have already proposed that a 4-point change is relevant, 90 which may also serve as a responder definition in clinical trials. 115
The relapse anchor is interesting from several perspectives. The notion of a cognitive relapse has been discussed in the literature116–118 but until recently mental status was not quantified and compared to baseline levels. In the available studies, SDMT was measured in three gradations: (a) all relapsing patients, ignoring mental status as is typically the case, 88 (b) patients meeting commonly accepted criteria for relapse but with some clinical evidence of mental status change, 89 and (c) relapse defined by actual change in cognition without other clinical evidence of acute disease activity but with radiological evidence of relapse. 90 As is evident in Table 2, changes in SDMT are uniformly greater in the relapsing patients. While an SDMT definition of relapse based on only three studies may be premature, it is clear that SDMT is the most useful metric discovered thus far for studying this phenomenon.
Another issue is whether or not these studies challenge our conceptions of disease activity in MS. As cognitive changes are documented, it begs the question of how we define disease activity–free status, also termed NEDA.119,120 If cognition were to be routinely monitored in all patients, regardless of their clinical presentation or subjective complaints, deterioration in cognitive status might serve as an additional indicator of disease activity. Damasceno and colleagues 91 recently reported that accounting for neuropsychological test abnormalities significantly lowers estimates of NEDA over 2 years. Cognitive status and processing speed in particular influence everyday functions such as employment, household activities, money management, and use of the Internet to perform everyday tasks. Clearly, expanding NEDA beyond sensory motor functions alone and including the influence of cognitive status will result in a more valid and broader understanding of the influence of MS on everyday life. Efforts to bring cognitive assessment into the clinical routine continue, using both conventional in-person27,28 and computer-based self-administered tests. 121
Finally, while measuring a construct by a single test such as the SDMT may be practical, such an approach runs the risk that the test does not fully represent the construct in question, that is, processing speed. Future research should be geared toward a greater theoretical understating of the concept of processing speed, as well as etiology and course of the impairment in persons with MS.
Footnotes
Acknowledgements
The authors gratefully acknowledge the expert services of Wendy Kaye (McKing Consulting) and the organizational support from Gary Lundstrom and Alicia West (Critical Path Institute).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Benedict receives research support from Accorda, Novartis, Genzyme, Biogen, and Mallinckrodt Pharmaceuticals; is on the speakers’ bureau for EMD Serono (designing CME courses); consults for Biogen, Genentech, Genzyme, Novartis, Abbvie, Roche and Sanofi; and receives royalties from Psychological Assessment Resources. Dr DeLuca receives grant funding from Biogen and EMD Serono, serves on an Advisory board for Biogen, and is on the speakers’ bureau for EMD Serono.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Multiple Sclerosis Society (grant number RG 4869-A-1 to the Critical Path Institute).