
Abstract
The treatment of people affected by multiple sclerosis, particularly the relapsing forms of the disease, has been transformed by the availability of various therapeutic agents. This landmark progress is due to an enormous foundation of clinical research and, particularly, numerous phase II and III clinical trials. Although the research community has many reasons to take pride in this progress, a fundamental question remains about whether opportunities for additional research are being lost due to inadequate clinical trial data sharing.
Clinical trials investigating therapies for people with multiple sclerosis (MS) are an active area of research. A keyword search of “multiple sclerosis” in clinicaltrials.gov on 26 February 2015 yielded 1373 studies. Of these, 447 are considered “open” and either “recruiting” or “unknown,” and 926 were “closed” meaning that they are “completed,” “terminated,” or “not recruiting.” Thus, a large amount of data from MS clinical trials is being generated. Making these study data available for secondary analysis could shed additional light on the disease process and improve the care and quality of life for those with MS, in part because unnecessary duplication could be avoided and drugs could be repurposed more efficiently. 1 The many factors influencing MS (i.e. genetics, environmental influences, immunological factors, cognitive/psychological issues, physical abilities, vocational concerns, and many others) raise the possibility that sharing clinical trial data across disciplines has the potential to impact multiple aspects of the lives of people with MS. However, data sharing also involves risks, challenges, burdens, and ethical considerations that must be addressed so that all stakeholders involved will receive maximum benefits while minimizing risks.
The United States Institute of Medicine (IOM) recently released a report entitled “Sharing Clinical Trial Data: Maximizing Benefits, Minimizing Risk” (http://www.iom.edu/Reports/2015/Sharing-Clinical-Trial-Data.aspx). The report, which was sponsored by a diverse group of stakeholders including government funding agencies, regulators, foundations, and pharmaceutical and medical device manufacturers, was produced by an expert committee (including the author) with the goal of fostering a culture of clinical trial data sharing that will increase scientific knowledge and ultimately improve therapies. The committee recognized that there are several stages in the clinical trial cycle at which data can be shared (Figure 1) and made four main recommendations for responsible sharing of clinical trial data (Table 1).
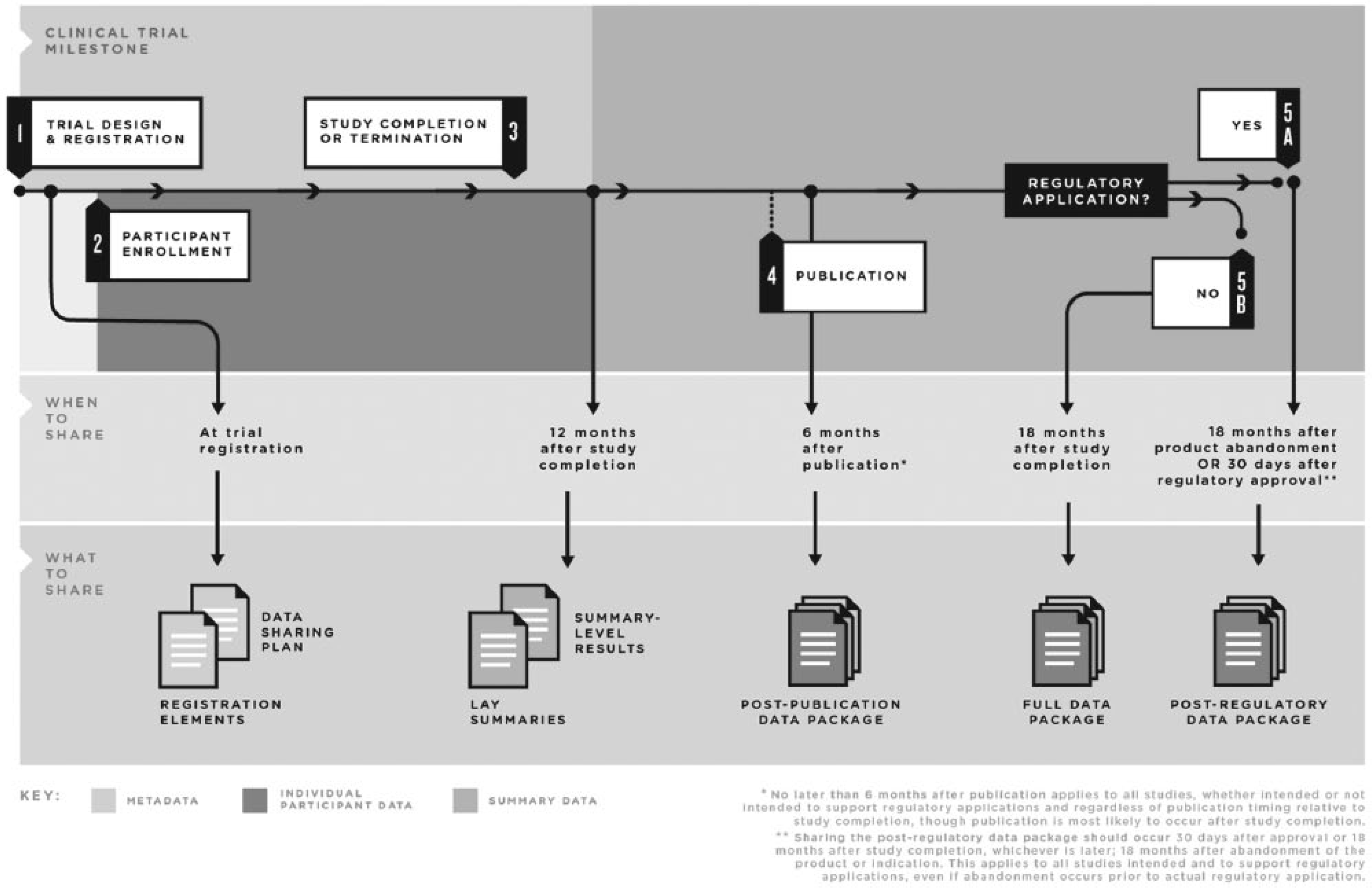
Clinical trial life cycle: when to share data.
Key recommendations for data sharing from the IOM report “Sharing Clinical Trial Data: Maximizing Benefits, Minimizing Risk” (http://www.iom.edu/Reports/2015/Sharing-Clinical-Trial-Data.aspx).
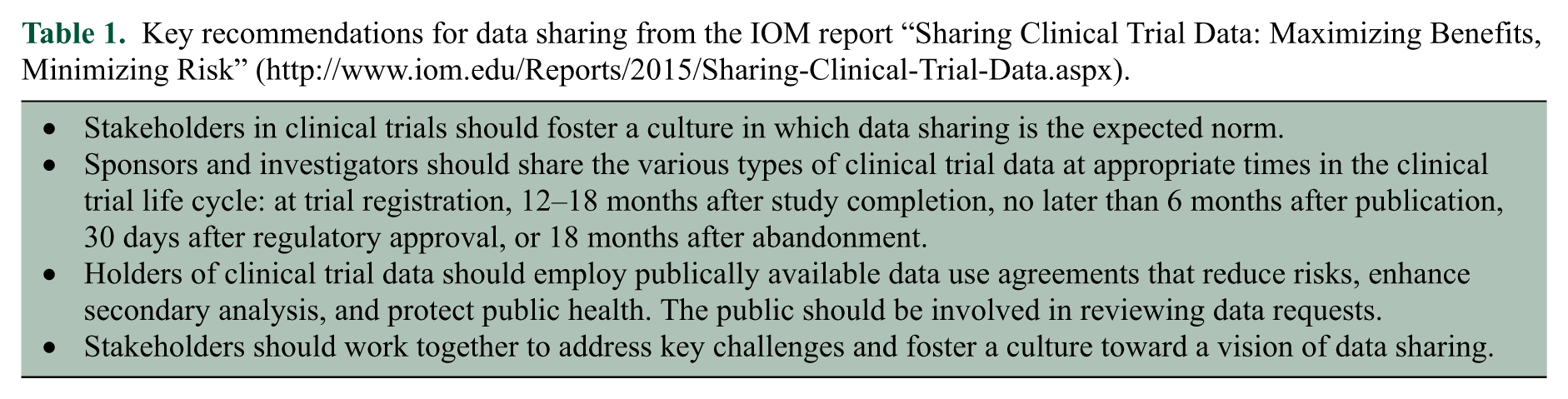
At the outset, the committee suggested that a data-sharing plan should be incorporated as part of the trial registration and that this plan should specify what data will be shared, with whom, and under what circumstances. 2 The committee also recommended that users of shared data generated by others should have certain responsibilities, including providing credit to the group that originally generated the data. 2
The committee also recognized that multiple stakeholders including patients, clinical trialists, companies, funders, regulatory bodies, and others have a vested interest in the data generated and the sharing of these data. Each class of stakeholder brings a distinct perspective and a different set of goals and concerns that should be honored when considering the sharing of clinical trial data. Clinical trialists, those who perform the trial and collect the data, are interested in analyzing and publishing the data with the hopes of observing a positive result that moves the therapy in question forward. Companies and other funders such as universities have a financial stake in what happens to the data from trials they sponsor. Such financial stakes should be carefully considered in the context of data sharing.
Of particular note are the expectations of patients whose views are evolving as a consequence of ready access to their health information. Many patients now expect to have access to their data, they expect that their data will remain confidential, 3 and they expect that researchers will share their clinical trial data. 4 Each patient is taking a risk when participating in a trial, and his or her contribution to science and the societal good should be acknowledged and not minimized. 2 Increased engagement between patients and scientists will increase public trust in the clinical trial process, thus increasing clinical trial participation and funding. 5 This trust, however, is threatened when trialists assume ‘ownership’ concerning data that they generate through clinical trials and unduly limit access to those data.
A welcome development is that the pharmaceutical industry is now sharing data more regularly, but an equally worrisome observation is that academic investigators 3 tend to use the data in a proprietary manner to maximize the number of papers they can publish. Although some investigators do recognize that the landscape is changing, considerable concern remains in the academic community about issues of credit and competition.
Additional concerns about data sharing among stakeholders include rogue analysis, lawsuits, championing of certain agendas, the inappropriate release of commercially competitive information, and patient confidentiality and consent.2,3,5 Initiation of a conversation among these various stakeholders is a necessary next step in establishing parameters and minimizing the risks to data sharing.
Finally, regulatory agencies are interested in the proper use of clinical trial data throughout the drug development pipeline, as this could lead to better outcomes, improved use of taxpayer-financed research, and optimal service to the public. 6 Moreover, sharing data will likely help optimize the regulatory decision process. 7
The publication of the IOM report provides organizations that fund MS clinical trials, including the various national MS societies, an opportunity to establish a model for responsible sharing of clinical trial data by specifying the responsibilities of the investigators, funders, and patients. Because MS is highly complex with many parameters being investigated during clinical trials, data sharing in this field is especially important for moving therapies forward and improving patient outcomes. The MS clinical research community has an opportunity to articulate the vision for the future of sharing MS-related clinical trial data and what sharing does for science. This possibility was anticipated the 2001 IOM report on MS. That committee recommended that ‘Better strategies should be developed to extract the maximum possible scientific value from MS clinical trials.’ 8 However, more work is clearly needed, and there are many challenges.
Currently, several approaches to promoting data sharing in the MS community are in place. One example is the Multiple Sclerosis Outcome Assessments Consortium (MSOAC), which is a collaboration among industry, academic researchers, patient advocacy groups, patients, and regulatory bodies that aims to pool phase III trial data to validate a new clinical measure of MS disability as a primary endpoint in clinical trials.1,9 A related effort is the Sylvia Lawry MS Center (SLMSCR). In addition, the International MS Genetics Consortium (IMSGC) and one of its shared DNA banks at the University of California at San Francisco incorporate an open-access data repository as a cornerstone of the effort. While data sharing by the genetic consortium is not quite the same as clinical trial data sharing, it is nevertheless a powerful example of data sharing that is already happening in the MS field.
Lack of standards in data coding is another barrier to achieving widespread data sharing. The Clinical Data Interchange Standards Consortium (CDISC) has established data standards, tools, and methods meant to standardize the parameters for determining and reporting diagnosis, medical history, disease course, relapse, visual acuity, imaging, functional tests, and others. Standardization consists of the use of common data elements as inputs into a database. 10 Through a working group of MSOAC, CDISC standards have now been established and accepted in MS (http://www.cdisc.org/therapeutic#MS). This important work could be further extended if the community turned its attention to standardization of data generation and collection. Indeed, such efforts could pave the way for harmonization of data from several real-world registries that already exist in the MS community (e.g. MS BASE, EPIC, CLIMB, EDMUS etc.).
Although efforts such as the MSOAC, SLMSCR, CDISC, and IMSGC are important steps in the right direction, the IOM report challenges stakeholders to go further. One possible action is that funders of MS research could require that all recipients of grant funding make their clinical trial data available for secondary analysis according to the timeline outlined in the IOM report. Indeed, such a precedent already exists, as investigators funded by the US Government, including the NIH, are required by law to deposit their results at clinicaltrials.gov. Although stiff penalties exist for failure to do so, only about 30% of investigators comply with this requirement.3,11 In addition, about one-third of clinical trials funded by the National Heart, Lung, and Blood Institute remain unpublished within 4 years of completion. 5 Such statistics raise important questions about the state of data sharing in many fields, including MS.
If routine data sharing is to become a requirement, the infrastructure to support sharing must become a reality. Progress in this area will also require concerted commitment by the funders of MS clinical trials. We currently do not know what such a database would look like, but efforts such as the Yale Open Data Access initiative (http://medicine.yale.edu/core/projects/yodap) point the way. An additional challenge is that investing in data-sharing infrastructure may channel funds away from other areas. In today’s resource-constrained environment, such investments will provoke an important discussion of prioritizing infrastructure at the expense of other research priorities.
Additional considerations must be given to the potential downsides of data-sharing efforts. Reasonable concerns exist about a potential flood of legal actions against investigators and institutions who may be inadequately prepared to provide requested data. Additional concerns exist regarding potential misinterpretation of data and ‘rogue’ analyses, the conclusions from which could create confusion for both patients and health providers. Although we must acknowledge these and other potential risks, they should not prevent efforts directed at a culture of greater data sharing.
In summary, clinical trial data sharing, including data generated from MS trials, has many potential benefits to the scientific community and to patients. However, risks and concerns remain, and the infrastructure and culture to support data sharing are currently only in their infancy. Nevertheless, the complexity of MS disease causation and progression demands more robust clinical trial data sharing. To change the culture, data sharing must be required, rewarded, and enforced. Protections of all interested parties must be in place, and user-friendly infrastructure to support data deposition must be developed and standardized. The challenge is significant, but worthy of our collective effort.
Footnotes
Conflict of Interest
The author was a member of the Institute of Medicine ad hoc committee that developed the recommendations referenced in this viewpoint. In addition the author is an employee of an organization that funds clinical trials.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.