
Abstract
In the article The use of gaming technology for rehabilitation in people with multiple sclerosis, DOI:
Exergaming studies. published trial methodology 25-FWT: 25 Foot Walk Time; ABC: Activities-specific Balance Confidence; AI: Ambulation Index; BBS: Berg Balance Score; CoP: Centre of Pressure; EDSS: Expanded Disability Status Scale; EQ-5D-5L: EuroQual 5 Dimensions-5 Levels; FRT: Functional Reach Test; FSI: Fatigue Symptom Inventory; FSST: Four Square Step Test; GLTEQ: Godin Leisure-Time Exercise Questionnaire; HADS: Hospital Anxiety and Depression Scale; MFIS: Modified Fatigue Impact Scale; MMSE: Mini-Mental State Examination; MS: Multiple Sclerosis; MSIS-29: Multiple Sclerosis Impact Scale; MSSE: Multiple Sclerosis Self-Efficacy Scale; MSWS-12: MS Walking Scale; QoL: Quality of Life; RCT: Randomized Control Trial; RPE: Ratings of Perceived Exertion; SCI-ESES: Spinal Cord Injury Exercise Self-Efficacy Scale; SF-36: Short-Form Health Survey; SOT: Sensory Organization Test; TUG: Timed-Up-and-Go.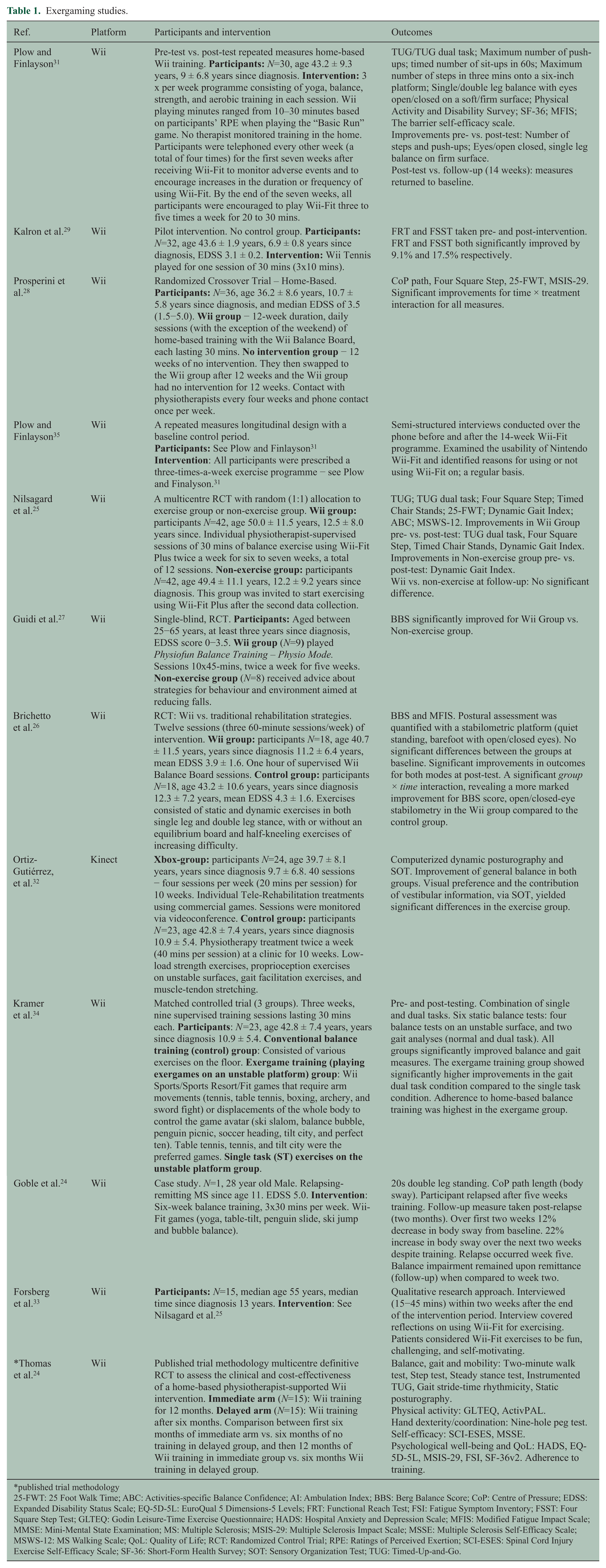
Ref.
Platform
Participants and intervention
Outcomes
Plow and Finlayson31
Wii
Pre-test vs. post-test repeated measures home-based Wii training.
TUG/TUG dual task; Maximum number of push-ups; timed number of sit-ups in 60s; Maximum number of steps in three mins onto a six-inch platform; Single/double leg balance with eyes open/closed on a soft/firm surface; Physical Activity and Disability Survey; SF-36; MFIS; The barrier self-efficacy scale.
Improvements pre- vs. post-test: Number of steps and push-ups; Eyes/open closed, single leg balance on firm surface.
Post-test vs. follow-up (14 weeks): measures returned to baseline.
Kalron et al.29
Wii
Pilot intervention. No control group.
FRT and FSST taken pre- and post-intervention. FRT and FSST both significantly improved by 9.1% and 17.5% respectively.
Prosperini et al.28
Wii
Randomized Crossover Trial – Home-Based.
CoP path, Four Square Step, 25-FWT, MSIS-29. Significant improvements for time × treatment interaction for all measures.
Plow and Finlayson35
Wii
A repeated measures longitudinal design with a baseline control period.
Semi-structured interviews conducted over the phone before and after the 14-week Wii-Fit programme. Examined the usability of Nintendo Wii-Fit and identified reasons for using or not using Wii-Fit on; a regular basis.
Nilsagard et al.25
Wii
A multicentre RCT with random (1:1) allocation to exercise group or non-exercise group.
TUG; TUG dual task; Four Square Step; Timed Chair Stands; 25-FWT; Dynamic Gait Index; ABC; MSWS-12. Improvements in Wii Group pre- vs. post-test: TUG dual task, Four Square Step, Timed Chair Stands, Dynamic Gait Index.
Improvements in Non-exercise group pre- vs. post-test: Dynamic Gait Index.
Wii vs. non-exercise at follow-up: No significant difference.
Guidi et al.27
Wii
Single-blind, RCT.
BBS significantly improved for Wii Group vs. Non-exercise group.
Brichetto et al.26
Wii
RCT: Wii vs. traditional rehabilitation strategies. Twelve sessions (three 60-minute sessions/week) of intervention.
BBS and MFIS. Postural assessment was quantified with a stabilometric platform (quiet standing, barefoot with open/closed eyes). No significant differences between the groups at baseline. Significant improvements in outcomes for both modes at post-test. A significant group × time interaction, revealing a more marked improvement for BBS score, open/closed-eye stabilometry in the Wii group compared to the control group.
Ortiz-Gutiérrez, et al.32
Kinect
Computerized dynamic posturography and SOT. Improvement of general balance in both groups. Visual preference and the contribution of vestibular information, via SOT, yielded significant differences in the exercise group.
Kramer et al.34
Wii
Matched controlled trial (3 groups). Three weeks, nine supervised training sessions lasting 30 mins each.
Pre- and post-testing. Combination of single and dual tasks. Six static balance tests: four balance tests on an unstable surface, and two gait analyses (normal and dual task). All groups significantly improved balance and gait measures. The exergame training group showed significantly higher improvements in the gait dual task condition compared to the single task condition. Adherence to home-based balance training was highest in the exergame group.
Goble et al.24
Wii
Case study. N=1, 28 year old Male. Relapsing-remitting MS since age 11. EDSS 5.0.
20s double leg standing. CoP path length (body sway). Participant relapsed after five weeks training. Follow-up measure taken post-relapse (two months). Over first two weeks 12% decrease in body sway from baseline. 22% increase in body sway over the next two weeks despite training. Relapse occurred week five. Balance impairment remained upon remittance (follow-up) when compared to week two.
Forsberg et al.33
Wii
Qualitative research approach. Interviewed (15−45 mins) within two weeks after the end of the intervention period. Interview covered reflections on using Wii-Fit for exercising. Patients considered Wii-Fit exercises to be fun, challenging, and self-motivating.
*Thomas et al.24
Wii
Published trial methodology multicentre definitive RCT to assess the clinical and cost-effectiveness of a home-based physiotherapist-supported Wii intervention.
Balance, gait and mobility: Two-minute walk test, Step test, Steady stance test, Instrumented TUG, Gait stride-time rhythmicity, Static posturography.
Physical activity: GLTEQ, ActivPAL.
Hand dexterity/coordination: Nine-hole peg test.
Self-efficacy: SCI-ESES, MSSE.
Psychological well-being and QoL: HADS, EQ-5D-5L, MSIS-29, FSI, SF-36v2. Adherence to training.
Get full access to this article
View all access options for this article.