
Abstract
Background:
Falls are common in people with multiple sclerosis (PwMS). Previous studies have generally included small samples and had varied methods.
Objectives:
The objectives of this paper are to compile fall rates across a broad range of ages and disease severity and to definitively assess the extent to which MS-associated and demographic factors influence fall rates.
Methods:
Individual data from studies in four countries that prospectively measured falls for three months were analyzed. We determined fall rates, prevalence of fallers (≥1 falls) and frequent fallers (≥2 falls), location and timing of falls, and fall-related demographic factors.
Results:
A total of 537 participants reported 1721 falls: 56% were fallers and 37% frequent fallers. Most falls occurred indoors (65%) between 6 a.m. and 6 p.m. (75%). Primary progressive MS was associated with significantly increased odds of being a faller (odds ratio (OR) 2.02; CI 1.08–3.78). Fall risk peaked at EDSS levels of 4.0 and 6.0 with significant ORs between 5.30 (2.23–12.64) and 5.10 (2.08–12.47). The fall rate was lower in women than men (relative risk (RR) 0.80; CI 0.67–0.94) and decreased with increasing age (RR 0.97 for each year, CI 0.95–0.98).
Conclusion:
PwMS are at high risk of falls and there are important associations between falls and MS-associated disability, gender and age.
Introduction
Interest in falls in people with multiple sclerosis (PwMS) has increased significantly in the last decade. Studies have reported that at least 50% of PwMS suffer falls within periods of three to six months, with falls in this group being associated with injury,1–3 fear of falling4–6 and reduced activity and social participation. 5
Several studies have identified a diverse range of factors associated with falls among PwMS,3,7–16 and a recent systematic review identified four factors with major association with falls in PwMS: the use of a mobility aid, imbalance, cognitive dysfunction, and progressive MS subtype. 17 However, past studies have differed significantly with respect to their designs, limiting their generalizability and interpretation of their findings. For example, while most studies of falls in PwMS have included adults over age 18, some have focused on older samples aged at least 45 10 or 55 years of age.18,19 Among older adults with MS, impairments related to MS and age may contribute to the risk of falling.
Disease severity and gender mix also vary among the published studies. While some investigators have included people with an Expanded Disability Status Scale (EDSS) score of zero,20–22 others have set a higher EDSS minimum for inclusion.11,13 Although most studies are representative of the gender distribution of MS, one sample included only women 21 and one mostly men. 2 In addition, most have collected falls data retrospectively, asking participants how many times they have fallen in a specified period of the recent past. However, retrospective data collection likely underestimates fall frequency 13 and hence prospective fall recording, although more time consuming and labor intensive, is recommended. 23 Thus, more recent studies of factors associated with falls in PwMS have collected data prospectively.11,13,20–22,24
In order to more accurately assess the relative importance of commonly measured predisposing factors for falls in PwMS, this study combined individual data from studies recently conducted in Australia (AUS), Sweden (SE), the United Kingdom (UK) and the United States (US) to provide the largest sample of PwMS to date with prospectively recorded falls data. This individual level meta-analysis tested the hypothesis that, in PwMS, sustaining a fall or multiple falls is associated with age, gender, mobility aid use, disease severity (EDSS), and disease subtype; we also undertook descriptive analyses to document the frequency of falls by location (indoors vs outdoors) and time of day.
Methods
Standard protocol approvals, registrations and patient consents
Data collected by four centers from 2005 to 2012 were merged. Some of these data have previously been published.11–13 In addition, unpublished data from Sweden and the US were used. All data were collected in accordance with the International Declaration of Helsinki; institutional review boards or ethics committees at the institutions in each country approved the separate protocols (AUS HC09253; SE 2005:119 and 2012:077; UK 10/H0203/66 and US E7244W). Written informed consent was obtained from all participants.
Participants
Data from 537 PwMS were included in this analysis. The sample included 210 participants from AUS, 125 from SE, 148 from the UK and 54 from the US. All samples used standardized criteria for MS diagnosis.25,26 Participants were aged 18 years and older. There were no restrictions for MS subtypes. Disease severity was measured by the EDSS 27 in all samples except in AUS, where the Disease Steps scale 28 was used and converted to EDSS by mobility criteria. Common exclusion criteria were inability to understand and sign an informed consent or record falls for linguistic, cognitive or other reasons, and self-reported health conditions that would interfere with testing procedures. Differences among samples are described below.
Additional inclusion criteria for the Australian sample were ability to stand unsupported for 30 seconds and ability to walk 10 meters with or without aid. Participants in the Swedish sample were restricted to an EDSS score between 1.5 and 7.0, an upper age limit of 75 years, and being relapse free for at least 30 days prior to baseline examination. The UK participants were restricted to an EDSS score between 3.5 and 6.5, and full recovery from the most recent relapse was required for inclusion. EDSS was assessed by self-report using a telephone interview. 29 Additional inclusion criteria for the US sample included an EDSS score of 6.0 or less, an upper age limit of 50 years, being relapse free for 30 days prior to baseline examination, and ability to walk at least 100 meters.
Recruitment strategies
The Australian sample was recruited by a physiotherapist from the outpatient physiotherapy clinic at the MS Australia (MSA) Center in Lidcombe, Sydney. The Swedish sample was recruited by a physiotherapist inviting PwMS living within the recruitment area of Örebro University Hospital; the Mälarhospital in Eskilstuna; the Primary Health Care of Western and Eastern Östergötland County in Motala and Norrköping, and the Sahlgrenska Hospital in Gothenburg. The US sample was recruited from patients receiving medical care at specialty MS center outpatient clinics at a Department of Veterans Affairs medical center and a university medical center, and from the surrounding area, in the Northwest of the United States. The UK sample was recruited from the South-West Impact of MS database, a patient-centered longitudinal study of disease course in PwMS living in the Southwest of England.
Outcome variables
Prospectively collected falls data were obtained using fall diaries. The participants recorded falls daily for three months following their baseline assessment. The fall diaries were returned using reply-paid return envelopes every two or four weeks with reminders (telephone, letter or email) if the diaries were not received in a timely fashion. All studies used specific definitions of falls based on those recommended in consensus guidelines. 23 Circumstances of the falls, including fall time and location, were either collected for all falls (UK n = 148, SE n = 76) or for the first two (US n = 54, AUS n = 210) or four (SE n = 49) falls each month.
Factors with potential association with falls
Data on walking aid use, demographics and MS subtype were collected at baseline on self-report questionnaires at all study centers.
Data analysis
Following analysis of normality of distribution, the data sets from each country were compared for heterogeneity using a Kruskal-Wallis test, with post hoc analysis using Bonferroni-corrected Mann-Whitney tests for between-group comparisons. Although the data sets were demonstrated to be heterogeneous, sensitivity analysis of the main logistic regression by sequential removal of each country’s data set did not significantly affect the outcomes, therefore all data sets were retained in the final analysis. Frequencies were calculated for circumstances of falls with within-variable differences assessed using the one sample test of proportions. Associations between the demographic and MS disease status variables were analyzed using multi-variable logistic regression analysis, including EDSS as a categorical variable. To control for family-wise error rates, adjusted confidence interval (CI) and p values were also calculated using a Bonferroni correction. 30 In these analyses, participants reporting no falls during three months or “non-fallers” were compared with participants reporting one or more falls or “fallers.” Additional logistic regression analyses compared factors with potential association with falls between fallers (0 or 1 falls) and frequent (≥2) fallers. Fall rates in men and women were compared with an incident rate ratio computed with negative binomial regression.
Results
Demographic and MS disease characteristics for each cohort and for the total sample are presented in Table 1.
Demographic and prospective three-month falls data for each cohort and for the total sample.
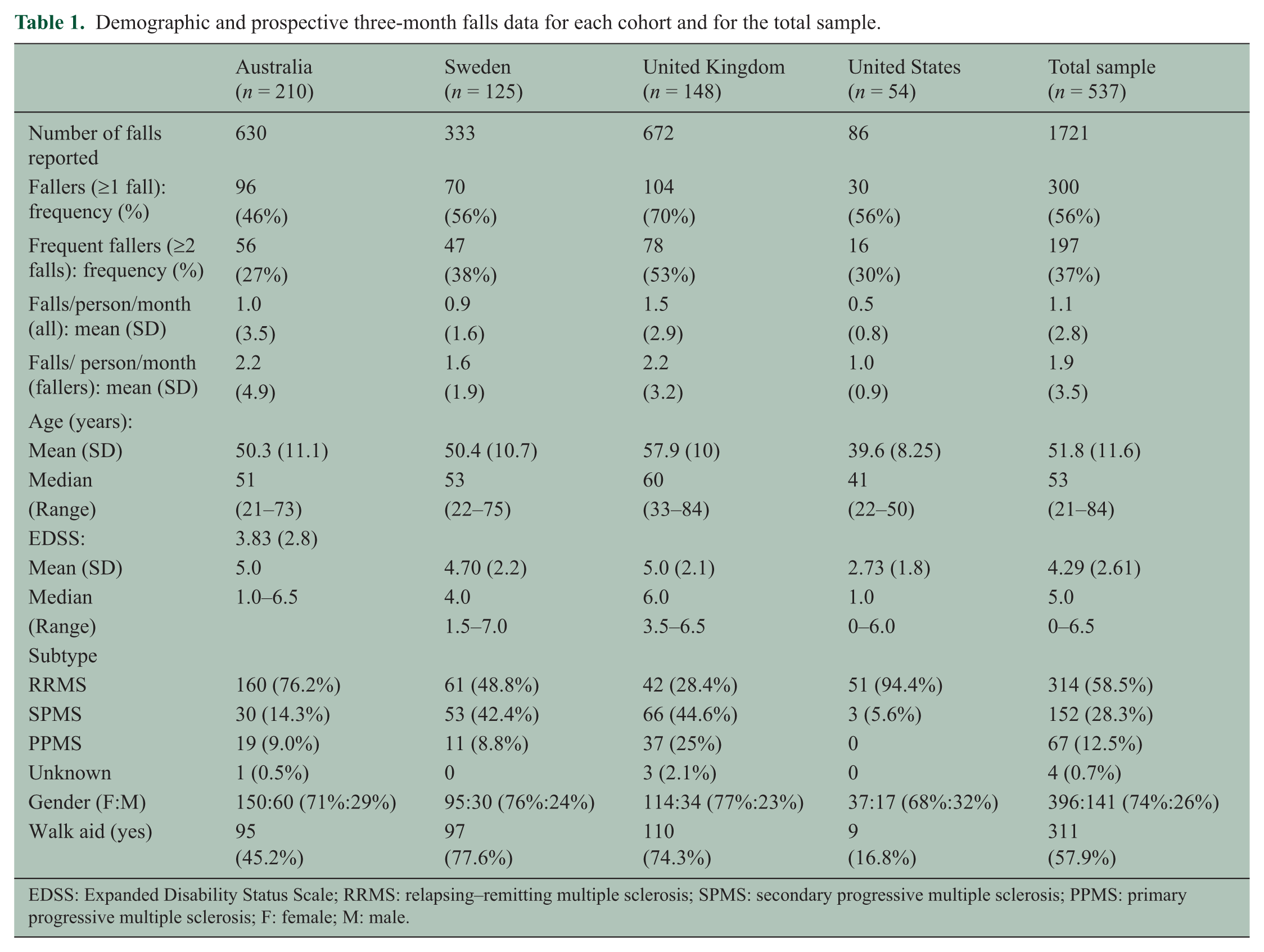
EDSS: Expanded Disability Status Scale; RRMS: relapsing–remitting multiple sclerosis; SPMS: secondary progressive multiple sclerosis; PPMS: primary progressive multiple sclerosis; F: female; M: male.
Prevalence and rate of falls
Of the total sample, 300 participants (56%) reported falling at least once (defined as fallers) and 197 (37%) participants reported falling at least twice (defined as frequent fallers) in the three-month follow-up periods. Participants reported a total of 1721 falls and the average rate of falls was 1.1 falls/person/month. Within the fallers, the fall rate was 1.9 falls/month. The UK cohort had the highest fall frequency (falls/month), and the US had the lowest. The Australian cohort had the lowest proportion of frequent fallers, but the highest rate of falls within the faller subgroup. The number of falls, fallers and fall rates are summarized in Table 1.
Fall location and time of day
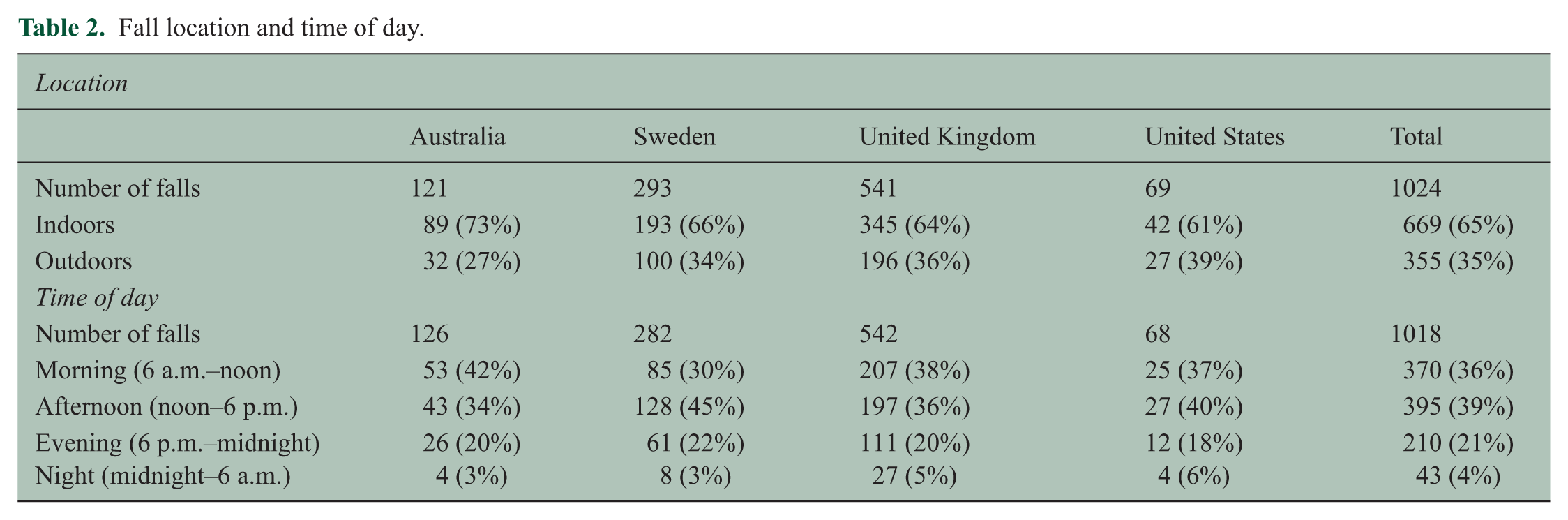
Fall location data were available for 1024 falls and fall time data were available for 1018 falls (Table 2). In all cohorts participants fell more frequently indoors than outdoors (total sample, z = 20.13, p <0.0001—one sample test of proportions), and falls occurred more frequently in the morning and afternoon (total sample = 75%) than in the evening or night.
Fall location and time of day.
Factors associated with falls
Logistic regression revealed that being a faller was statistically significantly associated with being classified as having primary progressive MS (unadjusted odds ratio (OR) 2.02; 1.08–3.78) and there was also a trend for association between being a faller and younger age (OR 0.98; 0.97–1.00 for each year ). There was a non-linear relationship between being a faller and EDSS classification, with the OR peaking at EDSS levels 4.0 and 6.0 (Figure 1). These peaks were statistically significant both in the unadjusted and adjusted analyses, although the CI were wide in both analyses. The differences found between the fallers and non-fallers were also found when comparing the fallers and frequent fallers, with one exception as the association between being a frequent faller and younger age was statistically significant in this analysis (unadjusted OR 0.97; 0.95–0.99). There were no statistically significant associations between fall status and gender or use of a walking aid (Table 3).
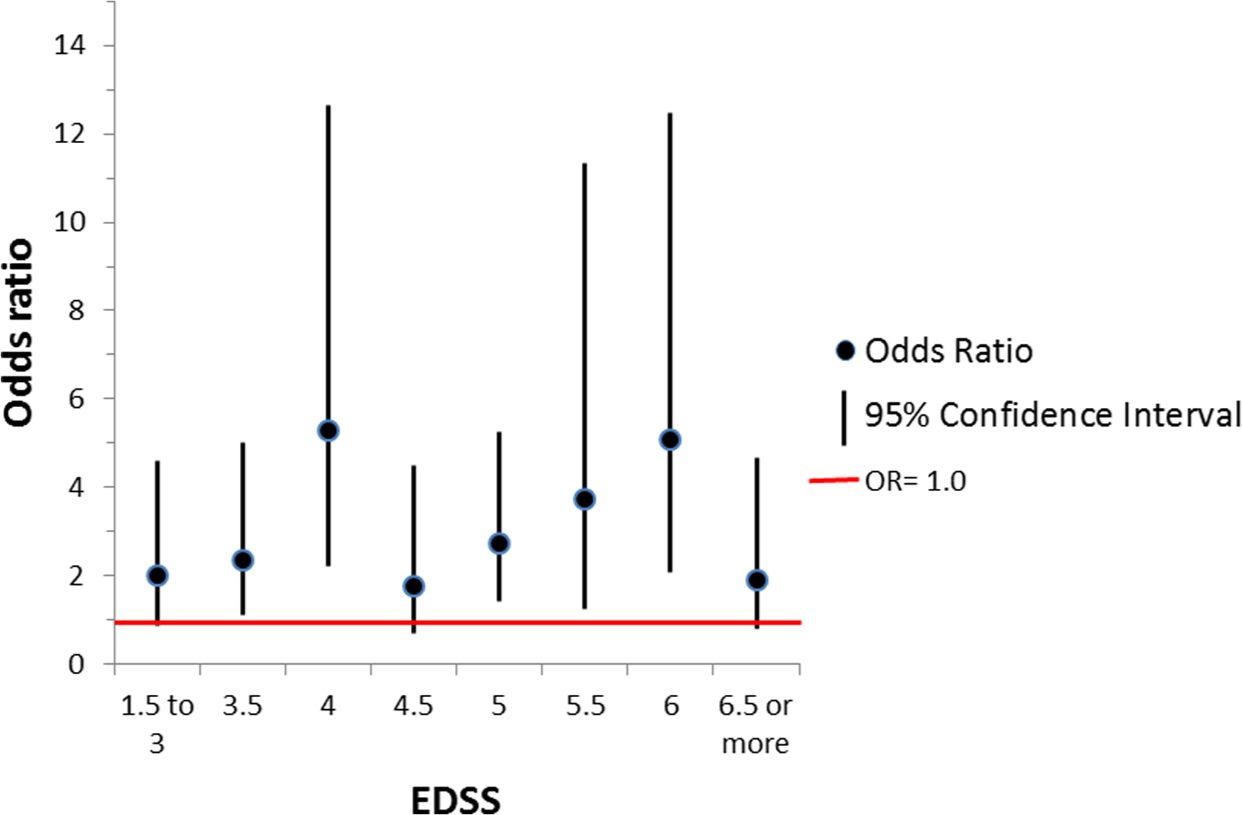
Association between EDSS and risk of being classified as a faller (≥1 fall, unadjusted OR).
Analysis with adjustments for multiple comparisons.
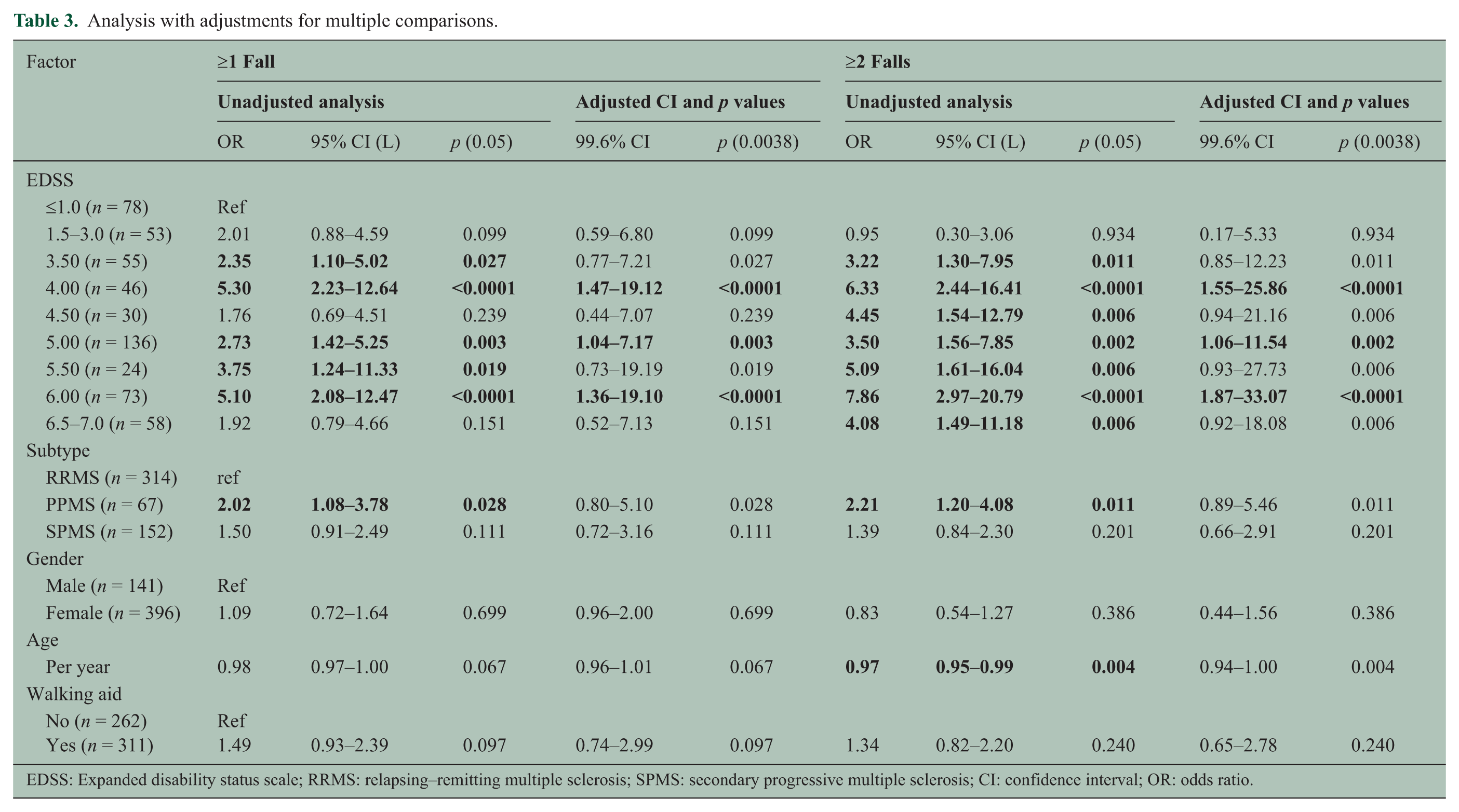
EDSS: Expanded disability status scale; RRMS: relapsing–remitting multiple sclerosis; SPMS: secondary progressive multiple sclerosis; CI: confidence interval; OR: odds ratio.
Fall rate (falls/person/month)
Interestingly, whereas no significant differences were evident in the proportion of men and women fallers, fall rate was lower in the women than the men (RR = 0.80; CI 0.67–0.94). Similar to the analyses of the odds of being a faller, the rate of falls decreased by 3% with each year of age (Table 4).
Relative falls rate.
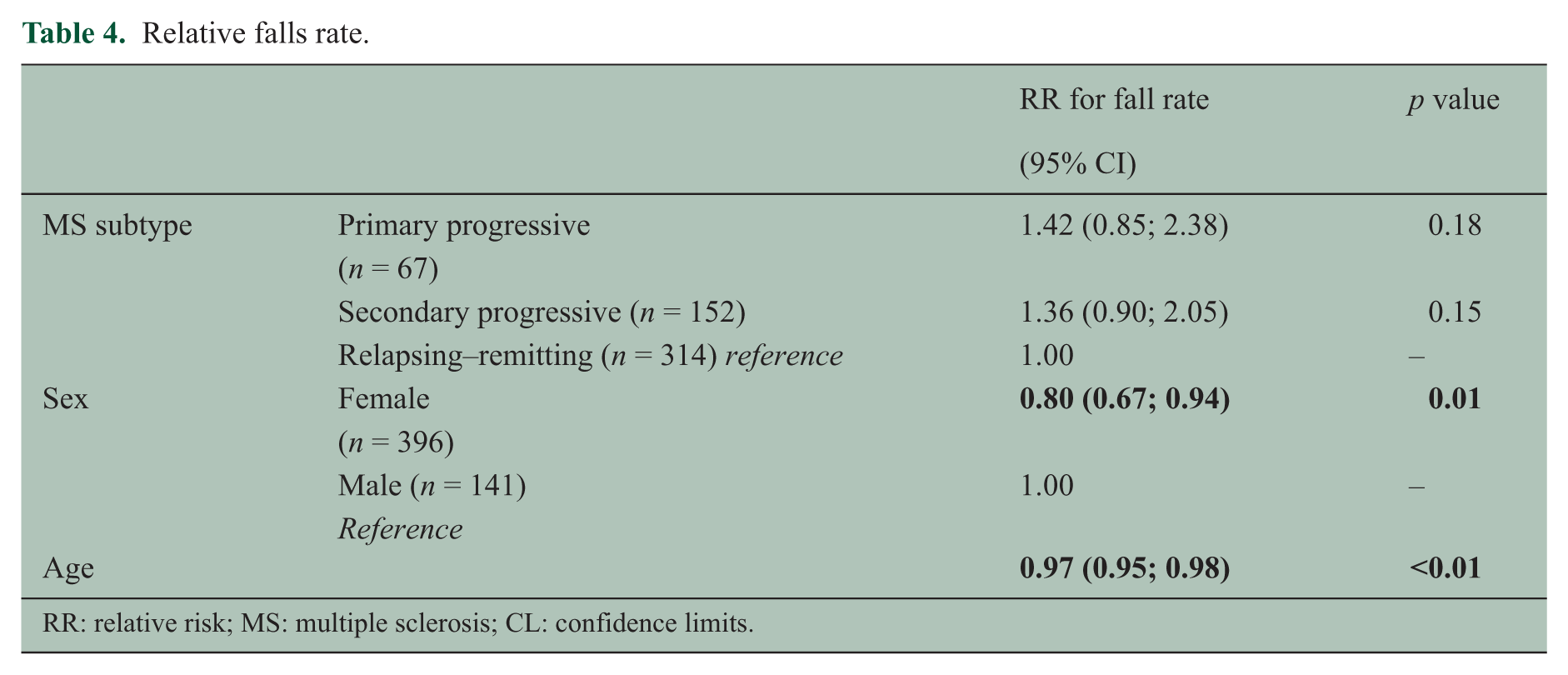
RR: relative risk; MS: multiple sclerosis; CL: confidence limits.
Discussion
This is the first meta-analysis of risk factors for falls in PwMS using only prospectively collected fall data. In this large pooled international sample of ambulatory individuals, the average fall rate was approximately one fall/month. Higher odds of being classified as a faller were associated with a primary progressive MS subtype and higher EDSS scores, consistent with previous studies.10,28,31 In contrast with previously reported results, use of a walking aid was not significantly associated with higher fall risk.
This meta-analysis provides further detail on the relationship between fall risk in MS and disease severity as measured by the EDSS. It suggests that fall risk peaks at an EDSS score of 4.0 (when quantifiable mobility limitations are first acknowledged) and 6.0 (when a walking aid is required). While this could be an artifact of the nonlinear nature of the EDSS scale, 32 it may also be that this increase in risk is associated with these important transitions in mobility status. EDSS is primarily a measure of MS-associated impairments, although walking distance and need of walking aids are also included in the scale. 31 In this study we also found an association between falls and primary progressive MS subtype. Since this association was independent of EDSS it does not reflect the higher level of disability in primary progressive MS but may reflect the difficulty of adapting to a constantly, and sometimes fairly rapidly, progressing level of disability.
Interestingly, there were statistically significant associations between more falls and younger age. Sustaining multiple falls was associated with younger age and the relative rate of falls was higher for younger participants. These results are surprising given that previous studies in older adults suggest that older age is a risk factor for more falls. 33 It is possible that in a relatively young sample (mean age 52 years; range 21–84 years), the higher fall rates in the younger participants may reflect differences in activity levels with age, with younger people undertaking more activities that put them at risk for falls. Unfortunately, we did not collect data on exposure, including activities involving standing, walking, and more physically challenging activities, and so are not able to confirm this hypothesis. It is also possible that falls decrease as people with MS become older because they become more aware of their risk for falls and become more cautious and possibly less active. 34
In our sample the men had a significantly higher fall rate than the women, suggesting that men with MS who fall are at risk for frequent falls. This finding is in line with previous studies.10,17 We also documented that most falls occurred indoors and during the daytime, guiding fall prevention interventions. Among older adults, risk factors for indoor and outdoor falls differ. Outdoor falls are associated with younger age, being male, and greater physical activity whereas indoor falls are associated with older age, being female, poor health and greater physical disability. 33 Providing information on when and where falls occur may help promote awareness of specific risks in PwMS and caregivers. Personal level interventions, such as use of fall-risk reduction strategies or regular exercise, and environmental level interventions such as reducing hazards and installing safety devices in the home or workplace, could be guided by this information. Strategies on when to use walking aids or scheduling activities and rests could be outlined if a pattern of fall risk is detected.
Strengths of this study
This analysis pooled data from a number of similar studies. This provided a large sample with participants from four different countries covering a major part of the world where MS is prevalent. The sample size allowed subgroup analyses and the impact of outliers in the separate samples was reduced by merging the data sets. The sample was not restricted by MS subtype, and the participants represent PwMS living both in urban and rural areas. In addition, data were collected during different times of the year and captured different climate conditions. Differences in inclusion criteria across the cohorts also provided a broad spectrum of demographic and diagnostic characteristics for the total sample.
The prospective recording of falls minimized recall bias, enhancing the validity of the results. Using fall diaries returned every two or four weeks combined with reminders resulted in a high return rate. Similar reminder systems are recommended for future studies. Now that many people have cell phones and computers, other approaches to fall counting, such as using telephone text messages, purpose-designed applications, or emailed electronic surveys to capture falls would also be interesting to evaluate.
Limitations of this study
This study has a number of limitations. As this was not a planned multi-site study, data were collected and reported differently at the different sites and participant inclusion and exclusion criteria also differed. The analyses were also limited to data elements collected consistently among the sites, limiting analysis of potentially important variables identified in other studies such as muscle weakness, impaired balance and continence. We were also unable to assess the consequences of falls such as associated injuries, which may have significant personal and financial implications.
The results of this study may also be affected by the limited three-month time period of recording falls. Longer periods may identify additional fallers but have the potential disadvantage of lower reporting compliance. Reporting falls on a regular basis can also increase the awareness of falls risk and thus possibly reduce fall frequency. Moreover, the willingness to participate in a falls study may be higher in those having experienced falls. The risk of over- or underestimating the overall fall prevalence in the present study is albeit considered to be small.
Suggestions for future research
While the evidence base for the factors contributing to falls risk in MS has developed significantly in recent years, the high incidence of falls in PwMS found in this study indicates that there is still a pressing need for research to identify approaches to help PwMS manage falls and reduce fall risk. The International Classification of Functioning, Disability and Health has been suggested as a framework for developing and evaluating multi-disciplinary fall risk consultations to identify individuals at high risk for falls, map their risk factors, and provide accordingly targeted interventions. 35
This study provides further support to previous evidence indicating that PwMS around the world are at high risk for falls. Those with primary progressive MS are at increased fall risk and fall risk peaks at an EDSS score of 4.0 and 6.0, likely representing transitions in walking ability. Younger patients and men have higher rates of falls. These falls occur most often indoors during the day. As PwMS rarely talk to health care professionals about fall prevention, 20 to help prevent falls, care providers should conduct simple fall risk screening and recommend appropriate interventions to reduce the occurrence of falls in this high-risk group.
Footnotes
Acknowledgements
The authors thank statistician Garnett McMillan, PhD, National Center for Rehabilitative Auditory Research, Portland VA Medical Center, Portland, OR, USA, and Siobhan Creanor, associate professor in Health Statistics, Centre for Medical Stats & Bioinformatics-Translational & Stratified Medicine (Peninsula Schools of Medicine and Dentistry), Plymouth Hope, UK.
Conflicts of interest
None declared.
Funding
SE: Ylva Nilsagård was supported by the Research Committee in Örebro County Council, Biogen Idec and the Norrbacka- Eugenia Foundation.
US: Michelle Cameron was supported by a Career Development Award from the VA, Rehabilitation Research & Development Service.
Rajarshi Mazumder was supported by the Oregon Multidisciplinary Training Program in Health Services Research, grant number T32 HS017582 from the Agency for Healthcare Research and Quality (AHRQ) and the 2012 Foundation of the Consortium of Multiple Sclerosis Centers.
AUS: Phu Hoang and Stephen Lord were supported by NHMRC Fellowships and a grant from Multiple Sclerosis Research Australia.
UK: Hillary Gunn and Jennifer Freeman were supported by a grant from the Physiotherapy Research Foundation, Chartered Society of Physiotherapy, UK.