
Abstract
Background:
Risk for multiple sclerosis (MS) disease-modifying therapies (DMT) must be assessed on an ongoing basis. Early concerns regarding the first-approved DMTs for MS have been mitigated, but recently licensed therapies have been linked to possibly greater risks.
Objectives:
The objective of this review is to discuss risk assessment in MS therapeutics based on an international workshop and comprehensive literature search and recommend strategies for risk assessment/monitoring.
Results:
Assessment and perception of therapeutic risks vary between patients, doctors and regulators. Acceptability of risk depends on the magnitude of risk and the demonstrated clinical benefits of any agent. Safety signals must be distinguishable from chance occurrences in a clinical trial and in long-term use of medications. Post-marketing research is crucial for assessing longer-term safety in large patient cohorts. Reporting of adverse events is becoming more proactive, allowing more rapid identification of risks. Communication about therapeutic risks and their relationship to clinical benefit must involve patients in shared decision making.
Conclusions:
It is difficult to produce a general risk-assessment algorithm for all MS therapies. Specific algorithms are required for each DMT in every treated-patient population. New and evolving risks must be evaluated and communicated rapidly to allow patients and physicians to be well informed and able to share treatment decisions.
Introduction
Since the first well-designed clinical trials of disease-modifying therapies (DMTs) for multiple sclerosis (MS), short- and long-term risk assessment and the evaluation of risk/benefit of therapy has been a concern. Interferon-betas and glatiramer acetate had noted risks that raised initial concerns about their use and compromised adherence, 1 but those concerns have been largely mitigated over two decades of use. Newer and ostensibly more-effective agents have been associated with other, probably greater, risk concerns. 2 The evaluation of therapeutic risk for MS is an ever-changing landscape as new agents are introduced and more systematic risk information evolves. An International Workshop on Risk Evaluation and Monitoring in Multiple Sclerosis Therapeutics (Paris, 19–21 September 2012) explored therapeutic risks in general and specifically in MS. Highlights of the discussions and recommendations are reported.
Risk and risk assessment
Assessment of therapeutic risk is complex and includes objective elements guided by data and subjective elements reflecting risk perceptions. A major issue is who is best placed to judge on risks. Risk perception may differ among patients and their families, health care providers, society and policy makers. The evaluation and acceptance of risk must consider demonstrated clinical benefits and costs at a population and individual level. Currently, an integrated perspective and consistent approach to articulating and monitoring risk is lacking.
Therapeutic risk assessment involves the interplay of evidence, clinical practice, epidemiology, individual and societal acceptance and politics and can be accurately determined only with access to all data on the risks/potential benefit of intervention. Risks associated with scientific uncertainty of a new therapeutic agent must be recognised, and to enable shared decision making, the inherent value judgements required to assign acceptable levels of risk need to be assessed by an effective bidirectional communication between patients and health care professionals.
The concept of risk varies depending on its context. In common usage, a ‘risk’ is an adverse event (AE) related to any identified cause, such as the risk of lung cancer in smokers. In an administrative context with regulatory authorities responsible for licensing therapeutic agents, risk assessment is based on evidence that the potential benefits of a new therapy will outweigh the likely risks; in some cases the balance may necessitate the imposition of recommended/required risk-management plans. Sociologically, risk monitoring requires organising the social responsibility of decision making and imposing accountability. In decision theory, risk involves purely mathematical probabilities to calculate, for example, a rate of ‘expected utility’. 3
Known risks for MS therapies
Based on clinical trials outcomes and postmarking data, AEs are known for currently licensed MS DMTs. As more DMTs have been licensed, and with longer-term usage of older therapies, risk perception of both older and newer therapies has changed. Adverse effects associated with the newer therapies tend to be more severe than those associated with earlier approved agents, such as the risk of progressive multifocal leucoencephalopathy (PML) with natalizumab, rituximab and fumarate, and bradycardia and herpes varicella-zoster (HVZ) infections with fingolimod (Table 1).
Risks of licensed, frequently used and anticipated multiple sclerosis therapies.
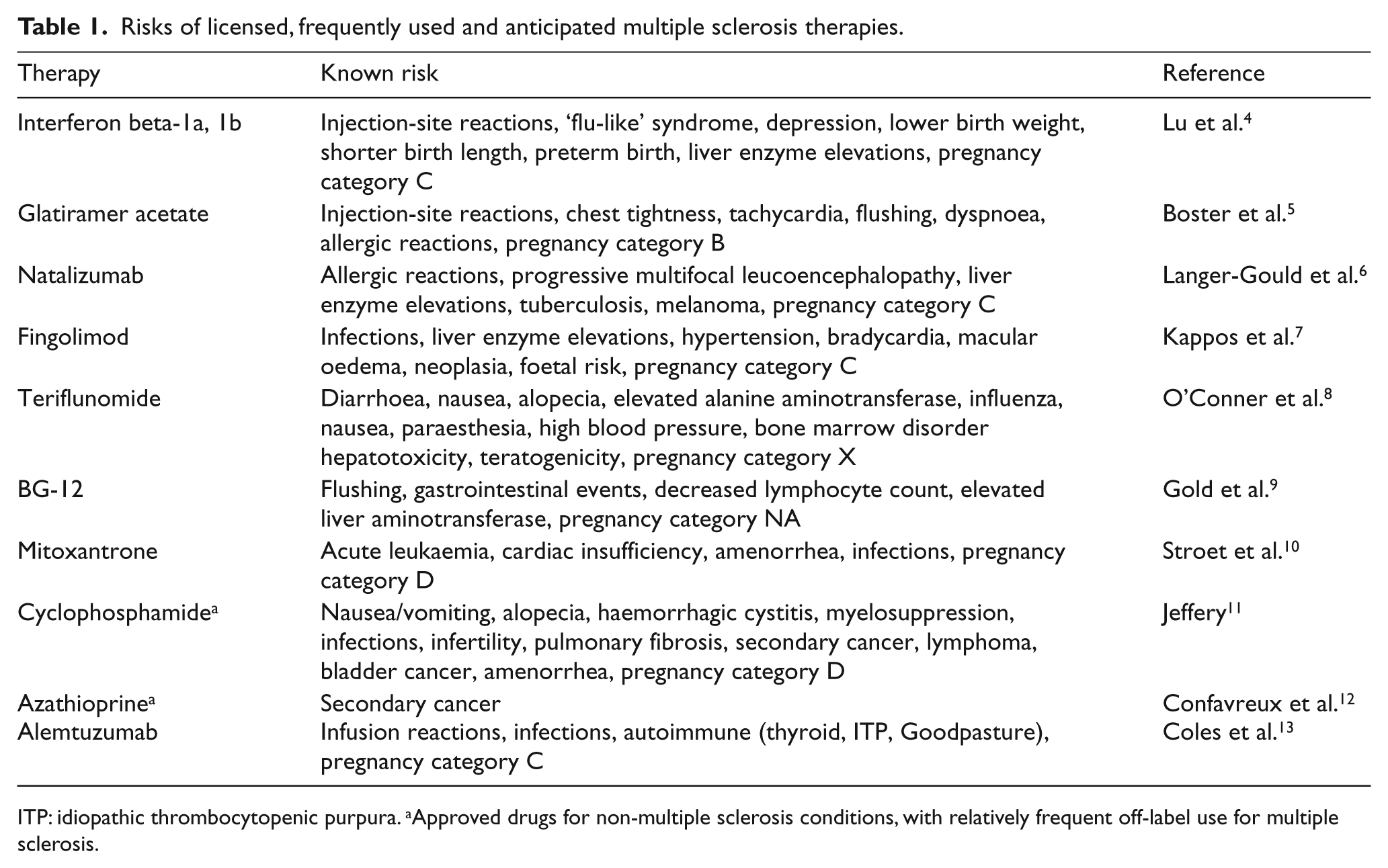
ITP: idiopathic thrombocytopenic purpura. aApproved drugs for non-multiple sclerosis conditions, with relatively frequent off-label use for multiple sclerosis.
When treatments are registered there is a scientific uncertainty about their risks. It can be difficult to detect a risk signal associated with therapy because of the influence of confounding issues such as uncertainty about general or non-treated MS population prevalence of the signals, use of concomitant therapies and comorbidities unrelated to therapy, and delayed emergence of AEs relative to therapy initiation. These may not have been captured in controlled, relatively short trials with insufficient numbers of patients. Once specific AEs have been identified with a therapy, risk-management programmes can be developed, (e.g. PML with natalizumab (retrospectively after emergence of the events in open-label use) and cardiac side effects with fingolimod (both prospectively and retrospectively).
Assessing risk in developing MS therapies
Assessment of risk for any therapeutic product begins with preclinical studies, initial clinical assessments (phase I), proof-of-concept (phase II) and larger-scale pivotal trials (phase III). A Data and Safety Monitoring Board (DSMB) serves as a sponsor- and investigator-independent oversight group for safety, study integrity and often efficacy and helps mitigate harm by recommending trial changes recruitment, screening or treatment parameters (e.g. dosing levels), or even trial termination if a safety signal emerges. 14
When rare, noteworthy events are detected during a clinical trial or in phase IV post-marketing studies, a clearly defined statistical boundary that helps separate the emerging signal from pure chance must be defined which, when crossed, requires the DSMB to consider termination for risk (or early signs of efficacy).
After an agent is approved, post-marketing research programmes are crucial for monitoring longer-term safety in larger numbers of treated subjects. 15 Phase IV post-marketing studies should be more safety oriented with requirements imposed by local regulatory agencies. Increasingly, reporting of safety is changing from passive (reactive) surveillance to proactive surveillance involving fuller reporting by patients and the public. Reactive surveillance has many limitations: An accurate analysis of adverse drug reaction rates cannot be performed because of the often substantial under-reporting of AEs, and of the limited number of exposed patients; causal links between the treatment and AEs cannot always be shown; and a correct risk/benefit ratio cannot be evaluated since safety events are not linked to efficacy results.
Disease registries represent a powerful tool for building a long-term safety record useful for assessing risk/benefit ratios in a real-world setting, but require a greater workload for doctors, significant financial support, and suffer from attrition of patient and doctor involvement over time. Strategies such as matching controls, stratification, regression and propensity score analysis can reduce bias and confounding factors. 16 Pharmacovigilance programmes must identify safety issues immediately and rapidly alert healthcare professionals so that they and patients can jointly consider whether to stop/switch therapy.
Strategies for risk avoidance and mitigation once risks are known
Therapeutic benefit can be seen in the context of the potential benefit from treatment that would be lost with the failure to treat. The determination of treatment risk dynamically evolves over the therapy’s lifetime. Clinical trials may capture many of the important risks of a drug, but are short term and with generally low numbers of treated patients in a highly controlled environment. True risks may become evident only in less ‘selected’ patients exposed to a drug for a much longer period. Post-marketing safety surveillance can identify unforeseen risks but may be the hardest data to collect unless long-term proactive vigilance is initiated. Since acceptability of treatment risk usually depends on the magnitude of a treatment’s clinical benefits, the greatest risk acceptance is generally associated with the highest treatment impact.
In most relevant cases in MS, risk avoidance or mitigation strategies have been developed in response to specific known risks for individual agents, usually developed with intense research after an agent has been approved for use. For example, anti-John Cunningham (anti-JC) virus antibody status, duration of treatment exposure and pre-treatment immunosuppression have been identified as risk factors for developing PML with natalizumab in relapsing MS that guide decisions to avoid or terminate the therapy in patients with these risk factors. 17 Quantification of neutralising antibodies to interferon-betas can inform treatment responsiveness and the potential need to switch therapy, thus avoiding unnecessary exposure in those who may be predicted to have low treatment benefit. 18 Finally, now alemtuzumab has been approved in the European Union (EU) as a therapy for MS, the search for a reliable pre-treatment serum marker heralding the development of humoral autoimmunity may help stratify and reduce risk of emergent complications such as immune-mediated thrombocytopaenia, thyroiditis, and glomerulonephritis for some patients. 19
Assessment of risk by regulators and technology assessors
Frameworks for risk-mitigation are developed by regulators for therapies to assess the potential risks and provide recommendations for additional post-marketing collection of safety data (risk-management and pharmacovigilance plans). The European Medicines Agency (EMA) 2012 guidelines recommended that the goal of treatment determines the type of post-marketing study design/duration, populations, and primary endpoints and indicated which potential AEs characteristic of the drug class should be assessed. 20 The MS clinical community should provide scientific and clinical expertise to regulators concerning approval of agents, but with a clearly defined policy on conflicts of interest.
The United Kingdom (UK) National Institute for Health and Clinical Excellence (NICE) aims to reduce variation in the availability and quality of National Health Service (NHS)-provided treatments and care through evidence-based guidance on which represent their assessment of the best-quality care and value for money, using quality-adjusted life years (QALY) (where each QALY is a year of life in full health). This is a social approach to estimate cost effectiveness and NICE decisions are primarily driven by cost and demonstrated therapeutic benefit rather than risk, but do not assess the financial consequences of AEs, or social costs.
In 2012 the United States (US) Institute of Medicine (IOM) reviewed the Food and Drug Administration (FDA)’s system of assessing approved drugs and made recommendations including the adoption of a consistent decision-making framework for regulatory actions and the monitoring and evaluation of benefits/risks of a drug throughout its life cycle using a benefit and risk-assessment management plan (BRAMP). 21
Patients’ perception of risks
The role of the patient in therapeutic decision making is central. Up-to-date, balanced, and evidence-based discussions are essential in the modern patient/doctor partnership to help inform decision making. 22 Understanding that patients differ in their desire to be involved in the discussion and their understanding of sophisticated and complex research, and differing methods of weighing benefits and risk is a rapidly expanding research focus.23,24
A survey of natalizumab-treated MS patients and their doctors showed that patients understand uncertainties communicated openly and many consider their disease sufficiently severe to be more willing than their doctors to take higher risks. 23 A study using a North American MS patient self-report registry (North American Research Committee on Multiple Sclerosis (NARCOMS)) found an extremely wide spectrum of tolerance to risk regarding MS therapies. 25 Factors, including sex, disability, and recent MS disease activity predicted tolerance to risk. The psychodynamics of aversion to risk, vs seeking gain, should be considered. 26
Communicating risk and risk assessment for health care providers, patients and other parties
Communicating risk and risk assessment is crucial to enable accurate, shared treatment decisions with patients. Individual patients do not experience ‘likelihood,’ or population-level rates of events. They experience single outcomes (something happens or does not) and people making decisions may be frightened or too ill to process complex information and make appropriate decisions. 27
Using numbers and statistics to highlight risk and benefit can be helpful, but the ability for a patient to understand complex numerical representations of risk can be limited. 27 Thus, numbers should be communicated in a standardised, consistent way (visual aids are useful) and related to a relative risk with which people are familiar. Doctors tend to translate numbers into words when discussing the risk of treatment AEs with their patients, but there is no universal agreement as to the correct words to use. Risk reduction should be expressed in absolute numbers, since the concept of relative risk reduction often overstates treatment effects. 27 Often the optimum way to present risk is to use non-numeric possibility (relative, comparative or categorical) and quantifiable, graphical probability (absolute, comparative or incremental). 27 It is important to consider that each patient will have different priorities and risk tolerance and may change his or her perception and tolerance of risk over time.
Risk communication needs to be an informed and understandable dialogue between health care professionals and patients and depends on establishing mutual respect and trust involving simple, relevant information in a two-way exchange. The doctor must be aware of the conflicting information sources accessible by the patient (for example via the Internet) and be sensitive to the psychological and social factors that influence how patients respond to risk information. The physician and allied health professional staff should clearly outline all treatment options (including no treatment), and the consequences, ensuring that the patient understands. The medical team should accept the patient’s decision even if they believe it may not be the best decision, but the doctor’s experience, expertise and personal ethics should not be compromised in the process.
Concluding remarks
Currently known risks and the likelihood that risk will increase with longer and broader use of MS therapies makes it essential to give more attention to MS therapeutic risk assessment (Table 2). Risk assessment during clinical development is generally adequate, largely because of DSMB oversight and regulatory monitoring, even if insufficient to assess long-term risks in open market usage. Post-registration risk assessment is neither universally standardised nor adequate. Improvements will require consistent, enforceable policies, preferably harmonised on a global rather than a national basis. The feasibility of developing a general risk assessment algorithm for all MS therapeutics is questionable. There is a need to produce specific risk assessment algorithms for each therapy and each treated-patient population, based on the risk/benefit profile of the therapies in question and the specific patient populations in which they are used.
Recommendations for managing treatment safety for multiple sclerosis (MS).
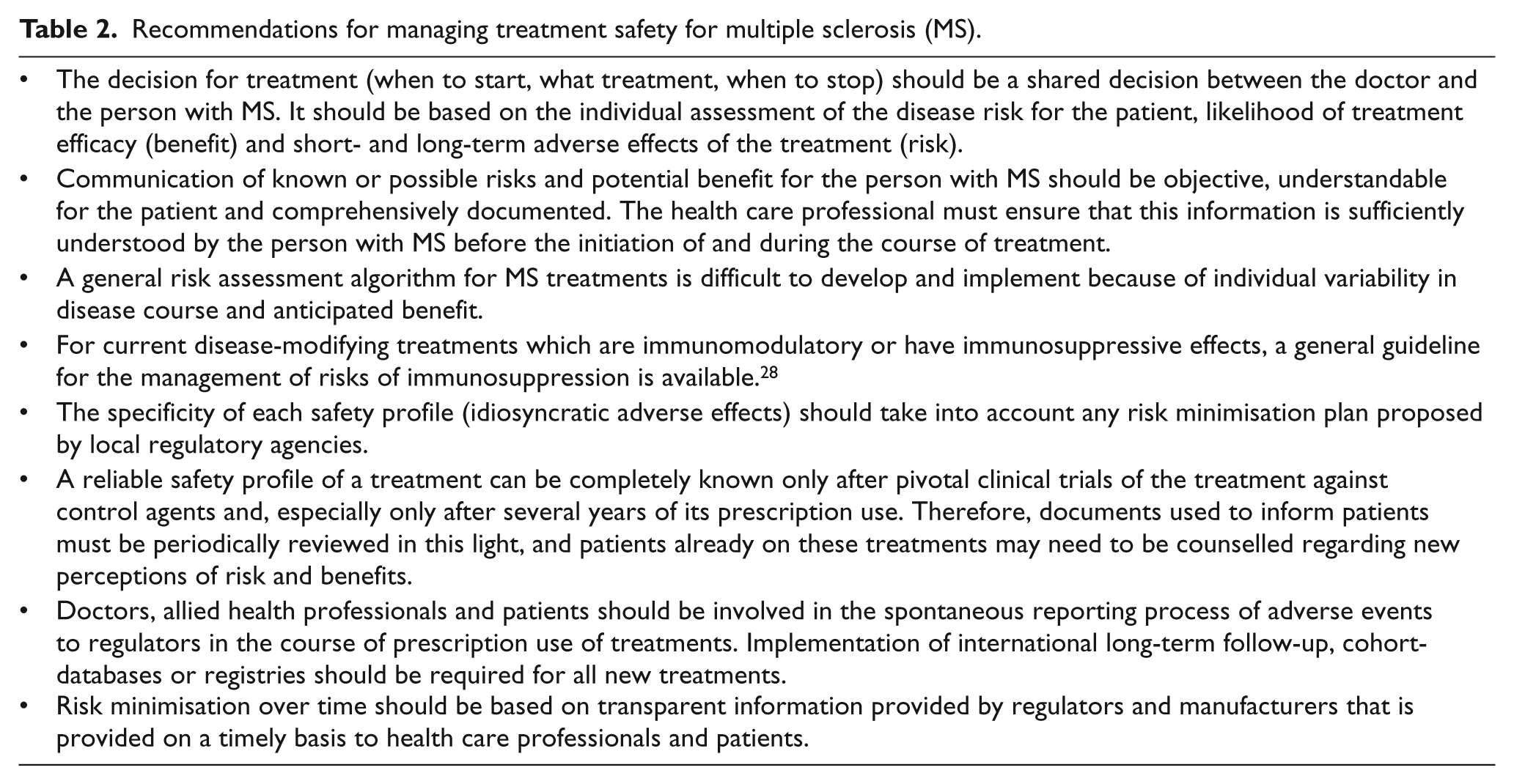
Risk monitoring, avoidance and mitigation/correction by industry, regulators and healthcare providers requires clear proactive plans for gathering and analysing data, and for communication between all parties, including patients and their families. Ongoing updates of new and evolving data on recognised risks must occur in a timely fashion, so that physicians, patients and their families are well informed. More active measures of communication between patients and doctors are needed, using and developing all available media and technological supports, including social media and educational activities for health care professionals and patients.
Workshop participants
J-P Boissel, Lyon, France; M Clanet, Toulouse, France; J Cohen, Cleveland, OH, USA; G Comi, Milan, Italy; G Cutter, Birmingham, AL, USA; P De Jager, Boston, MA, USA; A Fischer, London, UK; R Fox, Cleveland, OH, USA; M Freedman, Ottawa, Ontario, Canada; A Goodman, Rochester, NY, USA; H-P Hartung, Dusseldorf, Germany; C Heesen, Hamburg, Germany; B Keller-Stanislawski, Frankfurt, Germany; B Kieseier, Dusseldorf, Germany; C Lubetzki, Paris, France; F Lublin, New York City, NY, USA; RA Marrie, Winnipeg, Manitoba, Canada; H McFarland, Bethesda, MD, USA; E Meslin, Indianapolis, IN, USA; A Miller, New York City, NY, USA; X Montalban, Barcelona, Spain; T Moreau, Dijon, France; J Palace, Oxford, UK; C Polman Amsterdam, The Netherlands; S Reingold, Salisbury, CT, USA; A Rid, Zurich, Switzerland; N Scolding, Bristol, UK; J Seegar, Boston, MA, USA; M Trojano, Bari, Italy; S Vukusic, Lyon, France; E Waubant, San Francisco, CA, USA; M Wiles, London, UK; J Wolinsky, Houston, TX, USA.
Footnotes
Conflicts of interest
Over the past 12 months MC had consulting agreements or received speaker honoraria from the following commercial entities, or its institution received research financial support from: Biogen Idec, Merck Serono, Teva Pharmaceuticals, Sanofi Genzyme, Novartis. Travel funds for this workshop that served as the basis of this manuscript were provided by the foundation ARSEP.
SCR has received consulting fees and/or travel funds in the past three years for data safety monitoring board and other advisory activities from Bayer HealthCare, Coronado Biosciences Inc, Cleveland Clinic Foundation, Eli Lilly & Company, Merck Serono, European Committee for Treatment and Research in Multiple Sclerosis, Genentech, F. Hoffmann-LaRoche, INC Research, Ironwood Pharmaceuticals Inc, Isis Pharmaceuticals Inc, MediciNova Inc, Medimmune, National Multiple Sclerosis Society, Novartis Pharmaceuticals Corporation, Observatoire Français de la Sclérose en Plaques, Opexa Therapeutics, Sanofi-Aventis, SK Biopharmaceuticals, Synthon Pharmaceuticals Inc, and Teva Pharmaceuticals Industries; travel funds for the meeting that served as the basis for this manuscript were provided by the Fondation pour l’aide à la Recheche sur La Sclérosis en Plaques.
Over the past 12 months, JSW has served on advisory boards or data monitoring committees, has had consulting agreements, or received speaker honoraria from the following commercial entities: Genzyme, advisory board, speakers bureau, Hoffman LaRoche (member steering committee), Janssen RND (consultant), Medscape CME (consultant), Novartis Pharmaceuticals Corporation (member steering committee and consultant), Sanofi (member steering committees), Serono Symposia International Foundation (speaker), Teva Neuroscience (consultant), Teva Pharmaceuticals (consultant), XenoPort (consultant). Royalties are received for out-licensed monoclonal antibodies through the University of Texas Health Science Center at Houston (UTHSCH) to Millipore (Chemicon International) Corporation since 1993. Grant or contractual support to the UTHSCH derives from the National Institutes of Health, 2 U01 NS045719-07 (principal investigator of the subcontract to UTHSCH for image analysis) and 2RO1-EB002095-06A1 (co-investigator), the National Multiple Sclerosis Society (RC-1019 A5), and Sanofi/Genzyme.
HPH has received speaking fees and honoraria for consulting from Bayer HealthCare, Biogen Idec, Genzyme, EMD Merck Serono, Novartis, Teva Pharmaceuticals, Sanofi Aventis and Hoffmann-La Roche.
RJA received compensation as medical writer to assist in preparation of the manuscript and was engaged by the co-authors independently of meeting sponsorship.
Funding
The workshop was organised with the financial support of ARSEP (Aide à la Recherche sur la Sclerose en Plaques) Foundation through an unlimited educational grant from Teva Pharmaceuticals. The Foundation and its sponsor had no role in the scientific programme of the workshop. Members of the foundation or its sponsor neither attended the workshop nor participated in the meeting or in the writing of the draft.