
Abstract
Background:
Chronic cerebrospinal venous insufficiency (CCSVI) has been proposed as a possible cause of multiple sclerosis (MS).
Objectives:
The CoSMo study evaluated the association between CCSVI and MS.
Methods:
The primary end-point of this multicentric, case-control study was to compare the prevalence of CCSVI between patients with MS, patients with other neurodegenerative diseases (ONDs) and healthy controls (HCs). Color-coded duplex sonography was performed by a sonologist and the images were sent to one of three central sonologists for a second reading. Agreement between local and central sonologists or, in case of disagreement, the predominant judgment among the three central readers, was required for a diagnosis of CCSVI. All readings, data collection and analysis were blinded.
Results:
The study involved 35 MS centers across Italy and included 1874 subjects aged 18–55. 1767 (94%) were evaluable: 1165 MS patients, 226 patients with ONDs and 376 HCs. CCSVI prevalence was 3.26%, 3.10% and 2.13% for the MS, OND and HC groups, respectively. No significant difference in CCSVI prevalence was found amongst the three cohorts (MS versus HC, OR = 1.55, 95%CI = 0.72–3.36, p = 0.30; OND versus HC, OR = 1.47, 95%CI = 0.53–4.11, p = 0.46; MS versus OND, OR = 1.05, 95%CI = 0.47–2.39, p = 0.99). High negative and low positive agreement was found between the local and centralized readers.
Conclusions:
CCSVI is not associated with MS.
Keywords
Introduction
In 2009, Zamboni et al. proposed that anomalous cerebrospinal venous return due to multiple stenoses of the jugular veins, vertebral veins and azygous veins, a condition called chronic cerebrospinal venous insufficiency (CCSVI), could be the cause or one of the causes of multiple sclerosis (MS). 1 This abnormal condition was detected in almost all MS patients in their study by means of a high-resolution echo color Doppler (ECD) and transcranial color-coded Doppler sonography (TCCS), with a sensitivity, specificity and predictive positive/negative value of 100%. They suggested that the increased venous pressure may result in colloids, lymphocyte and erythrocyte extravasation, with an inflammatory reaction in the brain and spine. 1 The strong association of CCSVI to MS found in this initial study was considered a proof of the pathogenetic theory. 1 Angioplasty of jugular veins, the so-called “liberation therapy,” was then proposed to correct these venous abnormalities, 2 with claims of beneficial effects on disease activity and burden. The strong impact that these claims had on the MS community hastened attempts to confirm these findings. As a consequence of this pressure, the majority of epidemiological studies on the association between CCSVI and MS were of small sample size and monocentric design. Most were performed by blinded operators, but only few had a second reader to give a diagnosis by double-checking the scans and completely avoiding any contact with the study subject. An extensive overview of the studies performed to date on the possible association between CCSVI and MS is presented in Table 1. The most important limitations of these studies are also summarized. 1,3 –24
Studies on the association between CCSVI and MS.
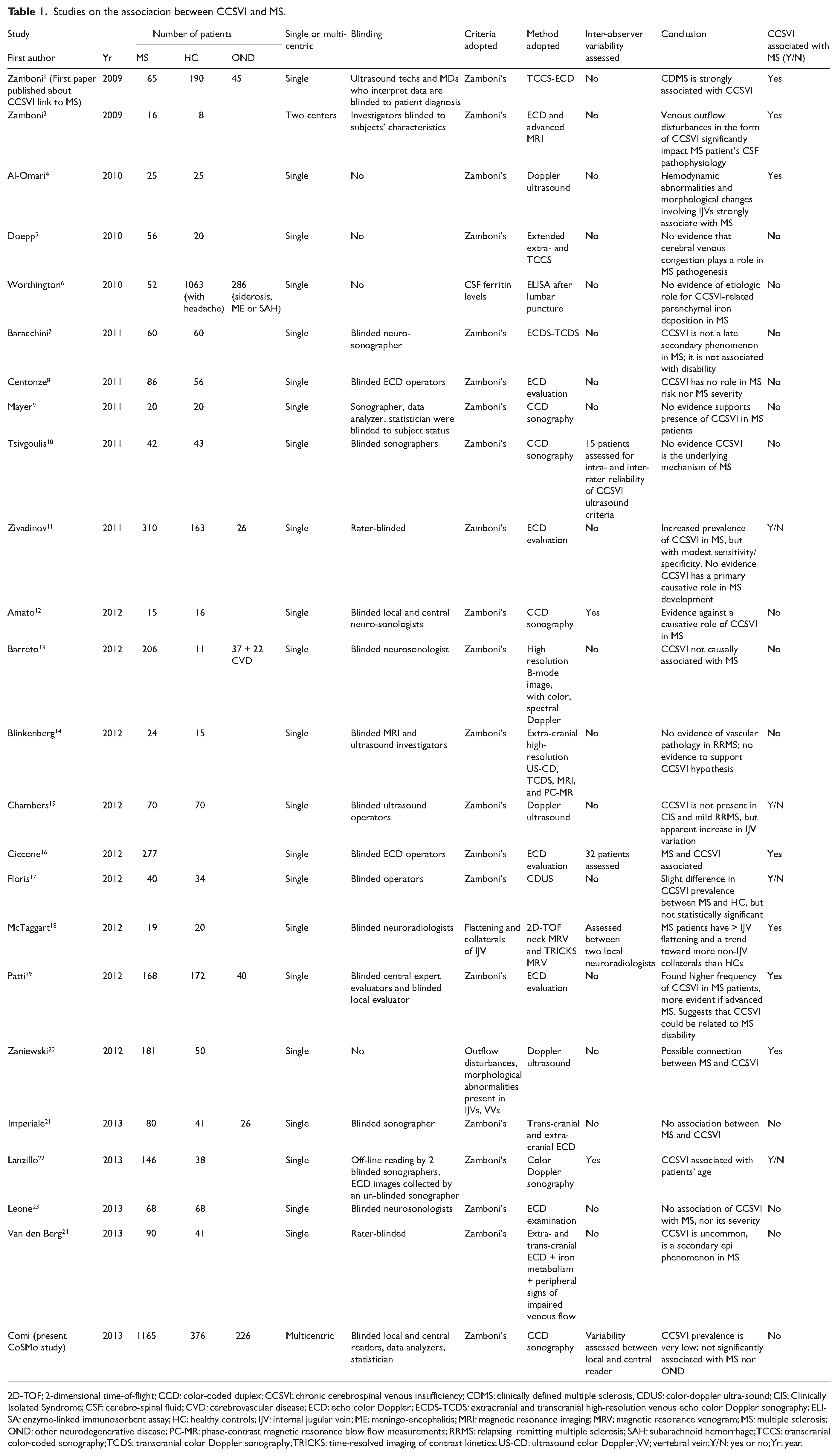
2D-TOF; 2-dimensional time-of-flight; CCD: color-coded duplex; CCSVI: chronic cerebrospinal venous insufficiency; CDMS: clinically defined multiple sclerosis, CDUS: color-doppler ultra-sound; CIS: Clinically Isolated Syndrome; CSF: cerebro-spinal fluid; CVD: cerebrovascular disease; ECD: echo color Doppler; ECDS-TCDS: extracranial and transcranial high-resolution venous echo color Doppler sonography; ELISA: enzyme-linked immunosorbent assay; HC: healthy controls; IJV: internal jugular vein; ME: meningo-encephalitis; MRI: magnetic resonance imaging; MRV; magnetic resonance venogram; MS: multiple sclerosis; OND: other neurodegenerative disease; PC-MR: phase-contrast magnetic resonance blow flow measurements; RRMS: relapsing–remitting multiple sclerosis; SAH: subarachnoid hemorrhage; TCCS: transcranial color-coded sonography; TCDS: transcranial color Doppler sonography; TRICKS: time-resolved imaging of contrast kinetics; US-CD: ultrasound color Doppler; VV; vertebral vein; Y/N: yes or no; Yr: year.
Many of these studies failed to confirm the strong association reported by Zamboni. 5 –9,12,14 Two independent systematic reviews point towards a possible association between CCSVI and MS; however, owing to the substantial variation in the strength of this association, lack of blinding and heterogeneity between studies, definitive conclusions could not be made. 25,26 Furthermore, the occurrence of serious adverse events following interventional procedures led national health authorities and scientific societies to produce clear statements on this topic. 27 –29 Overall, this issue has both concerned and confused the MS community.
In late 2010, the “Fondazione Italiana Sclerosi Multipla” (FISM) funded this large epidemiological study to evaluate the association between CCSVI and MS. The rationale, study design and methodology were recently published. 30 The primary objective of the CoSMo study, named after the Italian words ‘‘CCSVI: Studio Osservazionale Sclerosi Multipla e OND,’’ which translates to Observational Study of the prevalence of CCSVI in multiple sclerosis and OND, is to compare the prevalence of CCSVI in MS patients, healthy controls (HCs) and patients with other neurological diseases (ONDs). The secondary objectives are the evaluation of the correlation of CCSVI with demographic and clinical parameters.
Patients and methods
The CoSMo study methods are described in detail elsewhere. 30
Study design and participants
CoSMo was an observational, case-control, cross-sectional, multicentric study, where MS patients, HCs and patients with ONDs were recruited in a competitive manner from centers throughout Italy. All examiners and data analysts were blinded. Subject recruitment began in November 2010 and ended in June 2012. Male and female individuals aged between 18–55 years were included in the study. Exclusion criteria for all groups were: the presence of any acute or chronic invalidating disease/s which could interfere with the objective of the study.
The MS group included patients with either relapsing–remitting (RR), secondary progressive (SP), or a primary progressive (PP) course, with disease duration between 1 month and 25 years before the screening visit; and patients with clinically-isolated syndrome (CIS) with a maximum disease duration of 5 years. Patients could not be in clinical relapse (at least 30 days since the last relapse). The second group included HCs, namely subjects without any relevant disease and without any family history of MS or family relation to another MS patient. The third group included patients with OND. Two subtypes of patients were included in the OND group: patients with neurodegenerative diseases (ONDn), such as Parkinson’s disease or amyotrophic lateral sclerosis; and patients with inflammatory CNS disorders (ONDi), such as neuromyelitis optica (NMO), acute disseminated encephalomyelitis (ADEM), encephalitis and neuro-systemic lupus erythematosis.
This study was approved by the Ethics Committee of each study center. We obtained written informed consent from all patients and healthy controls participating in the study. The CoSMo study was registered at ClinicalTrials.gov (NCT01384825).
Procedures
The primary end-point of the CoSMo study was to compare the prevalence of CCSVI among the three study subgroups. In order to have a positive CCSVI diagnosis, study subjects needed to fulfill at least two of the five criteria previously described by Zamboni 1 :
Reflux in the internal jugular veins (IJVs) and/or vertebral veins (VVs);
Reflux in deep cerebral veins;
Presence of proximal IJV stenosis or other anatomical abnormalities;
Absence of flow in IJVs and/or VVs; or
Negative difference between the cross-sectional area (CSA) of the IJV in the supine position and the CSA in the upright position.
CCSVI assessment was performed after color-coded duplex (CCD) examination, carried out by a trained sonologist in a blinded manner. To maintain blinding, we instructed subjects not to communicate with the examiner and their bodies were covered to avoid revealing any evidence of medication by injection. The sonologist entered the examination room only after the patient was positioned on the bed. A specific training and final examination were required for each sonologist, in order to address possible limitations attributed to poor training and to guarantee uniform behavior in performing the examination. After the local sonologists performed the investigation and made their diagnoses, all images and video clips of the CCD examination were sent at random to one of the three central expert sonologists (three of the authors), whom performed a second blinded reading. If the CCSVI (presence/absence) diagnosis matched, the final report was issued for that patient. If there was no agreement between the local and central examiners, the other two central readers would perform independent readings and the one which was accepted by at least two of the three central sonologists became the final diagnosis.
Statistical analysis
We calculated study size in order to guarantee a power of 80% at a 5% significance level, to detect an association of CCSVI with MS, described by odds ratios (ORs) ranging from OR = 2 (MS versus HC and MS versus OND) in the case of a low CCSVI prevalence in the HC reference group (5%), to OR = 1.50 in the case of a high prevalence of CCSVI in the HC reference group (30%). We compared CCSVI prevalence in MS patients and HCs or patients with ONDs by the Chi-squared test. CCSVI prevalence was calculated, along with its 95% confidence interval (CI), in the three study groups. We calculated the strength of the association by ORs and their 95% CI. An additional aim of this study was to evaluate CCSVI prevalence in the MS subgroups (CIS, RR, SP and PP). We evaluated differences in CCSVI prevalence among MS subgroups by Chi-squared test for heterogeneity and for trend. The impact of other risk factors (age, sex, sonological center, geographical region, echograph) on CCSVI prevalence was evaluated by logistical regression analysis (a penalized regression model was used to assess the single sonologic center effect). We assessed agreement between the local sonologist and central reader by Cohen kappa statistic, along with positive/negative agreement. 31
Results
The CoSMo study enrolled 1874 subjects: 52 were excluded for technical reasons related to the CCD exam and registration, and 55 because of protocol violations (age, disease duration, associated pathologies). Therefore, the final analysis was performed on 1767 persons, including 1165 MS patients, 226 patients with ONDs and 376 HCs. Table 2 summarizes the main characteristics of the study subjects. Patients with ONDs were significantly older than both MS and HCs (p < 0.001) and, in the MS group, a significantly higher prevalence of females was observed, compared to both groups of HC and OND patients (p < 0.001). MS group disability, measured by the “Expanded Disability Status Score” (EDSS), was associated with increased age, and, with the exception of the PP form, with disease duration.
CoSMo study subjects.
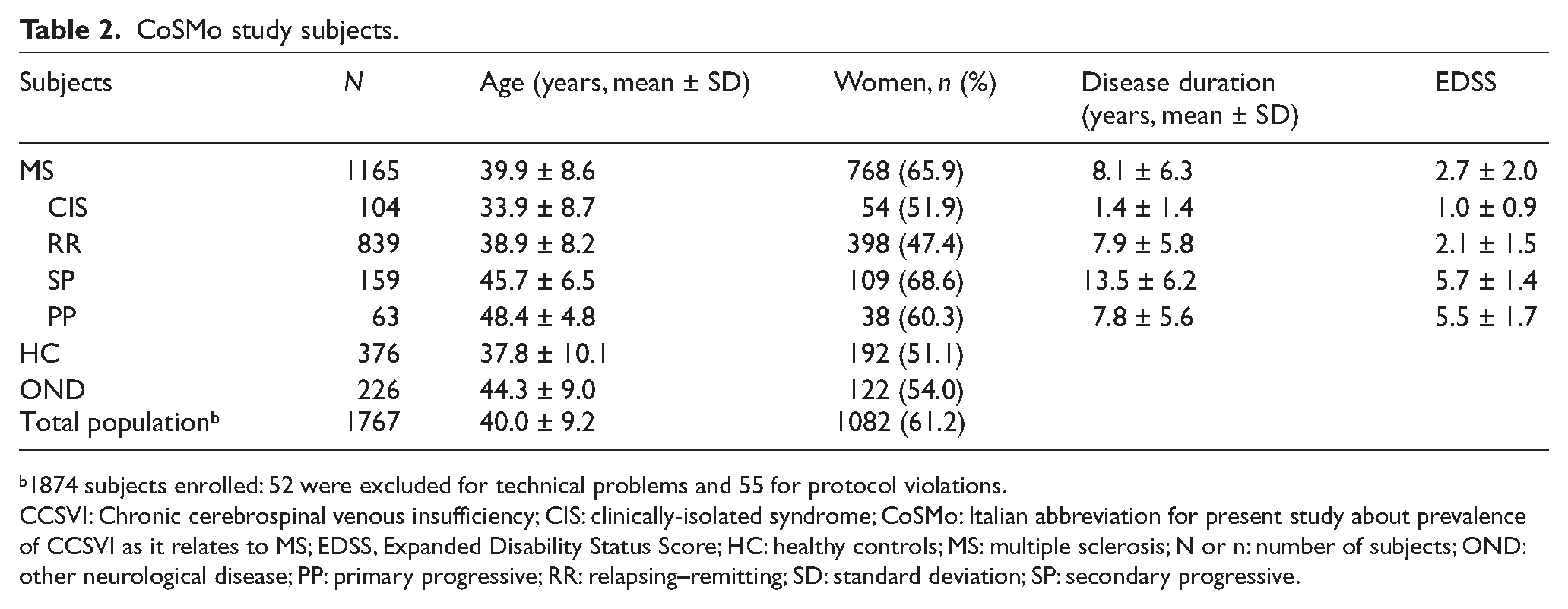
1874 subjects enrolled: 52 were excluded for technical problems and 55 for protocol violations.
CCSVI: Chronic cerebrospinal venous insufficiency; CIS: clinically-isolated syndrome; CoSMo: Italian abbreviation for present study about prevalence of CCSVI as it relates to MS; EDSS, Expanded Disability Status Score; HC: healthy controls; MS: multiple sclerosis; N or n: number of subjects; OND: other neurological disease; PP: primary progressive; RR: relapsing–remitting; SD: standard deviation; SP: secondary progressive.
Recruiting centers (n = 35) were distributed over the entire Italian territory. For further details on participating centers, see supplemental Table A1 (in Appendix).
CCSVI prevalence for all three study groups, the primary end-point of the CoSMo study, was 3.00%, with a 95% CI = 2.28%–3.93%: Specifically, prevalence was 3.26% in MS patients, 3.10% in OND patients and 2.13% in HC. No statistically significant difference was observed among these three study groups (MS versus HC: OR = 1.55, 95% CI = 0.72−3.36, p = 0.30; OND versus HC: OR = 1.47, 95% CI = 0.53–4.11, p = 0.46; MS versus OND: OR = 1.05, 95% CI = 0.47–2.39, p = 0.99). MS patient subgroup analysis did not reveal an association between CCSVI and disease course (Figure 1). Although the PPMS form had a slightly higher CCSVI prevalence, it did not attain statistical significance.
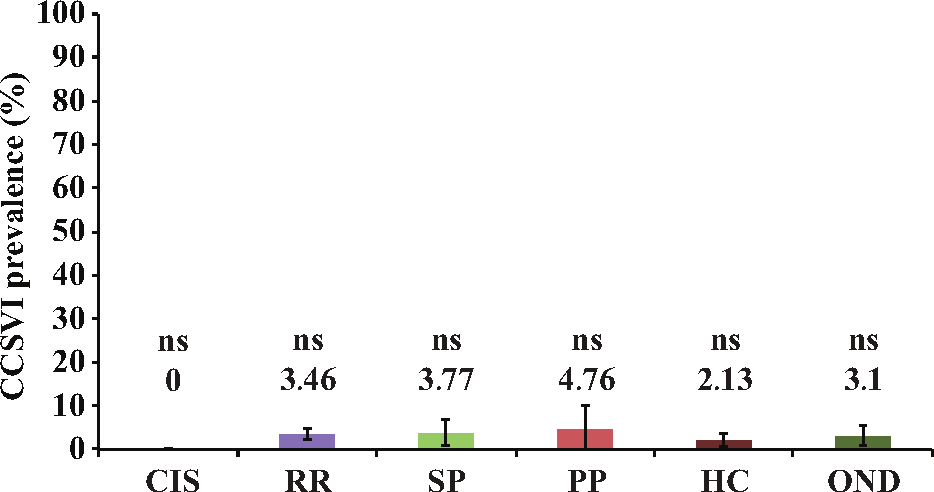
CCSVI prevalence in multiple sclerosis patient subgroups.
The overall CCSVI prevalence in the local readings was significantly higher, as compared to the first central reading (14.9% versus 3.2%; p < 0.001); however, there was no difference in prevalence among the three groups (MS versus HC: OR = 1.39, 95% CI = 0.98–1.97, p = 0.07; OND versus HC: OR = 1.30, 95% CI = 0.80–2.10, p = 0.28; MS versus OND: OR = 1.07, 95% CI = 0.72–1.59, p = 0.84). Even though CCSVI prevalence among the three study groups was comparable, overall CCSVI prevalence according to local readings had a very high degree of variability (p for heterogeneity = 0.013) among sonology centers.
For the central reading, the frequency of CCSVI in the three groups overlapped with results of the primary analysis, with no differences among the three groups (MS versus HC: OR = 1.02, 95% CI = 0.53–1.98, p = 0.99; OND versus HC: OR = 0.83, 95% CI = 0.31–2.23, p = 0.31; MS versus OND: OR = 1.24, 0.52–2.96, p = 0.84), separately.
The CCSVI risk factor analysis, by univariate and multivariate regression, is summarized in Table 3. We grouped sonologic centers according to geographical region, in order to obtain a sufficient number of cases in each group to be included in the multivariate model. Following univariate analysis, factors significantly associated with CCSVI were: geographical region (p = 0.013) and the ultrasound machine used for the CCD exam (p = 0.011). Multivariate analysis revealed that the only factor associated with CCSVI prevalence was the geographical region (p < 0.001). For further details on frequency of CCSVI in the three populations for each of the different regions, see supplemental Table A2 (Appendix).
CCSVI risk factors.
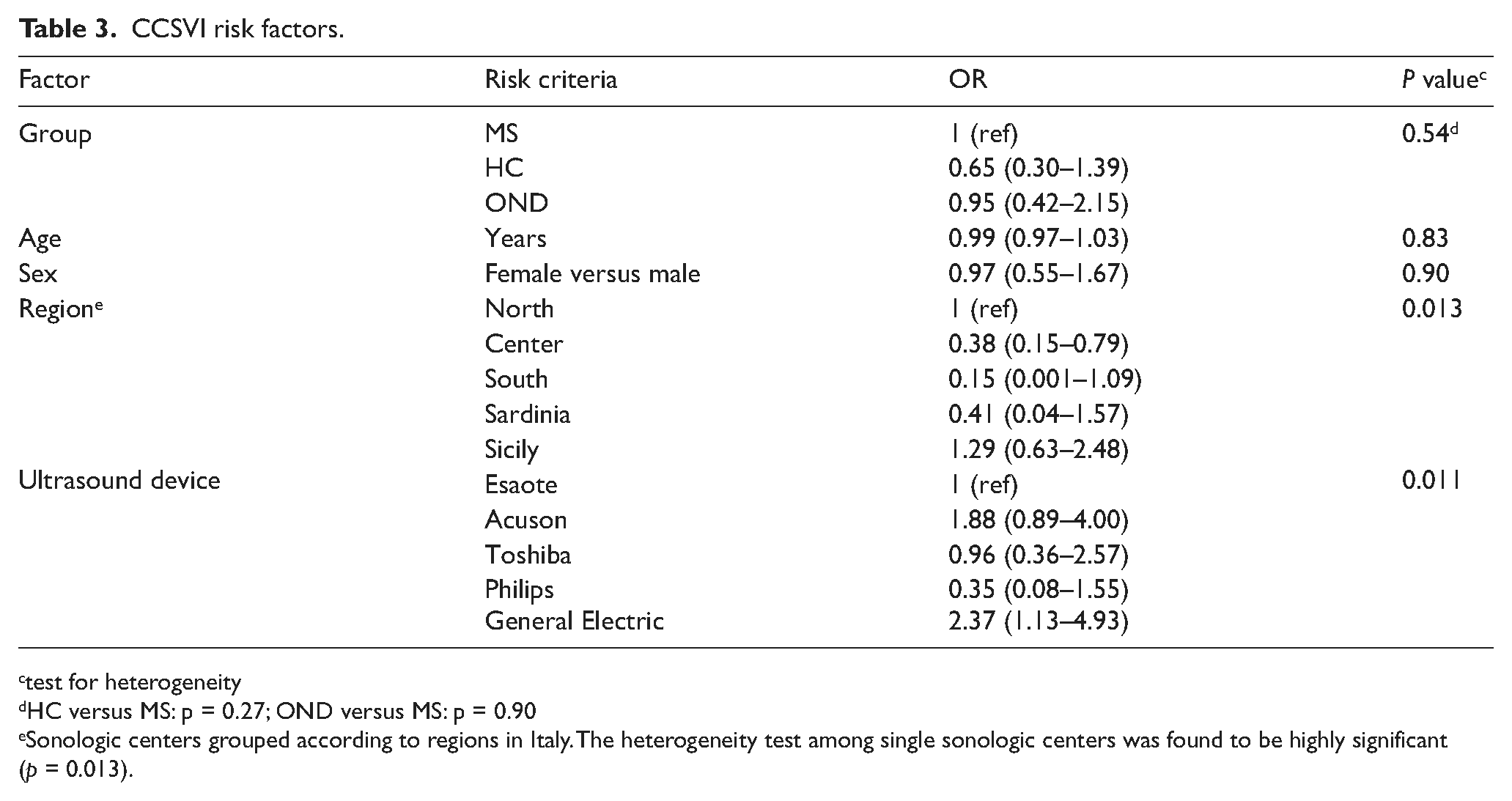
test for heterogeneity
HC versus MS: p = 0.27; OND versus MS: p = 0.90
Sonologic centers grouped according to regions in Italy. The heterogeneity test among single sonologic centers was found to be highly significant (p = 0.013).
Agreement between the local sonologists’ CCSVI diagnosis and the central expert reader diagnosis was very low. Table 4 displays the frequency of agreement in the positive and negative diagnosis between local and central readers. Kappa statistics test was 13% (standard error = 3%). The negative agreement was 92% and the positive agreement was 18%.
Agreement on CCSVI diagnosis between local and central readers.
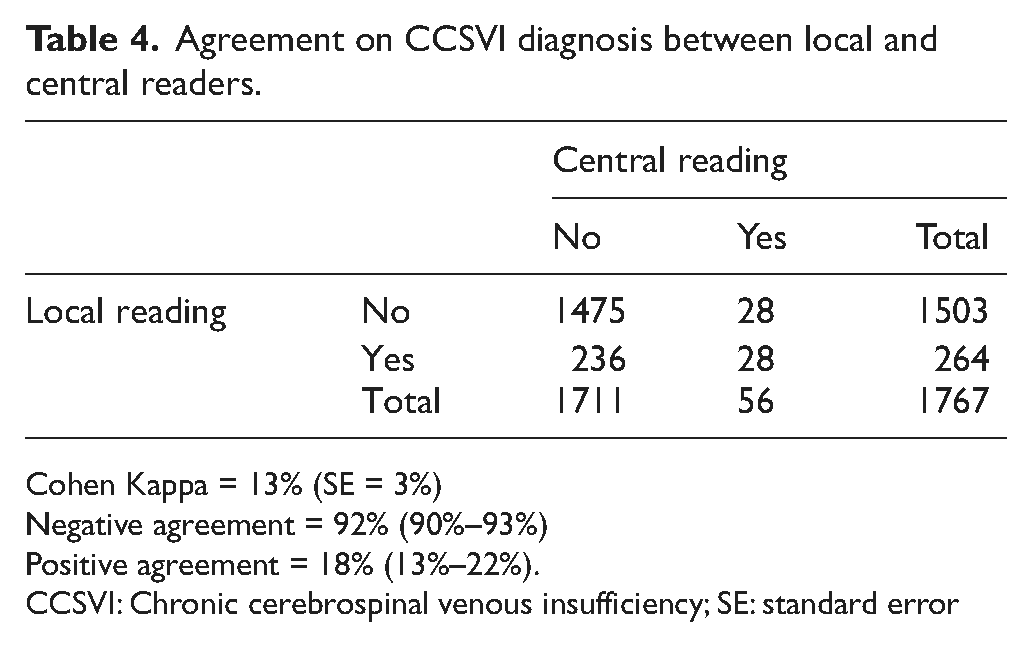
Cohen Kappa = 13% (SE = 3%)
Negative agreement = 92% (90%–93%)
Positive agreement = 18% (13%–22%).
CCSVI: Chronic cerebrospinal venous insufficiency; SE: standard error
Among the 28 subjects where agreement in CCSVI-positive diagnosis ocurred, single Zamboni’s criteria agreement between local and central reading was also variable. Approximately one-half of subjects were diagnosed positive for CCSVI according to the same two criteria, predominantly criteria number one and number three. The rest disagreed on criterion number one.
Discussion
Results from the CoSMo study indicate that the prevalence of CCSVI in patients with MS and ONDs is extremely low (2–3%), and not significantly different among MS patients, OND patients or HCs. A higher frequency of CCSVI in progressive MS compared to RRMS was previously reported, 11 whereas no differences related to disease course emerged in this study, and there was no correlation between CCSVI and disability. These findings do not support an association between MS and CCSVI.
Since Zamboni et al. first reported a high prevalence and strong association between CCSVI and MS, 4,19 other groups tried to replicate these findings, with varying degrees of success. Whilst some investigators claim to confirm Zamboni’s findings, 1,10,12,14,18 other groups did not report any abnormality in the cerebrospinal venous outflow in MS patients, providing compelling evidence against a significant contribution of CCSVI in the pathogenesis of MS disease (Table 1). 2,3,5,7,8,16,17 Although two independent systematic reviews point towards a possible association between CCSVI and MS, definitive conclusions could not be made, owing to the substantial variation in the strength of the association, lack of blinding and heterogeneity between studies. 20,25 Previous studies about CCSVI have limitations, such as: lack of an adequate number of controls, monocentric design and incorrect/absent blinding (Table 1). To address these, we adopted a stringent methodology in the design of the CoSMo study, whereby blinding procedures were adopted by local and central readers, a multicentric design was used and the study included a large sample size, appropriate controls and healthy individuals.
In our study, the difference in the prevalence of CCSVI between the participating centers was high, with centers having a prevalence of CCSVI of around 50–60% of examined cases and centers with a prevalence of approximately zero. This variability can be explained by the individual propensity of the local examiner to “see” the ultrasound abnormalities; however, because of the blindedness, this propensity produces the same effects across the three groups. Indeed, in centers with very high levels of CCSVI positivity, “the believers”, there never was a difference in CCSVI prevalence among the three groups. Other factors may have contributed to the inter-center variability of results, including examiner expertise and type of instrument used. The multicentric design and large sample size of the CoSMo study partially controlled for instrument variation at the local level, whereas complete blinding of the central reader further controlled for inter-user variability and subjectivity at the local level.
While recruitment of unimpaired or minimally-impaired patients may account, to some extent, for the differences observed between CoSMo and other studies, methodological limitations are the most plausible and robust explanation for the almost unprecedented degree of discrepancy that characterizes the literature on CCSVI. The maintenance of a local and central blinded analysis is a significant improvement over previous studies, where often the real blindness of the sonologist was uncertain. Ultrasound investigation of veins is susceptible to rater bias, because of the unfavorable signal-to-noise ratio of the vein signals. Moreover, many factors influence the results of the ultrasound examination of neck veins, including hydration status and level of compression by the ultrasound transducer. 32 Therefore, blinding of the rater is fundamental. Some involuntary unblinding may have occurred in the local analysis, because the examiner may have perceived some level of disability in patients with MS or ONDs; on the contrary, the central reader was completely blind. The results of the central readings show almost identical prevalence in HCs and MS (3.19% versus 3.26%). Interestingly, local readings show almost identical prevalence in the MS and OND groups (15.8% versus 15.0%, respectively), with a trend toward lower prevalence in HCs (11.9%).
While there was good agreement between the local and central examiners with regard to the absence of CCSVI, there was, on the contrary, poor agreement in the positive diagnosis of CCSVI. It is likely that this problem is related to the already discussed problems of the CCD examination; however, the intrinsic characteristics of the criteria proposed by Zamboni for the diagnosis of CCSVI may represent another factor accounting for the variability of these results. Most of these criteria have been criticized both for conceptual and technical reasons. 9,32 The absence of an abnormality is easily recognized, but the presence of a change is not uniformly evaluated by ultrasound readers. In this context, it is worth noting that results variability in the literature, but also within a single multicentric study, and the very low presence of CCSVI when confounders are controlled through central reading, pose the basic question of whether CCSVI does exist as a syndrome, 33 i.e. an association of clinically-recognizable features that, together, are linked to a disease state. At present, the answer is no.
Conclusions
Findings from the CoSMo study do not support the role of CCSVI as a recognizable clinical condition that is causally related to the development or progression of MS. The prevalence of CCSVI, detected in a multicentric setting by a shared local and central assessment, was very low and was not significantly associated with MS. Based on the lack of evidence of CCSVI in MS that emerged from this CoSMo study, we do not recommend vascular intervention in MS patients.
Footnotes
Declaration of conflicting interests
GC received consulting fees for participating on advisory boards from Novartis, TEVA, Sanofi-Aventis, Merck-Serono and Bayer-Schering; lecture fees from Novartis, TEVA, Sanofi-Aventis, Merck-Serono, Biogen-Dompè, Bayer-Schering and Serono Symposia International Foundation. He is a member of the Board of the Italian MS Foundation.
LT and MAB are members of the Board of the Italian MS Foundation.
AB has been on steering committees in clinical trials sponsored by Biogen-Idec and Roche; has received speaker’s honoraria from Biogen-Idec, Merck-Serono, TEVA, Bayer-Schering, Sanofi-Aventis and Novartis; has received research support from Biogen-Idec, Bayer-Schering, Merck-Serono, Sanofi-Aventis, the Italian Multiple Sclerosis Society and the European Union Sixth Framework Program.
GM, PZ, ES and MDS report no disclosures.
AG received speaker’s honoraria from Bayer-Schering, Biogen-Dompè, Merck-Serono, Novartis, Sanofi-Aventis and Allergan; payment for consulting from Actelion, Merck-Serono, TEVA and Novartis; support for participating in National and International Congresses from Bayer-Schering, Biogen-Dompè, Merck-Serono, Novartis and Sanofi-Aventis.
MS receives grant support from Bayer-Schering, Merck-Serono, Sanofi-Aventis and Biogen-Idec.
MPS received consulting fees or honoraria from Biogen-Idec, Merck-Serono, Actelion, Synthon and TEVA.
GLM received honoraria for lecturing; travel expenses for attending meetings and financial support for research from Bayer-Schering, Biogen-Idec, Sanofi-Aventis, Novartis and Merck-Serono. He is a member of the Board of the Italian MS Foundation.
Funding
This work was funded by the Italian Multiple Sclerosis Foundation.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.