
Abstract
This study investigates how organisational professional boundary drawing affects the ability of Māori home-based carers (HBCs) in Aotearoa New Zealand to provide culturally grounded care. As in many caring professions, this home-based sector relies on the fulfilment that caring is assumed to bring to workers in order to attract and retain good staff. Such meaningfulness is tied to the close relationships and rapport needed to undertake intimate cares. Paradoxically, these relationships are discouraged through organisational and professional boundary drawing that is designed to maintain distance between care workers and their clients. Through a community-based participatory research (CBPR) methodology, it was found that Māori HBCs experienced significant tensions when navigating the drawing of professional boundaries. These boundaries, while deemed necessary for legal, client and worker safety, are underpinned by Western cultural values and social norms, legitimised in Western models of care. These can conflict with Māori ethics of care, which emphasise relationality and belonging through whānau (extended family) roles and responsibilities. These insights call for a re-evaluation of professional boundary drawing to better align with culturally grounded care models, advocating for policies that support the integration of tikanga Māori in home-based care.
Keywords
Introduction
Home-based care is a rapidly growing aspect of the wider healthcare sector as governments move focus and resources from hospital-based care to community-based care. This transition supports those who require care to remain in their homes and communities and maintain their independence, but it also reshapes how care responsibilities are structured, blurring the line between public and private care systems (Ravenswood et al., 2022). Despite its importance globally to health systems, home-based care work is not considered by the general public as a healthcare profession. It is typically characterised by poor work and pay conditions, and is highly feminised and ethnically diverse (England, 2010; Sims-Gould and Martin-Matthews, 2010). This workforce is largely viewed within society as low-skilled and providing low value care work that centres on household cleaning chores. These societal perceptions are underpinned by historical gender discrimination and the economic devaluation of interpersonal care (Ravenswood and Douglas, 2017). Yet, the importance of home-based care came to the fore during the Covid-19 pandemic, with accounts of missed care and inaccessible support, largely due to the lack of available home-based care workers and the way in which the work is organised (Baker & King, 2022).
This paper explores how the drawing of professional boundaries within the Aotearoa New Zealand (NZ) context of home-based care and support services reflects a Western perspective that often conflicts with Indigenous understandings of care. This issue emerged within a wider project that investigated the wellbeing challenges experienced by home-based care workers (HBCs) during Covid-19, which found that ongoing and systemic issues were intensified by the pandemic, placing more risk, workload and responsibility on workers, with little or no additional support or resources. For Māori, the Indigenous population of Aotearoa NZ, who are estimated to make up 11% of the HBC workforce (Ravenswood et al., 2022), we found that these issues were exacerbated through the additional systemic discrimination they faced, as well as cultural misalignment. However, the sparse research on home-based care workers in Aotearoa NZ generally has tended to subsume Māori cultural issues into the mainstream narrative of HBCs.
Our study found that Māori HBCs grapple with the tension between organisational expectations and cultural values through having to operate within Western frameworks of care and support that do not allow the expression of tikanga Māori (customary law, ethical relationality, practices) (Ravenswood et al., 2022). It emerged that the drawing of professional boundaries, particularly those that enforce emotional distance between care workers and clients as mandated by company policy, are not always in line with Māori ethics of care that emphasise relationality and interconnection. This led to the development of the research question: How do Māori home-based care workers in Aotearoa New Zealand experience and navigate the tensions between Western professional boundary drawing and tikanga Māori in their care practices?
Professional boundary drawing in home-based care work
The work of home-based care workers – also referred to as ‘health care assistant’, ‘home care’, ‘personal care assistant’ or ‘community support worker’ – is complex. A care worker may be required to perform technical and specialised medical tasks, intimate cares, support of medication needs alongside a wide range of other health-related activities, including end-of-life care. As such, home-based care work entails significant, yet largely invisible, emotional labour, relationship building and skill (Ravenswood et al., 2023; Tsui et al., 2019; Yakhlef and Essén, 2013). Paradoxically, however, the centrality of relationships and the emotional labour of the role is devalued by employers through professional boundary drawing that imposes expectations of professional distance.
The drawing of professional boundaries is deemed to be an important mechanism to safeguard workers, clients and organisations from serious harm from power imbalances, exploitation or discrimination (O'Leary et al., 2013). These boundaries aim to separate and define the relationship between the professional practitioner and client, determining what behaviours and emotional attachments are acceptable and therefore ensuring that power is not abused (Abrams et al., 2019). Professional boundary drawing imposes a level of distance between the two parties and discourages familial, friendly or emotional attachments. The tensions involved in establishing and maintaining acceptable boundaries in care work, specifically healthcare settings, are a significant focus of clinical training.
The drawing of professional boundaries and the inherent professional distance assumed highlight a reductionist view of physical care as a structured, transactional activity with clearly defined tasks, rigid schedules and organisational forms of control. This detaches care from meaningful relationships, limiting personal, social and cultural ethics of care, which are sometimes in conflict with the values of the care worker and client (Curtis and Hodge, 1994; Sims-Gould and Martin-Matthews, 2010; Woods et al., 2017; Yakhlef and Essén, 2013). Separating the professional worker from the client presumes that rational objectivity and a neat homogenous delineation of roles is both essential and beneficial to both parties (Abrams et al., 2019; O'Leary et al., 2013). Additionally, separating tasks and relational ethics that are perceived to be legitimate for a ‘professional’ to perform brings forth a space from which relational work can be judged as over-involvement or ‘non work’ (Cataldi and Tomatis, 2024; Chiarella and Adrian, 2014). These professional boundaries sit within a system of commodified care where business rationalities and corporate logic are imposed onto care services (Farris and Marchetti, 2017; Macdonald, 2021).
As scholarly work has established, the professional boundary drawing imposed on non-professional care work by employers and service providers is heavily influenced by entrenched social norms that assume care work is an extension of domestic familial roles of ‘woman’s work’ (England and Alcorn, 2018; Hartmann and Hayes, 2017). Such gendered stereotypes reinforce care labour as an innate quality of women, therefore not ‘real work’ nor a skill (Dodson and Zincavage, 2007). In practice, funding models of home-based care define care tasks as discrete physical tasks within set, limited blocks of time (Macdonald, 2021), which perpetuates the gendered norms that non-professional care work involves lower skill levels and less ability to make judgements on the care needs of clients (Ravenswood and Harris, 2016). That is to say, whilst women are designed to care, they are not thought to be (or trusted to be) emotionally resilient or regulated enough to manage attachment to those they care for (Cataldi and Tomatis, 2024; Oerton, 2004). Consequently, because the drawing of professional boundaries is based on gendered assumptions of care work, when a care assistant cares ‘too much’ for a client, this is seen as crossing the client-private-professional boundaries, which is considered by employers and healthcare providers as a serious error of judgement. Furthermore, establishing familial bonds is similarly taboo, and genealogical links between client and worker is labelled a conflict of interest. In other words, the commodification of caring in Western models of funding and work, in the form of outsourced physical healthcare tasks, defines the emotional bonds inherent in familial caring as incompatible with professional behavioural expectations (Tsui et al., 2019).
Culturally specific boundaries
Professional boundary drawing of ‘appropriate’ care is culturally and contextually specific. The privileging of autonomous and independent notions of health and wellbeing are argued to be culturally relevant to Western values (Christopher, 1999; Durie, 1985). In the context of social work, codes of ethics developed in Anglo-Western countries reflect the strong emphasis of individual rights and a highly professionalised workforce, which distinguishes them from non-professionals. Whereas in societies, such as Maori, with more collectivist values and interdependent notions of health and wellbeing, ethical considerations of conflicts of interest, dual relationships and the role of whānau (extended family) differ from the Anglo-Western norm (Congress and McAuliffe, 2006; Eketone, 2021). Yet, the universal drawing of professional boundaries within the Aotearoa NZ care sector prescribe what care is appropriate for all cultural groups to provide within Anglo-Western norms of care, expertise and value.
Culturally grounded care within te ao Māori (a Māori worldview) is holistic, underpinned by collective and interdependent principles. Māori models of health and wellbeing locate the individual within a broader context of spiritual, environmental, social, cultural and economic forces. When one dimension is not cared for, it risks the entire system, just as caring only for the physical body does not allow care for the whole individual (Spiller et al., 2011a; Wilson, 2008). In Durie’s (1985) renowned Te Whare Tapa Whā model, it is the wairua (spirit), hinengaro (mind), tinana (physical body) alongside the whānau (extended family) that denote the four cornerstones of hauora – Māori health and wellbeing. To provide care is to recognise and empower the mana (spiritual power, authority, and sovereignty) in others (Dell et al., 2018; Spiller et al., 2011b). In contrast to Western professionalism, the mana of the care recipient is intertwined with the mana of the care giver.
In this te ao Māori framing, social relationships are not external factors to wellbeing, instead they are part of one’s constitution (Durie, 1985; Yap and Yu, 2016). Relationships are characterised by the roles and responsibilities undertaken between people. Whānau, which denotes the extended family, have an active and significant role in Māori development; they are recognised and obliged to provide reciprocal spiritual and emotional support, and share the responsibility of care for each other (Nicholson et al., 2012). The term whānau can stretch beyond genealogical lines and apply to those who fulfil whānau roles and responsibilities (Nicholson et al., 2025). Whanaungatanga is the social process of establishing these whānau relationships and is one of the first rituals observed when Māori meet, providing a foundation for interactions (Brannelly et al., 2013; Durie, 1985; Nicholson et al., 2012). Whanaungatanga looks to create connections and belongingness rather than distance. Whereas familial or friendly care relationships are associated with a lack of judgement in Western care models, in te ao Māori, relationships are fundamental and in themselves create the boundaries of safe spaces. As we found, tensions and conflicts often arise when Māori HBCs wish to provide culturally appropriate forms of care whilst also adhering to the boundaries drawn by their employers. These tensions can manifest as personal conflict or feelings of disempowerment, as workers are forced to choose between suppressing culturally grounded expressions of care to comply with policies, or act in ways that align to their notions of holistic care that knowingly infringe on such policies and risk disciplinary action. Ultimately, this marginalises Māori approaches to care and reinforces the systemic inequalities embedded within Western care system.
Methodology
This research was conducted in home-based care work in Aotearoa NZ. The approach to this work in Aotearoa NZ is similar to the international context: while it is government-funded, it is outsourced to mainly private agencies (70%) and a few non-profit agencies (HCHA, 2020). Aotearoa NZ’s funding system follows a marketised and commodified care model (Farris and Marchetti, 2017; Macdonald, 2021), with clients’ care needs largely focusing on physical care rather than relational or social needs. Additionally, care needs are funded by counting discrete blocks of time for each type of care. This workforce suffers from invisibility within society (Ravenswood et al., 2023) and thus there is limited demographic data about home-based carers. However, approximately 16,000 care workers provide services to over 100,000 New Zealanders annually (HCHA, 2020). It is estimated that 93% of the workforce are women, 82% of NZ European descent and 55% are over 55 years of age. Approximately 11% of this workforce are Māori (Ravenswood et al., 2022).
A community-based participatory research (CBPR; Nicolaidis et al., 2015) methodology was adopted and positioned the research community as equal partners in the project. The two partner union organisations, E tū and Public Service Association Te Pūkenga Here Tikanga Mahi (PSA) unions, represent the largest proportion of community home-based care workers in Aotearoa NZ. The partner organisations collaborated on the research design, from the concept through to data collection, analysis and knowledge dissemination, including the activist-style presentation of the findings to the New Zealand government’s Health Select Committee and the Minister of Health. Built on existing research partnerships, this process spanned approximately 2 years with data collection (including participant researcher training) taking place over 9 months in 2021 when Aotearoa NZ was still under Covid-19 restrictions.
Māori-centred stream
The wider research project included a separate stream of Māori participants, and findings from this stream form the basis of this article. Led by a Māori researcher, experienced in kaupapa Māori research (a Māori research paradigm; see Henry and Pene, 2001)) and Māori-centred research, this stream privileged mātauranga Māori (Māori knowledge and experience) and ensured that the research process aligned with tikanga Māori (Māori customary practices or behaviours). In doing so, we adhered to the ethical obligations and responsibilities to the research community as outlined by Hudson et al. (2010): Māori participation is significant, including senior members of the research team; Māori knowledge is generated that has particular relevance to the Māori community; and cultural safety is recognised through the inclusion of Māori values and protocols. In centring both the community concerns and the systems of power within play, CBPR aligns well with Māori-centred research (Kerr et al., 2010). A key element of the research project was to bring attention to the inequity for Māori as there has been little or no focus on Māori home-based carers, leaving these workers with a lack of voice and visibility. Our project aimed to provide a platform for Māori home-based carers to voice their own concerns and meaningfully engage with the development of their own solutions.
Participant Researchers (PRs) were a key part of the research design, involved in the data collection and analysis. We wanted to ensure that those on the front lines were actively involved with the data, as well as recognising that participant researchers may have greater access to HBCs and have experiential knowledge that could elicit more in-depth information. The two Māori PRs were interviewed and trained by the research team to conduct interviews and were given the opportunity to carry out as few or as many interviews as they preferred. They were compensated at either their hourly rate or the New Zealand living wage, whichever was higher. Partnership also extended to publication, with the project report and initial publications appearing with participant researchers (anonymised) as co-authors.
The research process was aligned to kaupapa Māori guidelines, such as opening and closing karakia (incantations to bring focus and to create safe spaces), mihi (greetings and acknowledgements according to Māori custom), kai (food, shared to acknowledge the collaboration of both parties), koha (gifting to honour the contribution of the participant) and the use of te reo Māori (Māori language). The utilisation of such tikanga allow for the validity and legitimacy of a Māori way of being, adhering to social and cultural norms of te ao Māori. They serve as a pathway to acknowledge ancestors and whānau of participants and researchers, and to clear a space for each party to fully engage in the process.
Access into Māori research communities often rests on whether the community believes the researcher has the cultural knowledge to interact, interpret and validate the experiences of participants in the research context (Bishop, 2008). Therefore, it was essential to ensure that we had the right expertise and support within the research team. Recruitment through the union networks identified participant researchers and participants who self-identified as Māori. One of our PRs, fluent in te reo Māori, conducted bilingual interviews. Consent forms, Participant Information Sheets and sections of the final report (executive summary, introduction, Māori community support worker wellbeing, conclusion and recommendations) were translated into te reo Māori.
Recruitment, ethics and sample
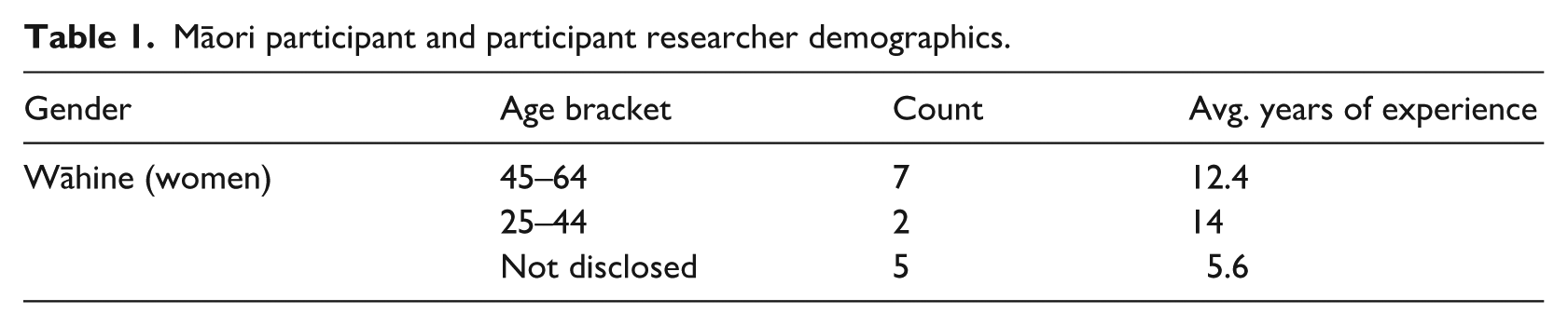
In this stream, purposive and snowball sampling generated 14 interviews with wāhine Māori (Māori women) comprising two participant researchers (PRs) and 12 participants. All were recruited through partner organisation networks and interviewed using an in-depth semi-structured approach. Of those who shared their age, only two were aged 44 and under, the rest aged between 45 and 64. Eight of the participants were employed by for-profit providers, and six were employed by not-for-profit organisations. No Māori participants worked for Māori health providers, which may be due to a lack of Māori HBC union members and/or a lack of Māori HBCs within the organisations affiliated with the union partners. Table 1 below presents the Māori participant demographics:
Māori participant and participant researcher demographics.
Complete ethical approval was obtained for the project, which included standard provisions of informed consent and confidentiality. In consultation with the partner organisations, counselling services were made available for all participants, as well as debriefing processes for PRs and university researchers. Checks were in place to ensure that PRs and their matched participants were comfortable with each other and were not in any conflicting reporting lines. All PRs undertook training on interviewing and research ethics prior to conducting any interviews. Two Māori participant researchers were involved in interviewing others. In-person interviews were carried out where possible; however, with the changing pandemic situation and rural locations of some participants, most interviews were carried out via Zoom and phone calls.
Analytical strategy
The wider project employed a staged thematic analytical strategy (outlined in Figure 1) that aligned with the CBPR process (Hennink et al., 2017) involving participants, participant researchers and research partners. A reflexive thematic analysis was the key analytical process used (Braun et al., 2019). This iterative process involved the development of initial codes by the research team, which were built to themes through a continuous movement between data and codes. The process required critical reflection on the meaning of said codes and themes in relation to the phenomena studied, and its situation within society (Braun et al., 2019).

Staged thematic process.
In alignment with both the aims of CBPR and kaupapa Māori methodology to centre and empower participants, analysis really began during interviews, with participants and participant researchers responding to questions and engaging in the broader meaning of their experiences. Indeed, interviews held by participant researchers were led by participant voice. Thus, the issue of Western professional boundaries began to surface during data collection as participants spoke to the themes of wellbeing, tikanga Māori and the tensions participants faced working in Western organisations. Furthermore, during the data collection process the research team held discussions with participant researchers to discuss or debrief their experiences interviewing. These conversations, along with a town hall style presentation of early themes to participant researchers and a Māori rūnanga (council) of one of the unions surfaced the daily lived experiences of participants in relation to the data and preliminary findings. Key to this for Māori participants, was the limits imposed on their wellbeing and cultural safety by organisational professional boundary drawing in Western-based healthcare. Consequently, we interrogated the data led by these insights to understand how Māori home-based care workers in Aotearoa NZ experience and navigate the tensions between Western professional boundary drawing and tikanga Māori in their care practices.
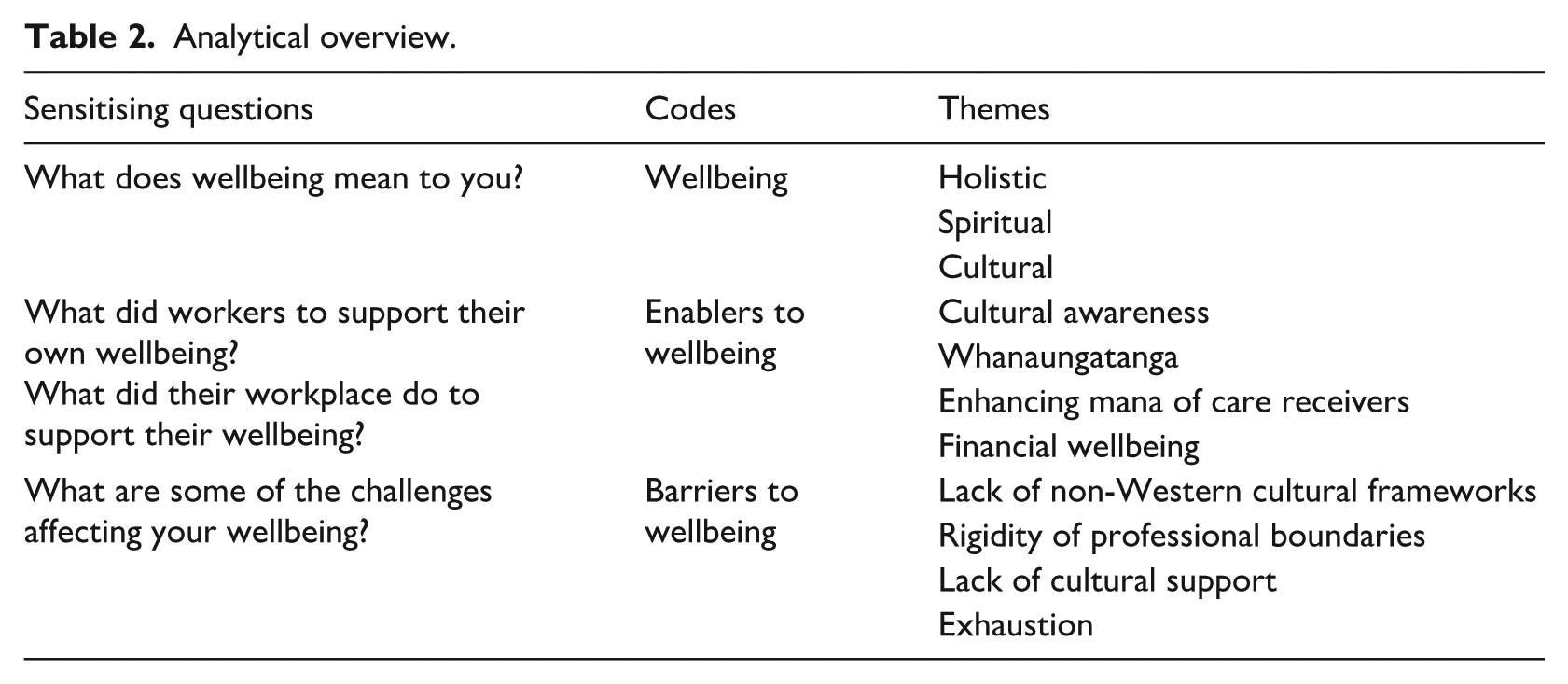
Table 2 below summarises the sensitising questions used to guide initial analysis, along with the emerging codes and themes across the wider project. It illustrates how the theme of professional boundaries emerged from the wellbeing themes specific to the Māori participants. In particular, it suggests that cultural awareness and cultural frameworks (that deviate from the dominant norm) are integral to wellbeing. It suggests that professional boundary drawing, when shaped by a lack of cultural awareness, can act as key barriers to wellbeing and in providing culturally grounded care.
Analytical overview.
Findings
In this section, we present how Māori participants experienced, set and navigated professional boundaries in the course of their everyday work. We begin by outlining one of the key themes that were integral to the wellbeing of all participants in our wider study, that of meaningfulness. For many HBCs, providing support and forming connections with those they care for was not only a core aspect of their role but also a source of personal fulfilment. This meaningfulness was a reason they go to work each day as they found purpose in their role of caring for and being of service to others. This is important to highlight, as it reflects the values that underpin both the individual and collective ethic of care.
I love going and meeting new people and I love meeting kaumātua [elders] for sure. They’re just such a blessing to have in our lives and it’s a real special gift [to] have that time with them. There’s a lot of conversations that we can have with them while doing mundane tasks. Yeah, and I have been really blessed with who I have met. So that is what makes me love my job (P7, wahine Māori [Māori woman])
Furthermore, our Māori participants spoke about how their connection to their Māori culture is integral to their wellbeing and their role as home-based care workers. Cultural identity and values are seen as strengths in caring practices. One HBC expressed that ‘sometimes being Māori, we have sort of inner strength’ (P48, wahine Māori), especially when specialising in end-of-life care. Others expressed how their cultural background supported them in being able to provide care for others.
I like to believe that our inherent values and tikanga and way of doing things that subconscious looks after many Māori without them even knowing it. (P74, wahine Māori)
Empowering the people they care for and ‘lifting their mana’ (P7, wahine Māori) through tikanga Māori were fundamental to their own ethic of care.
The emergent paradox was that the elements that contribute most significantly to the wellbeing of Māori HBCs – tikanga Māori and meaningfulness – are actively discouraged and unsupported within Western models of care and support. This misalignment creates equity issues and professional tensions for Māori working within these systems. In the sections that follow, we examine how Māori HBC workers express tikanga, particularly through whanaungatanga (the social process of establishing relationships) and manaakitanga (care and hospitality), in order to provide what is considered culturally grounded care from a Māori perspective. Following each theme, we present participants’ experiences of the incongruence between these cultural expressions and the professional boundary drawing imposed by their employer organisations, namely, the enforced separation of self from others, and lack of organisational support.
Expression of Tikanga: Whanaungatanga
Whanaungatanga or the intentional establishment of meaningful relationships was seen as a fundamental part of the caring process due to the intimate nature of the work and the need to respect the mana of the people receiving care. Māori HBCs saw these as whānau relationships.
That word ‘client’ is a dirty word to me. . . Because that makes me feel like they are a number. They are just another person that you need to—I don’t know, it’s hard to put it into words. Once you’ve been on with someone for a certain amount of time, they become your whānau. (PR15, wahine Māori)
Whānau, in this sense, indicates the associated roles and responsibilities of the extended family. Participants described the ‘whānau’ level of caring, that is to care for someone as if they were your own, was what made a good care worker; another spoke about how they were given keys to the home because ‘they’re vulnerable and they’re counting 100% on you and the family do too’ (PR6, wahine Māori). In this context, it provides a different structure for how care is conceptualised and empowers both the client and worker to determine the nature of their relationship.
Some spoke of attending whānau rituals (such as birthday celebrations or attending funerals), and another was asked to undertake cultural protocols usually reserved for whānau.
I’ve been to all their funerals we’re invited to and then to do the karanga [ceremonial call] and all that. (PR6, wahine Māori)
These HBCs saw these relationships as positive for all involved. When questioned about the alignment of whanaungatanga and the organisational drawing of professional boundaries, a tension was noted: If you’re treating people like you’re treating your own whānau, then that boundary isn’t even there to start with. And that only becomes a boundary when somebody with a different worldview comes along and tells you it’s one. . . And then for Maori, that’s when they struggle in their workplaces because they actually haven’t done anything wrong. (P74, wahine Māori)
Māori HBCs were all very aware of the cultural constraints of their roles. They felt that to provide meaningful care went beyond the confines of impersonal relationships. A lack of cultural awareness and support from their employers impacted their role and wellbeing, as well as the wellbeing of their clients.
Professional boundary drawing: Separating self from others
In contrast to the ethic of whanaungatanga, professional boundary drawing prescribes a separation between client and worker. This deliberate discouragement of personal relationships was one of the major challenges faced by Māori HBCs. Some spoke of the expectation to depersonalise themselves, not share information or foster a caring relationship with their client. This was difficult because sharing information is the foundation of interpersonal relationships. This was particularly so in the case of long-term care relationships.
We’re not even meant to interact with our clients outside of the care plan. So, if you go and see someone once a week for housework, but you know that they are particularly lonely, you can’t become friends with them and go and have a coffee with them at another time. Yeah, it’s very, very structured. This is what you were paid to do; this as your job. We’re not meant to. We’re told on day one not to form relationships with our clients, which I think is completely barbaric. They push the professionalism is what they call it, which I just think is heartless. And I refuse to be like that. (P76, wahine Māori)
The implication of such professional boundary drawing is that the personal values that impel someone to take on the role of a HBC, such as compassion and service, can be compartmentalised or minimised. When caring for someone’s physical body, it is assumed that workers can do so without recognising the spiritual or social being attached to the body, or without recognising the spiritual or social needs of the worker. Professional boundary drawing restricts the ability of Māori HBCs to provide what is considered to be appropriate holistic care. To do so requires constant negotiation between cultural values and professional boundaries, which was taxing on our participants.
Expression of Tikanga: Manaakitanga
Manaakitanga is the ethic and practice of nurturing, protecting and respecting the mana of others (K. I. N. Author Collective, 2021). For HBCs, this often meant going above and beyond the formal expectations of their role. Many participants spoke of engaging in unpaid acts of care that extend beyond their job descriptions, often crossing professional boundaries set by employers in order to uphold their internalised values of care. These acts also contributed to the emotional overload and stress felt by HBCs.
We’re only supposed to do what’s on the care plan but we go over and beyond because no one else is there with them. Family is not around. . . And you know the clients—they are crying—they’ve got tears. . . (PR6, wahine Māori)
This was especially so during the Covid-19 pandemic as the government-mandated lockdowns and social distancing restrictions placed extra burden on HBCs as they felt they were unable to provide care and support to a level that some of their more vulnerable clients needed.
So that’s why I did the seven days was just to help them and I knew work were also struggling to cover people. And I didn’t want any of my people missed out. (P76, wahine Māori)
However, most choose to hide the extra work they do and the relationships they have, lest they are reprimanded, because they are acutely aware that their actions do not align with company professional boundary drawing. For some, they say the boundaries are more tightly held at the higher levels of management: They push the professionalism is what they call it, which I just think is heartless. And I refuse to be like that. So, I sort of—the coordinators in the office have come to know me, and they know that I don’t really follow the rules too well, but they know that what needs to be done will be done. So they sort of turn a wee bit of a blind eye, but I know if it got further up the line in the ways of management, there would be words had, I would imagine, because they’re very, very red tape and you know, they’re running a business and that’s kind of what it comes down to. (P76, wahine Māori)
The sentiment conveyed in this quote depicts the way in which HBCs are often infantilised through company policy, not trusted to regulate their own behaviours and yet are knowingly allowed to continue with their care practices. This indicates an organisational culture that does not align with the policy of professional distance, as well as a vast detachment between HBCs everyday reality and management policy setting.
Participants did acknowledge the reason that professional boundaries were in place, with some having experienced uncomfortable or unsafe interactions. However, it was also apparent that rather than these boundaries being monitored and maintained, it was the HBC who determined when these boundaries were crossed and how to deal with it. The organisation stepped in only when called to. In these instances, the HBCs are trusted to maintain boundaries and provide solutions. However, when it comes to creating personal relationships, HBCs are seen as unable to balance this tension. In all of these accounts, the long-term nature of the caring duties, the private spaces in which the care occurs, and the subsequent personal relationships formed problematised the notion of clear care boundaries.
Professional boundary drawing: Separating emotion from care
Participants expressed that the emotional burden of caring was, at times, overwhelming, even when maintaining professional distance. While supporting others was rewarding, some clients could be challenging to work with, physically and mentally. Additionally, many HBCs discussed the heaviness associated with clients who passed whilst in their care. The emotional burden went largely unnoticed by employers due to the expectations of impersonal care. This meant that there was little support for HBC workers from their employers in managing the emotional labour. Many workers did not have an accessible manager with whom to discuss their wellbeing: Now, we talk to a faceless person. Sometimes you can talk to dare I say it, to an idiot black phone. The idiot box I call it. (P54, wahine Māori)
Although some organisations are paid members of the nationwide Employment Assistance Programme (EAP), emotional support was not seen as an integrated and embedded part of the organisation. Those that did receive support was due to the relationship between worker and individual manager, rather than an organisational structure. This lack of positive work relationships and denial of personal attachment through the imposition of professional boundaries made it difficult to deal with stress and issues such as grief that are part and parcel of this work. One HBC talked about the ‘Eurocentric view’ of the company in how they supported the ‘wellbeing of the client, but not so much the support workers’ (P7, wahine Māori).
Discussion
Home-based care work is an occupation that, due to the intimate nature of some tasks and the invitation to enter one’s home, is premised on relationships with and between individuals. Our findings echo others (Abrams et al., 2019; Mears, 2009; Sims-Gould and Martin-Matthews, 2010) who have found that the personal relationships experienced by care workers and the meaningful contribution to their lives was what instilled a sense of pride in their job and contributed to holistic wellbeing. Many care workers go beyond employer policies to provide valued care for their clients. Like many caring occupations, the home care industry relies on the fulfilment that caring brings to its workers in order to recruit and retain its workforce (England, 2010).
However, these meaningful relationships do not align with professional boundaries, as unilaterally defined by employers, and are often discouraged and unsupported. As invited guests into other people’s private sanctuaries, HBCs must adhere to the social and cultural expectations of their clients and families, as well as their lifestyle choices. Additionally, these workers may seldom see other colleagues or supervisors and, therefore, rely heavily on their own expertise and abilities to keep them safe. The complexity of home-based care work requires HBCs to navigate role ambiguity through flexibility, adaptability and improvisation (Yakhlef and Essén, 2013), alongside subtle self-reflexive practices (Mumford et al., 2022). Despite this high level of autonomy, neither HBCS nor their clients have a role in the setting of organisational professional boundaries. The employers, having established policies for professional boundaries, seemingly absolve themselves of responsibility for emotional bonds. It then becomes a burden that the care workers must manage themselves (Mears, 2009; Tsui et al., 2019). Indeed, whilst HBCs are asked to provide intimate care that usually resides within the familial domain, they are also dissuaded from mourning those they care for and given little support if they choose to. Findings show this can lead to burnout and exhaustion of care workers (Dodson and Zincavage, 2007; O'Leary et al., 2013; Ravenswood et al., 2022).
Whilst acknowledging the need to maintain safety, it is argued that in many cases, the drawing of boundaries is a social construction designed to maintain the appearance of professionalism and, therefore, legitimacy. In this sense, this boundary drawing can be seen to be ‘based in part on the necessity of being seen to be professional as opposed to simply being professional’ (Oerton, 2004: 545). The focus on personal responsibility of both the rational consumer to choose their carer, and the care provider who must abide by a set of professional boundaries, puts the blame for any transgressions onto the individual care worker, ignoring any existing inequalities in the system (Brannelly et al., 2013; Wilson, 2008; Woods et al., 2017). This does not mean that transgressions of trust and abuses of power are not harmful, nor does it ignore the exploitation of this workforce who are already overworked and underappreciated. However, it does highlight the need to redesign the boundary lines between HBCs and the people they care for in order to recognise that these emotional and social relationships do exist, regardless of company policy.
Our study has highlighted that Māori understandings of care work, based on interconnection and relationality, sit in stark contrast to care work boundaries that have been shaped by Western and commodified models of care. In Māori models of care, wellbeing is located within a web of relationships between spirit, ecosystems, as well as socio-cultural and economic environments. Centring relationships, and in particular whānau roles and responsibilities, is fundamental to care work. These connections invoke a sense of reciprocity and trust, which is seen to enhance the mana of all parties (Brannelly et al., 2013). Some have recognised the theoretical kinship of a Māori view of health with Tronto’s (1998, 2013) ethic of care work that recognises the complexity of care and the importance of relationships, where care is deeply personal and relational, not objective and limited by externally imposed boundaries (Brannelly et al., 2013; Spiller et al., 2011a; Woods et al., 2017).
In highlighting such ethics of care, we join the call for the development of alternative and holistic understandings of professional boundary drawing within care work sectors, and specifically within home-based care and support. As our study highlights, the drawing of boundaries in practice reinforces false, Western ideals of distance: separating the employer from responsibility, separating emotional or kinship care from physical care, and excluding the bodies of knowledge and care held by Māori workers from ‘professionalism’. Instead, acknowledging whānau relationships, we argue, need not conflict with professionalism. In the field of Māori social work practice, Eketone (2021) notes that dual relationships or perceived conflicts of interest are more likely to breach organisational policies rather than any professional codes of ethics that focus on power imbalances. Indeed, previous care and support research tells us that when close familial relationships or friendships are formed between client and worker, power and status gaps are reduced, client satisfaction is increased, and workers feel valued (Dodson and Zincavage, 2007; Mears, 2009; Piercy, 2000). Furthermore, the notion of ‘kinning’ is a new research focus that describes the process of creating familial relationships between genealogically unrelated care givers and care receivers (Baldassar et al., 2017).
Following O’Leary et al. (2013), we ask for more attention to be given to the ‘why’ and ‘how’ boundaries are set rather than focusing on the standardised ‘what’. From a Māori viewpoint, this means looking at the kawa, the cardinal ethics that underlie the tikanga (Nicholson et al., 2012). The kawa is to manaaki – to nurture and protect others through enhancing the mana of others (K. I. N. Author Collective, 2021). It is our role to ask what tikanga can best express this ethic of care? One such example has been outlined by Eketone (2021), who has offered some guiding principles and processes that promote tikanga and whanaungatanga to navigate boundary crossing. The framework creates reciprocal obligations for both parties that can enhance the relationship, service and outcome. Further research into professional boundary drawing within home-based care work that involves all level of workers, as well as clients and their whānau, is needed to find relevant ways for organisations and industry to address this issue.
Continuing the status quo, as our research has outlined, leads to a misalignment between unacknowledged cultural frameworks and standardised organisational policies, which can impact the quality of experience for both HBCs and the people they care for. Healthcare that is not culturally appropriate or acceptable can lack relevance and compromise efficiency, access and use (Wilson, 2008). Discouraging relationality between those receiving and giving care, as professional boundary drawing does, was expressed to have a negative effect on the wellbeing of HBCs, leading many of them to ignore and subvert such rules in order to provide appropriate care. This supports the findings by Walker et al. (2016) of Māori nurses who are forced to disregard both personal cultural practices to meet the needs of tauiwi (those not of Māori descent) patients, as well as override ‘professional’ protocols in order to meet the needs of their Māori communities and patients.
There is an added danger that when outcomes are not achieved, the blame is placed on the non-compliance of the client or worker rather than the cultural deficits of the health service itself (Wilson, 2008). Our participants spoke about how their cultural background enhanced their ability to do their role, as well as the importance of respecting the culture of the client. However, they argue that the cultural element is also unsupported by employers. Research into Māori at work consistently talks to how Māori are required to ‘bridge two worlds’ (Wilson and Baker, 2012), laboured with a ‘cultural double shift’ (Haar and Martin, 2022) and bound by cultural responsibility (Staniland et al., 2021). These notions refer to the relentless work of defending and advocating for Māori tikanga, often with little success, whilst also being expected to provide advice and upskill tauiwi colleagues and superiors. This ‘cultural tax’ (Love and Hall, 2022) is often unrecognised, which creates stress and conflict, and can stifle careers.
Conclusion
HBCs are bound to standardised care models dictated by organisational policies and codes of conduct, yet the reality is that the majority of this workforce provides care independently, autonomously and invisibly. The drawing of professional boundaries applied to home-based care and support are not context- or place-specific, and instead are modelled on the boundaries set within clinical environments for professionalised occupations, such as nurses or doctors (Abrams et al., 2019). Establishing rapport through emotional and social relationships between carers and clients has a greater emphasis in this context. Additionally, the drawing of professional boundaries is based in dominant Western paradigms of care, which often leave little room for culturally diverse frameworks. The resulting cultural misalignment can constrain Māori carers’ ability to practice care in ways that reflect their relational values and responsibilities, which negatively affect their wellbeing.
Our research holds a number of implications for policymakers, organisations and future research, calling for professional boundaries in home-based care to be reframed. Professional boundary drawing should promote connection, not separation and be negotiated between client and worker (O'Leary et al., 2013). Indeed, Curtis and Hodge (1994: 16) say that ‘if community support workers are not facing relationship boundary issues in their daily work, they are probably not doing their jobs most effectively’. Our findings reinforce the need for more research that critically analyses the ways in which boundaries are drawn, and how they may be used to exclude some workers, their knowledge and identity and to maintain the dominance of Western ideals of professionalism and care. Ultimately, we argue for the integration of holistic models of care that include Māori concepts of wellbeing that provide culturally appropriate care for Māori care receivers, their whānau and care workers.
Footnotes
Acknowledgements
E Tū, PSA Unions and all our participant researchers.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a New Zealand Health Research Council Grant number 20/1383.