
Abstract
The dominant wellbeing discourse (DWD) in neoliberal economies can be understood as a form of bio-power that presupposes healthy individuals. It seeks to produce subjects who take responsibility for their wellbeing and, in this way, render themselves productive. Drawing on interviews with individuals who volunteered a diagnosed mental health condition (MHC), we explore how they resisted the negative associations with MHCs through making their conditions invisible. Hence they sought to blend in and make themselves visible as ‘normal’, well, healthy, responsible, productive subjects. Although we call this chameleon resistance it is bound up with consent and compliance as it reproduces the DWD and negative associations with MHCs.
Introduction
Our contemporary understanding of wellbeing reflects a neoliberal discourse (Holmqvist et al., 2013; Wallace, 2022) that fosters individual responsibility for health (Greco, 1993; Zoller, 2003) whether through fitness (Kelly et al., 2007; McGillivray, 2005), diet or other lifestyle changes (Holmqvist et al., 2013; Maravelias, 2009, 2018). We refer to this as the dominant wellbeing discourse (DWD). It is constructed around the need to address ‘individual’ problems such as stress, anxiety or obesity as a means to improve ‘work performance’ (Maravelias, 2018: 342) and thereby reap ‘economic benefits’ (McGillivray, 2005: 131). According to the UK Government’s ‘Mental Health and Wellbeing Plan: Discussion Paper’ (online April 2022), wellbeing is irrefutably ‘positive’ enabling ‘long, healthy, independent, purposeful and flourishing lives. Good wellbeing can support effective learning and productive working’. Critical scholars have pointed towards more negative associations arguing that corporate demands and indeed wellbeing initiatives can contribute to the problems wellbeing purports to remedy (Calvard and Sang, 2017; Cederstrom and Spicer, 2015; Foster, 2018; Haunschild, 2003; Moore, 2018; Wallace, 2022) thereby serving to exacerbate ‘(mental) health issues’ (Harvey, 2019: 639). Whilst we recognise that the ‘evolution’ of the ‘idea of mental illness’ ‘is complex and polymorphous’ (see Foucault, 1984a: 191), we seek to add to a critical understanding of wellbeing by exploring the subjectivity and actions of those diagnosed with Mental Health Conditions (MHCs).
The DWD assumes that if we work on our bodies, fitness and mental wellbeing we can generate a ‘fitter, happier, more productive’ (McGillivray, 2005: 125) version of ourselves. As an expression of bio-power, it is a ‘diffuse apparatus of control’ that ‘operates indirectly through the manipulation of culture’ (Munro, 2012: 348) creating a ‘duty to stay well’ (Greco, 1993: 357). It is evident in the framing of health issues, management and self-help books, workplace health promotion schemes and lifestyle magazines (see Dailey et al., 2018; Greco, 1993; Hancock and Tyler, 2004; Haunschild, 2003; Kelly et al., 2007; Maravelias, 2018; McGillivray, 2005). Reinforcing a ‘norm of physical, mental and emotional health’ (Foster, 2018: 189) citizens and employees are urged through the DWD to ‘self-manage’ (Moore, 2018: 55) and ‘contribute more of themselves’ (Harvey, 2019: 641). It is assumed that they can choose to be ‘productive’ by taking ‘responsibility for their own health’ (Haunschild, 2003: 52) thereby better meeting the demands of capital (see Dailey et al., 2018; Holmqvist et al., 2013).
We draw inspiration from the Management and Organization Studies (MOS) literature that has examined how ‘our sense of ourselves as distinct subjectivities is constituted’ (Clegg, 1989: 151) through disciplinary power (Foucault, 1977) operating through workplace discourses such as enterprise (Du Gay, 1996), strategy (Knights and Morgan, 1991) and HRM (Townley, 1993). This literature highlights that ‘while not being determined, the self is regulated’ through ‘discourse and disciplinary practices’ and how ‘we contribute to this process by turning ourselves into particular subjects’ (Thomas and Davies, 2002: 377). Although there is no outside of power, freedom ‘involves strategically reworking power relations to which we are subjected’ (Allen, 2011: 51). The situation is therefore complex, ambiguous and uncertain generating processes of ‘adaptation, subversion and reinscription of dominant discourses’ (Thomas and Davies, 2005: 363) whereby ‘consent, compliance and resistance’ (Collinson, 1994: 51) merge and overlap.
Bio-power coexists with and ‘incorporates certain aspects of disciplinary power’ (Lilja and Vinthagen, 2014: 121) such as training, education and surveillance, it is ‘directed at society rather than towards individuals’ (Lilja and Vinthagen, 2014: 121) and ‘applied in the whole fabric of society, by the state, as well as by corporations and civil society actors’ (p. 119). As bio-power targets ‘whole populations’ (Haunschild, 2003: 49), it necessitates a broader focus than individual workplaces, which has been the mainstay of the MOS literature. Recent theoretical interest in bio-power (e.g. Fleming, 2014; McNay, 2009; Munro, 2012) does not relate to ‘the fetishism for counting’ populations (Hacking, 1982: 294) but to neoliberal governance’s ‘tendency to expand’ (Foucault, 2007: 44) into new domains that urge individuals to embrace ‘responsible self-management’ (McNay, 2009: 56). It relates to Foucault’s concept of governmentality that refers to how individuals are regulated ‘at a distance’ (Miller and Rose, 2008: 7) ‘without the need for intervention’ (Foucault, 1984b: 241). Individual freedom or autonomy becomes the battle ground whereby the ‘“self-steering” mechanisms of individuals’ (Miller and Rose, 1990: 18) are enrolled and extended into ‘broader ways of living’ merging work and ‘life itself’ (Fleming, 2014: 882). This is partly achieved by discursively managing ‘the environment, the milieu in which they live’ (Foucault, 2003: 245). Empirical analysis of bio-power has considered control and consent (Moisander et al., 2018) but, as Fleming (2014) and Moisander et al. (2018) assert, resistance has been empirically neglected. We add to such work therefore by considering bio-power in relation to the DWD, resistance and MHCs.
Through drawing on interviews primarily with individuals diagnosed with MHCs, we argue that they may resist the DWD through making their MHCs invisible whilst also making themselves visible as ‘normal’ subjects. We call this chameleon resistance that reflects compliance and consent because through it subjects attempt to ‘blend in’ and represent themselves as well, healthy, responsible and productive. The seminal literature on resistance (e.g. Ackroyd and Thompson, 1999; Jermier et al., 1994) and key concepts including making out, distance and cynicism (e.g. Burawoy, 1979; Collinson, 1994; Fleming and Spicer, 2003) have neglected those with MHCs and so this article adds to our understanding of resistance.
The critical literature on wellbeing has quite rightly emphasised its negative implications. Hence Maravelias (2018) explored the role of Workplace Health Promotion schemes in Sweden and posited that ‘they implicitly contribute to the exclusion’ (p. 333) of individuals. Likewise, Harvey (2019) argues that corporate wellness ‘serves to further marginalise and stigmatise the unfit, unhealthy or those with disabilities’ (p. 642). By contrast, we argue that the DWD can also be understood as ‘productive’ of chameleon resistance whereby the marginalised engage in individualised struggles. This is ‘resistance at the level of subjectivity’ (Meriläinen et al., 2004) or identity (Ezzamel et al., 2001; Knights and McCabe, 2000) but it also requires subjects to act or not act in particular ways.
Mental Health Conditions pose a problem for the DWD or the expectation of wellbeing for wellbeing is not something that those with MHCs can easily control or simply choose. Although a significant part of the population can improve their wellbeing through diet, exercise, mindfulness, abstinence or other lifestyle changes, for many, not just those with diagnosed MHCs, there is no simple remedy. It could be argued that they are forced to engage in chameleon resistance due to assumptions within the DWD that government, society, organisations, peers and even they enforce as we shall explore below. This challenges how the DWD is supposed to work potentially thwarting but also enabling it. It enables as those with MHCs work on themselves, in part, so as to appear to conform with the DWD whilst hiding their MHC. It thwarts because this could increase suffering (see Smith and Ulus, 2020) and make health problems worse whilst subverting the DWD in terms of how it should work. In this sense, although the DWD ‘transmits and produces power; it reinforces it’, it ‘also undermines and exposes it, renders it fragile and makes it possible to thwart it’ (Foucault, 1979: 101).
The article is organised as follows; in the next section, we explain what we mean by the DWD through reviewing relevant literature. We then explain the research methods before presenting the empirical data. Finally, we draw out the main insights and arguments of the article in a discussion and conclusion.
The dominant wellbeing discourse and mental health conditions at work
The assumption underpinning the DWD is that individuals have the capacity to be more productive by taking responsibility for and developing their wellbeing. Individuals are tasked to work on themselves to maximise ‘a version of their happiness and fulfilment’ (Miller and Rose, 2008: 215). In this section, we explore how the DWD operates as bio-power through identifying disparate strands of the discourse that ‘targets a population of living beings en masse’ (Moisander et al., 2018: 5) directing them towards certain subjectivities and actions. In this sense, it ‘moves beyond the particular forms of activity usually understood to constitute wellbeing practice’ (Wallace, 2022: 3).
In 2010, David Cameron, the then Prime Minister and leader of the UK’s coalition government launched the National Wellbeing Programme. A policy paper ‘Wellbeing: policy and analysis’ published in June 2013 stated: ‘Nationally, Public Health England (PHE) has been established to protect and improve the nation’s health and wellbeing’. The aim of PHE was to integrate ‘wellbeing into national public health and health improvement campaigns and communications’ (Wallace, 2022: 3). In April 2022, the ‘mental health and wellbeing plan: discussion paper’ launched by the UK’s Conservative government, marked the success of this roll out. Its ministerial foreword states ‘we’re talking more about our mental health and wellbeing than ever before’. The paper stated that ‘health is essential to a stable and functioning economy’ for a ‘healthier and happier population is also more likely to access employment opportunities, which will reduce inactivity and improve productivity’. Mental ill health was defined as ‘a negative state of wellbeing’ whilst wellbeing involves being able to ‘engage in work productively’. The economic underpinning of wellbeing is clear.
The DWD is also evident in the mainstream literature on wellbeing where ‘well-being means developing as a person’ (Shah and Marks, 2004: 2) and elsewhere the ability to fulfil goals (Foresight Mental Capital and Wellbeing Project, 2008). This focus on setting goals so as to develop as a person fits with individual’s taking responsibility for their wellbeing. The DWD is bound up with managerialism indeed in a review of the HRM literature and its treatment of well-being, Guest (2017) argues that ‘the primary focus is invariably on organizational performance’ such that ‘well-being may be a by-product, but it is incidental’ (p. 25) to performance. This disadvantages and excludes those with MHCs as they may not always be able to fulfil goals.
The DWD places ‘the pursuit of wellbeing in the hands of individuals’ (Dodge et al., 2012: 231) and so decontextualises wellbeing and employees from the demands of capitalism (see Hancock and Tyler, 2004; McNay, 2009). It is particularly problematic for those with MHCs for they may be unable, at times, to engage with what Ryff and Singer (2008) depict as the core dimensions of psychological wellbeing including environmental mastery, positive relationships and personal growth. The potential for exclusion is evident in Headey and Wearing’s (1991) dynamic equilibrium theory of wellbeing which assumes that ‘subjective well-being is fairly stable’ (p. 49).
We can also observe the DWD in lifestyle magazines (see Hancock and Tyler, 2004) and self-help books, for example, Jeffers (1987) Feel the fear and do it anyway has sold over two million copies worldwide and states ‘Taking responsibility means never blaming anyone else for anything you are being, doing, having or feeling’ (p. 49) whilst recognising that ‘you are the cause of your unhappiness’ (p. 52). It tells individuals to ‘set your goals – then go out and work toward them’ (p. 59) realising ‘that at every moment you are choosing the way you feel’ (p. 60). Similarly, popular management texts including the One Minute Manager that has sold over 18 million copies in 25 languages requires individuals to set goals and take responsibility through ‘managing their own behaviour’ (Blanchard and Johnson, 1983: 92). The link with wellbeing is that through engaging in such practices and subjectivity people are said to ‘feel good about themselves’ (p. 7). Yet, through this DWD, MHCs are rendered negative being ‘construed as a problem of irresponsible self-management’ (McNay, 2009: 64).
Covey’s (1989) The 7 Habits of Highly Effective People crosses the line between a self-help book and a management text. It has sold more than 25 million copies in 40 languages worldwide. Covey presents 7 habits which focus on changing ourselves before we can change others and so we can observe ‘life itself’ becoming ‘enmeshed with power relations’ (Fleming, 2014: 881). The habits are couched in relation to free choice and responsibility coupled with ‘setting goals’ (Covey, 1989: 92). The link with wellbeing is clear when Covey (1989) tells us that his habits ‘represent the internalization of correct principles upon which enduring happiness and success are based’ (p. 23). Wellbeing, it seems, is a choice or ‘health that can be ‘chosen” (Greco, 1993: 369) and so a lack of health/wellbeing is negative and ‘implies a personal fault’ (p. 370).
The first of Covey’s habits is ‘proactivity’, which means that ‘we are responsible for our own lives’ (Covey, 1989: 71). He breaks responsibility down– ‘“response-ability” – the ability to choose your response’ (Covey, 1989: 71) and so ‘Happiness, like unhappiness, is a proactive choice’ (p. 90). This logic is indicative of ‘bio-power’ where ‘additional freedom’ is introduced ‘through additional control’ (Foucault, 2008: 67) such that wellbeing is achieved through self-discipline. It suggests that we should all be proactive people who do ‘not blame circumstances, conditions, or conditioning for their behaviour’ (Covey, 1989: 71). It sets up a discursive position against which it is possible to rebel but it is also potentially productive of chameleon resistance as it renders MHCs negative.
As we have seen, the DWD is part of ‘the milieu in which’ contemporary employees ‘live’ (Foucault, 2003: 245) and it is also reproduced through corporate health and fitness programmes, that foster the belief that health issues can be addressed through individual dietary changes or fitness programmes (Greco, 1993; Haunschild, 2003; McGillivray, 2005). Maravelias’ (2018) research into workplace health promotion (WHP) schemes asserts that they define ‘a healthy individual as a person that is self-conscious and responsible with regards to risks while active and positive with regard to opportunities to improve in all of life’s spheres’ (p. 343). It does not seem entirely correct to us to argue that WHP ‘does not seek to impose ideals and norms’ (p. 343) because responsibility, choice and wellness are the ideals and norms it endeavours to foster.
Another example of research into a workplace health and fitness programme resonates more with disciplinary power for it explored how individuals are made ‘visible’ through measuring and examining them against fitness and health norms (Kelly et al., 2007: 279). As Foucault (1977) puts it the ‘normalizing gaze’ serves to establish ‘over individuals a visibility through which one differentiates them and judges them’ (p. 184). Kelly et al. (2007) argue that within such regimes ‘there is no place for unhealthy workers’ (p. 280), which could help to explain why employees may resort to making themselves invisible through chameleon resistance. We can observe that bio-power ‘does not exclude disciplinary technology but dovetails into it’ (Foucault, 2003: 242) hence workplace health and fitness programmes require employees to ‘practise their freedom in the pursuit of goals devised and designed by management’ (Kelly et al., 2007: 280). They are potentially negative for individuals with MHCs who, due to their condition, may not be able to act responsibly, productively or pursue management goals, all of the time. Kelly et al.’s (2007) empirical study presented a corporate ‘Mind and Body Profile’ that listed ‘being over-weight’ or ‘drinking too much caffeine’ alongside being ‘depressed’ (p. 278). It therefore erroneously equates MHCs with issues that individuals can control. These health programmes are therefore potentially repressive for individuals with MHCs but they may also be productive– spurning individuals on to struggle with their condition so as to comply with corporate demands and hide their MHC through chameleon resistance.
Within employment, there is often ignorance and misunderstanding about the nature of MHCs. Hence those with MHCs are represented as negative or lacking the ability to meet the economic and social demands of work or indeed work is portrayed as not being healthy for MHCs (Krupa et al., 2009). This pejorative discourse has begun to change recently but still the DWD assumes that ‘individuals’ personalities, lifestyles and social relations’ are ‘potential resources’ and ‘potential risks that should be managed’ (Maravelias, 2018: 334). This sits uncomfortably with MHCs and helps to explain chameleon resistance and the marginalisation of those with physical or mental disabilities (see Foster, 2018; Jammaers and Zanoni, 2021; Jammaers et al., 2016). Hence the assumption ‘that all performers start at an equal level of competence’ places those with MHCs at a disadvantage that ‘can easily result in unequal judgements and appraisals’ (Moore, 2018: 56).
In terms of studying marginalised others, Zanoni and Janssens (2007) have analysed the experiences of minority employees but neglected those with MHCs. This article is distinctive therefore as our primary focus is on the wellbeing of individuals diagnosed with a MHC. Jammaers et al. (2016) assert that disabled employees are constructed ‘as less capable, willing and productive workers and thus less valuable for and/or employable by organizations’ (p. 1366). This exercise of power, reproduced through the DWD, exerts ‘pressure on employees to preserve their health and to demonstrate fitness’ (Haunschild, 2003: 46). Although power exercised in this way serves to ‘produce and maintain subordinate identity positions’ (Jammaers et al., 2016: 1366), we need to consider power relations, whereby the seemingly powerless exercise power as it could generate chameleon resistance.
The DWD requires individuals to work on themselves and this creates pressures to perform, to appear well, happy and healthy. This can be a struggle for seemingly ‘healthy’ or ‘normal’ employees but it presents a burden for individuals who experience MHCs who may, at times, struggle to live up to standard work norms let alone ‘compete with the corporate athlete’ (Harvey, 2019: 643). To do so may lead to ‘higher levels of work strain’ (Harvey, 2019: 643) and ‘a deterioration in workforce mental health’ (p. 644). Extant research acknowledges that ‘we know relatively little about workers’ perspectives concerning workplace wellness’ (Dailey et al., 2018: 613) and we know even less about employees with MHCs. Indeed, Jammaers et al. (2016) assert that ‘Scant attention’ has been given ‘to how disabled subjects’ (Jammaers et al. 2016) engage with such discourses (see also Woods et al., 2019) for they ‘feature rarely’ (Foster, 2018: 189) in the wellbeing literature. An exception is a recent paper by Smith and Ulus (2020) that explored the wellbeing of academics only some of whom were ‘formally diagnosed’ (p. 841) with a MHC. It challenges ‘existing discourses’ (p. 840) about wellbeing that ascribe responsibility for pain and suffering to individuals rather than the institutions for which they work. They identified ‘recurring themes of shame and fear of being judged incompetent’, which they posit necessitates ‘silencing and disappearing – making invisible the anguish of human struggle’ (Smith and Ulus 2020).
These findings lend support to those we will shortly explore hence an academic with a MHC stated ‘I have hidden the symptoms. They are masked, veiled, denied by me’ (p. 849). Smith and Ulus (2020) do not present this as resistance perhaps because they focus on suffering. Nevertheless, we argue that such struggles can be understood as resistance that extends well beyond academia. Smith and Ulus (2020) ‘surface’ the negative aspects of academic life including the ‘pain’ and ‘struggles of emotional health’ (p. 847) but, in doing so, they tend to omit what it potentially positive about such struggles. Hence subjects exercise power as they don a mask, refuse to take time off, strive for normality or remain silent. Naming these subjectivities and actions chameleon resistance, is a way to collectivise this experience. It brings it into focus and helps to crystallise something that was previously known but nebulous helping us to discuss it and initiate ‘solidarity at work’ (Smith and Ulus, 2020: 847).
According to Jammaers and Zanoni (2021), ‘hiding one’s disability from the organization’s view represents a clear form of resistance’ (p. 19) and yet chameleon resistance, is not clearly resistance for it is entangled with compliance and consent. Hence chameleon resistance involves making oneself visible through a ‘performance’ (Maravelias, 2018: 341) of ‘normal’ health that simultaneously renders the individual and their condition invisible. Smith and Ulus (2020) describe their ‘biggest concern’ as ‘the silence around these struggles’ and how individuals ‘function yet remain hidden in pain’ (p. 852). To address these concerns, we will now explore the experiences of those with MHCs in relation to the DWD.
Research methods
Hadar interviewed forty-two individuals who volunteered that they had been diagnosed with a MHC and these included 30 males and 12 females. She also interviewed employers [10], health professionals [3] and mental health charity workers [7] all from the UK. The representation to follow is inevitably ‘partial’ because ‘one cannot tell all’ (Clifford, 1986: 7) and ‘no one reads from a neutral or final position’ (p. 18). In this study, the generation and presentation of research data are understood as the co-construction of the authors and interviewees (Alvesson, 2003). We did not therefore follow an ‘inductive logic’ (Janssens and Zanoni, 2005: 312) where findings are seen as respondents’ constructions for ‘discourses, are not objective – they, themselves, are socially constructed’ (Hardy et al., 2000: 1233) and so it is necessary to acknowledge the part that we play in their construction. We do not claim to speak on behalf of those with MHCs not least because neither of us have experienced MHCs. We are therefore distanced from the multiplicity and complexity of such experience. The following account is an attempt to theorise the experiences interviewees related to Hadar. The interviewees did not talk in terms of resistance, consent and compliance. Nevertheless, the following account seeks to understand the concerns they raised in a sympathetic way. It would be useful for future research to focus upon and explore the specific issues raised here especially through asking participants with MHCs to consider their relevance to their lives.
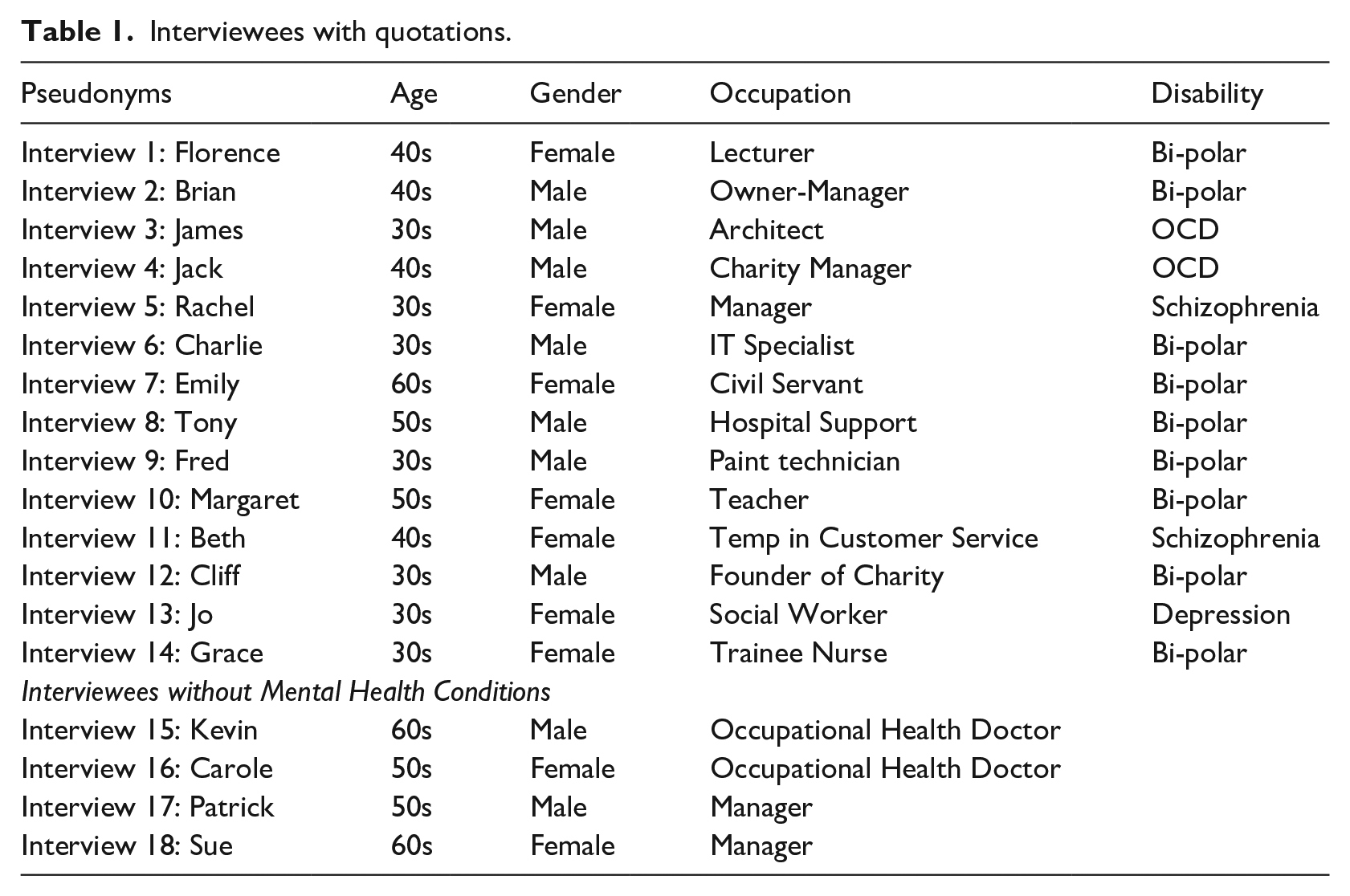
Information about the research was distributed by Hadar through a leading mental health charity in the UK and other mental health organisations and support groups. The participants had been diagnosed with one of the following MHCs: bi-polar, anxiety disorder (including Obsessive Compulsive Disorder), schizophrenia or depression. The ratio corresponds with what are considered the most common workplace MHCs relating to mood [30], anxiety [7] and psychosis [5] (Fryers et al., 2005). The participants’ occupational backgrounds spanned the voluntary, private and public sectors (see Table 1 for a summary of the interviewees represented in this article).
Interviewees with quotations.
The semi-structured, recorded interviews, lasted approximately 1 hour and were transcribed. Hadar did not seek to impose meaning on the interviewees. Instead, general questions were posed about their work experiences and mental health allowing for flexibility, adaptation and themes to emerge. The following questions were asked: Could you talk about your health condition in relation to your employment? Could you tell me about your day-to-day experiences inside and outside of work? What are your experiences in relation to mental health? How do you get on in the workplace? How you think others in this organisation (colleagues/managers) view you or your work performance?
Interviewees were promised confidentiality and anonymity both in relation to themselves and their employer and in any publications the research might generate. In view of this, all of the names used are pseudonyms and measures have been taken to ensure that the respondents cannot be identified. In view of the sensitivity of the subject, interviewees were afforded every opportunity to take a break or stop the interview/recording in an endeavour to create ‘a relatively safe environment for the interviewees to speak frankly’ (Zanoni and Janssens, 2007: 1379). This was explained at the outset and interviews were conducted with vigilance for any signs of distress. In practice, this did not prove to be an issue perhaps because individuals volunteered that they had a MHC and expressed a willingness to talk about it indicating that they were relatively comfortable about doing so. Indeed, the interviewees were far from passive and they referred to tools and techniques they employed to manage their mental health. Nevertheless, to ensure a relaxed setting, Hadar avoided jargon, wore casual clothing and talked to the interviewees as partners in the generation of knowledge. The interviews predominantly focused on work experience related to MHCs, however, the participants were invited to add anything they considered important.
Data analysis and development
Data analysis paid close attention to the discourse the recipients used and involved a number of stages as the interview data was explored and meaningful themes emerged. These themes are not separate from the authors because ‘there is no such thing as “pure” description’ (Walcott, 1994: 13) for as Watson (1994) expresses it, ‘Management researchers select, interpret, colour, emphasis, shape their research findings’ (p. 106). The first stage of the analysis began during the interviews as Hadar wrote notes and these were revisited immediately after and expanded into memos as a sense making device. The concern was to identify key words, issues and possible themes. Through this analysis different themes arose including that of invisibility. The interviewees expressed a desire for their voices be heard and their experiences to be known and so we have sought to remain true to their concerns whilst analysing the complexity and ambiguity of their experiences.
This gave rise to the second stage of the analysis whereby Hadar coded the data according to different themes and extracted illustrative quotes from the interview transcripts. Hadar analysed the interview transcripts and selected extracts to explore how mental health is constructed discursively in the workplace; how those with MHCs cope and how this is related to stigma, prejudice and discrimination. Hadar then produced a first draft of the article by organising and analysing the data in relation to (1) Invisibility and behavioural symptoms (2) Pretence, disclosure and struggle at work and (3) self-stigma; internalizing a mental illness subject position.
It was then that Darren became involved in the development of the article. He analysed Hadar’s empirical extracts in relation to different exercises of power and this included re-organising and analysing the empirical extracts in relation to the categories of (1) society (2) corporations and (3) self, which will be explained below. The focus of Hadar’s empirical research on the experience of individuals with mental health conditions lent itself to a consideration of wellbeing and so in preparation for this special issue, Darren positioned the article in relation to the wellbeing literature by critically examining it in relation to what is referred to as the Dominant Wellbeing Discourse.
The reviewers then instigated the final stage of the paper’s development as they prompted a rethink of its theoretical and empirical focus. This required greater engagement with the literature on wellbeing, resistance and a new focus on biopower. Darren responded to the reviews and, drawing on the empirics, developed the idea of chameleon resistance connecting this to the literature on biopower, resistance and wellbeing. In order to do this, he also re-analysed the empirical material in relation to chameleon resistance and visibility as well as invisibility.
The three categories that the data is organised around are not mutually exclusive. Each imbues the other in terms of how power is exercised and resisted in relation to the DWD but each has a different emphasis on society, organisations and the self. The first relates to how the interviewees referred to ‘people’ or the ‘generalized other’ (Berger and Luckman, 1967: 153) when discussing their experiences rather than particular individuals/settings. It was inferred from this that they meant society in general although clearly society is constituted through individuals, workplaces and so on. The interviewees alluded to how society exercises power in a negative way rendering them and their condition invisible. Through voicing opposition to this during the interviews, it seemed that they were resisting such negative representations and endeavouring to make their subjectivity and the lived reality of their conditions visible. The interviewees presented themselves as ‘normal’ and capable therefore of fulfilling at least some of the expectations of the DWD, which can be understood as indicative of consent.
The second category explores how power is exercised by employers, managers, peers and the interviewees in ways that are bound up with the DWD that are more specific to the workplace. It considers dynamics around the self-disclosure of MHCs, economic pressures and ‘making out’ (Burawoy, 1979) or, in other words, escaping work demands. It examines how individuals engaged in chameleon resistance in order to escape negative associations and hide their condition. Moreover, it also considers how, in some instances, medical professionals colluded in helping them to do so. Paradoxically, through chameleon resistance, those with MHCs also sought to make themselves visible as subjects that are not defined by a MHC. At times, resistance can be seen as an act of compliance as it reflects that jobs and careers were threatened unless individuals were able to make their MHCs invisible.
The third category explores how interviewees engaged in struggles in relation to the DWD that related to their identity or subjectivity. It examines how individuals consent to and resist the DWD discourse as part of a ‘complex and unstable process’ (Foucault, 1979: 100–101). This partly reflects how bio-power extends into ‘broader ways of living’ merging work and ‘life itself’ (Fleming, 2014: 882) and individuals drew on their self-understanding to engage with but also resist the DWD. As we shall see, this renders outcomes unpredictable because although bio-power encourages subjects to ‘be themselves’ (p. 878) this can be used both for and against the DWD. The interviewees exercised power in productive and negative ways rendering themselves visible and invisible in relation to the DWD. We now turn to our empirical findings, which are organised in three sections that reflect these categories.
The DWD and society
Interviewees referred to ‘people’ or their experiences of society in a way which suggested that they are rendered invisible through it, partly due to ‘negative identity regulation’ (Jammaers and Zanoni, 2021: 14) that defines them as ‘inferior to’ (Jammaers and Zanoni, 2021) others: ‘People don’t talk about it [mental health conditions] or aren’t aware. . . and feel embarrassed to talk about it, and feel it’s a secret. . . it’s almost a fear factor. . . people who don’t have mental health conditions almost have a superstitious fear that it’s almost like they might catch it. It’s almost as though: “if I acknowledge that mental health conditions exist then I might be at risk of it. So, I just have to pretend that it’s all nonsense and that these people are simply weak, and somehow dysfunctional”. And I think people find it quite scary’ (Florence, lecturer, mid 40s, diagnosed bipolar).
Embedded in the DWD is the assumption that people are well and responsible for their wellbeing. As Florence’s comments suggest, those with MHCs are therefore seen as ‘weak’ or ‘dysfunctional’ which implies that they have failed to take responsibility for their wellbeing. These insights indicate that the DWD not only impacts those with MHCs but everyone due to the ‘fear’, ‘secrecy’, ‘embarrassment’ and general negativity that circulates around MHCs. This renders MHCs invisible because one cannot talk openly about them and it detaches MHCs from the experiences of those with MHC. Cliff is in his early fifties and is the founder of a mental health charity. He has been diagnosed bi-polar and stated: ‘self-stigma is a very complicated thing which, because of stigma in society, it’s very difficult to rinse out of your mind’. Cliff’s comments imply that he experiences the societal exercise of power in a negative way. Similarly, Brian, the owner/manager of an Equality and Diversity organisation, who has been diagnosed bi-polar, remarked: . . .[society] might think that people with schizophrenia or bi-polar are somehow monsters. They don’t understand that it could be your brother, your sister, your child, which is often portrayed in the TV as the killer with the psychotic condition, the drug addict or they are alcoholic. We don’t hear of any normal people with MHCs, who just don’t affect anybody else rather than themselves and their family– they are not all raving murderers
These remarks elucidate a belief that society does not understand MHCs and regards them negatively such that both the person and the condition are distorted and rendered invisible. To regard individuals as ‘murderers’, ‘monsters’, ‘weak’ and ‘dysfunctional’ stereotypes, generalises and demonises them therefore rendering subjectivity visible but in a distorted and pejorative way. These negative understandings and representations help to explain why individuals may engage in chameleon resistance to avoid visibility.
Brian referred to not hearing ‘of any normal people with MHC’s’, which resists the ‘negative identity’ (Jammaers et al., 2016: 1375) associated with MHCs through ascribing ‘normalcy’ (Foster, 2018: 191) to people with MHCs. It can be understood as an attempt to render his subjectivity visible whilst resisting negative subjectivities such as the monster, killer or drug addict. Zanoni and Janssens (2004) found that HR managers constructed diversity in ways that obscured the ‘individuality’ of diverse [disabled, migrant] workers, arguing that it ‘eliminates their agency’ (p. 62). Likewise, the individuality of those with MHCs is rendered invisible when they are represented as ‘murderers’ or ‘monsters’ and Brian resisted this distortion, simplicity and negativity. Nevertheless, presenting those with MHCs as ‘normal’ reflects consent because it implies that they are able to comply with the DWD and its expectations. This could be seen as chameleon resistance, as it attempts to blend those with MHCs into the wider society. It also makes those with MHCs visible as human beings rather than monsters or killers. Brian drew on the target of bio-power, his subjectivity or ‘unique personal attributes’ (Fleming, 2014: 885), to resist the negative associations with MHCs.
James, an architect in his early thirties, who has been diagnosed with OCD remarked – ‘OCD becomes like a “watered down” subject. . ..It’s not a funny thing’. He referred to the popular conception of OCD as an obsession with cleaning, which some might regard as funny. His comments resist such simplicity that renders his subjectivity, experience and condition invisible but it also seeks to make his understanding of his MHC and subjectivity visible. Similarly, Jack, a regional manager for a charity in his mid 40s who has also been diagnosed with OCD opined: ‘I don’t think people really understand much about mental health still. I don’t think people know what an obsessive compulsion is. They think, like they’ll say, someone has OCD ‘cos “they’re tidy”, or something like that. They say someone is schizophrenic when they’re confused or they can’t make their mind up. . ..Or someone is depressed when they’re grumpy or sad’
These insights suggest that MHCs are diluted and transmogrified through the filter of the DWD hence those with MHCs are deemed well but unusually tidy, indecisive, grumpy or sad. Jack and James’ discourse resist through attempting to break through the distortion, the ignorance to render their MHC and subjectivity visible in a way that is truer to their lived experience. Likewise, Rachel, who has been diagnosed with schizophrenia and manages a mental health self-help group, recounted: ‘some people think I am just lazy. . ..why doesn’t she pull herself together? Why can’t she just carry on?’. These insights express opposition to the DWD and its assumption that individuals are responsible for their wellbeing and so should ‘just carry on’ or ‘pull’ themselves ‘together’ as if they can choose to have a MHC or not. The comments of Charlie, an IT specialist in his early thirties who has been diagnosed bi-polar, are also relevant: ‘I feel sorry for members of families who have a bi-polar relative and they just, they don’t realise that, that person actually has a health condition. They just think it’s their personality that their personality is awful and they are just really hard work’.
The DWD assumes that individuals are well and therefore responsible for their wellbeing and so MHCs are assessed negatively against this discourse. This renders those with MHCs and their condition invisible but the individuals Hadar interviewed were not passive and expressed opposition to the way in which they believe ‘society’ understands them. This included referring to the unreasonable assumptions underpinning the DWD. Hence they indicated that their conditions are not trivial and indeed prevent compliance with the DWD. They wanted to be heard and this can be seen as a productive struggle against bio-power to affirm their sense of self, rights, dignity and visibility. We will now turn to experiences that relate more directly to the workplace.
The DWD and corporations, managers and peers
The self-reporting of MHCs requires individuals to make themselves visible as subjects who potentially do not conform with the DWD. In a context where economic performance is everything, this poses a threat to employment and career prospects and so there is pressure not to disclose. Kevin, an occupational health doctor, explained how practitioners may collude in this: ‘GPs (General Practitioners) wouldn’t declare it (their patient’s MHC) on the sick note, they put something else’. Although this collusion protects the confidentiality and economic interests of patients, not declaring MHCs on sick notes contributes to the invisibility of MHCs. It obfuscates an aspect of their patients’ subjectivity and yet it is productive for them in economic terms. Emily is in her sixties, has worked for the civil service and has been diagnosed bi-polar. She explained ‘I had a cooperative GP. He deliberately wrote me certificates that I suffered from flu, bronchitis and anything that was going around. . .he never revealed on the certificate that I was mentally ill’. This can be understood as GPs exercising chameleon resistance-by-proxy for they hide their patients’ condition allowing them to appear well, productive and competitive. Zanoni and Janssens (2004: 64) found that HR managers reproduce ‘discourses of difference’ but these GPs produced similarity by rendering difference invisible.
There are many forms of resistance including work avoidance, whereby individuals make life easier or more tolerable for themselves by creating ‘space’ in the working day (see Knights and McCabe, 1998). Indeed, ‘making out’ (Burawoy, 1979) means finding ways to cheat the system or surreptitiously doing things more quickly than expected to free oneself from work demands (see Roy, 1952). To falsely declare a MHC can be understood as resistance by deception if the intention is to reduce one’s workload or otherwise game the system. Kevin (occupational health doctor), referred to this as ‘getting away from work with mental health’. It could be seen as an obverse form of chameleon resistance because instead of trying to blend in, appear well and hide a MHC, the individual falsely claims to be unwell and therefore makes a fake version of themselves visible. The remarks of Carol, another occupational health doctor, who provides occupational health services for financial services organisations, are relevant: we regularly see people who will use a mental health presentation to leverage something they want to achieve because a lot of mental health’s are self-reported. The symptoms are self-reported. So who is really suffering and needs my help? And who has decided they want to stream this out? It becomes associated with playing things for your own benefit. . .if you are a HR department and the word stress means: “please give me a larger pay off”, it’s very, very difficult not to allow that to colour your thinking about somebody who is genuinely unwell.
By declaring they are unwell, individuals indicate that they are not entirely responsible for their wellbeing and work performance. If individuals without MHCs use mental health to shirk their responsibilities or if individuals exaggerate their mental health problems then this could create difficulties for those with genuine or more serious MHCs as it could add to the negative associations with MHCs. It may contribute to chameleon resistance whereby individuals with genuine MHCs hide their condition for fear of being labelled a shirker or game player. Hence Sue, a line manager in her early sixties, who works in a large insurance organisation and manages employees with MHCs, asserted: ‘A lot of people seem to take the slightest thread of something and build it up into this big stressful situation where the genuine people with MHCs don’t want to be treated differently. Like most people with problems like that, they don’t. They just want to be normal. They struggle on, struggle through much, until they have gone a bit too far’.
Sue’s remarks indicate that those with genuine MHCs may engage in chameleon resistance, which reflects consent. Hence through their actions and subjectivity, they ‘struggle on’, seek to blend in, appear well and hide their condition ‘stressing similarity to other employees’ (Jammaers and Zanoni, 2021: 11). In such instances, they draw on ‘broader life qualities’ (Fleming, 2014: 889) such as resilience, dignity, self worth to resist and appear well. In so doing, these qualities become a ‘resource for the firm’ (Fleming, 2014: 889) that may increase the risk of more serious health issues when the struggles of those with MHCs lead them to go ‘a bit too far’. If this struggle creates meaning or a sense of purpose and direction, then it could be productive for some of those with MHCs even if it reproduces suffering. It is, of course, difficult to assess whether someone is feigning a MHC or exaggerating mild conditions. Indeed, the very idea delegitimises MHCs and renders them negative. It reinforces the DWD by suggesting that individuals have a choice in relation to their mental health, that MHCs are not ‘real’, which may lead some to engage in chameleon resistance to avoid such negative associations.
According to Calvard and Sang (2017), there are ‘employer expectations of wellness’ (p. 2259) and this reflects the DWD. It pressurises those with MHCs to engage in chameleon resistance and indeed Tony, who has been diagnosed bi-polar, is in his mid-fifties and works as a member of a hospital support team, explained that his manager ‘more or less said – if we’d known you were unwell we would have never employed you’. This is indicative of a ‘culture of intolerance’ (Foster, 2018: 190) and a ‘culture of silence’ (Smith and Ulus, 2020: 843) in relation to MHCs. Fred, a paint technician in his mid-thirties who has been diagnosed bi-polar, similarly recounted: ‘they told me I was lucky to have a job because if I had told them [about the MHC] they might not have given me a job’. The result is that ‘economic calculability’ (Fleming, 2014: 883) imbues Fred and Tony’s ‘broader life’ (Fleming, 2014: 883) and they know that to secure a job they must act so as to make their MHC invisible, which suggests compliance. Charlie adopted a strategy of silence for as he said ‘It’s a very difficult thing to tell somebody ‘cos there is a lot of stigma. If people don’t know then they can’t judge you’. Through chameleon resistance, he therefore hid his condition, to avoid being disadvantaged. As bio-power, the DWD enlists ‘life itself’ (Fleming, 2014: 895) and yet life finds ways to resist even if it only amounts to silence.
After being absent from work due to a mental health episode, Fred was afraid: ‘I didn’t want people thinking I was someone pulling a “fast one”, you know – trying to get out of work. . .I didn’t want them to think that I was a slacker’. Fred did not want his employer to think that he is a ‘slacker’ and expressed concern about what peers or co-workers might think. As Barker (1993) illustrated, peers can exercise power to ensure conformity with corporate and group norms nevertheless Fred also exercises power by representing himself as other than he is. He works on himself and engages in chameleon resistance to present himself as well, productive and not a ‘slacker’. Margaret is in her early fifties and is a music teacher who has been diagnosed bi polar. She also indicated that peers exercise power and in this way contribute to the DWD: ‘I was discriminated against. I think if you suffer from depression people can understand but I was mainly a bi-polar 1. So I was mainly “up” but they couldn’t understand why I was a bit outrageous, you know. So it was the people that I was working with not so much the employers’.
The fear of economic desolation haunts employees, which may be exacerbated for those with MHCs. Like other employees, they must represent themselves as ‘model’ (Zanoni and Janssens, 2004: 63) subjects but, in addition, they engage in chameleon resistance to conceal their MHC’s from peers and employers.
In this section, we have focused on the workplace and considered how employees with MHCs may feel pressure not to declare their condition to avoid economic discrimination. Employers, managers and peers exercise power through the DWD and so those with MHCs may engage in chameleon resistance to hide their condition. The next and final section, analyses more directly how individuals with MHCs may exercise power in relation to their sense of self, which has been alluded to in the first two sections.
The DWD and subjectivity
We have explored how power is exercised through the DWD by considering how our interviewees experienced this in relation to ‘society’ and the ‘workplace’. As we have indicated, those with MHCs are not passive recipients of the DWD but, in this final section, we concentrate more on how their struggles relate to subjectivity. Beth is in her early forties, temps in customer service and has been diagnosed with schizophrenia. Illustrating Woods et al.’s (2019) point that ‘few workers are likely to willingly embrace being identified, by themselves or others, as experiencing mental illness’ (p. 956), she engaged in chameleon resistance by hiding her lack of wellbeing: ‘I didn’t tell anyone that I was mentally ill. I hoped to come across normal, you know, I tried to put on a brave face, you know, and you don’t admit things like that. I didn’t say that I was schizophrenic, you know, you don’t use that word ever’.
Beth’s life has become ‘a sort of permanent and multiple enterprise’ (Foucault, 2008: 241) as she works on herself ‘to come across normal’. She therefore avoids certain words and manages her persona by putting on ‘a brave face’ and remaining silent about aspects of herself. The self that is bound up with a MHC is made invisible whilst she works to make a version of herself visible that conforms to the expectations of the DWD.
Brian is the owner-manager of an Equality and Diversity company and so appears to conform to the DWD. His occupation involves resisting discrimination and yet, despite being visibly and actively engaged in resisting the DWD, he also engages in chameleon resistance by hiding his condition: the majority of people will not go around and wear a badge and say ‘I have bi-polar disorder’. . . I certainly don’t advertise that fact (diagnosed bi-polar)
Brian works on himself to display the identity of an entrepreneurial, competent and responsible owner-manager. This is productive for him and others and it renders him compliant with the DWD. He also resists the expectations of the DWD through his Equality and Diversity business. Nevertheless, it seems that he cannot escape the negative associations with his MHC and so whilst his business endeavours to make MHCs visible he hides his own condition. This indicates ‘contradictory representations of the self’ (Jammaers et al., 2016: 1380), reflecting that the expectations of the DWD interact with his sense of self in multiple ways: ‘If somebody was judging me and labelling me as —I have a mental health problem— it would just make my depression and self-esteem worse really. . . I am ashamed of it and embarrassed. . .you feel like there is a big label you wear in your head’. (Charlie, IT Specialist, early 30s, diagnosed bi-polar)
Charlie’s comments elucidate the paradox ‘that well-being is a bad thing’ (Kowalski and Loretto, 2017: 2236) especially for those with MHCs as its expectations can lead them to deny or hide their suffering. Nevertheless, such negative associations mobilise resistance that may be productive of their sense of self. Hence Jo (social worker), who is in her late thirties and has experienced depression, recollected: ‘I suppose I had fallen into the trap of seeing depression as a weakness. And I assume that if I feel that about myself, other people must see that too or perhaps feel that, even in the profession which I work [social work]’. Jo referred to the ‘trap’ of ‘seeing depression as a weakness’ that she ‘had fallen into’ and so she has reflected on, engaged with and resists such negative associations. Grace is in her late thirties, diagnosed bi-polar and is training to become a nurse. She also engaged in chameleon resistance through silence: ‘It’s an embarrassment because of the ignorance of people. If everyone knew what it was and accepted it, I’d be like— ‘yeah I have got it and it’s fine’. But they don’t, so I just don’t say. I just don’t feel as if I am worth the same as normal people’.
Bio-power encourages individuals to ‘be themselves’ (Fleming, 2014: 878) and yet Grace uses this capacity to be herself to paradoxically hide part of herself. Of course, this hidden self is not free nor separate from power but is forged through power relations. It could be said that Grace is being herself through hiding a part of herself although this raises questions. Do individuals with MHCs regard themselves as separate from their MHC? If a MHC is part of oneself then can one be oneself through denying it? Does it depend on the MHC, its severity, duration and the individual? Do people feel ambivalent about whether a MHC is or is not part of them? Chameleon resistance works in complex ways ‘as resources’ (Maravelias, 2018: 333) for corporations who gain economically from individuals acting to obfuscate their condition and for individuals who are able to secure/retain employment by blending in. The struggle to do so may be productive for some but others may suffer as a consequence of hiding their condition. It may be an ambivalent experience but, however, it is experienced, it does little to challenge the DWD: He [GP] said you don’t need to work you can be on benefits for the rest of your life. . .I wanted to be like other people I didn’t want to live on the sick. I wanted to work, that was normality as far as I was concerned. I didn’t want to be abnormal and I felt if I live my life on the sick I was abnormal (Emily).
Emily is concerned about how others see her, how she lives her life and so she wants to make herself visible as a ‘normal’ person who works and, in this way, display her ‘value as human capital’ (Maravelias, 2018: 344). Here the DWD works in negative and productive ways. Emily turns ‘the propensities and self-regulating capacities of the worker into an economic resource for the organization’ (Moisander et al., 2018: 14) but also for herself. The ‘shame’, ‘embarrassment’ or negativity that is felt by those who fail to conform to wellbeing norms is productive as it leads Emily to seek employment so as ‘to be like other people’. It therefore works as a resource or motivation for her. Struggling to be visible as a ‘normal’ person also requires her to hide and repress her MHC through chameleon resistance, which could generate suffering. The struggle over one’s sense of self then in relation to the DWD can therefore be seen as both productive and negative.
Discussion
This article has explored invisibility and visibility through exploring the experiences of those with MHCs in relation to the DWD. The term chameleon resistance was introduced to depict how individuals may seek to evade the negative associations with MHCs by rendering their condition invisible. In doing so, they make part of themselves ‘invisible’ whilst endeavouring to make another version of themselves visible. Individuals confront a dilemma over whether or not to disclose and make their MHC visible. To be open may mean that they cannot gain employment. To conceal can protect them for failing to conform to the DWD but it can also lead to a lack of understanding of their condition making discipline for poor performance more likely. As we have seen, the DWD is not only achieved through rendering individuals ‘visible’ as Kelly et al. (2007) argue but also through creating the conditions whereby some individuals make aspects of themselves invisible. This contributes to the literature on wellbeing especially ‘the darker socio-political sides of well-being’ (Calvard and Sang, 2017: 2261).
We explored how chameleon resistance, like other forms of resistance such as ‘cynicism’ (Fleming and Spicer, 2003), ‘making out’ (Burawoy, 1979) or ‘distance’ (Collinson, 1994), is ambivalent because it includes both opposition and consent. It opposes negative associations with MHC and yet it is complicit in that which it opposes hence chameleon resistance reflects that individuals want to appear well, responsible, economic, productive and visible as ‘normal’ subjects. In this sense, chameleon resistance is not a rejection of the DWD. It might be argued that chameleon resistance is merely decaf resistance (Contu, 2008) because it guarantees ‘rather than’ disturbs or disrupts our ‘way of life’ (p. 370). Indeed, its purpose is assimilation rather than disruption nevertheless it is not passivity. It reflects struggle over what one is or is not, what one makes visible or conceals. This includes repression of self but it is also productive of self as those with MHCs learn to frame how others see them through their actions and subjectivity thereby developing ‘a sense of themselves as actors through the very process of struggle’ (Fleming and Spicer, 2007: 53).
Instead of examining how ‘organizations manage diversity’ (Janssens and Zanoni, 2005: 332), through focussing on the DWD as bio-power, we have explored how power is exercised in multiple ways. We have focused on how power is exercised in productive and repressive ways in a context of struggle. The DWD and its expectation of wellbeing can be said to repress and produce subjects but it also produces resistance as subjects struggle to conform to its demands. Chameleon resistance is an unexplored example of how resistance can be ‘productive’, which has been examined in relation to middle managers (Courpasson et al., 2012), employees and trade unions (McCabe, 2019) but not in relation to MHCs.
Chameleon resistance is ambiguous because it potentially both hinders and aids employers and employees. It hinders by reproducing the plight of our interviewees as it does little to challenge the DWD or the negative associations with MHCs. Nevertheless, it aids them because it seemed less damaging than unemployment and disclosing themselves as ‘disabled’, which posed a threat to their jobs, careers and identity. The struggle to appear well or ‘normal’ is ambivalent because whilst it may give purpose and meaning to those with MHCs harm may arise due to repressing an aspect of oneself, hiding suffering and perpetuating prejudice and inequality. In contrast to Contu’s (2008) arguments then even decaf resistance is not without ‘risk’ (p. 2). It allows corporate relations to continue, which aids employers whilst potentially hindering them through burying problems that might fester.
The limitations of chameleon resistance suggest the need for a ‘Rights discourse’ in relation to MHCs. McNay (2009) describes this as ‘a key mechanism whereby ignored, marginalized forms of social suffering are made visible as a valid form of political speech about justice, disrupting dominant conceptions of the legitimacy of the status quo’ (p. 73). This article along with the others that we have cited could be seen as a modest contribution to such a discourse. Chameleon resistance is an individualised form of struggle but to challenge the DWD would require collective action (see Smith and Ulus, 2020) along the lines of what Contu (2008) depicts as ‘real’ resistance as its aim would be to disrupt our ‘way of life’ (p. 370). The bio-power exercised through the DWD could be taken up through a counter-wellbeing discourse by ‘a population in resistance’ (Lilja and Vinthagen, 2014: 120). Through its individualising emphasis on ‘self-regulation and self-control’ (Haunschild, 2003: 50), the DWD pushes ‘the pathologies of contemporary work’ and society ‘onto employees’ and individual citizens ‘themselves’ (Fleming and Spicer, 2007: 86). A counter-wellbeing discourse would turn this around and open up debate beyond individual explanations questioning the conditions that generate or exacerbate poor mental health dealing with ‘causes’ not ‘consequences’ (see Haunschild, 2003: 51). As a productive form of resistance, it would target society and therefore go beyond individual organisations.
The UK’s Conservative Government has cited the enormous economic cost of mental health at a time of falling living standards, spiralling government debt and declining productivity. According to its 2022 ‘Mental Health and Wellbeing Plan: Discussion Paper’– ‘The total annual cost of mental ill-health in the workplace to government has been estimated at between £24 billion and £27 billion. The overall annual loss to the economy has been estimated at between £70 billion and £100 billion’. A counter discourse could therefore advocate measures to address conditions that might exacerbate MHCs including unrewarding and insecure work, work intensification and poor terms and conditions of employment, whilst advocating care and counselling services and education regarding mental health and wellbeing on the basis that this could have huge economic benefits. Neo-liberalism and government’s that neglect such issues could be presented through the counter-discourse as the enemy of wellbeing, mental health, the efficient use of resources, competitiveness and productivity. Of course, such a counter-discourse would not occupy ‘a position of exteriority to power’ (Foucault, 1979: 96) because there is no power-free haven from which to resist nor destination to sail. Moreover, without a radical redistribution of resources and new forms of democratic governance it risks reproducing and legitimising the status quo.
Conclusion
The MOS literature that has focused on discourse, power and resistance has shed considerable light on how subjects are produced through power relations and how they resist but limited attention has been given to MHCs. Attending to MHCs can provide additional insights and illuminate processes that we are all caught up in. How many of us struggle, at times, to act and appear ‘well’? Vulnerability must be hidden if we are to secure a job, avoid redundancy, gain promotion or just function. How much more difficult is it then for those with MHCs. Although biopower encourages employees to ‘be themselves’ (Fleming, 2014: 878) as a resource to be utilised, we have observed a paradox hence our respondents used themselves as a resource to mask or hide their condition. To render themselves visible as a ‘normal’ person meant making their MHC invisible – the self, working to hide aspects of itself. Since ‘bio-political regulation seeks to utilize’ subjects ‘unlimited qualities’ (Maravelias, 2018: 335) the project is apt to meet with resistance given that these ‘qualities’ can be used to resist. Chameleon resistance reflects this and giving it a name may help to crystallise experiences that others can share and discuss. Nevertheless, chameleon resistance reproduces the status quo and so other forms of resistance are required such as a counter-wellbeing discourse.
Footnotes
Acknowledgements
The anonymous reviewers and James Wallace provided in-depth and challenging comments on the article during the review process. Their thoughtful and supportive insights deserve gratitude as have helped to transform and considerably improve the original submission.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Hadar Elraz received funding from the ESRC for the empirical research that this paper draws from, award number ES/H032002/1.