
Abstract
Knowledge co-creation at the boundaries of communities of practice (CoPs) can lead to heightened tensions and power struggles. This study examines how power struggles among CoPs can begin to structure knowledge creation processes. Drawing on a qualitative case study of a new medical research project, the study shows how power and knowledge negotiations became manifested through conflicting discursive positioning and coercive power affecting knowledge co-creation efforts. One CoP adopted an authoritative leader role, prioritized their own problem definition and knowledge creation process, and engaged in the peripheralization of other CoPs. The power and discursive moves prevented the development of shared problems and interconnected practices contributing to epistemological suspicion among the participating CoPs. The study offers new insights to research on power dynamics in situated learning and knowing by problematizing the relationship between localized practices and emerging interconnected practices, by shedding light on how discursive positioning and coercive power operate together, and by developing peripheralization and epistemological suspicion as potential explanations for how and why knowledge workers struggle to act on opportunities for knowledge co-creation.
Introduction
The communities of practice (CoPs) literature has advanced research on organizational learning, knowing, and innovating and the role of CoPs in these processes (Brown and Duguid, 1991; Lave and Wenger, 1991; Wenger, 1998). CoPs have been defined as close-knit communities of mutually engaged people who learn together and from each other and share interest in the same problems and practice (e.g. Wenger, 1998; Wenger and Snyder, 2000). Many have criticized the CoP literature for its emphasis on harmony and togetherness and consequently limited focus on tension and conflict (e.g. Contu and Willmott, 2003; Gherardi, 2009; Gherardi et al., 1998; Reynolds, 2000). Research is increasingly showing that knowledge co-creation among CoPs with varied skills, identities, and statuses intensify boundaries and accentuate power tensions (e.g. Contu, 2014; Gherardi and Nicolini, 2002a; Heizmann, 2011; Mørk et al., 2010; Wenger and Snyder, 2000).
This study examines how power struggles among distinct CoPs begin to structure knowledge creation processes by analyzing a new medical research project where members from different areas of research and practice sought to create new medical applications and treatments. From a situated and practice-based view of learning and knowing, knowledge is understood as localized and embedded in the practices of communities (e.g. Carlile, 2002; Contu, 2014; Gherardi, 2000). In medical research directed at interactions across disciplines and increased innovation, CoPs must disentangle their localized practices to create opportunities for interconnected practices (e.g. Mørk et al., 2006; Swan et al., 2002). Yet, in the present case I show how a specific group engaged in the peripheralization of other CoPs, which prevented the development of interconnected practices and created a sense of epistemological suspicion among the knowledge workers. Given the presence of multidisciplinary ways of working, knowledge specialization, and the promotion of innovations across organizational sectors, understanding how such power struggles shape knowledge co-creation is of great importance to researchers and practitioners in the fields of management and organization (e.g. Engstrand and Enberg, 2020; Mørk et al., 2008; Oborn and Dawson, 2010).
More specifically, the objective of the study is to understand how power and knowledge negotiations affect knowledge co-creation in a new collectivity of practice. I conceptualize the medical research project under investigation as a collectivity of practice, because the term refers to “temporary organizations or project groups” that consist of participants who have not met before, go through swift socialization, and have “highly specialized competences, making it difficult to establish shared understandings or a common knowledge base” (Lindkvist, 2005: 1190). It was developed to describe loosely connected social formations that engage in knowledge co-creation at the boundaries of CoPs (Boland and Tenkasi, 1995; Lindkvist, 2005; Swan et al., 2016). While there are conceptualizations such as constellations of interrelated CoPs (e.g. Gherardi and Nicolini, 2002a; Wenger, 1998, 2000), nexus of practice (e.g. Brown and Duguid, 2000; Nicolini, 2011), and networks of practice (e.g. Brown and Duguid, 2001; Roberts, 2006), they depict social formations that are capable of knowledge creation among CoPs due to some common norms, beliefs, and socialization mechanisms. Lindkvist (2005) proposed this term for less cohesive groups where individuals lacked shared practices, understandings, and repertoires and were given limited time to develop them. Moreover, the aim in collectivities of practice is to achieve novelty by fusing elements not connected before, drawing on interactions across boundaries, and venturing into uncharted knowledge territories (Lindkvist, 2005). Therefore, knowledge co-creation is organized around exploratory projects where participants from varied backgrounds come together to “experiment with new knowledge of a path-breaking nature” (Amin and Roberts, 2008: 361). Although the CoP literature has focused on identity formation as part of a shared knowing process (Lave and Wenger, 1991; Wenger, 1998; Wenger-Trayner and Wenger-Trayner, 2020), the term collectivity of practice highlights the pressure to “get the job done” despite weak identification and interconnectedness.
Consequently, I conceptualize the different groups of researchers and practitioners (e.g. bioinformaticians, geneticists, obstetricians) as CoPs and the medical research project as a potential, emerging collectivity of practice. The analysis focuses on ethnographic observations from meetings and qualitative interviews collected over the course of 18 months. Drawing on discursive positioning, I follow in the footsteps of prior studies that have shown how discourse can be used to legitimate knowledge and bring about political effects (Engstrand and Enberg, 2020; Gherardi and Nicolini, 2002a; Grant et al., 1998; Hardy and Phillips, 2004; Heizmann, 2011). I also explore how coercive power contributes to power and knowledge negotiations in knowledge co-creation by enhancing conflicting discursive positioning and preventing the building of coactive power (e.g. Carlsen et al., 2020; Follett, 1924, 1940; Salovaara and Bathurst, 2018).
This approach reveals how power and knowledge negotiations at the boundaries of CoPs become manifested through discursive positioning and the use of coercive power. One CoP took control of the medical research project by adopting an authoritative leader role, prioritizing their own problem definition and knowledge creation process, and peripheralizing the other CoPs. They were able to use this powerful position to push certain groups outward, which prevented the development of shared problems and interconnected practices and contributed to mutual epistemological suspicion.
These findings contribute to power and knowledge negotiations in situated, practice-based understandings of learning and knowing in organizations. First, by utilizing the term collectivity of practice and problematizing the relationship between localized practices and emerging interconnected practices, the study contributes to the debates on the limits of the CoP concept to explain the varieties of situated learning and knowing in organizations (e.g. Amin and Roberts, 2008; Lindkvist, 2005; Roberts, 2006). Second, the findings offer new insights to existing research on power struggles by showing how mechanisms of discursive positioning in power/knowledge claims are reinforced by coercive power moves (e.g. Contu, 2014; Fox, 2000; Heizmann, 2011; Heizmann and Olsson, 2015). Finally, the concepts of peripheralization and epistemological suspicion that emerge from the analysis provide potential explanations for how and why knowledge workers struggle to act on opportunities to engage in knowledge co-creation. While the CoP literature has focused on the idea of legitimate peripheral participation where newcomers engage in peripheral tasks before moving toward the core community (Lave and Wenger, 1991; Wenger, 1998), peripheralization shows how CoP associated power can be used to push other groups outward and, in this way, exclude them from knowledge co-creation. Epistemological suspicion, in turn, draws attention to the importance of the affective dimension in situated learning and knowing (e.g. Contu, 2014; Kofman and Senge, 1993; Vince, 2001).
The paper is structured as follows. The literature review frames the analysis of how CoPs attempt to form a collectivity of practice, and the kinds of power and knowledge struggles that may develop. I then describe the research setting and the methodological and analytical approaches. The findings on power and knowledge negotiations begin by describing how the bioinformaticians took control of the project and how the other CoPs responded to this in the shared project meetings. I conclude by discussing the implications of the findings to knowledge co-creation and power and knowledge struggles in situated learning and knowing.
Theoretical background
Communities and collectivities
The term CoP was initially defined as “a set of relations among persons, activity, and world, over time and in relation with other tangential and overlapping CoPs” (Lave and Wenger, 1991: 98). Or, as Wenger et al. (2002: 4) later put it, “groups of people who share a concern, a set of problems, or a passion about a topic and who deepen their knowledge and expertise in this area by interacting on an ongoing basis.” The concept included the idea of varied forms of participation: through legitimate peripheral participation novices take part in simple tasks at the edge of the community, while masters participate in key activities at the center (Wenger, 1998). Yet, what binds different members together is their shared practice (Wenger and Snyder, 2000), understood as “a set of frameworks, ideas, tools, information, styles, language, stories, and documents” (Wenger et al., 2002: 29). As members engage in shared practice, they develop the three structural elements of a CoP: mutual engagement, joint enterprise, and shared repertoire (Wenger, 1998). The three elements refer to what members do and how they work together, the topics they are passionate about, and the concepts and artifacts they create (Pyrko et al., 2017).
The CoP literature has paved a way for a rich and closely related research stream concerned with the practice-based view of learning and knowing in organizations (e.g. Corradi et al., 2010; Nicolini, 2013). In this context, practice is perceived as “a system of activities where knowing is not separate from doing” (Gherardi, 2000: 251). Moreover, it has been proposed that the more people interact meaningfully with other members of the group and participate in the shared practice, the more they invest their identity in the community (e.g. Gherardi et al., 1998; Nicolini and Meznar, 1995; Thompson, 2005). However, when knowledge is understood as localized, embedded, and invested in specific practices, sharing it across CoPs can become difficult (Brown and Duguid, 2001; Carlile, 2002, 2004; Contu and Willmott, 2003; Wenger, 1998; Wenger et al., 2002).
Scholars have argued that the term CoP can be problematic for understanding temporary, loosely connected teams where participants rarely share identity and practice the way they do among established CoPs (Amin and Roberts, 2008; Boland and Tenkasi, 1995; Lindkvist, 2005; Swan et al., 2016). While there are existing conceptualizations for describing more loosely connected social formations, I found it difficult to apply them to the present case. One of these concepts is “networks of practice” which are looser social formations, but their members are oriented toward the same practice (e.g. Brown and Duguid, 2001; Roberts, 2006). Heizmann (2011) used the concept to analyze HR practice within a large insurance company. A “constellation of interrelated CoPs” identifies shared historical roots, enterprises, artifacts, and interactions as its key characteristics (Lindkvist, 2005; Wenger, 1998, 2000). Gherardi and Nicolini (2002a) utilized the concept in their study of safety in a construction site, arguing that practice ties distinct CoPs, such as site foremen and engineers, together and performs the constellation of communities. In the constellation being studied, site foremen and engineers had distinct identities, vocabularies, and practices, but they were still able to contribute to safety, the shared objective in the construction site. Finally, the concept “nexus of practice” conveys the idea that the site of knowing is not a single practice but a pattern of connected activities. Analyzing the field of telemedicine as a nexus of practice where activities where connected and often dependent on each other, Nicolini (2011: 615) stated that the organization and form of these arrangements stem from “specific history and interest-led projectuality.”
While these conceptualizations acknowledge the presence of different CoPs, identities, and practices, they imply that there is some level of shared practice, objective, or history that motivates groups to participate in the loosely connected social formations. As such, they are not well suited for explaining knowledge co-creation in emerging, temporary, project-based, and multidisciplinary teams. Rather than developing another concept for describing such groups, I draw on Lindkvist’s (2005) ideas on the relationship between CoPs and a collectivity of practice. Members of a CoP share history, understandings, and problems, but when participating in a collectivity of practice their collaborative efforts are organized within a temporary working group and directed toward a potentially shared goal. Lindkvist (2005: 1200) said that those participating in a collectivity of practice had “a very limited overlap of knowledge bases, and little time to erect communal knowledge during the lifetime of a project.” He argued that researchers should explore the potentially dynamic relationship between CoPs and a collectivity of practice as the two were processually linked.
To summarize, I have considered different terms for describing loosely connected groups in the CoP literature and explained why I draw on the relationship between established CoPs and a collectivity of practice (Lindkvist, 2005). Next, I discuss the significance of power and knowledge negotiations in the context of an emerging collectivity of practice.
Power and knowledge dynamics in an emerging collectivity
The CoP literature has been criticized for overemphasizing harmony and togetherness while downplaying conflict and tension (e.g. Gherardi, 2009; Gherardi et al., 1998; Reynolds, 2000). Contu and Willmott (2003) even pointed out that the CoP concept was defined using harmonizing language (e.g. joint enterprise, shared repertoire), which left little room for exploring the role of social tensions and power struggles. Scholars have addressed this research gap by showing how knowledge sharing, knowledge creation, and innovation processes intensify boundaries, lead to power struggles, and enhance conflict (e.g. Contu, 2014; Gherardi and Nicolini, 2002a; Heizmann, 2011; Mørk et al., 2010; Wenger and Snyder, 2000). Knowledge workers’ identities, worth, and skills seem to be at stake when they engage in knowledge creation at the boundaries of different CoPs (e.g. Contu, 2014; Heizmann, 2011; Mørk et al., 2010; Thompson, 2005). Mørk et al. (2010) studied evolving power relations in innovation processes in medicine and showed that the implementation of new innovations resulted in varied experiences of empowerment and disempowerment among CoPs thus questioning traditional understandings of mastery in the literature. Drawing on networks of practice, Heizmann (2011) observed that organizational power/knowledge struggles impacted participation and challenged knowledge sharing between geographically dispersed HR practitioners. Studying tensions and creative abrasions in design work, Contu (2014) advanced research on power dynamics among groups that have highly varied skills, ideas, and ways of seeing a problem.
These studies highlight that power and knowledge are inherently linked and emerge from interactions between people from different CoPs. Foucault (1980) argued that knowledge that is accepted as “truth” and that is unquestioned conceals a history of power that is interwoven with an established field of knowledge. As Carlsen et al. (2020: 831) pointed out in relation to Foucault’s views on the connections between power and knowledge, “it is not so much that knowledge is power but that power relations frame knowledge.” Moreover, Foucault (1979; 1980) saw power existing in a network of relations, where everyone is caught and where power is in constant motion. From this view, power emerges from social interactions between knowledge workers from different CoPs as they negotiate meaning in relation to power/knowledge relations (Heizmann and Olsson, 2015).
Foucault’s relational understanding of power combined with a focus on practices, and his view that power and knowledge are mutually constituted in discourse, have made his work relevant for practice-based studies on power and knowledge dynamics in learning and knowing (e.g. Contu and Willmott, 2003; Foucault, 1980; Fox, 2000; Heizmann, 2011). Relatedly, discursive positioning has been seen as a strategy to legitimate knowledge within CoPs (Gherardi and Nicolini, 2002a; Grant et al., 1998; Hardy and Phillips, 2004; Heizmann, 2011). If a CoP develops a regime of truth (Foucault, 1979), its discourses can take on a dominant role and affect which knowledge practices are seen as valid. Heizmann (2011) noted that such discursive positionings are concerned with processes of differentiation and separation from other CoPs. As such, displays of power also relate to the identity formation of those engaging in the practice (Fox, 2000; Heizmann, 2011; Wenger, 1998).
I complement Foucault’s views on power/knowledge with Follett’s ideas on coactive and coercive forms of power. For Follett (1924, 1940), power was ideally coactive power-with, as opposed to hierarchical power-over, and it evolved from the integration of diverse groups working together toward joint discovery. At times of conflict, authoritative power-over positions were unhelpful as creative solutions depended on engagement from multiple participants. Follett (1924, 1940; see also Salovaara and Bathurst, 2018) argued that it was the situation, or social context, that held authority and determined an appropriate role for each participant. The idea that a single individual exercised power over others was absurd and it was the leader’s responsibility to make sure that power was exercised with a team rather than as a personal power. Such a form of power would support “higher synthesis,” where participants would search for, embrace, and take advantage of the differences among their knowledge and skills (Follett, 1919, 1998: 96). As Salovaara and Bathurst (2018: 183) noted, Follett saw this as “a process of negotiating that went beyond compromise and that actively engaged parties in creating something new and previously unknown within their organizations.” This conceptualization of power aligns well with an emerging collectivity of practice where CoPs interact and collaborate across boundaries to achieve novelty by combining knowledge not connected before (Amin and Roberts, 2008; Lindkvist, 2005). Whereas coactive power practices include “letting-go, engaging others, facilitation, and horizontal leadership” (Salovaara and Bathurst, 2018: 194), coercive displays of power can hamper knowledge co-creation by closing down opportunities for collaboration, shared problem definitions, and alignment of practices.
From the perspective of discursive positioning and coercive power, the analysis shows how power and knowledge are performed in a collectivity of practice and how these political moves affect knowledge co-creation. Next, I will describe the empirical context and research methods.
Empirical context and research methods
The findings presented in this article are part of a more extensive research project on a transdisciplinary medical research organization located in an American research university. The organization, led by a group of senior medical researchers, was formed when it received a major grant from a foundation that was committed to supporting research on understanding and developing new solutions to the problem of premature birth. The research proposal for the organization, which the senior medical researchers prepared, consisted of four distinct transdisciplinary teams and in the present study, I analyze the development of one of these projects.
Empirical material
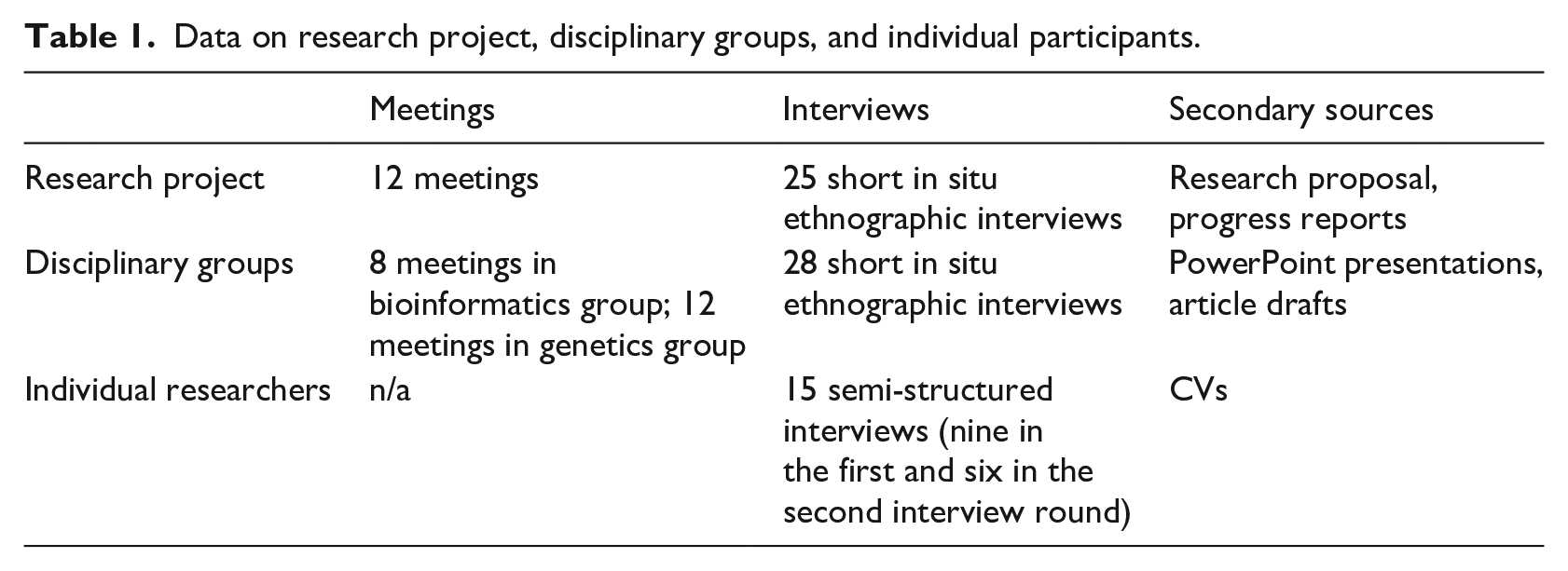
The qualitative case analysis focuses on a project where the goal was to study biological markers related to premature birth and potentially use them in the development of new ways of diagnosing and treating patients. Similarly to prior studies seeking to uncover the nature of situated practice (e.g. Brown and Duguid, 1991; Contu, 2014; Lave and Wenger, 1991), I employed an ethnographic approach to analyze the project (Hammersley and Atkinson, 2007; Jacobson, 1991). In line with ethnographically oriented research, the data collection involved different types of evidence—non-participant meeting observations, recordings and transcripts from meetings, interviews, and documents—collected over the course of 18 months (Yanow and Schwartz-Shea, 2006). Table 1 summarizes the different types of data the article draws on.
Data on research project, disciplinary groups, and individual participants.
Medical research project
My primary source of data includes ethnographic observation from the project meetings supported by recordings and transcripts of those meetings. I also draw on short in situ ethnographic interviews conducted before and after the meetings with informants sitting close to me or with whom I walked out of the meeting room toward coffee shops or bike racks (Hammersley and Atkinson, 2007; Jacobson, 1991; Spradley, 1979). In situ ethnographic interviews were not recorded and transcribed, but they were reported in the fieldnotes. I observed, recorded, and transcribed all 12 project meetings occurring since the formation of the center. I took extensive fieldnotes about the scientific content to track how the project evolved, the descriptions of knowledge practices, and the interactions and exchanges between the participants. As most meeting participants had their laptops in front of them, it was feasible to write quick fieldnotes to a Word document and then write out the observations in detail after the meeting. When waiting for the meetings to begin and when packing up after meetings, the short in situ ethnographic interviews allowed me to ask clarifying questions on topics that had been discussed.
The research project had monthly meetings, but occasionally a few months passed between meetings due to academic breaks and the participants’ busy schedules. The number of attendees at project meetings varied between seven and eleven. The typical participants comprised a senior scientist working in the field of bioinformatics, his two graduate students, a project administrator, and researchers from genetics and obstetrics. The meetings lasted between 60 and 90 minutes and the transcripts were between 27 and 40 pages long. On the meeting transcripts, speakers were identified using codes (e.g. ID-2, ID-21) and the same codes are used in the analysis.
Semi-structured interviews and documents
As part of a larger research project, I interviewed members of the research organization just as it formed and 2 years later. Here, I draw on 15 interviews relevant to the project: nine from the first round, six from the second. In the first interview round, the interviews were conducted with the bioinformatics group’s team leader (male) and two junior researchers from his team (male and female). In addition, interviews were conducted and analyzed with a project administrator (female) and five participants from other fields of research and practice (genetics and obstetrics; one female and four males) who participated in team meetings (in total, nine interviews from the first round). In the second interview round, interviews were conducted with six informants from the first round: the bioinformatics group’s team leader (male), one junior researcher from the team (male), and four active meeting participants from genetics and obstetrics (one female, three males).
The interviews were semi-structured and included both open-ended and close-ended questions. The protocol covered questions relating to the interviewee’s training, academic career and research themes (informed by their CVs), perceptions of the problem of premature birth, and experiences of participating in multidisciplinary medical research as part of the research organization. The interview data is used in the analysis to provide a better understanding of the varying perspectives presented as part of the power and knowledge negotiations in the shared meetings. I rely on secondary sources—the research organization’s research proposal, progress reports, and project evaluations—to further ground the observations.
Disciplinary groups
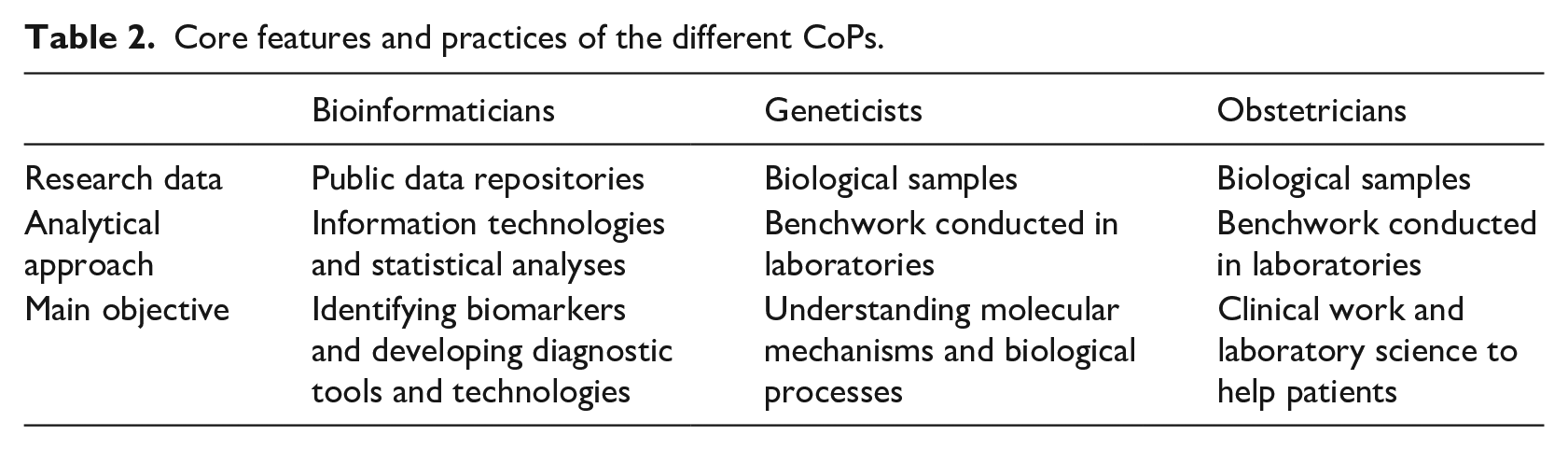
I gained a general understanding of how the disciplinary groups (e.g. bioinformaticians, geneticists, obstetricians) typically worked through the semi-structured interviews and the ways in which the groups presented their knowledge in the shared meetings. During data collection, I noticed a particular tension between the bioinformaticians, who relied on information technologies and statistical analyses to analyze information in public data repositories, and the geneticists and the clinician investigators in obstetrics, who conducted traditional benchwork analyzing biological samples in laboratories.
To develop a better understanding of this tension, in the next phase of the data collection I familiarized myself with the home laboratory of the bioinformaticians, who had taken the role of leading the project, and observed eight of the team’s research group meetings and took fieldnotes coupled with in situ ethnographic interviews (Hammersley and Atkinson, 2007; Jacobson, 1991; Spradley, 1979). I similarly collected data on 12 research group meetings in a genetics laboratory—also conducting in situ ethnographic interviews—whose researchers sought to collaborate with the bioinformaticians. At the research group meetings, I was able to gather some of the PowerPoint presentations and article drafts that the researchers presented.
These additional observations among the two research groups were undertaken to develop an in-depth understanding of the core features and practices of the participating disciplinary groups, which I conceptualize as CoPs, and the issues that made the formation of the collectivity of practice difficult. Moreover, these observations allowed me to explore an emerging theme in the project meetings (e.g. epistemological suspicion). Table 2 summarizes the core features and practices of the distinct CoPs.
Core features and practices of the different CoPs.
Analytical techniques
As I had entered the field with a broad aim in mind—wanting to study how the project evolved over time and how collaboration was organized across boundaries—I approached the data inductively. Following principles of inductive research, the analysis iterated between data collection, data reduction and representation, and conclusions and verification (Glaser and Strauss, 1967; Miles and Huberman, 1984; Strauss and Corbin, 1998). Although the analysis developed iteratively and moved across different types of evidence, it consisted of two main phases.
First, I started by doing initial coding of the fieldnotes from both the project and the disciplinary meetings, meeting transcripts, and semi-structured interviews to develop a preliminary account of the case (Charmaz, 2006). The benefit of having both the fieldnotes and the meeting transcripts was that I was able to go back to what was said at a specific meeting and triangulate my observations and interpretations in the fieldnotes. After several iterative rounds of initial coding, I was able to identify three main descriptive themes in the account of the case. The themes that emerged revealed, first, how the bioinformaticians, who positioned themselves as the main agent in knowledge co-creation, narrated their knowledge practices (e.g. problem selection, data, analytical approaches, and research outcomes) and connected it to the research project on premature birth. Second, the themes showed how the other participants positioned their knowledge practices in relation to the bioinformaticians’ approach and how they identified opportunities for contributing to the shared project. Third, the descriptive themes revealed how the bioinformaticians responded to the attempts of the collaborators to position their knowledge as part of the project.
In the second phase of focused coding (Charmaz, 2006), I concentrated on how CoPs positioned themselves in power and knowledge negotiations and how these positionings developed in the project meetings. I also analyzed the semi-structured interviews and fieldnotes from disciplinary research group meetings to understand the epistemological justifications for different perspectives. As my analytical focus was on discursive positioning and different forms of power, I zoomed in on descriptions of and reactions to the bioinformaticians’ knowledge practices as this was the baseline activity in the project. When interrogating the data, I asked, how are the participants reflecting on the practices of the bioinformaticians and positioning their knowledge in relation to it? What kinds of differences are drawn, how, why, by whom, and with what outcomes?
Bioinformaticians as the leaders of knowledge co-creation
The analysis begins with a description of the bioinformaticians’ knowledge practices and how they connected them to the study of premature birth. As bioinformaticians were assigned the leader role in the initial proposal to form the research organization focusing on premature birth, they were able to prioritize their own practices and affect the abilities of other CoPs to contribute to knowledge co-creation. The analysis is based on interviews conducted with bioinformaticians, observations conducted in their research group meetings, and secondary sources.
Knowledge practices in bioinformatics
Instead of traditional laboratory benchwork and conducting analyses on actual biological samples, bioinformaticians store, search, and manage existing biological data using information technologies and aiming to reveal patterns and statistical trends in the data as a whole (Stevens, 2011). The bioinformaticians of the present study sought to identify the kinds of biomarkers that were associated with particular diseases by using information technology to analyze large amounts of publicly available data. The public databases, which contain information on previously conducted and published experiments, allowed the bioinformaticians to work with large amounts of data and search for candidate biomarkers that were associated with a disease of interest. As one bioinformatician explained: We use a lot of public data. That’s data that has been generated by other scientists in their labs and that have been published, and they upload the data online to these depositories. Most of where my data comes from is the Gene Expression Omnibus, which has thousands and thousands of experiments. The beauty of that is you can combine all of these data from other people that you didn’t have to work hard to make yourself. A difficulty with that is you don’t always trust other people’s data, but if you combine like 20 data sites and you take the average, then that’s probably more robust. [ID-15]
Gene Expression Omnibus is a public data repository that contains functional genomics data. As the interviewee explained, when it came to data repositories, the bioinformaticians counted on volume: that is, by analyzing the information resulting from a mass of prior experiments they were likely to produce accurate findings. Because the team utilized large volumes of genomic, genetic, and phenotypic data, they had developed computational tools for automatically combing the databases. Through this approach, they could study any health problem, and, in fact, their prior research projects had focused on diverse conditions: obesity, diabetes, and different types of cancers. One bioinformatician described the freedom to choose the research question as something that distinguished them from other computational laboratories: So, if I had a question about which diseases have this gene in common, that’s different than saying I’m going to study this kind of cancer and figure out what kind of genes are important to this kind of cancer. We are not limiting ourselves to any diseases or any types of data, but we say: what’s the question I have? Then I go find the data that I can use to answer the question. [ID-15]
When describing his research group, the team leader even said: “We have a motto in the lab. Outsource everything but the question” [ID-2]. This meant that they could outsource everything else: literature reviews, data, and validation experiments.
After identifying a biomarker that was correlated with a given disease, the bioinformaticians would find a way to validate it in actual biological samples using laboratory science approaches. As the team leader explained: We start in a deductive way. We think something [biomarker] in this measured dataset is going to correlate with something, let’s say a disease. Let’s say we usually find something. Then we need to prove it, so we have to show it in another [data] set or actually measure it in real biological samples. [ID-2]
The bioinformaticians could either look for a researcher to collaborate with, who could analyze biological samples from individuals suffering from the disease of interest and see if the biomarker could be confirmed, or they could buy biological samples from independent companies and outsource the analysis and validation process. Usually, they adopted the latter approach, because it made the validation process much faster, as the team leader noted: “For example, cancer samples, like blood samples, serum, plasma, urine, you can purchase all of those. Pathology samples, we also collaborate with folks on campus, but it is so much faster to just order it now on the Internet.” [ID-2]
The final step in the knowledge creation process was the development of a diagnostic test on the basis of a validated biomarker: “What that means is we try to use informatics tools in genomics to make inferences about disease and what we would like to do is transfer or translate our discoveries into clinical practice. How can we quickly find drugs that may be administered as therapies using genome wide data? How can we improve clinical decision-making? How can we make better diagnostics for diseases?” [ID-21]. They were interested in starting companies based on the diagnostic tools the identification and validation of biomarkers had helped to create. As the team leader noted, “We start a lot of companies because I think it’s a higher definition of having utility to people. There are a lot of folks on campus that don’t do this. They just run a standard lab” [ID-2].
Bioinformaticians adopting a leader role and prioritizing their own practice
When agreeing to lead the research project, the bioinformaticians planned to follow their own research process and practices rather than engaging in knowledge co-creation with other CoPs. Being members of the research organization, however, they could not work only among themselves, but they had to meet with the other CoPs on a regular basis in shared project meetings. The team leader had a preconceived notion, which can also be seen as a sign of epistemological suspicion, that there was no real potential for knowledge co-creation, observing, “It [the research center] is more pediatrics focused, and obstetrics and gynecology. I’m going to use them as an audience for our findings, more than collaborators. They’re going to come to the meetings, but I’m not sure how involved they want to be” [ID-2]. Because he thought that collaborating with these CoPs was going to be futile, he assigned them the more limited role of “us[ing] them as an audience for our findings.” The role of an audience member is strikingly different from that of a collaborator: an audience member reacts to research; she does not participate in its creation.
The bioinformaticians planned to conduct genome-wide association studies to identify biological markers associated with premature birth. This form of study scans biological traits to find genetic variations associated with a disease of interest and researchers then develop strategies for detecting, treating, or preventing the disease on the basis of the findings. Because premature birth is a complex syndrome associated with many different pregnancy-related diseases, the bioinformaticians narrowed the research question by focusing on one specific disease, preeclampsia, which is a pregnancy complication characterized by high blood pressure and organ damage. It usually begins after 20 weeks of pregnancy and, if left untreated, can lead to death for both the mother and the baby. The only known treatment for preeclampsia is early delivery, which results in premature birth. This focus for the project was decided prior to the shared project meetings, which meant the other CoPs could not influence the problem definition. One bioinformatician noted in an interview, “We started out looking at preeclampsia because it’s a really big problem, and it’s also a narrower problem than all of premature birth” [ID-15]. The team leader explained, “People argue whether that’s really premature birth or not. I happen to think it is. I think it’s a big problem” [ID-2]. By “people” he referred to clinicians who treated patients suffering from preeclampsia. Before conducting analyses on the available biomedical data, however, it was impossible for the bioinformaticians to know what kinds of markers they would find (e.g. biomarkers for diagnosis, disease progression, or treatment): We’re hoping to find genes that are expressed differently between women that have preeclampsia and that don’t have preeclampsia. These genes could fall into one of two categories. One is that they indicate the presence of the disease; they’re good for diagnosis. Another category is that they’re somehow related to the cause of the disease and tell you more than just that the disease is there or it’s not, but they functionally lead to something going wrong that leads to the disease manifesting. Those can be the more interesting genes. [ID-15]
While the interviewee acknowledged that the goal was to find biomarkers that could be used in the development of new treatments for preeclampsia, he also stated that finding “genes that deal with the cause and the function of the disease is much harder.”
Power and knowledge negotiations in an emerging collectivity of practice
The other CoPs joined the research project to discover that the bioinformaticians had decided to follow their own problem definition and knowledge creation process. Still, from the perspective of these CoPs, two instances appeared as obvious opportunities for knowledge co-creation. First, geneticists who routinely analyzed biological samples in laboratories could help with contextualizing the analysis and validating biomarkers. Second, clinician investigators in obstetrics, who not only treated pregnant women but also researched pregnancy-related diseases, could help with developing diagnostic tests that were needed in medical practice. The following sections are based on an analysis of the shared project meetings. They demonstrate power and knowledge negotiations through discursive positioning and coercive power moves as the bioinformaticians ignored these opportunities for knowledge co-creation and peripheralized the geneticists and the obstetricians. Realizing they were assigned to a limited role, these CoPs began to draw on conflicting discursive positioning when interacting with the bioinformaticians. These interactions created a sense of mutual epistemological suspicion, that is, overall skepticism toward a foreign community’s knowledge practice and its ability to contribute to knowledge creation within and beyond the project.
Bioinformaticians peripheralizing the geneticists
In the normal working conditions in their own research group, the bioinformaticians sought assistance from laboratory scientists experienced in benchwork—either through collaboration or purchasing their analytical services, as described previously—who could help them with validating a biomarker for a given disease they had discovered. In the present project, the geneticists could similarly have contributed by contextualizing the analysis and validation of biomarkers, which they themselves recognized as an opportunity for knowledge co-creation. In these instances, the bioinformaticians relied on discursive positioning to differentiate their research approach from other available approaches. Through the use coercive power, they could close off discussions on suggestions that differed from their chosen research process.
As a first step in peripheralization of the geneticists, the bioinformaticians introduced their knowledge creation process and explained how it would be applied in the study of premature birth. At one of the first shared meetings, the team leader explained that their strategy was to identify the biomarkers most associated with preeclampsia, “Someone’s already gotten the human sample, someone’s already run the microarrays, and all the raw data is available for intersection here. That gives us a head start” [ID-2]. Another bioinformatician added, “This [analytical approach] gives us the advantage of combining all these different samples that are all measured in placenta [. . .] and we can just leverage all of these data sets and try to find the genes that are consistently implicated in preeclampsia” [ID-15]. These statements highlight how the bioinformaticians positioned their knowledge practices as faster, cheaper, and more comprehensive than traditional laboratory science. As the bioinformaticians already had access to data available in the public data repositories and had developed analytical tools from prior research, they argued they could begin research immediately rather than waste time in gathering, preparing, and analyzing biological samples.
By prioritizing their own knowledge creation process, the bioinformaticians closed off more exploratory approaches in the shared research effort. When it became apparent that opportunities for knowledge co-creation were limited, the geneticists took a critical discursive positioning challenging the bioinformaticians. An investigator who ran his own laboratory and was knowledgeable of preeclampsia responded to the team leader’s description of the project by reminding those present of the kinds of researchers available to the bioinformaticians as part of the project. He questioned whether the bioinformaticians had considered possible biological pathways, asking, “Do you need those of us in the room that know the various [biological] pathways and what the signals [biomarkers] are to let you know what that [candidate biomarker list] should look like?” [ID-27]. Biomarkers are signals of biological processes related to a disease that can provide information on the kinds of processes occurring in human body during an illness. Based on prior research, as this speaker suggested, those knowledgeable on the topic could theorize which biomarkers made sense and which could reveal something new about preeclampsia. The bioinformaticians responded, however, that they focused on “data-driven candidates,” which meant that their large data sets would reveal important biomarkers with or without prior knowledge of biological pathways and processes. While the previously mentioned researcher took the position that prior knowledge of preeclampsia would help the bioinformaticians in their search for answers—and offered to participate in knowledge co-creation—the bioinformaticians’ position implied that prior knowledge could bias the search for answers. The data would allow the bioinformaticians to see true patterns, independently of what other researchers thought they already knew about the disease. Through this discursive positioning, the bioinformaticians differentiated their own practice as superior to traditional laboratory science and, through coercive power, closed off the discussion.
Such instances sparked further critical discursive positioning on the side of the geneticists. In addition to their issues with the contextualization of information gathered from the data repositories, they were concerned about the analytical strategy, which ignored how the samples they used were created in the first place. They insisted that knowing the details of the biological samples was imperative for reliable results: the specific part of the placenta which had been sampled, for example, was a critical detail in their experience. When a bioinformatician discussed the experiments in the data repositories on which they would rely, a geneticist asked, “Is it really placentas that were being sampled and not placental bed? Bed is different than placenta. Bed is essentially maternal surface” [ID-31]. This question, presented as an audience member rather than someone engaged in knowledge co-creation, highlighted the geneticist’s knowledge in relation to the bioinformatician’s, but also implicitly offered it for consideration in the shared project. The bioinformatician responded that he did not know the answer and went on with the presentation. Later, during the same meeting, another geneticist pointed out that it was important to know what part of the placenta was sampled in the initial analysis: It might be worth to see what they are actually sampling [in the selected studies from the dataset]. Is it a big core through the center [of the placenta] or are they scraping something off [from the surface of the placenta]? You could be getting a core that has mostly epithelial cells on it. They can be getting a core that has trophoblasts or different kinds of other cells, so just be aware, placental cells are really heterogenic. [ID-1]
A bioinformatician replied that various kinds of placenta samples were present in the data they had selected from the data repositories; they had not focused on any one cell type. Another argued that although the geneticist had made a valid point, they should not worry about it, because the reliability in their analyses came from the volume of data, not the details. Again, the bioinformaticians conveyed that the suggestion was futile and that the geneticists’ knowledge would not provide additional value for the project.
The bioinformaticians’ knowledge creation process drawing on data repositories, information technology, and statistical analyses produced results quickly, which they saw as an advantage compared to traditional laboratory science, the core expertise of the geneticists. Within a few months, they had identified a biomarker for preeclampsia and were considering how to validate it. At this point, the geneticists felt that testing the presence of a biomarker in “real” biological data would ensure that the biomarker was not discovered from the data repositories by chance. One suggested that the research organization should collect biological samples from patients in the university hospital’s clinics. This would be easy as they had other data collection efforts already ongoing. The bioinformaticians agreed in principle but thought that would needlessly slow their research process down. They made the decision to outsource the work and bought placenta samples from a private company, thus further closing off the opportunity for knowledge co-creation.
Bioinformaticians peripheralizing the obstetricians
No company had developed a diagnostic test for preeclampsia at the time of my data collection, which the bioinformaticians saw as an opportunity. In current medical practice, clinicians would diagnose preeclampsia based on the pregnant woman’s symptoms, such as high blood pressure or protein in urine, and the only known treatment was early delivery. Because preeclampsia threatens the lives of both mother and baby, clinicians must make quick decisions about early deliveries and sometimes they misdiagnose the symptoms. The bioinformaticians’ stance was that if they found a biomarker for preeclampsia and developed it into a blood test, the discovery could be used in preventing unnecessary early delivery, which was a significant problem in current medical practice.
This described discursive positioning involved the work of the obstetricians, who diagnosed and treated pregnant women suffering from the condition, as well as studied it. From the start, some of them questioned the bioinformaticians’ perspective on the value of a diagnostic test for preeclampsia. When the bioinformaticians presented their ideas about developing the biomarker into a diagnostic test, two obstetricians (ID-32 and ID-16) discussed its value.
ID-32: Can I ask—as a clinician, I can diagnose preeclampsia for 10 cents doing just a urine analysis and a blood pressure cuff. Why do I need a chip on an iPad and an iPhone and a whatever to diagnose this?
ID-16: I would strongly disagree with what you just said. I can think of a woman at 28 weeks that we shared [as a patient] who had low platelets, who had elevated blood pressures, who had protein in her urine—
ID-32: But those are the 5% that are gray. Those are the 5%.
ID-16: The baby was a 28-weeker who got delivered because someone thought she had preeclampsia when she could have had it because of the medication she was on, so it’s the cases that are confounded where it matters. I agree that most often preeclampsia looks like that’s what it is, but there are times when you are pushed into a corner of delivery very early and it may not be preeclampsia.
ID-32: I would say it’s few and far between.
The obstetricians disagreed about the value of the kind of diagnostic test that the bioinformaticians’ proposed to develop, a decision that the bioinformaticians had made without consulting the obstetricians. One argued that the existing practices which included urine analysis and a blood pressure test were still effective ways to diagnose preeclampsia, whereas the other noted that a diagnostic test might prove to be useful in cases where the symptoms were caused by something else.
As the leaders of the project, the bioinformaticians could ignore this debate and continue to argue that a diagnostic test for preeclampsia would improve the obstetricians’ practice; it was a better tool than basing an early delivery decision on various symptoms. A few months later, one bioinformatician again took the position of criticizing current medical practice: “There’s currently no test on the market for preeclampsia. What people [obstetricians] come to do is very non-specific. They measure blood pressure, other things. What we want is a very accurate test for preeclampsia earlier on in pregnancy” [ID-15]. This time the obstetricians—the “people” who were the potential end-users of this test—took a collective critical discursive positioning. They did not appreciate the description of their practice of diagnosing preeclampsia cases as “non-specific,” and they were not convinced a preeclampsia test would improve treatment and care. As an illustrative example of the discursive positioning of the obstetricians, one responded to the bioinformaticians’ argument, saying, “Clinically speaking, [this is] not necessarily so entrepreneurial” [ID-32]. This suggested that from the perspective of those who were engaged in clinical practice, the test was not innovative or needed.
Obstetricians repeatedly took another position in response to the proposed value of a diagnostic test: if and when preeclampsia cases were confirmed by the tool developed by the bioinformaticians, the treatment would still be early delivery, resulting in a premature baby. Therefore, the bioinformaticians’ work would not have an impact of the rate of premature birth, which was the main challenge the research organization was supposed to address. One obstetrician presented and reflected on this critique particularly well and urged the bioinformaticians to think about the biological mechanism for preeclampsia rather than simply identifying a biomarker that was associated with it: A diagnosis of preeclampsia is not hard and it’s a clinical diagnosis. The proteins and genes that you find associated with it are ones that would help you in understanding the biology of preeclampsia and potentially developing some therapy, because you would want to counteract that biology. When you talk to obstetricians about all of this, they will say, ‘Oh, there’s no problem.’ Once someone has preeclampsia you deliver them. That’s the cure. But that also means the babies are born too soon. If there were a better treatment it would be nice to have, although you would have a hard time to convince obstetricians not to deliver women who had preeclampsia. From the idea of trying to prevent premature birth right now, prevent preeclampsia and you prevent premature birth, but to diagnose preeclampsia, you just give us [obstetricians] another reason to deliver early. [ID-33]
His position was that a diagnostic tool for preeclampsia would give obstetricians another reason to deliver a baby early, but if they could understand the biological processes behind preeclampsia—which was a core feature of the expertise of those engaging in laboratory science—they could develop new strategies for preventing it. Through this discursive positioning, he questioned the value of the diagnostic test. Despite agreeing that understanding what causes preeclampsia was important, the bioinformaticians’ position was that with their knowledge creation process, they had achieved the goals and succeeded, claiming, “Our original goal was to find some biomarkers. I think as icing on the cake, maybe even the new cake, is figuring out the mechanism of how preeclampsia happens. To figure out why people get this is way beyond what we were thinking” [ID-2].
The previously described power and knowledge negotiations explain how and why the development of shared problems, understandings, and interconnected practices became impossible in the emerging collectivity of practice. Figure 1 summarizes the main power and discursive moves of each CoP before I explain in detail how they contributed to mutual epistemological suspicion.
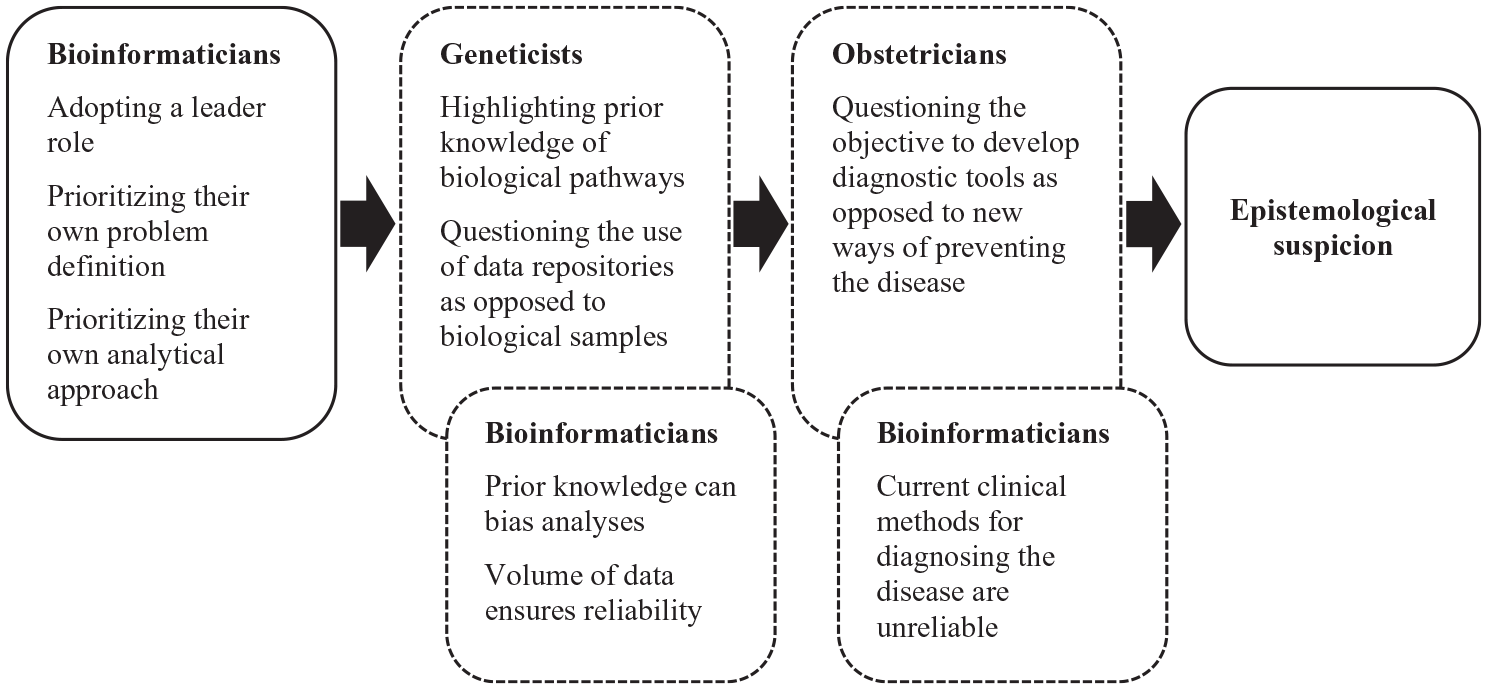
Power and discursive moves of each CoP.
Epistemological suspicion
The power and knowledge negotiations in the shared meetings contributed to a growing sense of epistemological suspicion among the participating CoPs. While epistemological suspicion can be an affect that is not expressed openly, in this study the CoPs expressed their skepticism toward foreign knowledge practices in the shared meetings as well as reflected on it in the interviews.
The bioinformaticians seemed to experience some epistemological suspicion from the start of the project as they immediately peripheralized the other CoPs assigning them as audience members without considering the value of their knowledge practices for the project. With the help of coercive power, they could act on this epistemological suspicion and prioritize their own knowledge creation process. These instances of peripheralization led to a growing sense of epistemological suspicion among the geneticists and the obstetricians. Feeling frustrated, one obstetrician claimed in an interview that the bioinformaticians had never considered what discoveries had already been made on preeclampsia in obstetrical research, observing, “The bioinformatics stuff needs to be framed much more directly with the people looking at placental pathology in the obstetrics world [. . .] The bioinformaticians’ work is not grounded in the obstetrical science adequately” [ID-29]. Despite their efforts to express what was already known about preeclampsia, the bioinformaticians did not see value in this prior knowledge and peripheralized the obstetricians from knowledge co-creation.
Epistemological suspicion grew even stronger among the geneticists who relied on traditional laboratory benchwork. At the center of the suspicion was how the different CoPs’ knowledge making practices differed with regards to biological data. This issue—what biological matter was being analyzed and how—sheds light on the importance of both the social and the material aspects of learning and knowing (e.g. Fenwick et al., 2012; Gherardi and Nicolini, 2002b). Emphasizing how the bioinformaticians analyzed electronic forms and not actual biological samples, one researcher said in an interview, “They [bioinformaticians] use existing data to analyze, discover, and to pick apart whatever it may be they find from electronic forms” [ID-27]. Another stated, “Then you have the bioinformaticians out there mining datasets, fishing—big fishing expeditions trying to find the cause of premature birth” [ID-7]. Yet another compared the bioinformaticians’ approach to that of a drunk looking for his keys under the lamppost: They are tilted toward where there is data. It is sort of like where the drunk lost his keys; he is looking under the lamppost, you know? In some ways they are looking under the lamppost, but the keys may be in other places, but you have to start somewhere. That’s their world. [ID-25]
On the other end, the bioinformaticians experienced epistemological suspicion over the ability of traditional laboratory science to stay relevant in modern biomedical knowledge production. For them, analytical approaches relying on information technologies, statistical analyses, and public data repositories were fast, comprehensive, and represented the future of all biomedical sciences. At the end of the project, one project administrator explained where the epistemological suspicion between bioinformatics and traditional laboratory science came from: You realize if you got [name of a bioinformatician] in the room and [name of a geneticist] in the room, [the bioinformatician] would say that the time for laboratory science is almost over, and we actually have enough data and we can just analyze it all, which says to [a geneticist], “You have now become obsolete and useless.” [ID-23]
This account nicely captures the source of epistemological suspicion and why it was so impactful in the project. The bioinformaticians were conveying that those relying on approaches in traditional laboratory science were irrelevant for this project and for biomedical sciences in general. As their careers were based on these approaches, the geneticists in particular were insulted, which made them especially suspicious of the bioinformaticians as the project leaders and as potential collaborators.
Taken together, these accounts suggest that the mutual epistemological suspicion that developed among the CoPs was so strong that in addition to hindering knowledge co-creation in this specific project, it could carry on to future collaborative work with members from the same CoPs.
Discussion
The purpose of this research was to investigate how power and knowledge negotiations structure knowledge co-creation processes in a new collectivity of practice. I discuss the main contributions of this research to power and knowledge dynamics in situated and practice-based learning and knowing in organizations: (1) Knowledge co-creation in an emerging collectivity of practice; (2) Discursive positioning and coercive power; (3) Peripheralization and epistemological suspicion in knowledge co-creation.
Knowledge co-creation in an emerging collectivity of practice
Through an analysis of knowledge co-creation in a new collectivity of practice, the findings contribute to the debates on the limits of the CoP concept to explain the varieties of situated learning and knowing in contemporary organizations (e.g. Amin and Roberts, 2008; Roberts, 2006). Amin and Roberts (2008) urged researchers to consider the type of knowledge, organizational dynamics, social interaction, and mode of innovation in question when studying situated learning and knowing. Lindkvist (2005: 1190) was similarly concerned that the dominance of the CoP concept would lead to “reduced sensitivity in identifying other group level constructs.” He proposed the term collectivity of practice to describe multidisciplinary teams and projects assembled to advance innovative capabilities in organizations, but that did not have shared values and common understandings across group members.
While Lindkvist (2005) did not focus on the dynamic relationship between established CoPs and emerging collectivities, he argued that the two were processually linked and that future research should explore this potentially dynamic relationship. As the studied medical research project was new and emerging, it was an opportune moment to investigate how distinct CoPs form and take part in a collectivity of practice. This also meant that the analysis focused on a potential collectivity of practice rather than a successful one, which Lindkvist (2005: 1200) defined as a group whose members “embrace a collective goal and have good representations of what the others know” and “develop a pattern of interaction and the collective competence needed.” In this sense, the medical research project failed to become an effective collectivity of practice. As prior research has suggested, knowledge co-creation would have required the disembedding of existing localized practices to create potential for the development of new interconnected practices and ultimately a new knowledge creation process (e.g. Mørk et al., 2006; Swan et al., 2002). While some of the CoPs were able to identify opportunities for the creation of interconnected practices, the bioinformaticians held on to their localized practices and leader role making disembedding processes impossible. Although the collectivity of practice formation process was in the end reduced to limited boundary encounters (Barrett et al., 2012; Wenger, 1998), the concepts of an established CoP and an emerging and potential collectivity of practice captured the tensions between localized and interconnected practices that can impede knowledge co-creation.
Discursive positioning and coercive power
Prior research has shown that the power/knowledge and discursive positioning theory can be used to identify and analyze power and knowledge struggles in situated learning and knowing (e.g. Contu and Willmott, 2003; Fox, 2000; Handley et al., 2006; Heizmann, 2011). Heizmann (2011), for example, showed how mechanisms of discursive positioning can lead to the formation of two disparate groups and constrain knowledge sharing between them. The findings of this study similarly demonstrate how power and knowledge were mutually constituted in discourse and how discursive positioning allowed groups to maintain strong boundaries. The discursive positioning of the bioinformaticians showed how they perceived their knowledge practices as superior to those of the other two participating CoPs. As the previously quoted administrator noted, laboratory science was “obsolete and useless” and the obstetricians’ scientific knowledge trivialized, and understandings of current medical practice disregarded. In the shared meetings, the other CoPs began to respond to the bioinformaticians through a discursive positioning that questioned the superiority of their approach.
While conflicting discursive positionings alone can hamper knowledge sharing and creation (Heizmann, 2011), the findings suggest that critical discursive positioning combined with coercive power can make these mechanisms particularly obstructive for knowledge co-creation. In Follett’s view (1998), coactive power can support higher synthesis among varied knowledge and skills. In organizations, it can be implemented through practices such as letting-go, engaging others, facilitation, and horizontal leadership (Salovaara and Bathurst, 2018). Yet, the bioinformaticians relied on coercive power by adopting an authoritative leader role, assigning other CoPs as the audience for their work, and determining the problem focus, and knowledge creation process. Prior research has suggested that this kind of a competitive, vertically-structured, individualistic, and hierarchical environment does not create suitable conditions for effective knowledge co-creation and learning partnerships (Harvey et al., 2013; Pyrko et al., 2017; Roberts, 2006).
As part of innovation processes “knowledge and practice need to be constantly explored, tested and negotiated” (Mørk et al., 2010: 589). As such, power and knowledge conflicts are particularly likely in innovation processes that take place at the boundaries of CoPs (e.g. Mørk et al., 2010; Swan and Scarbrough, 2005). When coercive power is used as leverage in these negotiations, one group may begin to dominate a discourse and reproduce its own rationalities and practices (Heizmann and Olsson, 2015). Drawing on coercive power and conflicting discursive positioning, the bioinformaticians seemed to develop their own regime of truth (Foucault, 1979) taking a dominant role and closing off opportunities for knowledge co-creation. Such behavior is detrimental to knowledge co-creation and innovation processes. Future research should continue to explore how discursive positioning and coercive power operate together and how their emergence in new collaborative arrangements can be managed for the benefit of organizational learning and innovating.
Peripheralization and epistemological suspicion in knowledge co-creation
The notion of peripheralization, which emerged from the analysis, can be understood as the reversal of legitimate peripheral participation, a commonly discussed term in the CoP literature. Legitimate peripheral participation explains how newcomers are allowed to gradually move inward toward the core community as they develop the mastery of knowledge and skills required for full participation (Lave and Wenger, 1991; Wenger, 1998). The newcomers first engage in peripheral tasks that are less intense and risky than the demanding tasks conducted by the full members (Wenger, 1998). Wenger (1998: 101) noted that legitimate core members, compared to newcomers in the periphery, can be characterized as “being useful, being sponsored, being feared, being the right kind of person, having the right birth.” They embody a powerful position in the community which allows them to determine and oversee the activities of the newcomers.
In a collectivity of practice consisting of distinct CoPs, positions of power that determine who is in the center of the project and who is in the periphery are not as predetermined and obvious. Instead, positions of power develop over time through particular practices and interactions between groups. In this study, we saw how the bioinformaticians were able to draw on their CoP associated power and push the other CoPs outward to the periphery of the collectivity. They took on an authoritative role and repeatedly highlighted the legitimacy and the superiority of their own knowledge practices. Even still, the geneticists and the obstetricians identified opportunities for knowledge co-creation (e.g. validating biomarkers, offering knowledge on medical practice), although these instances were somewhat similar to the peripheral tasks of newcomers as they were often suggestions for how to contribute to the bioinformaticians’ established knowledge making process rather than demands for genuine, exploratory, and shared knowledge co-creation processes.
The findings also demonstrate that the practice of peripheralization contributed to epistemological suspicion—a deeply felt skepticism toward foreign knowledge practices. I suspect that if it is not openly expressed in interactions among different CoPs, epistemological suspicion may not be detrimental to knowledge co-creation. However, when it is repeatedly expressed through conflicting discursive positioning and displays of coercive power, it begins to consume potential for knowledge co-creation.
It is possible that the bioinformaticians experienced some epistemological suspicion at the start of the project as they peripheralized the other CoPs so quickly from the knowledge co-creation process. When the bioinformaticians’ skepticism toward other CoPs became evident in the shared meetings, it generated similar feelings among the geneticists and the obstetricians affecting how they perceived the bioinformaticians as project leaders and collaborators. Because the bioinformaticians’ skepticism was so immediate, it suggests that the affect was there prior to the project, which in turn implies that epistemological suspicion can stick and carry on from project to project. Future research should explore the temporalities of epistemological suspicion: When and how does it emerge? How does it spread? How far is it able to travel and with what consequences for knowledge co-creation?
Epistemological suspicion may also relate to the affective dimension present in situated learning and knowing (e.g. Contu, 2014; Kofman and Senge, 1993; Vince, 2001). Contu (2014) connected the affective dimension to discursive positioning and identities, because when subjects participate in situated practice, they internalize knowledge and competences that are meaningful for them and that they see as valuable. As Contu (2014: 294) argued, “meanings [. . .] are invested with a quality, a force of a desire that is of, and for, ‘this’ rather than ‘that’”. While I analyzed epistemological suspicion as a negative feeling CoPs experienced in relation to the value and the validity of another CoP’s knowledge practices, which then hindered knowledge co-creation, it can also be seen from the affective perspective as relating to their own identity formation and efforts to demarcate boundaries between communities.
There are many reasons for why CoPs position themselves in conflict and why knowledge co-creation fails. Yet, peripheralization and epistemological suspicion can partly explain why knowledge workers in multidisciplinary teams miss on opportunities for knowledge co-creation. Understanding how they develop gradually, in relation to one another, and affect knowledge co-creation across contexts is of great importance to researchers and practitioners in the fields of management and organization.
Conclusion
This article demonstrated how power and knowledge negotiations become manifested through discursive positioning and coercive power and structure knowledge co-creation processes among CoPs. Although the empirical case focused on how scientists and medical practitioners from different fields seek to form a multidisciplinary team and work together to develop new solutions to a specific health problem, the findings offer practical implications for the management of heterogeneous teams across sectors. Given the ways in which power and knowledge are linked and emerge from interactions between CoPs, it is important to pay attention to team formation and adoption of roles from the start of the project. There is a lot at stake—identities, worth, and skills—when knowledge workers engage in knowledge co-creation at the boundaries of CoPs (e.g. Contu, 2014; Heizmann, 2011; Mørk et al., 2010; Thompson, 2005). So, if given the chance, a specific group may take control of a multidisciplinary project, prioritize their own knowledge, and peripheralize the knowledge of others to the extent that knowledge co-creation and potential for innovation become limited.
From the perspective of the global COVID-19 pandemic and the development of new vaccinations, understanding the processes through which scientific and medical collaborations develop is especially timely. The pandemic highlights the value of medical research, where the aim is to promote cooperation and interaction among clinicians, scientists, and different stakeholders in an effort to translate scientific discoveries into new applications and treatments needed in medical practice (Sharp et al., 2016). Although clinicians and scientists from different fields generally agree on the social values associated with this approach (Sharp et al., 2016), motivating and facilitating engagement in such collaborative work can be difficult. Academic research and medical fields are competitive, excellence is defined quite narrowly, and there is a constant struggle for more personal funding, reputation, and success. These characteristics do not align well with the mission to collaboratively develop and translate scientific discoveries into social goods. While there is much discussion on the social impact of publicly funded research, its effective implementation in academic communities will require rethinking the nature of the academic achievement and reward system; what is it that we want to value and reward?
Footnotes
Acknowledgements
The author is grateful for Daniel McFarland, Woody Powell, Karen Cook, John Willinsky, and Benjamin Keep for reviewing earlier drafts of this article. The author would also like to thank the convenors and the participants of sub-theme 64 at EGOS 2021 as well as the editor Arne Carlsen and the three anonymous reviewers. They all provided valuable feedback, which guided the development of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is part of a project “The Emergence of Health and Life Science Innovations” funded by the Foundation for Economic Education.