
Abstract
Atopic dermatitis (AD) is a chronic inflammatory skin condition with significant psychosocial impacts on patients and caregivers. While patient education has become foundational to AD management, programs that explicitly integrate psychodermatologic content remain understudied. We performed a scoping review to characterize the landscape of psychosocial patient education for AD and to identify avenues for future research. We identified 40 studies spanning pediatric and adult populations. Studies were synthesized descriptively with evidence mapping of randomized controlled trials to visualize intervention effectiveness patterns on AD severity and quality of life (QoL). Pediatric interventions showed strongest evidence, with education on mindfulness and relaxation techniques demonstrating the greatest improvements to AD severity and QoL. In-person education programs were most common and effective for children, emphasizing caregiver empowerment and stress management. Adult-focused research remained limited and inconsistent, though mindfulness-based digital interventions showed promise. Digital and mobile health modalities demonstrated potential when incorporating interactivity and social connection, highlighting the importance of emotional expression and peer support. Key limitations include predominance of high-income country studies, small sample sizes, and substantial intervention heterogeneity. This review provides the first comprehensive mapping of psychodermatologic education for AD, revealing significant research gaps in adult populations while identifying promising approaches for future scalable interventions emphasizing emotional support and behavioral change principles.
Introduction
Atopic dermatitis (AD) is a chronic inflammatory skin disease affecting ~15% of children and 3% of adults in Canada.1,2 With profound impacts on quality of life (QoL), AD has been linked to poor sleep, lowered self-esteem, and functional impairment.3 -5 These effects extend to the caregivers and families of children with AD, who experience increased stress, financial burden, and feelings of helplessness regarding disease management.6,7 There is a well-defined link between AD and psychiatric comorbidity, including an increased risk of depression, anxiety, somatoform, trauma- and stressor-related, and personality disorders.4,8,9 In addition, the debilitating itch-scratch cycle associated with AD is thought to self-perpetuate through an interplay between both cutaneous and psychological factors. 10 The examination of this bidirectional relationship between mind and skin, known as psychodermatology, is crucial to the development of effective, multidisciplinary management strategies for AD. 11
Patient education has become a foundational component of AD management. Interventions promoting health literacy have been linked to improved health outcomes in chronic disease through patient empowerment, increased self-efficacy, and a strengthened physician-patient relationship.12 -14 In pediatric disease management, caregiver education is associated with reduced caregiver burden and increased confidence, self-esteem, and self-efficacy. 15 A systematic review evaluating patient education programs for adults and children with AD reported significant improvement in eczema severity and patient QoL outcomes, noting a need for further exploration of different intervention methodologies. 16
In parallel, psychological interventions have gained traction as an effective adjunct in AD management by targeting the behavioral and emotional drivers of the itch-scratch cycle and promoting more adaptive coping strategies for disease-related stress. Treatments such as cognitive-behavioral therapy (CBT), relaxation training, and habit reversal therapy (HRT) have demonstrated efficacy in reducing eczema severity, with inconclusive findings regarding their impact on QoL.17,18
To date, the literature has largely considered these intervention strategies in isolation. A systematic review of psychological and educational interventions for AD identified 6 studies combining the 2 methods, with 5 reporting improved AD severity. 17 However, this analysis was limited to randomized controlled trials (RCTs) that were primarily published over 20 years ago. A narrative review of multidisciplinary interventions for AD that most programs incorporate expert-led psychological treatment (eg, therapist-administered CBT) rather than educational content teaching patients about psychological mechanisms for self-directed management. 19 This represents a critical knowledge gap, as programs that explicitly teach patients about the psychological mechanisms driving AD, coupled with practical self-management strategies, may offer an opportunity to address the full spectrum of disease burden.
Current literature assessing AD patient education interventions highlights the difficulty of making definitive recommendations for effective management. A dearth of research and significant heterogeneity with respect to study design, treatment modality, and outcome measure highlights the need for an exploratory and descriptive approach to characterizing available interventions. Real-world studies employing quasi-experimental or observational designs are also omitted from existing analyses, limiting insight into the breadth and utility of management options.
This scoping review summarizes the landscape of psychodermatologic educational interventions for children and adults with AD, and provides an evidence map to support clinicians in addressing patient interest and guide counseling in practice.
Materials and Methods
This scoping review was conducted according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) Extension for Scoping Reviews framework to map and characterize studies that evaluate educational tools addressing the psychosocial impact of AD. The review aimed to examine the impact of these tools on AD severity and QoL while identifying unmet needs and knowledge gaps in the current literature.
Eligibility Criteria
We included randomized and non-randomized studies evaluating psychodermatologic educational interventions for individuals with AD. Initially, we required studies to report AD severity or QoL outcomes; however, to better align with scoping review principles, we broadened inclusion to all interventions regardless of outcome type. Studies solely reporting unrelated dermatologic outcomes were excluded.
Eligible studies were original research articles published within the past 20 years that included children or adults diagnosed with AD, or their caregivers. Studies must have evaluated educational tools or programs addressing at least 1 psychosocial impact of AD, such as stress, sleep disturbances, stigma, coping strategies, or mental health. Only English-language articles with available full text were included.
Information Sources and Search Strategy
On February 2, 2025, we searched peer-reviewed literature from 5 databases (MEDLINE, Embase, Psycinfo, CINAHL, and Scopus) published from January 1, 2005. The full electronic search strategy for each database can be seen in Supplementary File 1.
Selection of Sources of Evidence
Search results were imported into Covidence software (Veritas Health Solutions, Melbourne, Australia). Duplicate records were removed automatically. Title and abstract screening was conducted in duplicate by 3 independent reviewers (X.C., K.L., and M.S.Y.L.) using the inclusion criteria listed above. Any disagreements on the inclusion of a publication were resolved by another reviewer (T.T.). Publications that were accepted by 2 reviewers then underwent full-text review and subsequent data extraction.
Data Charting Process and Data Items
A standardized data extraction table was developed and piloted. Data were charted independently and in duplicate. Discrepancies were resolved by discussion. Charted data were stored in Google Sheets. Extracted information included study and population characteristics, AD severity assessments, and intervention descriptions (format, frequency, duration). We charted psychodermatologic educational topics covered (eg, stress management, itch-scratch cycle, mindfulness techniques, emotional impacts), psychosocial outcomes measured (QoL, stress, sleep), and the instruments used to assess these outcomes. The full data extraction table is available in Supplementary File 2.
Critical Appraisal of Individual Sources of Evidence
Risk of bias was assessed for all RCTs (n = 24) using the Cochrane Risk of Bias 2.0 (RoB 2) tool. 20 One reviewer (P.A.) independently performed the primary assessments. Secondary reviewers (S.D., K.L., and M.S.Y.L.) verified assessments in a split format. A traffic light plot summarizing the RoB 2 assessments can be seen in Figure S2.
Synthesis of Results
Results were synthesized descriptively. Outcomes were stratified by pediatric versus adult studies. An evidence mapping table was created to visualize outcome significance across intervention types and domains, taking into consideration effect size. Interventions were categorized based on the main mode of content delivery described in each study: in-person patient education programs (structured face-to-face sessions), digital educational modules (web-based or video content), psychosocial education programs (in-person and online interventions delivered and/or created by mental health professionals that focus exclusively on psychological skills such as mindfulness or relaxation training, without integrated education on medical management), mobile health (mHealth; smartphone applications or messaging platforms), and handouts/handbooks (primarily written materials).
A temporal evidence map with a legend was also created to present another way of visualizing our findings. Effect size was assessed using Cohen’s d, in which a d ≤ 0.2 is a negligible effect size, 0.2 < d ≤ 0.5 is a small effect size, 0.5 < d ≤ 0.8 is a moderate effect size, and d > 0.8 is a large effect size. 21 In RCTs with data collected at multiple timepoints, the Cohen’s d used in the evidence map reflected findings from the most recent follow-up. For studies where insufficient information was given to calculate Cohen’s d, the rank-biserial correlation (r) was used instead. Both maps allow for visual identification of trends in efficacy, highlight research gaps in psychodermatologic education for AD, and identify promising educational interventions.
Results
Of 2903 studies identified through electronic searching and 5 additional studies included by reference screening, 1718 were excluded due to duplicates and 1185 underwent title and abstract screening. Ninety-three articles were considered for full-text review, with 40 articles meeting our inclusion criteria.22 -61 A PRISMA flow diagram of the study selection can be seen in Figure S2 in the Supplementary File 1.
Summary of Included Studies
Of the 40 included studies, Germany and the United Kingdom (n = 5 each) were the most common study locations; followed by France and South Korea (n = 3); and Australia, Brazil, China, the Netherlands, Sweden, Switzerland, and the United States (n = 2). One study each was conducted in Croatia, Denmark, Hong Kong, Iceland, Italy, Japan, Norway, and Spain. Twenty-four of the included studies were RCTs,23 -29,34,36,39,43,46,47,49,51 -53,55 -58,60 with the remainder comprising 9 quasi-experimental studies,22,30,32,37,38,40,45,59,62 6 observational studies,31,33,41,48,54,61 and 1 qualitative study. 35 Twenty-four studies included educational interventions aimed at children living with AD and their caregivers,24,26 -31,34,35,40,41,44,46 -54,56,59,60 13 studies were focused on adults living with AD,23,25,32,33,37 -39,43,45,55,57,61,62 while 3 studies included both pediatric and adult participants.22,36,58 Breuer et al, Kupfer et al, and Staab et al present data from 1 RCT, as do Greenwell et al and Santer et al; these studies will only be represented by their earliest publication in our analyses to avoid double-counting. Full study characteristics are presented in Supplementary File 2.
Psychodermatologic Education for Both Children/Caregivers and Adults With AD
Three studies assessed educational modules that were aimed at both children with AD and their caregivers, as well as adults living with AD.22,36,58 Two studies used web-based platforms to deliver their modules.36,58 Santer et al and Greenwell et al report on the same RCT, wherein online self-guided educational modules addressed stress management, information about the itch-scratch cycle, emotional management strategies, and improving confidence. In both caregiver/child and adult participants, the intervention group saw a significant improvement patient-oriented eczema measure (POEM) score (AD severity) that remained at 52-week follow-up. A study by Andrade et al delivered its modules over a 7-day period using a WhatsApp group chat. 22 While AD severity and QoL were not included as outcome measures, participant health knowledge was increased post-intervention and at 1-month follow-up.
Psychodermatologic Education for Children With AD and Caregivers
Across 24 studies (27 articles) – reflecting multiple publications from single trials (Breuer et al, Kupfer et al, Staab et al, Greenwell et al, and Santer et al) – the most common delivery modality was the in-person patient education program, which was utilized in 15 studies (17 articles).24,29 -31,35,41,47 -51,53,56,60 Five interventions employed online training modules,22,27,36,58,59 while paper handouts46,52 and psychosocial patient education34,40 were both each used in 2 studies. mHealth-based interventions were the least frequent, appearing in only 1 study. 27
The 2 most commonly-included educational topics were caregiver empowerment (13/24 studies),24,29,31,34,41,46,49,50,54,56,58 -60 which included behavior-change strategies, building treatment confidence, and promoting positive parenting practices; and stress management techniques (12/24 studies).22,27,34,46,47,49,50,53,56,58 -60 Other topics included mindfulness and relaxation techniques like meditation, HRT, and infant massage (11 studies)28,30,31,34,35,40,46,52,54,58,60; information on the emotional and social impacts of AD, such as its effects on self-esteem, dealing with stigma, and bullying (10 studies)27,30,34,40,41,46,48,51,56,58; and education on the itch-scratch cycle (5 studies).46,52,54,58,60
Topics and Outcomes by Intervention Modality
In-Person Patient Education Programs
Fifteen interventions using patient education programs were identified.24,29 -31,35,41,47 -51,53,54,56,60 The target audience for these programs varied: 1 study was designed exclusively for children, 4 were for caregivers only,35,48,53,54 and the remainder targeted both. Most used group formats with multidisciplinary delivery involving psychologists, dietitians, and social workers alongside medical teams. Program intensity varied from a single 1-hour session 24 to 13 sessions over 18 months, 30 with follow-up periods up to 14 months. Content focused primarily on caregiver empowerment (9/14 studies),24,29,31,41,49,50,54,56,60 followed by stress management (7 studies),47,49,50,53,56,58,60 mindfulness/relaxation techniques (5 studies),30,31,35,54,60 the emotional and social impacts of AD (5 studies),30,41,48,51,56 and education on the itch-scratch cycle (2 studies).54,60 Of the 11 studies measuring AD severity (via the eczema area and severity score [EASI], POEM, SCORing Atopic Dermatitis [SCORAD]) and QoL (via the Child Dermatology Life Quality Index [CDLQI], dermatitis family impact [DFI], Infants’ Dermatitis Quality of Life Index [IDQOL], and QoL-AD) as intervention outcomes, 8 demonstrated statistically significant improvements,29,30,41,47,48,51,53,60 while 3 found no significant between-group differences.24,49,56
Digital Educational Modules
Five studies utilized online modules for patient education,22,27,36,58,59 3 of which (Andrade et al, Greenwell et al, and Santer et al) included both pediatric and adult participants and are described in a dedicated section above (see Section “Psychodermatologic Education for Both Children/Caregivers and Adults With AD”). Son and Lim’s 2-week web-based program provided AD information followed by quizzes and checklists for assessment. 59 Significant improvements to QoL (via the SCORAD and EASI) and AD severity (via the CDLQI) were observed. Brunner et al used 6 short videos featuring parent experiences to educate participants on stress management and the emotional impacts of AD. 27 No significant improvements in SCORAD or Family Dermatology Life Quality Index score were observed.
Handbooks
Two studies used handbooks as a primary delivery method.46,52 Norén et al taught caregivers HRT through written guides with daily symptom tracking, showing sustained improvements in AD severity (via the SCORAD) but not QoL (via the CDLQI). 52 LeBovidge et al employed a more passive approach by providing comprehensive take-home handbooks covering physiologic management and psychosocial topics, with no significant improvements in EASI or CDLQI/IDQOL scores observed at 3-month follow-up. 46
Psychosocial Patient Education Programs
Two studies assessed interventions using a purely psychosocial model.34,40 Fung et al implemented an in-person Integrative Body-Mind-Spirit program with 6 weekly sessions for caregivers. 34 Participants were taught to use mindfulness techniques to mitigate the emotional and social impacts of AD, build self-confidence, and manage stress. The authors did not assess AD severity or QoL, but noted significant improvements in depression, anxiety, and holistic wellbeing outcomes measures. Hughes et al delivered mindfulness training online over 10 weeks, through didactic teaching about neurobiology and education on practical techniques, including breathing and emotional awareness exercises. 40 AD severity was not assessed in this study and, although QoL was measured through the CDLQI, low sample size (n = 10) did not permit statistical analysis.
Mobile Health
One RCT by Cerqueira et al used an mHealth intervention that focused solely on relaxation and mindfulness techniques. 28 Designed for caregivers, the intervention group received daily text messages related to AD pathophysiology, triggers, and treatment for 4 weeks. At 1-month follow-up, no significant differences in AD severity (via the POEM and SCORAD) or QoL (via the CDLQI) were noted between the intervention group and the control group, who received messages on general health topics.
Psychodermatologic Education for Adults With AD
For adult participants, 4 main intervention modalities were identified across 16 studies.22,23,25,32,33,36 -39,43,45,55,57,58,61,62 The most common were in-person patient education programs (7 studies)25,32,33,39,45,55,57 and online educational modules (5 studies).22,36,38,58,61 These were followed by psychosocial education programs (3 studies),23,43,62 while mHealth interventions were used the least frequently (1 study). 37
The most frequently addressed topic in adult interventions was stress management, which was included in 14 of the 16 studies.22,25,32,33,36 -39,43,45,55,57,58,62 This was followed by education on the mind-body connection, such as an introductory lesson on psychodermatology (9 studies)23,25,32,37,38,43,45,55,57; mindfulness and relaxation techniques like at-home hypnotherapy, HRT, and progressive muscle relaxation (PMR; 9 studies)23,25,37,38,43,45,55,57,62; and education on the itch-scratch cycle (8 studies).32,33,36,38,43,58,61,62 Four studies aimed to increase patient empowerment in AD management through education on self-efficacy and improved confidence,32,36,37,58 and 3 studies incorporated education on the social and emotional impacts of AD, such as its effect on self-esteem and risk of self-isolation.22,38,62
Topics and Outcomes by Intervention Modality
In-Person Patient Education Programs
Seven studies used in-person group education programs for adults, all with multidisciplinary delivery, including psychologists and dietitians.25,32,33,39,45,55,57 Bostoen et al, Lambert et al, and Sahin et al tested the same 12-week intervention, requiring ~60 hours of total participation (roughly 5 hours weekly), where participants received education on stress management, mindfulness and relaxation techniques including yoga, and psychodermatology.25,45,57 AD severity and QoL were assessed by the EASI and Dermatology Life Quality Index (DLQI), respectively. Lambert et al’s quasi-experimental pilot showed significant improvements in both outcomes, but subsequent RCTs by Bostoen et al and Sahin et al found no significant differences.
Evers et al’s 3-month itch-coping intervention educated participants on the itch-scratch cycle, stress management, self-management skills, and HRT. 32 Greater improvements in EASI scores were noted in the intervention group at 12-month follow-up, although no significant differences in DLQI score were noted. Rotter et al taught participants how to conduct at-home hypnotherapy exercises, along with education on the mind-body connection and stress reduction. 55 Statistical analysis was not performed due to low sample size, but numeric improvements in AD severity (via the EASI and SCORAD) and QoL (via the DLQI) were noted at 26-week follow-up in the intervention group.
Psychosocial Patient Education Programs
Three studies used psychosocial education programs.23,43,62 Kishimoto et al’s 8-week mindfulness program taught participants about mindfulness, body awareness, stress management, and self-compassion, showing significant improvements in AD severity (via the POEM) and QoL (via the DLQI). 43 Kern et al’s self-directed CBT-based intervention also demonstrated sustained improvements in POEM and DLQI scores at 3-month follow-up. 62 Bae et al’s 4-week PMR program showed no significant differences in AD severity (via the EASI), and did not report QoL. 23
Digital Educational Modules
Five studies provided educational content through online modules, with 3 studies, by Andrade et al, Greenwell et al, and Santer et al including both child/caregiver and adult participants (see Section “Psychodermatologic Education for Both Children/Caregivers and Adults With AD”).22,36,38,58,61 Heckman et al’s 3-month intervention provided educational modules on itch-coping, including information on stress management, the mind-body connection, the itch-scratch cycle, mindfulness and relaxation techniques like PMR, and the social and emotional impacts of AD. 38 Van Os-Medendorp et al’s self-management modules educated patients on the itch-scratch cycle. 61 Heckman et al noted post-intervention improvements in QoL (via the ItchyQoL), while van Os-Medendorp et al did not gather post-test measurements on AD severity or QoL.
mHealth Interventions
Gudmundsdottir et al tested a digital intervention delivered to 299 participants through a smartphone app over a 6-week period. 37 The app used gamification and behavioral psychology principles to teach participants about the mind-body connection, stress management, self-efficacy through motivational practices, and mindfulness. AD severity (via the POEM and SCORAD) and QoL (via the DLQI) were significantly improved when measured post-intervention, although no follow-up was conducted.
Evidence Mapping
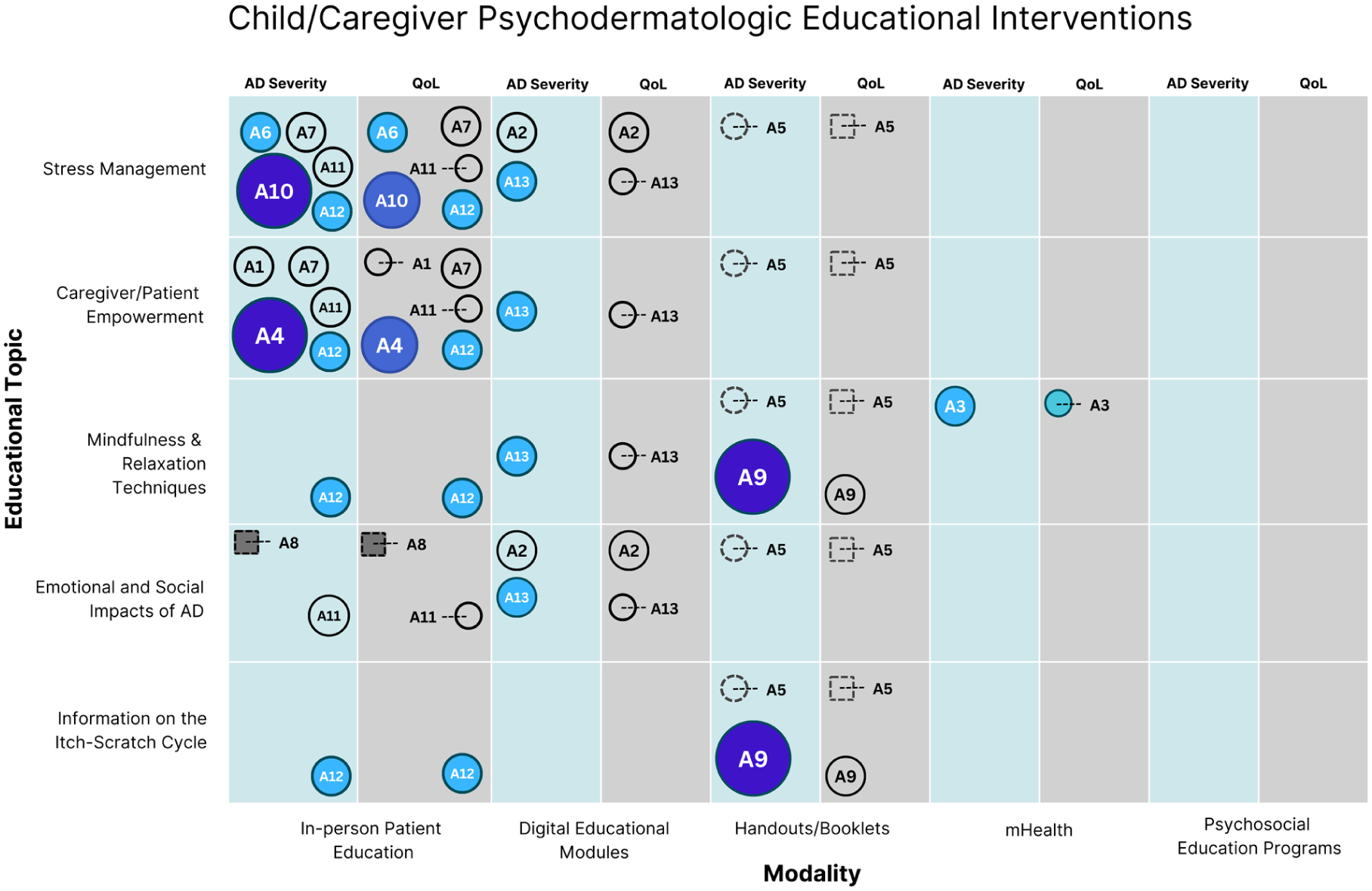
An evidence map of RCT findings was constructed to synthesize the included interventions and their corresponding effects on AD severity and QoL (Figure 1). Evidence mapping of 13 pediatric RCTs showed in-person education programs (8 studies) were most effective, with 5/8 demonstrating significant improvements in AD severity and QoL.24,29,47,49,51,56,60 Digital modules and handouts each showed improvements in AD severity in 1 study but not QoL.27,46,52,58 The single mHealth intervention showed small improvements in both outcomes. 28 While 1 RCT was conducted on the impacts of a psychosocial education programs, the study did not report on AD severity or QoL as an outcome measure.
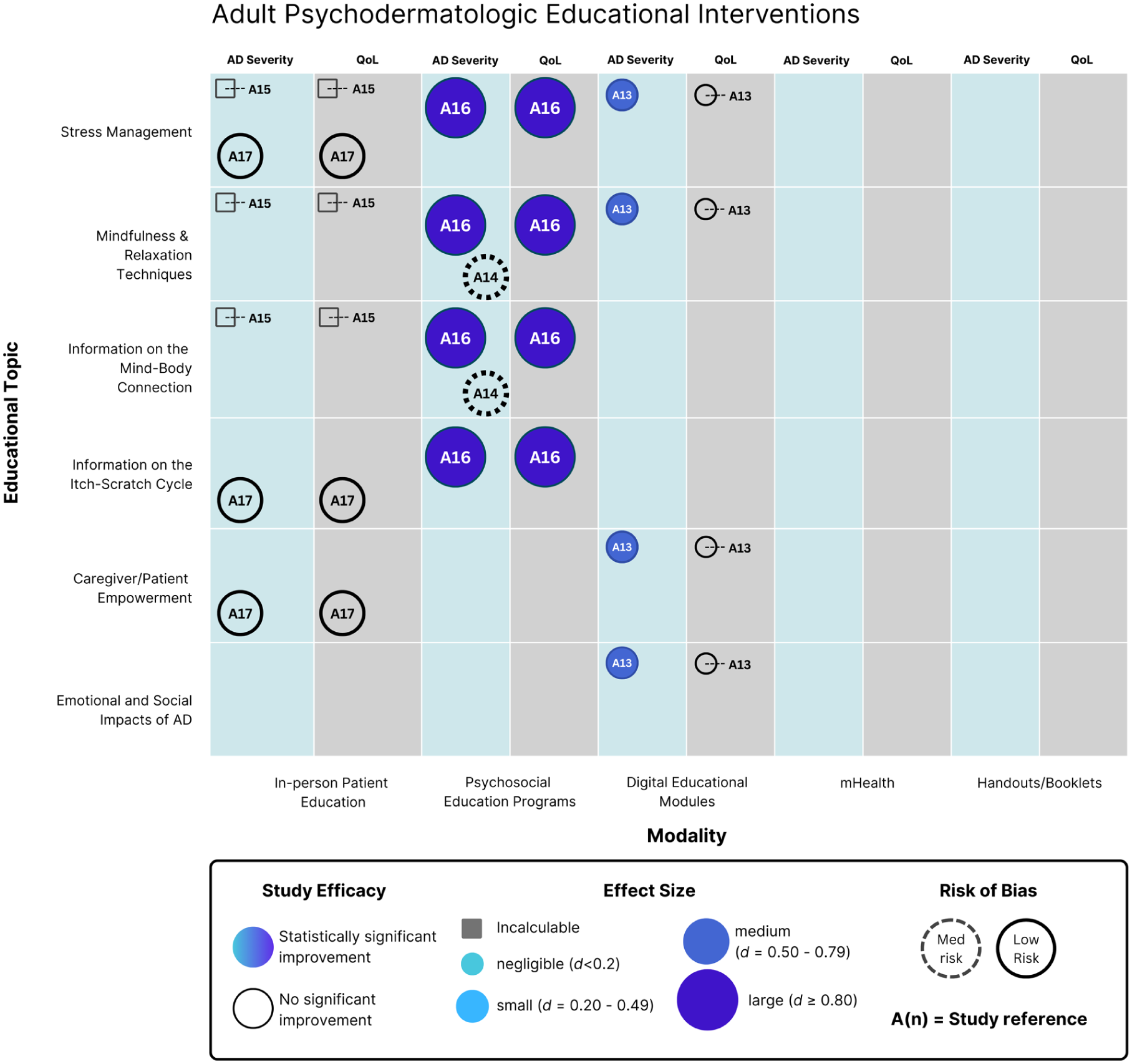
Evidence map of RCTs for adult patients with AD severity and/or QoL as primary or secondary outcomes. AD, atopic dermatitis; QoL, quality of life; RCTs, randomized controlled trials.
Interventions with education on mindfulness/relaxation techniques showed the greatest proportion of studies with significant improvements to AD severity (4/5 studies) and QoL (3/5 studies), with positive findings observed in 1 intervention from each delivery modality excluding psychosocial education programs.28,46,52,58,60 Stress management interventions that significantly improved AD severity (4/8 studies) and QoL (3/8 studies) primarily used an in-person education delivery modality, with 1 study using digital modules also showing success.47,49,53,58,60 Education on caregiver empowerment significantly improved AD severity and QoL in 3/7 and 2/7 studies, respectively, while itch-scratch cycle education was effective in 2/3 and 1/3 studies, respectively.46,52,60 Interventions on the social/emotional impacts of AD were the least effective, with 2/5 and 1/5 studies showing significant improvements to AD severity and QoL.27,46,51,56,58
Evidence mapping of RCTs focusing on adult AD patients reveals significant knowledge gaps, consisting of only 5 studies.23,25,43,57,58 Bostoen et al and Sahin et al assessed interventions using in-person patient education, with neither showing significant improvements to AD severity or QoL.25,57 Two studies used psychosocial patient education; Kishimoto et al’s mindfulness-based intervention showed significant improvements of a large effect size in both AD severity and QoL, while Bae et al found no difference in AD severity between control and intervention groups.23,43 Santer et al’s educational module intervention demonstrated significant improvements in AD severity and no significant changes to QoL. 58 No RCT data were available for interventions using handouts or mHealth as their primary delivery modality.
Grouping by educational topic yielded similarly heterogeneous results; interventions including education on stress management (4 studies), mindfulness and relaxation techniques (4 studies), the mind-body connection (3 studies), the itch-scratch cycle (2 studies), caregiver empowerment (2 studies), or the social and emotional impacts of AD (1 study) had <50% of studies showing statistically significant improvements to AD severity or QoL.
Quality Assessment
Quality assessment using RoB 2 found that 66.7% of studies had low overall risk of bias, 25.0% showed some concerns, and 8.3% were high risk (Figure S2). Minimal bias in the selection of the reported result (87.5% of studies being low risk) or arising from the randomization process (83.3% low risk) was noted. For risk of bias due to missing outcome data, 62.5% of RCTs were classified as low risk, with the remaining showing some concerns. Significant risk of bias due to deviations from the intended intervention was noted (37.5% low risk). Risk of bias in measurement of the outcome was greatest, with 20.8% of studies being high risk, and only 45.8% of studies being low risk.
Discussion
To our knowledge, this review is the first to characterize the psychosocial curricular content of educational interventions for patients with AD. The inclusion of RCTs alongside real-world quasi-experimental and observational studies enabled a broader characterization of the research landscape of psychosocial education in AD management.
Evidence is strongest for pediatric interventions that include education on mindfulness and relaxation techniques, which had the greatest proportion of studies showing significant improvements to AD severity and QoL (4/5 and 3/5 studies, respectively). These findings are further supported when including non-experimental study designs, with 5/6 studies and 4/7 studies showing significant improvements in AD severity and QoL, respectively. Consisting of both in-person education programs and various virtual interventions, these findings suggest that multiple intervention modalities may be similarly acceptable. Mindfulness-based interventions have shown promise in improving caregiver/child mental health and QoL across various chronic disease experiences.40,63 Future research should continue to trial new intervention modalities and deepen the body of evidence to allow for specific and valid recommendations for optimal service delivery.
Interventions for adults with AD remain understudied.16,18 Multidisciplinary in-person programs often fail to provide significant advantages over standard care in improving AD severity or QoL. Several factors may explain this pattern. Adult participants may enter such programs with entrenched coping behaviors, fixed beliefs about their disease, or competing life demands, reducing receptivity to generalized educational content delivered in group formats. Additionally, participants already receiving optimized dermatologic care may have limited capacity for measurable incremental improvement. In contrast, digital and mHealth interventions appear more effective when they incorporate interactivity, peer connection, and active skill-building.
These formats may better align with adult learning preferences, allowing flexible pacing and immediate application to daily symptom management.
Our evidence mapping revealed no clear correlation between the number of psychodermatologic educational topics included and intervention success, and baseline eczema severity did not consistently predict intervention outcomes.49,51 There are no intervention modalities that have clearly demonstrated better outcomes. Though RCTs evaluating in-person education programs showed the greatest improvements to AD severity and QoL, this may be attributed to a larger existing evidence base (Figure 2). A meta-analysis of therapeutic patient education for chronic diseases found that interventions were similarly effective at improving QoL, self-efficacy, and treatment adherence across different delivery methods and providers. 64 This suggests greater flexibility when determining optimal intervention development, allowing greater scalability to various material and structural contexts (Figure 3).
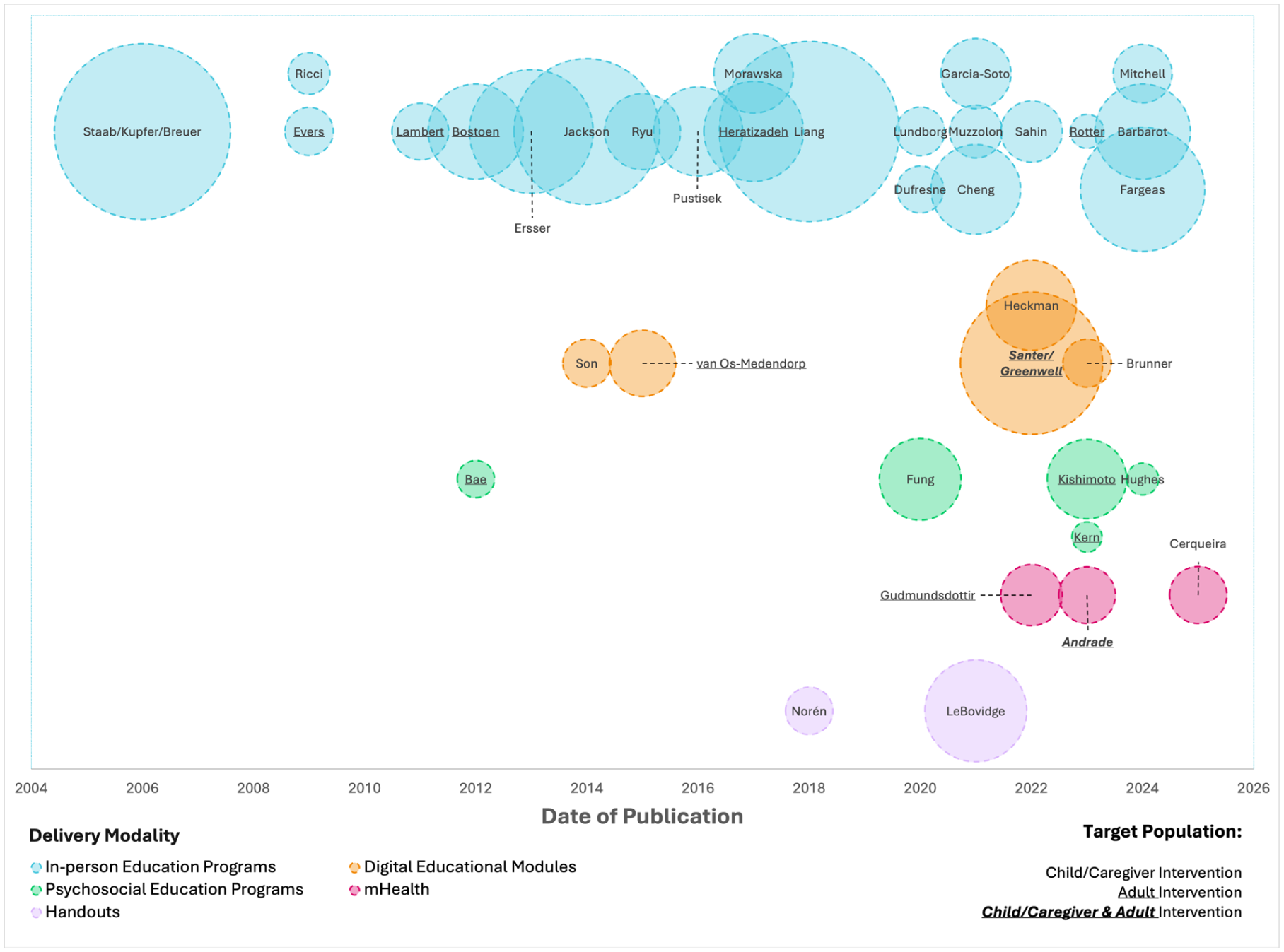
Timeline of included articles by publication date, organized by intervention delivery modality. Circle area is representative of study sample size. Studies are identified by their first author. Staab et al, Kupfer et al, and Breuer et al use data from the same trial, as do Santer et al and Greenwell et al. The studies are thus represented by only 1 circle. mHealth, mobile health.
Evidence map of RCTs for pediatric patients with AD severity and/or QoL as primary or secondary outcomes. AD, atopic dermatitis; QoL, quality of life; RCTs, randomized controlled trials.
The use of passive or active learning approaches may impact intervention success. LeBovidge et al’s comprehensive take-home handbook, providing extensive educational content, showed no significant improvements at 3-month follow-up. 46 In contrast, Norén et al’s intervention, using written handbooks to promote active skill acquisition (HRT), demonstrated sustained improvements at 12-month follow-up. 52 These findings suggest that effective psychodermatologic education may employ mechanisms promoting active skill practice rather than information delivery alone.
Greater intervention intensity yielded mixed outcomes. Staab et al’s 6-week pediatric program produced significant improvements, while Ryu et al’s similarly lengthy intervention showed no impact on AD severity or QoL despite marked gains in parental knowledge.56,60 A short 2-week follow-up in the latter may not have provided sufficient time to observe clinical change. Among adults, high-intensity programs yielded mixed outcomes. Kishimoto et al’s mindfulness-based intervention achieved notable success, likely supported by a motivated cohort and peer group dynamics. 43 Other major high-intensity programs failed to demonstrate significant improvements, potentially due to limited sample sizes and reduced statistical power.24,56 Interventions that foster emotional expression, normalize disease experiences through shared narratives, and promote self-efficacy appear to engage psychological mechanisms inadequately addressed by information-heavy, clinician-led sessions alone. Ferrer and Mendes highlight the importance of healthy emotional self-expression over suppression for coping, a concept consistent with AD patients’ experiences of feeling dismissed or trivialized.65,66 Santer et al’s modules incorporated shared caregiver narratives and interactive challenges designed to foster connection and self-efficacy.
For clinicians, these findings suggest that program format and engagement strategy may be more important than program intensity or multidisciplinary scope. Clinicians may achieve greater impact by directing patients toward interventions that prioritize active participation, emotional validation, and behavioral practice, even when delivered remotely.
Beyond efficacy, the real-world accessibility of psychodermatologic education programs represents a substantial barrier to implementation, particularly within publicly funded healthcare systems. Large, multidisciplinary in-person programs require significant institutional infrastructure, specialized personnel, and sustained funding, all limited resources in systems already facing workforce shortages and long wait times.18,19 These programs often require repeated visits and significant time commitments, which may be difficult to integrate into work, school, and family life. 66 These structural barriers may partially explain why high-intensity programs fail to demonstrate superior outcomes despite substantial resource investment. Scalable digital and mobile interventions may mitigate many of these challenges by reducing geographic constraints, lowering per-patient costs, and allowing asynchronous participation.67,68 From a health system perspective, interventions that can be embedded within routine care pathways may represent a more feasible and equitable strategy for integrating psychodermatologic education into practice.
Limitations
Most included studies originated from high-income countries, limiting the utility of our findings in lower-resource or culturally distinct settings. The relative paucity of culturally tailored or equity-focused interventions, as well as the reliance on quasi-experimental and observational designs among the real-world studies, introduces additional uncertainties in assessing intervention effectiveness across diverse populations. Small sample sizes and short follow-up periods in many studies limit the robustness and generalizability of results, particularly regarding long-term efficacy. Substantial heterogeneity across interventions regarding content, methodology, intensity, and outcome measures further complicates information synthesis. Excluding studies that did not assess AD severity or QoL, despite their potential contributions to psychosocial understanding, likely narrowed the evidence base.
Conclusion
This review provides the first comprehensive characterization of psychodermatologic educational interventions for AD, revealing that mindfulness and relaxation techniques show the strongest evidence for pediatric populations, while adult-focused research remains relatively underdeveloped. Rather than intervention intensity or topic breadth, intervention success appears dependent on fostering emotional expression and peer support, with digital modalities showing promise when incorporating interactivity and social connection. Future research should prioritize large-scale, well-powered trials with longer follow-up, culturally sensitive content, and expanded psychosocial outcome measures. Greater evaluation of digital and mHealth interventions, particularly those emphasizing engagement and social connectivity, may contribute to the development of scalable, equitable psychodermatologic education to better support individuals and families affected by AD.
Supplemental Material
sj-docx-1-cms-10.1177_12034754261453363 – Supplemental material for Psychodermatologic Patient Education for Atopic Dermatitis Management: A Scoping Review and Evidence Map
Supplemental material, sj-docx-1-cms-10.1177_12034754261453363 for Psychodermatologic Patient Education for Atopic Dermatitis Management: A Scoping Review and Evidence Map by Kevin Li, Michelle Sze Yiu Leung, Parsa Abdi, Serena Dienes, Tarek Turk, Xiaonan Chen, Liz Dennett, Sebastian Straube and Marlene Dytoc in Journal of Cutaneous Medicine and Surgery
Supplemental Material
sj-docx-3-cms-10.1177_12034754261453363 – Supplemental material for Psychodermatologic Patient Education for Atopic Dermatitis Management: A Scoping Review and Evidence Map
Supplemental material, sj-docx-3-cms-10.1177_12034754261453363 for Psychodermatologic Patient Education for Atopic Dermatitis Management: A Scoping Review and Evidence Map by Kevin Li, Michelle Sze Yiu Leung, Parsa Abdi, Serena Dienes, Tarek Turk, Xiaonan Chen, Liz Dennett, Sebastian Straube and Marlene Dytoc in Journal of Cutaneous Medicine and Surgery
Supplemental Material
sj-xlsx-2-cms-10.1177_12034754261453363 – Supplemental material for Psychodermatologic Patient Education for Atopic Dermatitis Management: A Scoping Review and Evidence Map
Supplemental material, sj-xlsx-2-cms-10.1177_12034754261453363 for Psychodermatologic Patient Education for Atopic Dermatitis Management: A Scoping Review and Evidence Map by Kevin Li, Michelle Sze Yiu Leung, Parsa Abdi, Serena Dienes, Tarek Turk, Xiaonan Chen, Liz Dennett, Sebastian Straube and Marlene Dytoc in Journal of Cutaneous Medicine and Surgery
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.