
Abstract
Background:
Hidradenitis suppurativa (HS) is a chronic, relapsing inflammatory skin disease lacking a standardized definition of disease control. While minimal disease activity (MDA) serves as a validated treatment target in psoriasis and atopic dermatitis, no equivalent framework exists for HS, limiting the implementation of treat-to-target strategies.
Objective:
To propose and validate clinically relevant MDA criteria for HS, integrating objective measures and patient-reported outcomes in a real-world cohort.
Methods:
Prospective, single-center, and observational study including all patients classified as well-controlled between April 2024 and January 2025. Sociodemographic, clinical, and therapeutic data were collected. In a paired analysis, a subgroup with prior moderate/poor control was compared against their pre-control.
Results:
Of 547 patients, 170 were classified as well-controlled. At assessment, 85.9% (146/170) had no active lesions, with a mean Localized Activity Index (LAI)—active areas/total affected areas—of 6%, and an International Hidradenitis Suppurativa Severity Score System (IHS4) of 0.38 ± 1.07. Symptomatic burden was minimal, with a mean global visual analog scale (VAS) of 1.24. In 114 paired patients, significant improvements were observed across all domains, including a 92% reduction in LAI and a 97% reduction in IHS4 (P < .0001). Factor analysis revealed 2 key dimensions—objective inflammation and patient-perceived symptoms—forming the basis for the proposed MDA definition: LAI ≤0.3, IHS4 ≤7, global/pain/suppuration VAS ≤3, and absence of structural progression. These criteria correctly identified 82% of well-controlled patients.
Conclusions:
This study introduces the first operational definition of MDA in HS, empirically derived and clinically feasible. Adoption of this framework could harmonize disease assessment, guide therapeutic targets, and advance precision management in HS.
Introduction
Hidradenitis suppurativa (HS) is a chronic inflammatory disease of the pilosebaceous unit, characterized by the recurrent development of painful nodules, abscesses, and draining tunnels in intertriginous areas.1 -3 Historically, treatment options for HS have been limited, but the advent of biologic therapies has significantly improved disease control and reshaped therapeutic expectations.4,5 Consequently, both clinicians and patients have adopted higher standards regarding treatment goals and long-term disease management.
Despite these advances, assessing disease control in HS remains challenging. Perceptions of adequate control often differ between clinicians and patients—and even among clinicians themselves—due to varying expectations and the subjective nature of disease burden. 6 Currently, there is no standardized tool to define or quantify the concept of “well-controlled” disease state in HS. While similar constructs have been developed in other chronic dermatologic conditions, such as psoriasis and atopic dermatitis, no consensus-based or operational definition exists specifically for HS.7,8 Given the multifaceted nature of HS—marked by clinical heterogeneity, episodic activity, and variable symptom perception—any such tool must integrate objective clinical parameters with patient-reported outcomes and remain sensitive to the dynamic course of the disease.6,9
Although complete and sustained remission remains the ultimate therapeutic goal, this is often difficult to achieve in real-world practice. As a result, there is an increasing need to define intermediate but clinically meaningful targets that can guide therapeutic decision-making and provide a standardized measure of disease control. One such concept is minimal disease activity (MDA), which has already been defined and validated in other chronic inflammatory skin diseases as a practical benchmark for adequate disease control.7,8
The aim of this study is to define and validate an operational construct of MDA in HS, grounded in real-world clinical data and designed to be easily applicable in daily dermatological practice.
Materials and Methods
Study Design
We conducted a prospective, single-center observational study at a dedicated HS clinic between April 2024 and January 2025.
Patient Selection
We included adult patients (≥18 years) with a clinical diagnosis of HS who were considered well-controlled at the time of assessment, based on the treating dermatologist’s clinical judgment. This expert evaluation routinely integrates both objective and subjective measures of disease severity and is applied to all patients to prioritize and organize scheduled follow-up visits. According to this approach, patients can be categorized into 3 groups: well-controlled, moderately controlled, or poorly controlled. Some patients were required to have documented medical records, including previous episodes of moderate or poor disease control, to enable intra-individual comparisons. Patients who refused to participate or had incomplete clinical data were excluded.
Variables of Interest and Data Collection
The primary outcome was the well-controlled disease state. The following variables were systematically extracted from electronic medical records:
Sociodemographic and biometric data: age, sex, and body mass index (BMI).
Clinical parameters:
Objective: disease duration, HS phenotype—according to both the classifications proposed by Martorell et al
10
and Molina-Leyva et al,
11
—refined Hurley stage, International Hidradenitis Suppurativa Severity Score System (IHS4), number of flares, treatment adherence—assessed using the Morisky-Green test
12
—and number of active anatomical areas. We also introduced a novel metric, the Localized Activity Index (LAI), defined as the ratio of currently active anatomical areas to the total number of areas affected, to provide a proportional and individualized measure of inflammatory burden. To the best of our knowledge, this is the first time that this concept has been proposed and applied in the context of HS. Subjective: patient-reported global disease severity, pain, and suppuration assessed using visual analog scales (VAS, 0-10).
Definition and Grouping of Candidate Domains
To explore the concept of MDA, we identified and grouped candidate items into 3 main domains: (1) active inflammatory burden (eg, IHS4, LAI), (2) symptomatic burden (eg, global, pain, and suppuration VAS), and (3) structural progression (eg, increase in number of active areas or draining tunnels).
Statistical Analysis
Descriptive statistics were used to characterize the study population. Continuous variables were expressed as mean and standard deviation (SD), and categorical variables as absolute and relative frequencies. The Shapiro-Wilk test was used to assess normality. Differences between pre- and post-control states were evaluated using Student’s t-test or Wilcoxon signed-rank test for continuous variables and chi-square or Fisher’s exact test for categorical variables, as appropriate. An exploratory factor analysis (maximum likelihood extraction with Varimax rotation) was performed to identify latent dimensions within the proposed MDA domains. Multivariate logistic regression was conducted to determine which variables were independently associated with well-controlled disease. To determine optimal cut-off values for each variable, we generated receiver operating characteristic (ROC) curves using disease control status (pre vs post) as the reference standard. Discrimination was summarized by the area under the curve (AUC) with 95% confidence intervals (CIs) obtained by bootstrapping (2000 replications). The Youden index (sensitivity + specificity − 1) was used to identify the most discriminative thresholds. Statistical analyses were performed using JMP version 14.1.0 (SAS Institute Inc., Cary, NC, USA) and P < .05 were considered statistically significant.
Ethics
The present study was approved by the Provincial Research Ethics Committee and is in accordance with the Declaration of Helsinki.
Results
Sociodemographic and Clinical Features
Out of 547 patients evaluated at the HS clinic, 170 (67 males, 103 females) were classified as well-controlled at the time of assessment. The mean age was 39.6 years (SD 14.6), with a long-standing disease duration of 15.4 years (SD 12) and an elevated mean BMI of 29.2 (SD 6.7). The majority exhibited an inflammatory (134/170, 78.8%) and lower phenotype (77/170, 45.3%). Sixty percent (102/170) of the patients were classified as refined Hurley stage Ia.
At the time of evaluation, 85.9% (146/170) had no active inflammatory lesions, and the mean LAI was 0.06 (6%). The mean IHS4 score was 0.38 (SD 1.07). Symptom burden was minimal, with a mean global VAS score of 1.24 (SD 2.08), and VAS scores for pain and suppuration of 0.72 and 0.65, respectively. Most patients (156/170, 92%) reported high adherence to prescribed treatments.
Clinical Improvement From Prior Disease States
From the initial cohort, a subgroup of 114 patients with documented periods of moderate or poor disease control—defined as sustained states classified as not well-controlled at routine clinical visits based on expert dermatologic assessment rather than isolated flares—was identified for paired analysis (Supplementary Figure S1). Baseline disease severity characteristics and concomitant treatment at both the well-controlled state and the preceding period of inadequate disease control are summarized in Table 1. Statistically significant improvements were observed across all clinical parameters following the achievement of better disease control. Specifically, patients showed a mean reduction of 11.1 points in IHS4, 0.74 in the LAI, 4.02 points in pain VAS, 2.54 points in suppuration VAS and 4 points in global VAS, corresponding to relative reductions of 96.8% (11.5/11.9), 92.1% (0.74/0.80), 84.6% (4.02/4.75), 79.2% (2.54/3.21), and 75.3% (4.00/5.31), respectively (all P < .0001). Importantly, no patient experienced an increase in the number of active anatomical areas or draining tunnels, supporting the stability of structural disease control (Supplementary Figure S2).
Disease Severity Characteristics and Concomitant Treatment Before and After Achieving Well-Controlled Disease in the Paired Cohort (n = 114).
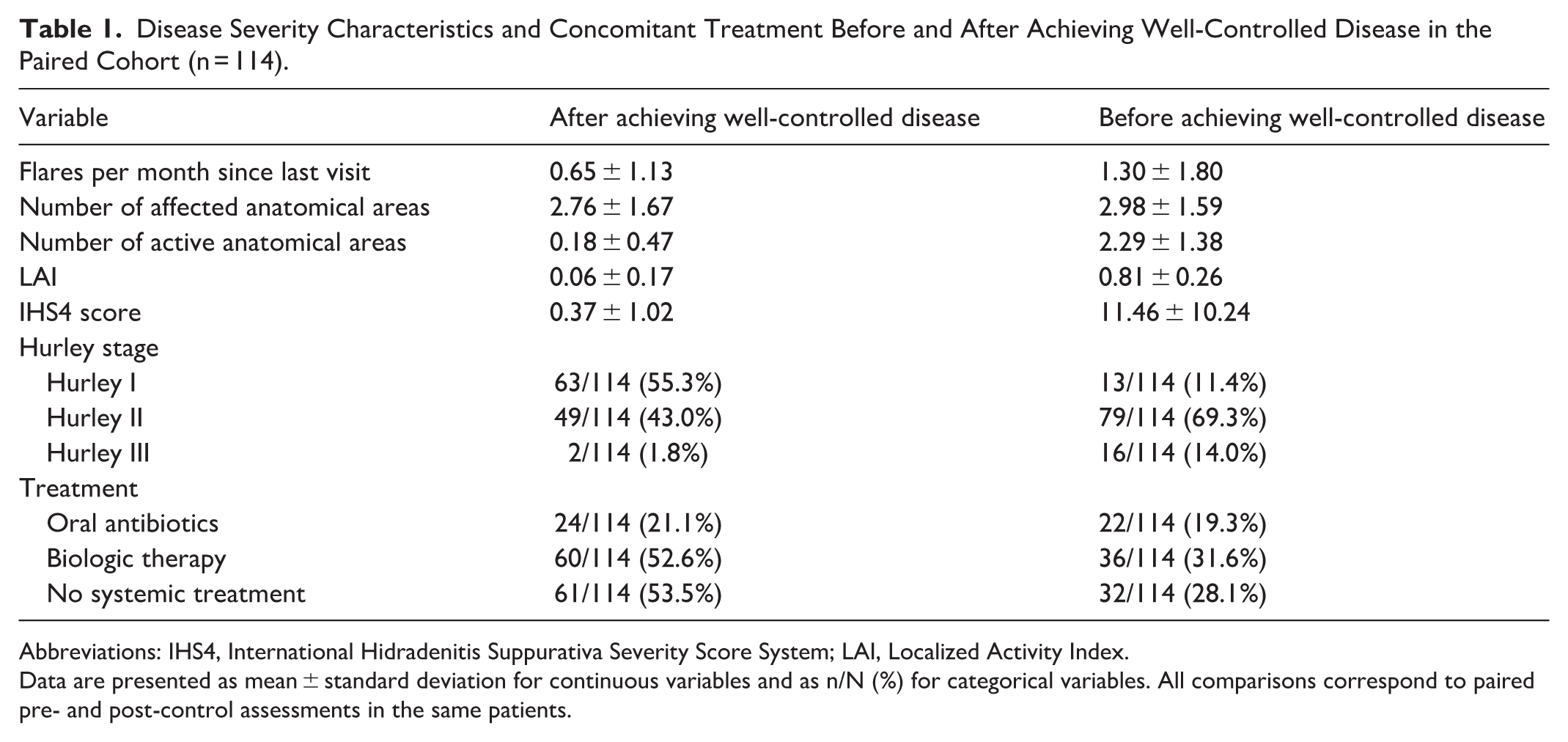
Abbreviations: IHS4, International Hidradenitis Suppurativa Severity Score System; LAI, Localized Activity Index.
Data are presented as mean ± standard deviation for continuous variables and as n/N (%) for categorical variables. All comparisons correspond to paired pre- and post-control assessments in the same patients.
Factor Analysis
An exploratory factor analysis using the maximum likelihood method with Varimax orthogonal rotation was performed to explore the latent structure of the proposed MDA domains. The analysis identified 2 factors with eigenvalues >1, which together explained 82.0% of the total variance (9.97/12.16). The first factor grouped subjective variables (global VAS, pain VAS, and suppuration VAS), while the second factor included objective inflammatory activity measures (IHS4 and LAI). The rotated factor loadings confirmed this bidimensional structure, with loading values above 0.5 in their respective domains. These results suggest the existence of 2 main dimensions in the assessment of well-controlled disease: patient-perceived symptomatic burden and objective inflammatory activity. This finding supports the inclusion of both domains in the operational definition of MDA in HS.
Logistic Regression Analysis
A multivariate logistic regression model was performed to identify clinical predictors independently associated with achieving MDA. The model showed excellent overall fit (χ2 = 136.5; P < .0001; R2 = 1.000). The most significant predictors were the LAI (χ2 = 190.8; P < .0001), global VAS (χ2 = 56.5; P < .0001), and suppuration VAS (χ2 = 13.8; P = .0002). By contrast, pain VAS and IHS4 did not reach statistical significance in the multivariate model, likely due to collinearity with other activity measures.
Determination of Optimal Thresholds
To determine the optimal thresholds for each clinical parameter included in the operational definition of MDA, individual ROC curve analyses were performed comparing patients’ status before and after reaching the well-controlled state. Internal validation by 2000 bootstrap replications confirmed excellent discriminative ability across all parameters. The IHS4 achieved an AUC of 0.99 (95% CI 0.98-1.00), with an empirical Youden cut-off around 2, supporting the clinically pragmatic threshold of ≤7 (sensitivity 1.00, specificity 0.60). The LAI also showed outstanding accuracy (AUC 0.98, 95% CI 0.96-0.99), with a Youden cut-off of ≈0.38, validating the predefined ≤0.3 threshold (sensitivity 0.89, specificity 0.97).
Symptom-based measures performed well, with AUCs of 0.86 for global VAS, 0.84 for pain VAS, and 0.72 for suppuration VAS, and optimal thresholds clustering around ≤3, consistent with clinical rationale and their distribution in the well-controlled cohort. Structural stability—defined as the absence of increased inflammatory areas or new draining tunnels—was confirmed in all cases meeting MDA.
Correlation matrices confirmed a strong association between LAI and IHS4 (r = 0.93) but only moderate correlations with VAS measures, reinforcing the independence of objective and symptomatic domains. These results support the robustness, clinical plausibility, and multidimensional nature of the proposed MDA criteria. Detailed metrics for each parameter are summarized in Supplementary Table S1, and their graphical representation is shown in Supplementary Figure S3.
Operational Definition of MDA
Based on the results, we established a set of operational criteria for defining MDA in HS. A patient was considered to meet MDA if all of the following conditions were fulfilled: (1) active inflammatory control, defined as a LAI ≤0.3 and an IHS4 ≤7; (2) symptomatic control, with global VAS, pain VAS, and suppuration VAS all ≤3; and (3) no structural progression, indicated by no increase in the number of active anatomical areas or in the number of draining tunnels since the previous visit. This proposed definition identified 82.2% of patients clinically classified as well-controlled and provides a practical, multidimensional framework for assessing disease control in real-world settings. The full criteria are summarized in Table 2.
Proposed Operational Criteria for Defining MDA in HS. Patients Were Considered to Meet MDA When All Listed Conditions Were Fulfilled, Encompassing 3 Domains: Inflammatory Control, Symptomatic Burden, and Structural Stability.

Abbreviations: IHS4, International Hidradenitis Suppurativa Severity Score System; LAI, Localized Activity Index.
Discussion
MDA in HS can be understood as a clinical state in which inflammatory activity is adequately controlled, symptomatic burden is minimal, and no therapeutic escalation is required. Based on our data, we propose a composite definition that integrates both objective measures of inflammation and structural stability, as well as patient-reported outcomes. This multidimensional approach aligns with recent international recommendations from the HiSTORIC consensus statement, which emphasize the importance of including both clinician-reported and patient-reported domains when evaluating treatment response and disease control in HS.7,13
Our findings strongly support the validity and clinical relevance of the proposed MDA criteria. When comparing patients before and after achieving well-controlled disease, we observed a 96.6% reduction in IHS4 and a 92% reduction in the LAI, confirming their value as objective markers of inflammatory control. In parallel, pain VAS scores decreased by 84.5%, and other symptom-related VAS scores (global severity and suppuration) showed reductions >75%, reinforcing the role of patient-reported outcomes. Importantly, structural stability—defined as no increase in the number of active anatomical areas or draining tunnels—was maintained in 100% of well-controlled patients, supporting its inclusion as a core component for assessing long-term disease control.
Each component of the proposed MDA definition demonstrated a significant association with well-controlled status, as shown in multivariate logistic regression and ROC curve analyses. Among these, IHS4, LAI, and global VAS emerged as the most powerful predictors. Although pain VAS and IHS4 did not reach statistical significance in the multivariate model—likely due to collinearity with other variables—they were retained in the final definition based on their strong clinical relevance, their contribution to distinct conceptual domains identified in the factor analysis (patient-perceived symptomatic burden and objective inflammatory activity), and their widespread use and validation in HS research and clinical practice. In addition, pain perception in HS may be partially underestimated, as patients often normalize chronic symptoms over time, which could attenuate its statistical weight despite clear clinical relevance. Their inclusion ensures a comprehensive assessment that balances statistical performance with clinical applicability, while remaining both evidence-based and aligned with established clinical frameworks used in HS. The final definition successfully identified 82.2% of patients classified as well-controlled in real-world practice, supporting its discriminative capacity; however, a non-negligible proportion of patients with residual disease burden may fall outside these criteria, highlighting that MDA should complement—rather than replace—clinical judgment.
Although an IHS4 score below 7 is traditionally classified as “moderate disease,” our findings suggest that such patients may still exhibit minimal residual activity when evaluated using a comprehensive and multidimensional approach. In particular, patients with an IHS4 ≤7 often showed low proportional inflammatory burden as reflected by a low LAI, absence of structural progression, and minimal patient-reported symptoms, indicating clinically meaningful disease control despite residual lesions. In our cohort, the mean IHS4 reduction exceeded 90%, largely reflecting the improvement of previously uncontrolled patients who had already surpassed their therapeutic window of opportunity. This highlights the unmet needs and limited granularity of the original IHS4 classification. Moreover, ultrasound assessment frequently revealed subclinical tunnels and inflammatory foci that may contribute to higher IHS4 values. External multicentric validation is currently underway to refine these cut-offs and confirm their generalizability.
A notable contribution of this study is the introduction of the LAI, a novel and simple metric that accounts for the proportion of anatomical regions with active inflammation relative to the patient’s total disease burden. This individualized and intuitive measure offers additional granularity compared to traditional scores and showed one of highest ROC performance in our cohort (AUC = 0.98). Importantly, IHS4 remains the primary measure of absolute inflammatory activity in our framework, while LAI was introduced as a complementary metric to capture proportional disease involvement; both criteria are required to be fulfilled simultaneously.
Taken together, these findings suggest that the proposed MDA definition is robust, clinically grounded, and feasible for use in routine dermatologic practice. It provides an intermediate yet meaningful therapeutic target, especially for patients in whom complete remission may not be achievable. Notably, the definition relies exclusively on clinical variables—without the need for laboratory data—making it particularly suitable for real-world settings. Its simplicity enhances its applicability in daily practice and opens the door to the development of practical tools, such as online calculators or digital applications that could streamline the evaluation of disease control and support clinical decision-making. 14
In this study, the concept of well-controlled disease was operationally defined by a single experienced dermatologist specialized in HS, integrating both clinical and patient-reported indicators routinely used in follow-up visits. This clinical judgment, while subjective, represents the current gold standard for disease control assessment in real-world HS practice, as no validated or universally accepted reference standard currently exists. The reliance on a single expert evaluator ensured internal consistency, although interobserver validation remains warranted.
The main limitations of this study include its single-center setting, which may limit generalizability. In addition, although the construct was validated using intra-individual comparisons and robust statistical methods, external validation is required. Finally, the classification of disease control was based on clinical judgment rather than a predefined gold standard, reflecting real-world practice but potentially introducing subjectivity.
Conclusions
To conclude, we are entering a new era in the management of HS, in which achieving maximal disease control must be a central therapeutic goal. Based on our findings, we propose the first operational definition of MDA in HS, grounded in real-world data and supported by strong statistical and clinical rationale. This framework may serve as a valuable tool to guide patient follow-up, assess treatment response, and improve standardization in both clinical care and research settings, while complementing clinical judgment in the evaluation of individual patients.
Supplemental Material
sj-docx-4-cms-10.1177_12034754261442925 – Supplemental material for Defining Minimal Disease Activity in Hidradenitis Suppurativa: A New Clinical Target
Supplemental material, sj-docx-4-cms-10.1177_12034754261442925 for Defining Minimal Disease Activity in Hidradenitis Suppurativa: A New Clinical Target by Carmen García-Moronta, Francisco Javier León-Pérez, Andrea Isabel Rodríguez-Sanna, Julia Castro-Martín, Alberto Soto-Moreno, Salvador Arias-Santiago and Alejandro Molina-Leyva in Journal of Cutaneous Medicine and Surgery
Supplemental Material
sj-tiff-1-cms-10.1177_12034754261442925 – Supplemental material for Defining Minimal Disease Activity in Hidradenitis Suppurativa: A New Clinical Target
Supplemental material, sj-tiff-1-cms-10.1177_12034754261442925 for Defining Minimal Disease Activity in Hidradenitis Suppurativa: A New Clinical Target by Carmen García-Moronta, Francisco Javier León-Pérez, Andrea Isabel Rodríguez-Sanna, Julia Castro-Martín, Alberto Soto-Moreno, Salvador Arias-Santiago and Alejandro Molina-Leyva in Journal of Cutaneous Medicine and Surgery
Supplemental Material
sj-tiff-2-cms-10.1177_12034754261442925 – Supplemental material for Defining Minimal Disease Activity in Hidradenitis Suppurativa: A New Clinical Target
Supplemental material, sj-tiff-2-cms-10.1177_12034754261442925 for Defining Minimal Disease Activity in Hidradenitis Suppurativa: A New Clinical Target by Carmen García-Moronta, Francisco Javier León-Pérez, Andrea Isabel Rodríguez-Sanna, Julia Castro-Martín, Alberto Soto-Moreno, Salvador Arias-Santiago and Alejandro Molina-Leyva in Journal of Cutaneous Medicine and Surgery
Supplemental Material
sj-tiff-3-cms-10.1177_12034754261442925 – Supplemental material for Defining Minimal Disease Activity in Hidradenitis Suppurativa: A New Clinical Target
Supplemental material, sj-tiff-3-cms-10.1177_12034754261442925 for Defining Minimal Disease Activity in Hidradenitis Suppurativa: A New Clinical Target by Carmen García-Moronta, Francisco Javier León-Pérez, Andrea Isabel Rodríguez-Sanna, Julia Castro-Martín, Alberto Soto-Moreno, Salvador Arias-Santiago and Alejandro Molina-Leyva in Journal of Cutaneous Medicine and Surgery
Footnotes
Acknowledgements
This article will be part of the doctoral thesis of Carmen García-Moronta.
Ethical Considerations
The study was approved by the local Ethics Committee and conducted in accordance with the principles of the Declaration of Helsinki.
Author Contributions
Carmen García-Moronta: conceptualization, methodology, formal analysis, writing—original draft preparation. Francisco Javier León-Pérez: writing—review and editing. Andrea Isabel Rodríguez-Sanna: writing—review and editing. Julia Castro-Martín: writing—review and editing. Alberto Soto-Moreno: writing—review and editing. Salvador Arias-Santiago: writing—review and editing, supervision. Alejandro Molina-Leyva: conceptualization, writing—review and editing, supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.