
Abstract
Background:
The Ontario Health Insurance Plan (OHIP) insures appointments for the assessment and diagnosis of hair loss, or alopecia. Although anecdotal, discussion suggests that, increasingly, dermatologists decline to see referrals of this nature. There has been a lack of objective surveillance to determine the proportion of dermatologists in practice who accept referrals for this concern.
Objectives:
This study investigated the proportion of dermatologists in Ontario accepting OHIP referrals for hair loss. Secondary objectives included wait times, consultation fees for non-OHIP visits, and factors affecting referral acceptance or rejection.
Methods:
A cross-sectional telephone survey was conducted, in which 284 dermatologists’ offices listed by the College of Physicians and Surgeons of Ontario (CPSO) were contacted. The study investigated the acceptance of OHIP referrals for hair loss, wait times, additional referral requirements, and private consultation fees. Descriptive statistics were employed to summarize data.
Results:
Of the 284 offices contacted, 38.38% (109/284) accepted OHIP referrals for hair loss, 48.59% (138/284) did not, and 13.03% (37/284) were unavailable for contact. The average wait time for offices that accepted referrals was 4.51 ± 4.07 months. Non-OHIP consultation fees ranged from $135 to $299 CAD. Some offices limited acceptance to specific conditions such as alopecia areata and male androgenetic alopecia.
Conclusion:
A total of 48.59% of dermatologists in Ontario do not accept OHIP referrals for hair loss, while the status of 13.03% remains unknown. This reality raises concerns about accessibility to care. Further research is needed to investigate factors influencing referral acceptance.
Introduction
Dermatology is a unique field of medicine in which the diagnosis of, treatment for, and prevention of skin, hair, and nail disorders are made. 1 This specialty plays immense importance in our health system; skin disorders affect 30% to 70% of people globally. 1 Within this field, the assessment and treatment for hair loss represents an important aspect of the field of dermatology due to its significance in a person’s medical and psychological well-being.2,3
The Canada Health Act states that all Canadians should have continuous access to health care without barriers to ensure the continued improvement and well-being of all.4,5 This act was intended to serve as sufficient legislation to ensure that all Canadians have equal access to health care. In recent years, however, it has been questioned whether the Canadian health care system has the capacity to adequately serve the growing population. 4 The Canadian health care system is both federally and provincially administered using a publicly funded health care system known as Medicare, which has 13 provincial and territorial insurance plans. Each health care insurance plan must meet the standards of public administration, comprehensiveness, universality, portability, and accessibility outlined in the Canada Health Act. 5 The plan in Ontario is known as the Ontario Health Insurance Plan (OHIP). The OHIP is a vital means by which patients obtain access to medical services to Canadians including access to specialists such as dermatologists.
Ontario has the largest provincial population with over 15 million residents, each of whom may require the care of a dermatologist on a short-term or chronic basis. Ideally, Ontarians, and Canadians in general, would have access to an adequate supply of dermatologists to meet the demand of the population.6,7 Despite the importance of dermatological care, there have been anecdotal reports, which suggest that some dermatologists in Ontario are no longer accepting patients referred for hair loss assessments through the OHIP. This raises concerns about the accessibility of care for individuals suffering from hair loss, a condition that affects a significant portion of the population and can severely impact quality of life both physically and psychologically.3,8 Despite the prevalence of hair loss, there are limited data on the availability of dermatologists’ acceptance of OHIP referrals for the assessment of hair loss in Ontario.
This study aimed to determine the proportion of dermatologists who accept medical OHIP referrals for hair loss.
Methods
Study Design
A cross-sectional study was conducted in which a telephone script was used to survey whether dermatologist offices in Ontario accept referrals from primary care providers (PCPs) for the diagnosis of and treatment for hair loss. The study size of 284 offices was based on registration of dermatologists with the College of Physicians and Surgeons of Ontario (CPSO) with independent practice certificates in Ontario. This cohort reflects all dermatologists in Ontario who, theoretically, were available during the study period. Secondary data on wait times, the price of consultations that are not OHIP-insured, and the criteria dermatologists employ with acceptance or rejection of a referral were obtained. The inclusion criteria were limited to offices with dermatologists holding an active CPSO license. Offices that could not be reached were classified as “unavailable” and included in the final analysis as its own separate category.
Telephone Survey
The telephone survey did not disclose the purpose of the study to minimize the risk of response bias. The researcher (VY) contacted the dermatologists’ offices via telephone from a patient perspective, inquiring about their ability to access care with a referral for hair loss. A standardized script was used to contact each office to maintain the comparability of assessment methodologies (Figure 1). The phone calls were made on Tuesday or Wednesday mornings between the hours of 9:00 AM to 12:00 PM during the months of April to June to avoid variability that might be influenced by the time or day of the week. All of the self-reported data were collected through the telephone survey. To minimize selection bias, offices were contacted multiple times (minimum of 5 attempts) if unreachable during the standardized times and days.
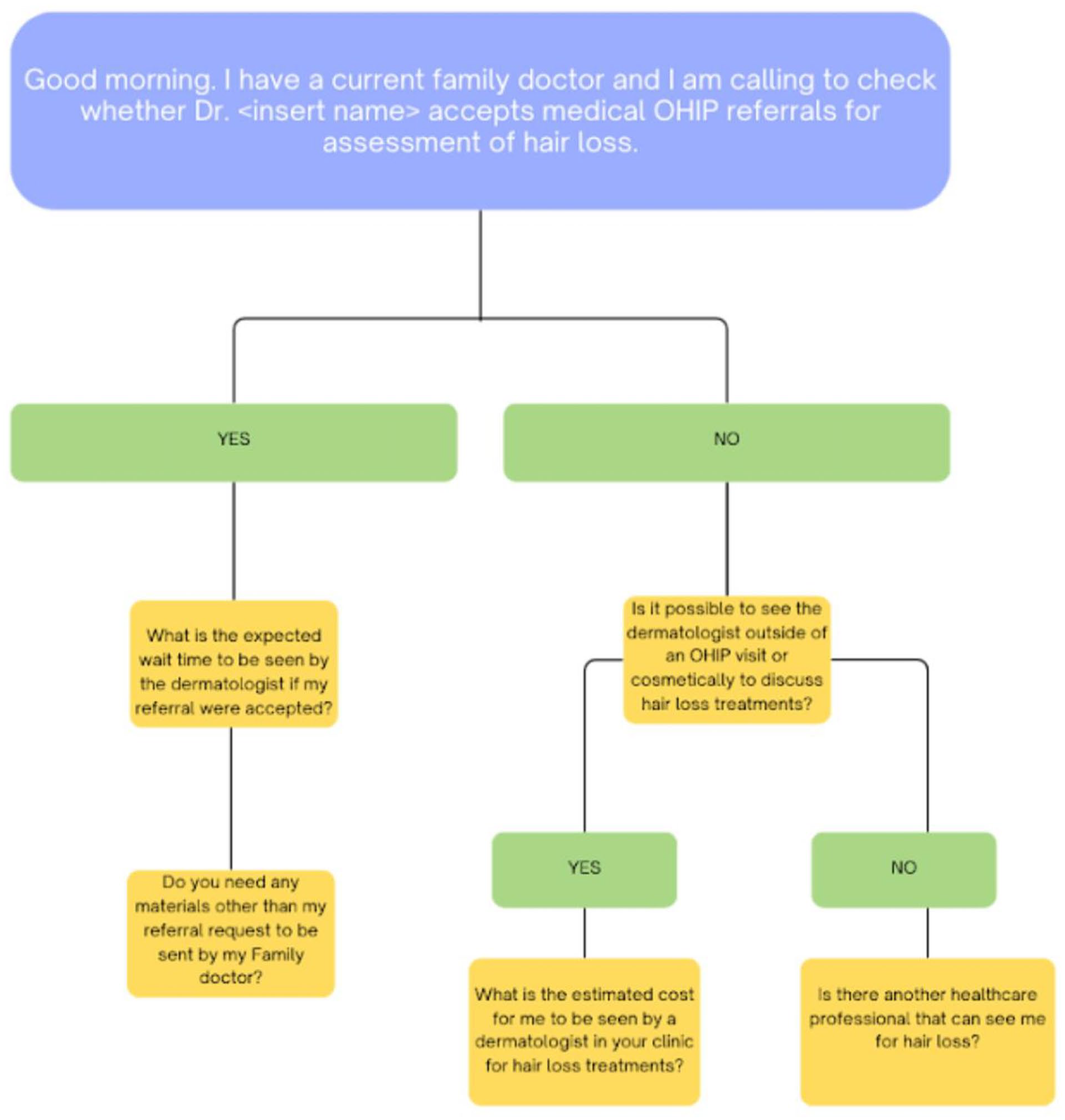
Telephone script used in cross-sectional study of dermatologist offices in Ontario.
Outcome Measures
Acceptance of OHIP referral for the assessment of hair loss was the primary outcome of interest. Wait time to be seen by a dermatologist (measured in months), materials other than a referral required to be sent from a family doctor or nurse practitioner, cost to see a dermatologist cosmetically (measured in Canadian dollars), and the availability of other health care practitioners to assess hair loss were the secondary outcomes collected. The primary focus of the study was to determine whether Ontario dermatology offices accept hair loss or alopecia referrals; thus, no specific diagnostic criteria for hair loss were applied.
The Ethics Committee of the University of Toronto waived the need for ethics approval and participant consent for the collection, analysis, and publication of the retrospectively obtained and anonymized data for this noninterventional study.
Bias
A standardized script was used to prevent interviewer bias, and multiple attempts were made to contact each office to further reduce bias. Selection bias was addressed by including the remaining unreachable offices in the final analysis.
Statistical Methods
The data gathered from the telephone survey was organized into a centralized database created for the study. The information was then summarized in table form using descriptive statistics (mean, standard deviation [SD], etc). We used the Strengthening the Reporting of Observational Studies in Epidemiology cross-sectional checklist when writing our report. 9
Results
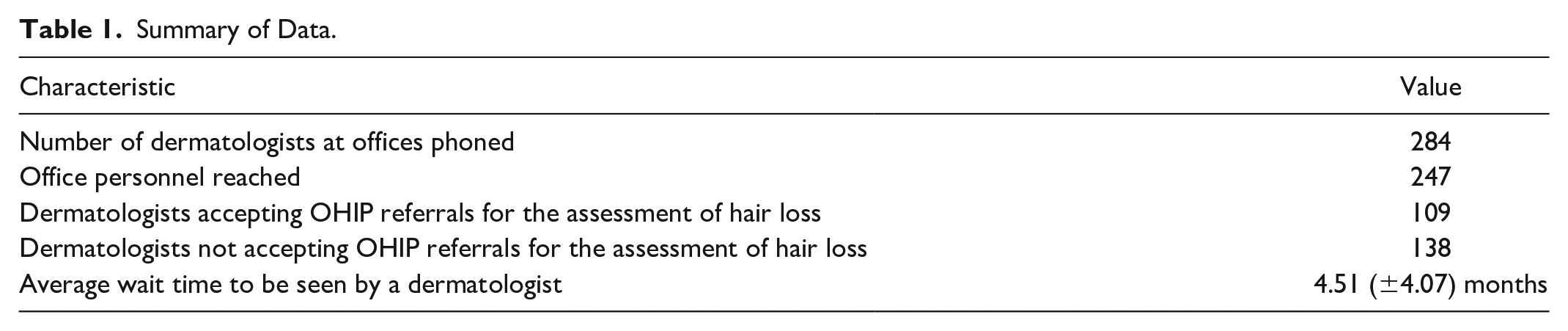
Results indicate that 38.38% (109/284) of the dermatologists at surveyed offices accepted OHIP referrals for the assessment of hair loss. Meanwhile, 48.59% (138/284) did not accept referrals, and 13.03% (37/284) were unavailable for contact. The reasons for unavailability included not being reachable by phone, dermatologists practicing elsewhere in Canada, dermatologists practicing outside of Canada (such as in the United States), or having retired. For the offices that were unavailable to contact, the researcher phoned at least 5 times throughout the survey period before deeming it unavailable. Among the offices that accepted patients, the average wait time to see a dermatologist was approximately 4.51 (±4.07) months. The cost for an initial hair loss consultation outside of OHIP coverage or for cosmetic consultations ranged between $135 and $299 (Table 1). Additionally, there were noted restrictions in the offices accepting OHIP referrals for hair loss. For instance, some limited assessments to specific diagnoses such as alopecia areata or male androgenetic alopecia.
Summary of Data.
Discussion
The results of this cross-sectional study indicate that almost half of dermatologists practice in Ontario, who are registered with an independent practice certificate by the CPSO, do not accept referrals for hair loss under the OHIP. This phenomenon is in place despite the schedule of benefits from the ministry of health and long-term care that includes dermatological consultation as an insured benefit for alopecia or hair loss with the applicable diagnostic code 704. 10
There are several potential reasons why dermatologists choose to decline referrals for patients with hair loss. Assessments for alopecia tend to be more complex and of a longer duration, particularly when a single patient has multiple diagnoses. 11 In a fee-for-service model of care, having a patient encounter that is of longer duration can impact the number of patients seen within a clinic and decrease overall remittance. Correspondingly, the remuneration for hair loss referrals, as for general medical dermatology consultations, has increased at a rate of 13% (from $72.15 to $81.55 CAD) whereas, in today’s dollars, equivalent remittance for consultations, with respect to inflation, would be $92.40 CAD.10,12 Ontario’s fee model, mandated by government policies rather than market forces, further limits the number of dermatologists with capacity to care for skin, nail, and hair disorders. As a result, dermatologists are forced to make a difficult decision about which conditions to prioritize. There is also the psychological burden and anxiety associated with patients experiencing hair changes, which some dermatologists may feel ill-equipped to manage or simply wish to avoid. 8 From a therapeutic perspective, there are very few on-label therapies for alopecia, particularly when alopecia has evidence of scarring. As practitioners who desire to assist patients and improve their condition, it can be frustrating and disheartening to lack effective medical treatments to offer patients that can regrow hair.
The lack of uptake of referrals specifically for alopecia has several implications. Perhaps the most obvious pertains to the deficit in patient care or unmet patient need. Although the burden of hair loss is difficult to quantify in a Canadian context, the fact that there is 1 dermatologist for 57,000 Ontarians, already a shortage of supply, means that alopecia concerns would be assessed by a minority of dermatologists in the province, at an even higher ratio of 1 dermatologist: ~130,000 Ontarians. 13
At a more granular level, the study results reveal that some of the teaching hospitals in Toronto do not accept new referrals for alopecia. (The caveat of one teaching hospital is that referrals for “alopecia areata” are accepted; however, this precludes that the referring physician or nurse practitioner is able to correctly make this diagnosis at the time of referral.) There was a tertiary hair loss referral clinic at the Women’s College Hospital in Toronto from 2012 to 2023; however, the clinic was eventually discontinued after 1 dermatologist moved their practice out of the province (2016) and the other decided to centralize dermatology practice at a single private-office site (2023). In its totality, these policies result in a downstream effect of future dermatologists not receiving exposure to alopecia cases and therefore lacking sufficient experience with diagnosing these patients, developing treatment plans, and subsequently seeing such patients in follow-up. Ultimately, this may result in a cyclical lack of care for this aspect of dermatology. Academic dermatologists often have a specific subspecialty, which can further limit their ability to accept certain referrals. A solution could be to establish general dermatology teaching clinics at academic institutions that accept all conditions.
This unmet patient need also creates opportunities for unlicensed health providers, such as trichologists, to assume the role of assessor, diagnostician, and therapy-provider for patients with hair conditions. These assessments occur by individuals without medical training, 14 outside of the purview of the OHIP, and often cost patients several hundreds of dollars privately with means of assessing and treating hair loss that can have questionable validity or lack evidence.
The results of this study also imply that dermatologists—the medical experts in diseases of hair—may consider hair loss diagnosis and management of lesser importance to include within their practice, although this remains a hypothesis that requires further investigation. Understandably, these dermatologists may identify that there is limited mortality associated with hair loss compared with various forms of skin cancer and inflammatory diseases. However, patients experiencing hair loss cite morbidity and psychosocial impact as significant factors of their disease. 15 For a dermatologist who performs medical consultations, the elimination of alopecia referrals may enable appointment time for other referral concerns and thereby help limiting the time patients await appointments for other concerns. The question then arises whether, with almost 49% of registered dermatologists not seeing alopecia referrals, despite its inclusion on the schedule of benefits, whether the assessment of alopecia should be delisted officially. To this end, it is notable that there were 5 offices, which did not accept OHIP-based hair loss referrals from a PCP, but they permitted patients to book appointments to be assessed for hair loss treatments that are billed privately outside of the OHIP.
The study has limitations, which include that a proportion of offices were unreachable, despite having been called on 5 separate occasions. It is possible that in some of these offices, OHIP referrals for alopecia are accepted. By its nature, a cross-sectional study is not continuous. This means that offices surveyed from April to June 2024 may have indeed updated or changed their policy in the interim. Another limitation is that dermatologists themselves were not accessed or interviewed to ensure their personal scopes of practice. This scope would be particularly important for dermatologists who practice in multiple offices—perhaps they see hair loss patients at 1 office, but not another. However, it is also common to contact a dermatologist’s office and inquire about referral matters and confirm scope of practice with an office employee, hired and delegated by the dermatologist to do so. This study design also did not examine factors such as urban and rural practice settings, full-time and part-time work schedules, or solo and group practice models, which may affect referral acceptance. Future studies should explore these variables to further access to dermatological care. Another limitation is that the investigation was limited to hair loss; it is possible that other conditions like acne or psoriasis are also restricted in their acceptance. Future studies may also attempt to access dermatologists via a poll or other feedback means to determine which factors have demotivated them to accept alopecia referrals, and even help provide solutions to remedy the issue (eg, increased remuneration, therapeutic advancements, insured on-site allied health for disease and treatment counselling, etc).
Conclusion
The results of this study reveal the lack of accessibility of dermatological care for OHIP-insured individuals suffering from hair loss in Ontario, as evidenced by only 38.38% of dermatologists’ acceptance of hair loss referrals. For those whose referral is accepted by a dermatologist, the wait time is estimated to be 4.5 months based on the survey that further exacerbates the issue, potentially leading to worse outcomes and prolonged distress for these patients. The survey also revealed that some offices also have limited acceptance criteria, such as specific types of hair loss or patterns like alopecia areata and androgenetic alopecia limited to males or have restrictions in place to see more severe cases, which increases barriers to access of care.
It is important to recognize that the challenge is not likely a simple matter of dermatologists refusing to accept referrals but rather symptomatic of a broader systemic issue that encompasses the state of our health care system in which there is an overwhelming demand for dermatological services in general without commensurate increased supply, increasing the risk of burnout among physicians and other allied health professionals.16-18
These findings demonstrate a need for future research into the factors that influence the limited acceptance of OHIP referrals for hair loss. Future research could investigate why dermatologists have eliminated these referrals and what systemic barriers might have contributed to the situation. It would also be valuable to determine which types of non-OHIP procedures dermatologists are offering for hair growth to gain insight on the potential shift from prescription medical to cosmetic and self-pay services within the field. Finally, input from actual patients on the impact of having hair loss coupled with a relative lack of access to dermatologist assessment, as well as patient preferences of delivery of care would provide valuable insight.
Supplemental Material
sj-docx-1-cms-10.1177_12034754251324941 – Supplemental material for The Dermatologist is Out? Assessment of Dermatologists in Ontario Accepting Ontario Health Insurance Plan (OHIP) Referrals for Hair Loss Evaluation
Supplemental material, sj-docx-1-cms-10.1177_12034754251324941 for The Dermatologist is Out? Assessment of Dermatologists in Ontario Accepting Ontario Health Insurance Plan (OHIP) Referrals for Hair Loss Evaluation by Victoria Young and Renée A. Beach in Journal of Cutaneous Medicine and Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Memberships on advisory boards or speakers’ bureau: Bausch, Loréal—Vichy, CeraVe; Pfizer.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Approval Status
IRB Exempt.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.