
Abstract
Primary psychodermatologic disorders such as body dysmorphic disorder, trichotillomania, and excoriation disorder present significant challenges in dermatological and psychiatric assessment due to their complex psychological and dermatological symptoms. Reliable and valid screening tools are essential for effective diagnosis and management, yet there is a lack of consensus on the most appropriate instruments. A systematic review was conducted, identifying 81 studies that employed 45 different psychodermatologic tools, of which 13 studies provided empirical data on their diagnostic accuracy. Tools were assessed for their psychometric properties, including sensitivity, specificity, reliability, and validity. The Body Dysmorphic Disorder Questionnaire (BDDQ) and its variants demonstrated high diagnostic accuracy, with the BDDQ showing a sensitivity of 0.97 [95% CI: 0.82-1.00] and specificity of 0.91 [95% CI: 0.86-0.95]. The Skin Picking Scale-Revised showed high diagnostic accuracy for excoriation disorder, with a sensitivity of 0.89 [95% CI: 0.84-0.94] and specificity of 0.95 [95% CI: 0.93-0.96]. Similarly, the Massachusetts General Hospital Hairpulling Scale, frequently utilized for trichotillomania, exhibited strong psychometric properties, with a sensitivity of 0.90 [95% CI: 0.81-0.96] and specificity of 0.72 [95% CI: 0.63-0.80]. Despite their frequent use, many tools lack a comprehensive assessment of the full range of symptoms, including social impairment and behavioural nuances. The review highlights the importance of developing standardized, multidimensional assessment tools that are valid, reliable, and easy to implement in daily practice. Further research is needed to establish the practical utility of these tools in routine dermatology settings, addressing gaps in effectiveness, referral and intervention limitations, and patient acceptability.
Keywords
Introduction
Psychodermatology, also known as psychocutaneous medicine, examines disorders at the intersection of psychiatry and dermatology. Despite its longstanding presence, this field has often been overlooked. 1 A survey assessing the training, awareness, and attitudes of dermatologists toward psychodermatology revealed that only 18% had a clear understanding, while 39% expressed interest in continuing medical education on psychodermatologic disorders (PPDs). 2 It is estimated that 30% to 40% of patients seeking dermatological treatment have an underlying psychiatric or psychological issue contributing to or exacerbating their skin condition.3,4 Primary PPDs, which are psychiatric disorders presenting with dermatologic symptoms, include conditions such as delusional parasitosis, trichotillomania, and pathological skin picking (excoriation) disorder (SPD). 5 Research has demonstrated that patients with PPDs experience significantly reduced quality of life; however, these disorders are often misunderstood and underdiagnosed. 6
Given the substantial psychological and social impact of PPDs, effective identification and management strategies are critically needed. To conceptualize the pathway from screening to intervention in psychodermatology, we present a framework (Figure 1) that adapts elements from established mental health screening models. 7 Despite the critical importance of early detection and comprehensive management, there is a notable gap in the literature regarding the reliability and validity of screening tools specifically designed for PPDs. Many existing studies lack robust methodologies, and there is a pressing need for standardized assessment tools applicable across various clinical settings. 8
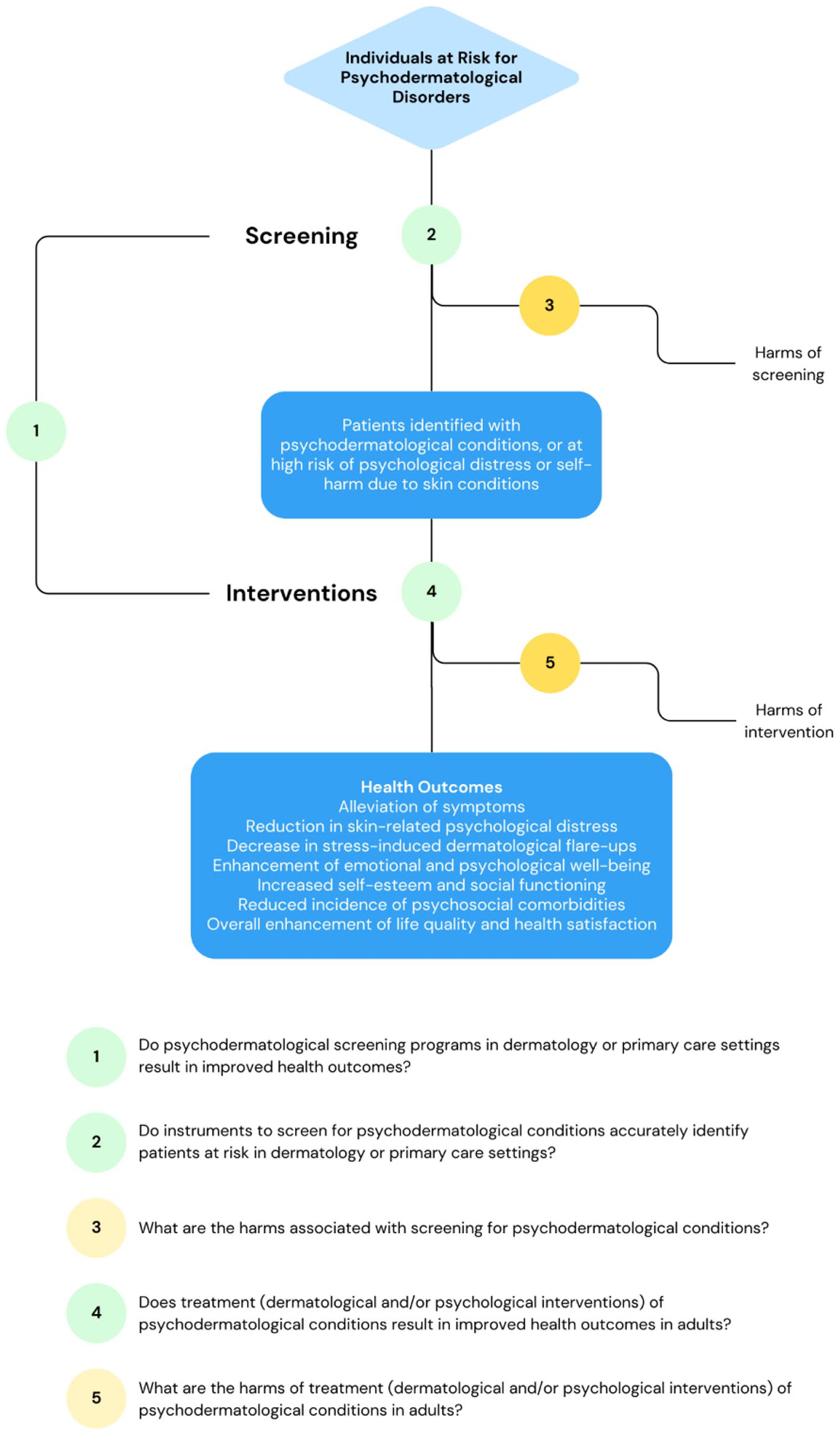
Proposed conceptual framework for psychodermatologic screening and interventions.
This systematic review aims to address these gaps by evaluating the current psychodermatologic screening tools and their diagnostic accuracy.
Materials and Methods
Study Design
This systematic review adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and is registered in the International Prospective Register of Systematic Reviews (PROSPERO) database (CRD42023484488). 9
Search Strategy
A sensitivity literature search was conducted from the inception date of the review to November 12, 2023, across 5 electronic databases, namely Scopus, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), Embase, and PsycInfo. The search focuses on studies highlighting mental health instruments used in dermatology, specifically targeting diagnostic criteria, screening tools, and assessment measures for psychodermatologic cases. To find target articles, an initial examination of relevant terms and their combinations was conducted to refine the search strategy considering Medical Subject Headings (MeSH) as well as non-MeSH phrases. A detailed list of search terms and strategies is available in Supplemental Table 1. In addition, manual searches were conducted in the reference lists of relevant studies to ensure comprehensive coverage.
Eligibility Criteria
Following the electronic database search, studies were chosen according to predetermined criteria for inclusion: (1) studies involving dermatology patients of any age, gender, or ethnicity; (2) studies that evaluate the validity, reliability, and clinical utility of assessment tools specifically developed or used for the identification of primary psychodermatologic conditions; (3) research that includes patients diagnosed with specific PPDs, where psychological factors are the primary cause of dermatologic symptoms; (4) studies that describe or validate diagnostic criteria, screening instruments, or assessment measures explicitly designed for psychodermatologic conditions; and (5) research conducted in various healthcare settings that specialize or have provisions for psychodermatology, including specialized clinics, psychiatric settings, and dermatology departments with an integrated mental health approach. The criteria for excluding studies from the systematic review were as follows: (1) studies focusing solely on mental health or dermatologic conditions without an integrated approach; (2) research lacking sufficient information on psychodermatologic symptoms, diagnostic criteria, or screening tools; (3) research that does not distinguish between primary psychodermatologic conditions and dermatologic symptoms secondary to generalized psychiatric disorders; and (4) animal studies or in vitro research without direct relevance to human patients. There were no limitations on the selection of studies based on factors such as date, language, or geographical location.
Data Extraction
All identified studies were uploaded into the Covidence systematic review software and the selection of included studies involved screening of titles and abstracts, followed by full-text review and data extraction. After duplicate removal, 3 independent reviewers (C.C., P.A., and K.L.) reviewed articles for eligibility based on the predefined criteria, with disagreements resolved through discussion or consultation with a fourth reviewer (T.T.). Data extraction was conducted using a standardized form, which captured key study characteristics, participant demographics, specific psychodermatologic conditions being investigated, characteristics of the screening tools used, and the main outcomes. The sensitivity, specificity, likelihood ratios, predictive values, and binomial 95% confidence intervals (CI) were computed for sensitivity and specificity using Reference Manager (RevMan) version 5.3 from the Cochrane Collaboration. 10
Measures of Reliability and Validity
The reliability and validity of each psychodermatologic screening tool were evaluated using a variety of established metrics. Cronbach’s alpha (α) was used to assess internal consistency, with values ranging from .71 to 1.00 considered acceptable to excellent. 11 Tools were also evaluated using Macdonald’s omega (ω) for internal consistency based on factor analysis, where scores of .71 or higher indicated acceptable reliability. 12 Intraclass correlation coefficients measured the agreement between raters or over multiple administrations, with values above .90 regarded as excellent. 13 To assess the stability of these tools over time, test-retest reliability was used, with scores above .76 indicating excellent reliability. 14 Area under the curve values provided insight into diagnostic accuracy, where values greater than 0.90 indicated excellent diagnostic performance. 15 Convergent validity was considered strong for correlation coefficients (r) above .71. 16 Construct validity was evaluated through confirmatory factor analysis, with comparative fit index values above 0.95 indicating excellent model fit, and root mean square error of approximation values below 0.05 considered ideal.
Quality Assessment
Considering the variety of study designs in the articles included, the Mixed Methods Appraisal Tool (MMAT) was used for quality assessment. 17 Each study was evaluated based on its methodological category: qualitative, quantitative descriptive, quantitative randomized, quantitative non-randomized, or mixed methods research. The MMAT consists of 2 parts, a 2-question screening checklist (Part I) and a 5-question explanation of the criteria (Part II). Studies that reported a response of “No” to one or more of the screening questions were excluded. For each criterion within the MMAT, the presence or absence was scored as 1 or 0, respectively. The score for each article was calculated by dividing the total points scored by the total possible points, resulting in a score out of 7. Each article was classified as weak (≤4/7), moderate-weak (5/7), moderate-strong (6/7), or strong (7/7) in terms of study quality. Discrepancies in quality assessments between reviewers were resolved through consensus. Detailed assessment of MMAT for individual studies is shown in Supplemental Table 2.
Results
Search Results
A total of 2730 studies were identified during the initial database search. After removing duplicates, 1851 studies remained. Initial screening based on titles and abstracts resulted in the remainder of 155 studies for full-text review. Following a detailed examination, 74 studies were further excluded due to reasons such as inadequate data reporting, wrong patient population, or wrong study design. Ultimately, 81 studies met all inclusion criteria and were included in this systematic review and meta-analysis. The selection process is comprehensively illustrated in the PRISMA flow diagram (Supplemental Figure S1).
Study Characteristics
The final 81 studies selected included a total of 45 specific psychodermatologic screening and assessment tools. Among these, 41 studies focused on the evaluation of body dysmorphic disorder (BDD), 23 for trichotillomania, 23 for SPD, and 3 for psychogenic pruritus (Supplemental Table 3). The majority of studies were conducted in North America (36), followed by Europe (26), Australia (9), Asia (6), and South America (4). The included studies spanned a range of settings, from monocentric or polycentric outpatient clinics (51), university settings (16) to online surveys (14). All the articles included in this systematic review assessed using the MMAT were rated equal to or above a score of 4/7 (average score 5.88, standard deviation 0.87). Of the included studies, 21 were rated as strong (7/7), 34 as moderate-strong (6/7), 21 as moderate-weak (5/7), and 5 as weak (≤4/7). A detailed summary of the characteristics of the included studies is presented in Supplemental Table 3.
Trichotillomania
Twenty-three studies addressed the evaluation of trichotillomania using 11 tailored psychodermatologic screening or assessment tools. The most used tools to evaluate trichotillomania were the Massachusetts General Hospital Hairpulling Scale (MGH-HPS) and the Milwaukee Inventory for Styles of Trichotillomania-Adult Version, totaling 7 and 5 validations, respectively. Most other tools only had 1 or 2 validation studies. The evaluation tools for trichotillomania exhibited a range of complexity, from the single-item National Institute of Mental Health Trichotillomania Impairment Scale (NIMH-TIS) to the 27-item Hairpulling Distress and Impairment Scale, which features a 3-factor structure. The instruments predominantly utilized a 1-factor structure, with 10 or fewer items (Supplemental Table 4). Most assessment tools were patient-rated, offering individuals the autonomy to self-report the severity and impact of their hair-pulling behaviour. However, there are 5 clinician-rated scales, namely the Psychiatric Institute Trichotillomania Scale, NIMH-TIS, NIMH Trichotillomania Severity Scale, Yale-Brown Obsessive-Compulsive Scale (YBOCS) for Trichotillomania, and the Trichotillomania Diagnostic Inventory. The Trichotillomania Scale for Children (TSC) has been developed as a measure that can be completed by children themselves or by their parents, offering a comprehensive view from both the child’s (TSC-C) and the parent’s perspective (TSC-P).
Excoriation (skin picking) disorder
Eleven personalized tools for assessing SPD across 23 different studies were identified (Supplemental Table 5). The Skin Picking Scale-Revised (SPS-R) emerged as the most frequently validated instrument with 5 studies, followed by the Skin Picking Impact Scale (SPIS) which was the subject of 3 studies. Most assessment tools followed a 1-factor structure, and almost all were under 15 items in length. Both the Milwaukee Inventory for the Dimensions of Adult Skin Picking (MIDAS) and the SPS-R are self-reported and have 2 scales used for the assessment of excoriations. The MIDAS was developed and validated as a 2-factor structure to distinguish between automatic (unconscious) and focused (conscious) picking, while the SPS-R offers 2 subscale scores for “impairment” and “symptom severity.” The YBOCS modified for neurotic excoriation is a 10-item clinician-administered tool, which also contains 2 subscales, assessing picking urge/thought and picking behaviour. Two assessment tools, namely the Diagnostic Interview for Skin Picking Problems (DISP) and the questionnaire on excoriation-related context by Misery et al, 18 did not utilize a Likert scale. The DISP comprises 16 items structured to evaluate both diagnostic criteria and clinical characteristics of SPD and were categorized into 4 domains. Snorrason et al also created a nearly identical diagnostic interview for trichotillomania; however, this scale was not utilized in any present works. 19 Unlike the assessment tools for trichotillomania and BDD, none of the SPD instruments were specifically designed to cater to adolescents and pediatric populations.
Body dysmorphic disorder
A variety of tools have been validated to assess BDD across multiple studies (Supplemental Table 6). The most frequently validated instruments include the Body Dysmorphic Disorder Questionnaire (BDDQ) and the YBOCS modified for BDD, each with 5 studies confirming their validity. Most assessment tools follow a 1-factor structure, with some using 2-factor structures, and generally consist of fewer than 35 items.
Psychogenic pruritus and transdiagnostic scales
There were limited studies utilizing screening or assessment tools for psychogenic pruritus (functional itch disorder/somatoform pruritus). Three studies utilized the Neuroderm Questionnaire consisting of 20 questions, where each question offers a number of categorical responses, any of which the patient can select.20-22 Although the Neuroderm Questionnaire was designed for chronic pruritus, it has shown adequate reliability in discriminating between psychogenic and non-psychogenic pruritus in clinical settings.20,21 Four assessment tools were identified as transdiagnostic scales, which identified more than one primary psychodermatologic condition including BDD, trichotillomania, and SPD. The Repetitive Body Focused Behaviour Scale, the Generic BFRB Scale-8, and the Body-focused Self-damaging Behavior Expectancies Questionnaire all screened for body-focused repetitive behaviours including skin picking, hair pulling, nail biting, and lip-cheek biting.23-25 All 3 tools demonstrated adequate reliability and validity and were recommend being used as a complement to symptom-specific scales clinically and in clinical trials due to the high comorbidity prevalence in body-focused repetitive behaviours. The Obsessive-Compulsive and Related Disorders-Dimensional Scales-Expanded is a comprehensive self-report scale designed to assess a wide range of obsessive-compulsive and related disorders, demonstrating excellent internal psychometric properties, adequate test-retest correlations, and good validity in detecting BDD, trichotillomania, and SPD. 26
Diagnostic Accuracy in Identifying Psychodermatology Patients
Limited studies reported quantitative measures of diagnostic performance for psychodermatologic assessment tools, with only 13 studies providing data on sensitivity and specificity.
For BDD, the BDDQ was validated in 2 studies with a sample size of 210 participants, showing a sensitivity of 0.97 [95% CI: 0.82-1.00] and specificity of 0.91 [95% CI: 0.86-0.95] using a cutoff score of ≥4. The BDDQ-aesthetic surgery version (BDDQ-AS) had a sensitivity of 0.90 [95% CI: 0.77-0.97] and specificity of 0.82 [95% CI: 0.71-0.91] in 1 study with 116 participants at a cutoff score of ≥16. In a smaller study with 48 participants, the BDDQ-dermatology version (BDDQ-DV) reached a sensitivity of 1.00 [95% CI: 0.59-1.00] and specificity of 0.95 [95% CI: 0.83-0.99]; however, no cutoff score was mentioned. The Cosmetic Procedure Screening Questionnaire demonstrated a sensitivity of 0.89 [95% CI: 0.81-0.94] and specificity of 0.81 [95% CI: 0.72-0.88] in a single study with 205 participants using a cutoff score of ≥40. The Dysmorphic Concern Questionnaire was used in 2 studies totalling 366 participants, yielding a sensitivity of 0.90 [95% CI: 0.62-0.98] and specificity of 0.91 [95% CI: 0.87-0.93] using a cutoff score of ≥9. Only 2 studies and 1 screening tool reported diagnostic test accuracy in trichotillomania, where the MGH-HPS was found to have a sensitivity of 0.90 [95% CI: 0.81-0.96] from 2 studies involving 192 participants, with a specificity of 0.72 [95% CI: 0.63-0.80] at a cutoff score of ≥9. The SPS-R demonstrated the highest diagnostic accuracy for identifying patients with SPD, with a sensitivity of 0.89 [95% CI: 0.84-0.94] and a specificity of 0.95 [95% CI: 0.93-0.96], across 2 studies involving 994 participants using a cutoff score of ≥9. In comparison, the SPIS, within a single study of 160 participants, yielded a sensitivity of 0.72 [95% CI: 0.61-0.82] and a specificity of 0.90 [95% CI: 0.81-0.96] using a cutoff score of ≥5. The SPS, from a study with 109 participants, showed a sensitivity of 0.84 [95% CI: 0.66-0.95] and a notably high specificity of 0.96 [95% CI: 0.89-0.99] at a cutoff score of ≥7 (Supplemental Table 7).
Systematic Analysis of Psychodermatology Tools
In evaluating the scales for different psychodermatologic conditions, 8 key dimensions were identified: duration spent on behaviour, control over behaviour, distress or emotional pain, life interference, social avoidance, shame/guilt, awareness, and preoccupation with appearance. These dimensions were chosen due to their critical importance in capturing the multifaceted nature of these conditions and their relevance in clinical practice. Among the 32 scales analyzed, 25 (78%) assessed duration spent on behaviour, 22 (69%) assessed control over behaviour, and 24 (75%) evaluated distress or emotional pain. Life interference was covered by 19 scales (59%), while social avoidance was considered by 17 scales (53%). Shame or guilt was addressed by 13 scales (41%), awareness by 10 scales (31%), and preoccupation with appearance by 17 scales (53%). For Trichotillomania, most scales included evaluations of duration (8/10, 80%), control (7/10, 70%), and distress (6/10, 60%). SPS primarily showed 82% of scales evaluating duration, 73% assessing control, 64% evaluating distress, and 64% considering life interference. In BDD assessment tools, scales consistently covered preoccupation with appearance (9/10, 90%) and emotional distress (9/10, 90%). Transdiagnostic scales typically demonstrated versatility by assessing most dimensions, excluding awareness (0/4, 0%). The summary of items used in the psychodermatologic questionnaires is shown in Supplemental Table 8.
Discussion
This systematic review represents a pioneering effort to address gaps in the current evidence base regarding the reliability and validity of primary psychodermatologic assessment and screening tools. Given the necessity for psychodermatologic-specific psychiatric assessment, this systematic review provides information on the selection of appropriate assessment tools for screening and monitoring PPDs such as BDD, trichotillomania, and excoriation disorder.
Our review identified 45 different psychodermatologic tools used to screen and assess PPDs in 81 studies, of which 13 provided empirical data on the diagnostic accuracy of the tools. The most frequently assessed tool for BDD among the included studies was the BDDQ, including its variants like the BDDQ-DV and BDDQ-AS. All versions demonstrated consistently high sensitivity, specificity, and reliability across various clinical settings, establishing them as efficient assessment tools for both patients with BDD and those seeking cosmetic procedures due to aesthetic concerns. However, there is no consensus on the most appropriate screening tools for BDD, and self-report instruments have several limitations. 27 These tools may not capture the full range of BDD symptoms that an individual might experience and often lack detailed information on social impairment, avoidance of specific activities due to BDD, the frequency of repeated behaviours, and the duration of these disturbances. In addition, the validity of a screening tool in one specific setting may not translate to other environments. Many tools have also not undergone psychiatric evaluation for authentication. Furthermore, several tools have not been updated to align with DSM-5 criteria, and comprehensive psychometric analyses of these instruments are often missing. With the increasing influence of social media on body image, future revisions of BDD scales have been suggested to incorporate questions that address patients’ behaviours related to social media. 28
For excoriation disorder, the SPS-R emerged as a prominently validated tool. The SPS-R, with 8 items assessing impairment and symptom severity, showed high diagnostic accuracy with a sensitivity of 0.89 and specificity of 0.95. Similarly, the MGH-HPS was the most frequently utilized tool for assessing trichotillomania, with numerous studies demonstrating its strong psychometric properties. The MGH-HPS, comprising 7 items, has validated 1- and 2-factor structures that effectively quantify the severity and impact of hair-pulling behaviours, making it a reliable tool for clinical use with a demonstrated sensitivity of 0.90 and a specificity of 0.72. Despite the frequent use of the MGH-HPS for trichotillomania, identifying the optimal assessment tool remains challenging. Furthermore, distinguishing trichotillomania from other psychological conditions with similar behavioural patterns, such as obsessive-compulsive disorder (OCD), BDD, or repetitive hair pulling in neurodevelopmental disorders can be difficult. 29 Several key differences exist, namely, individuals with trichotillomania often derive pleasure from hair pulling, whereas those with OCD do not typically find pleasure in their ritualistic behaviours. 30 Trichotillomania generally lacks the unwanted, intrusive thoughts characteristic of OCD and involves single repetitive behaviours rather than the multiple complex rituals seen in OCD. 31 In addition, OCD tends to respond much more positively to selective serotonin reuptake inhibitors as compared to patients with trichotillomania. 32 Neurodevelopmental disorders, such as autism spectrum disorder and stereotypic movement disorder, can involve repetitive hair pulling. However, in trichotillomania, hair pulling is driven and purposeful, unlike the often rhythmic and purposeless movements seen in stereotypies. In addition, neurodevelopmental disorders typically appear in early childhood, while trichotillomania usually develops later in life. 33 Individuals with BDD might pull hair to “fix” a perceived defect, focusing on cosmetic concerns, while those with trichotillomania usually do not have a cognitive fixation on hair-related issues, except in advanced cases of hair loss. 34 People with BDD often believe that pulling hair will enhance their appearance, whereas individuals with trichotillomania are frequently embarrassed or ashamed of the results of their hair pulling. This complexity is reflected in the assessment tools, as many of these complexities, such as feelings of shame and guilt, are not consistently evaluated. While shame and guilt are significant in both BDD and trichotillomania, they are just one example of some of the important dimensions that are often overlooked in these tools (Supplemental Table 8).
The variety of tools used in psychodermatologic assessments highlights both the importance and the ambiguity surrounding the most appropriate instruments for clinical practice. While many tools have demonstrated strong psychometric properties, their effectiveness in routine dermatological settings remains unclear. Practical barriers, such as time constraints, patient acceptability, and the complexity of integrating these tools into clinical workflows, limit their broader adoption.35,36 Furthermore, the lack of real-world validation and longitudinal studies impairs the understanding of their long-term applicability in fluctuating conditions like PPDs. 37 Future efforts should not only focus on refining existing tools to ensure they are both psychometrically sound and feasible for clinical use but also consider the development of a new psychodermatologic screening tool. Such a tool would address the current gaps in clinical practice by simplifying administration, enhancing accessibility, and improving integration into dermatology workflows. Developing a novel tool that is user-friendly and adaptable to various clinical settings could significantly improve the accuracy of PPD diagnosis. Additional research is needed to evaluate both existing and new tools in diverse settings, as well as to address the practical challenges dermatologists face when implementing these assessments. Incorporating digital platforms and enhancing clinician training will further support the routine adoption of these tools in dermatology practices.
Supplemental Material
sj-docx-1-cms-10.1177_12034754241311267 – Supplemental material for Systematic Review of Psychodermatologic Assessment Tools: Diagnostic Accuracy and Clinical Utility
Supplemental material, sj-docx-1-cms-10.1177_12034754241311267 for Systematic Review of Psychodermatologic Assessment Tools: Diagnostic Accuracy and Clinical Utility by Clayton Clark, Parsa Abdi, Kevin Li, Tarek Turk and Marlene Dytoc in Journal of Cutaneous Medicine and Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) received funding from Pfizer Canada for the research.
IRB Approval Status
Not applicable.
Patient Consent
Not applicable.
Reprint Requests
Dr. Marlene Dytoc, MD, PhD, FRCPC.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.