
Abstract
We aim to review modifiable risk factors and practices for surgical site infections (SSIs) reduction in cutaneous surgeries. The existing norms are assessed with the latest evidence, with the aim of enhancing and optimizing intra and postoperative strategies. This review seeks to offer an updated summary of the results of evidence for SSI reduction strategies tailored for practicing general dermatologists. Searches were conducted for “cutaneous surgery surgical site infection complications” using PubMed Central® and DynaMed®. Articles with pragmatic guideline recommendations were selected. We found evidence for intraoperative factors such as non-sterile gloves, brushless hand scrubbing/simple hand washing, sterile materials, and chlorhexidine gluconate as a skin antiseptic. For postoperative factors, there is a lack of evidence to support the use of topical antibiotic ointments, dressings, or waiting 48 hours before wetting to prevent SSI. Several intra/postoperative factors not specific to dermatologic procedures are briefly discussed for additional context. Several SSI risk factors are inherent to patients or necessary procedures; however, dermatologists have identified modifiable risk factors and developed protocols to mitigate SSI risks intraoperatively and postoperatively. By questioning established practices in cutaneous surgery aimed at preventing SSIs, we can work towards the optimal utilization of resources. This dual-focused approach not only enhances the efficiency of the healthcare system but also diminishes the risks associated with SSIs. It is important to acknowledge that this review does not encompass all factors essential for consideration in these recommendations. Nonetheless, it will approach these factors with an evidence-based lens, placing SSI prevention at the forefront.
Keywords
Introduction
Surgical site infections (SSIs) are the most common complication of dermatologic surgery (D-S). 1 SSIs are defined as infections occurring within 30 days after surgery, at or adjacent to the incision, and their rate ranges from 0.4% to 2.5%. 2 Surgical site infections (SSI) diagnosis is based on inflammatory features potentially accompanied by a positive culture. 2 The impact of SSIs includes increased mental and physical suffering, morbidity and mortality, increased healthcare costs, and poor cosmetic outcomes.3-5 There are patient, procedure, and post-procedure-related factors that increase SSIs. Dermatologic surgeons have put in place numerous intraoperative and postoperative procedures in attempts to reduce SSIs. There are recent comprehensive reviews on preoperative considerations for lowering SSI in D-S, including perioperative prophylactic antibiotics and decolonization protocols, which are beyond this article’s scope; readers are referred to recent articles.6-8 This review evaluates established intraoperative and postoperative procedures for SSI reduction. It reviews the relevant data to support or not support the protocols as they may relate to general dermatologists performing D-S.
Intraoperative Factors
This section discusses evidence for SSI reduction through various aspects of aseptic technique (hand hygiene, gloves, and surgical materials), hair removal, preoperative cleaning, suture material, ambient temperature, irrigation, adding antibiotics to local anesthesia, and intraoperative tight glycemic control (Table 1).
Summary of Recommendations for Intraoperative Interventions in Cutaneous Surgery to Reduce Surgical Site Infections.
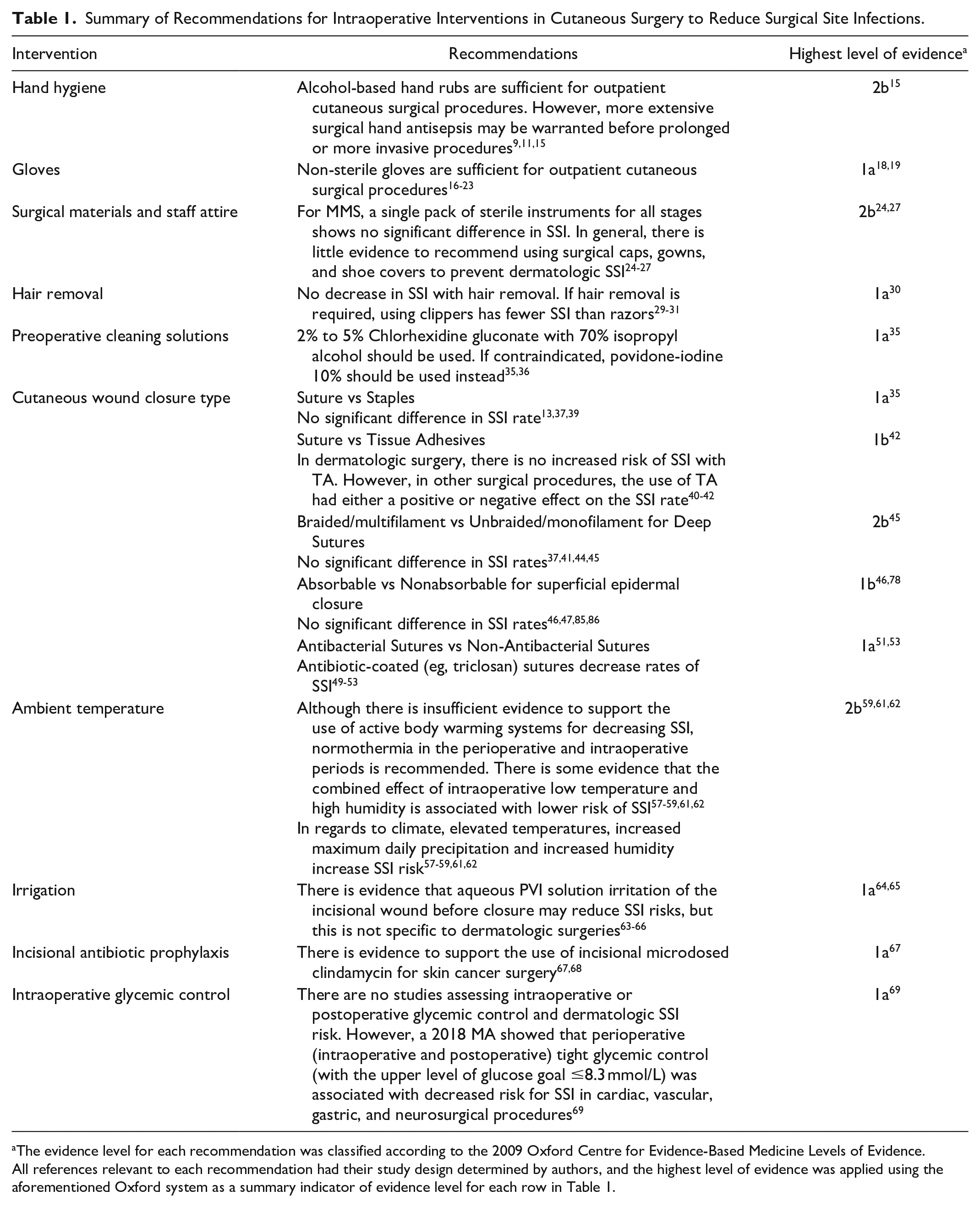
The evidence level for each recommendation was classified according to the 2009 Oxford Centre for Evidence-Based Medicine Levels of Evidence. All references relevant to each recommendation had their study design determined by authors, and the highest level of evidence was applied using the aforementioned Oxford system as a summary indicator of evidence level for each row in Table 1.
Definitions of Aseptic versus Clean
D-Ss are performed using both “aseptic” and “clean” techniques. Aseptic is “free from pathogenic organisms,” while “sterile” is “free from (all) microorganisms.” Clean is “free from visible marks and stains.” Although “aseptic” and “sterile” are often used interchangeably, the most achievable and appropriate term would be “aseptic.” 9 According to The Joint Commission, regarding the recommendation for the insertion of central venous catheters, the factors involved in determining whether the technique is “aseptic” (vs “clean”) is based on the utilization of barriers (eg, sterile gloves/gowns/drapes, with masks), patient and equipment preparation (eg, antiseptic skin preparation and sterile instruments), environmental controls (eg, keeping doors closed and minimizing traffic), and contact guidelines (eg, only sterile-to-sterile contact is allowed). 10 Based on this definition, most in-office D-Ss are performed using the “clean technique” with some aspects of the “aseptic technique.” Aseptic techniques are more frequently employed in more invasive dermatologic procedures such as excisional surgeries, flaps, grafts, and Mohs Micrographic Surgery (MMS). 9
Hand Hygiene
Hand hygiene refers to “any action of hand cleaning.” It includes using 70% to 90% alcohol-based hand rub (ABHR), hand washing, and surgical hand antisepsis in operative settings, which may use either an ABHR or antimicrobial soap. 11
In hand hygiene outside of the surgical setting, the Centers for Disease Control and Prevention recommends that ABHR be used for most instances except when hands are visibly soiled after using the restroom, when exposed to Clostridium difficile, and before eating. In those cases, hand washing with soap and water is preferred. 12 A randomized clinical trial (RCT) evaluating hand washing protocols concluded that ABHR protocols are as efficacious as chlorhexidine (CHH) handwashing and using ABHRs is the most time-efficient protocol for routine patient care activities. 13
In the general surgical settings, the recommendation is to perform “surgical hand antisepsis” before donning sterile gloves. This includes scrubbing the hands and forearms for the length of time recommended by the manufacturer (2-5 minutes). 11 Updated guidelines allow for the choice of scrubbing with antimicrobial soap and water or using a suitable ABHR prior to donning sterile gloves, which are supported by studies showing their equivalence. 11 A 2016 systematic review concluded that “hand-rubbing” techniques are as effective as traditional scrubbing for preventing SSIs whether the solution contained CHH or povidone-iodine (PVI). 14
Surgical hand antisepsis up the forearm is not routinely practiced in dermatology. 9 Considering low SSI rates in D-S, there is evidence that clean procedures and clean (non-sterile) gloves (NSG) do not increase the rates of SSI. The conclusion might be that current appropriate hand hygiene prior to cutaneous surgical procedures within dermatologic offices would suffice.9,15
Gloves
The World Health Organization (WHO) currently recommends using sterile gloves (SG) to prevent SSIs. 16 However, this guideline targets “surgical teams” in hospital settings and is not specific to D-S. Clear evidence-based guidelines are still needed in the field of D-S. NSG, if recommended, should not put the patient at greater risk compared to using SG. 17
A 2023 systematic review and meta-analysis (SR-MA) concluded that there was no difference between SG and NSG on SSI in minor surgical procedures. 18 This was supported by other studies, including a prospective randomized study of surgical excisions assessing SG and NSG.19-21 Furthermore, evidence demonstrates that NSG use in all stages of MMS does not result in higher SSI than SG. A 2006 review of the 1400 Mohs procedures by Rhinehart et al demonstrated no differences in SSI with the use of NSG versus SG during the tumour extirpation stage of MMS. 22 Then, in 2014, a study reviewing over 2000 MMS-treated tumours confirmed that the use of NSG for all steps of MMS did not result in increased SSI (SG SSI incidence = 0.50%, NSG SSI rate = 0.49%, P = .82) and resulted in significant cost savings. 23
As SG are more expensive and evidence shows there is no significant difference in SSI rate, this is one potential area where there are healthcare savings within D-S. 21 Opting for a less expensive but equally effective NSG is more cost-effective and environmentally friendly. 18 Evidence supports the safety of the use of NSG in all stages of MMS and other D-S.
Surgical Materials and Surgical Gowns/Caps/Shoe Covers
Instruments
A 2015 prospective study of 338 MMS patients using a single set of instruments revealed that the overall SSI rate was 2.1% (7/322) and concluded that using a single set of sterile instruments for all stages of MMS did not lead to patient harm and maintained the SSI rates within an acceptable range. 24 Enhanced surgical instrument sterilization protocols requiring that instruments be sterilized individually instead of “surgical instrument packs” did not seem to impact surgical infection rates. 25
Effect of Combination of Interventions
In general, evidence is lacking to recommend the use of surgical caps, gowns, and shoe covers in the prevention of dermatologic SSIs. 26
A 2010 prospective study of 1000 MMS patients using clean surgical technique (ie, NSG, towels, and a single pack of sterile instruments for all steps) did not demonstrate increased SSI. 15 However, a 2010 study of 950 tumours undergoing MMS revealed that heightened infection control measures reduced SSI (2.5% vs 0.9%). Both “intervention” and “control” groups had the following infection control practices: sterile trays and instruments, staff wearing scrubs, masks, and face shields, and using clean patient dressing post-surgery. The intervention included jewellery restriction, ABHR before stages and reconstruction, sterile gloves/gowns for staff, and sterile towels/dressings for the patient. 27 This was compared to the control group, which had no staff jewellery restriction, no surgical caps nor sterile gowns, and an aseptic technique only for the reconstruction.
A 2012 study compared SSI rates (670 tumours undergoing MMS) and costs to those of a 2010 retrospective study.27,28 An SSI rate of 0.7% (the previous study’s SSI rate was 0.9%) was achieved by adopting certain aspects of the aseptic technique described by the previous study. For example, they kept the jewellery restriction, surgical caps, staff hand washing with CHH/ethyl alcohol for all MMS stages, sterile paper drape during Mohs excision, and aseptic technique during the reconstruction. Still, they came up with cost savings by using NSG during the Mohs excision and using long-sleeved scrub tops (instead of sterile knee-length gowns). 28 How this may translate to non-MMS procedure is unclear since non-MMS surgical excisions usually involve excisions and repair within one procedure. These conflicting studies may demonstrate that certain aspects of the aseptic technique have different impacts on SSI and that each aspect cannot be considered in isolation regarding overall rates of SSI.
Hair Removal
D-S often involves hair-bearing areas, and hair removal may be a patient’s or surgeon’s preference. There is no advantage concerning SSI with hair removal. 29 The WHO guidelines in general surgery recommend avoiding cutting hair from the site of surgery unless it is necessary. 16 If unavoidable, clippers rather than a razor should be used.30,31 An SR-MA of RCTs indicated fewer SSIs with clipping, chemical depilation, or no depilation compared to razors.30,31 In a 1678-patient RCT, there was no difference in SSI between a group whose hair was clipped vs those who did not get hair removal in general elective surgery. 31
Cleaning Solutions
Immediate preoperative cleaning of the operative site is an essential step in all infection control protocols for D-S. 32 Antiseptic agents used include CHH, PVI, betadine, isopropyl alcohol, benzalkonium chloride. 33 The most common of these are CHH and PVI. 34 A 2022 SR-MA compared preoperative antiseptic agents in the prevention of SSI in patients undergoing surgery and concluded that 2% to 2.5% CHH in alcohol or 1.5% olanexidine is the most effective. 35 For clean surgery, there was no difference between concentrations of CHH. 35 In an SR-MA comparing alcoholic CHH 4% to 5% and aqueous and alcoholic PVI-based antiseptics, alcoholic CHH 4% to 5% was more effective than PVI in lowering SSI. 35
The WHO guidelines recommend the use of alcohol-based CHH solutions. 16 However, alcohol-based solutions should not be used on neonates or be in contact with mucosa or eyes. CHH should not come into contact with the eye or middle ear. For burned and denuded skin, 0.9% normal saline should be used. 36
Therefore, for in-hospital and outpatient procedures, it is recommended to prepare the skin using alcohol-based CHH solution unless it is contraindicated, in which case PVI 10% should be used. 35
Types of Cutaneous Wound Closure
D-S incisions can be closed using staples, sutures, or tissue adhesives (TA). 37 When discussing SSIs and cutaneous closures, variables include the material of the closure (suture vs staples or suture vs TA), location of the sutures (epidermal closure vs buried sutures), absorbable (AB-S) versus nonabsorbable (N-AB-S), braided multifilament (B-Mul) versus non-braided monofilament (N-B-Mon), and antibacterial properties of the suture.
Sutures versus Staples
While a 2021 review concluded that AB-S are preferable compared to staples and N-AB-S, with regards to cost, patient satisfaction, and pain, no conclusions can be made about SSIs. 37 A 2016 SR-MA looking at SSI after skin closure in orthopaedic surgery compared staples and sutures and showed no evidence favouring one method over the other. 38 This finding aligns with the 2020 study, which reported a lack of high-quality evidence comparing SSI rates between sutures and staples. 39 Based on these findings, we cannot conclude that either sutures or staples have an advantage in reducing SSI.
Sutures versus Tissue Adhesives
TAs have been used routinely in the emergency departments for skin lacerations and are gaining popularity in operating rooms and outpatient settings. 40 TAs include octyl cyanoacrylate (OCA) and N-butyl-2-cyanoacrylate (NBCA). 40
It was thought that TA may decrease SSI since it forms a barrier, protects the wound, and has possible antibacterial properties, but the studies are mixed. 41 Reports demonstrated equivalence of TA and sutures regarding SSIs. A 2014 Cochrane review evaluated TA in surgical incisions and concluded that sutures are significantly better than TA for minimizing dehiscence. Still, there was no evidence of TA advantage for all other outcomes, including infection. 41 Recently, an RCT involving 100 patients comparing TA and suture for closing carpal tunnel surgery found no differences in complications, including infection and allergic contact dermatitis (ACD) at 2 and 6 weeks post-closure. 42 A 2021 study examining the effects of TA on SSI following elective bariatric surgery revealed the use of TA was more common in patients with SSI compared with those without (54.3% vs 30.8%, P = .003), and on multivariate analysis, the use of TA was an independent predictor of SSI (OR, 2.77, P = .007). 43 This latter study shows that TA’s effect on SSI is likely specific to the type of procedure itself, and careful evaluation of study applicability to dermatology is required.
Cost and ACD risk should be considered in contemplating TA use. The rate of ACD to the TA is unknown, however, there was only one case of ACD to NBCA for surgical closure and more cases of ACD to OCA likely due to its increased use. 44 Overall, it appears that TAs are safe and cost-effective alternatives to sutures for superficial closure of low-tension wounds in D-S, but their effect on SSI in D-S is unclear.
Monofilament versus Multifilament Buried Sutures
Regarding buried sutures (B-S) and their rates of SSI, it has been thought that B-S carried a higher risk of infection when compared to N-B-Mon sutures despite the lack of evidence.37,41,44 For example, examining explanted AB-S and N-AB-S from infected and noninfected sites in 158 patients revealed no differences in microbial recovery between monofilament and multifilament sutures. The study suggested that all suture surfaces are hospitable environments for microbes. 45 Several articles that include SSI rates in their comparison of buried B-Mul sutures with buried N-B-Mon sutures failed to confirm any increased infection rates with the use of the former.
Absorbable versus Nonabsorbable Sutures for Epidermal Closure
Traditionally, N-AB-S for epidermal closures is advised since there is the dogma that the B-Mul configuration of AB-S can entrap more microorganisms, leading to infection. 46 A 2020 randomized, blinded split-scar trial of 105 patients with MMS facial excisions were epidermally closed with either rapidly absorbable polyglactin 910 (Vicryl RapideTM) on one-half of the repair and non-absorbable nylon (EthilonⓇ) on the other half. 46 The adverse events, including infection, did not differ between the groups. This is supported by other authors and by an international, prospective 3494-patient cohort study. 47
Antibiotic-Coated versus Non-Antibiotic-Coated Sutures
Antibiotic-coated sutures (ACSs), usually coated with triclosan (VicrylⓇ Plus, PDSⓇ Plus, MonocrylⓇ Plus), demonstrated their ability to prevent the colonization of Staphylococcus aureus and S. epidermidis in vitro and in vivo studies. 51 The balance of evidence seems to support the use of ACSs in reducing SSIs.48-53 A 2019 SR-MA involving 11,957 participants concluded that triclosan-coated sutures (TCSs) reduced risks of SSI at 30 days (relative risk 0.73, 95% CI 0.65-0.82) both in clean and contaminated surgery. 51 ACD to TCSs is reported, and it is not recommended in patients allergic to triclosan. 54 ACSs are more expensive than non-ACSs, however, the cost associated with reduced SSI rates may compensate for the price difference. 55 None of these studies were specific to D-S, so the benefits of their use on SSI in dermatology need further exploration.
In summary, with the currently available data, there does not seem to be any increased SSIs between sutures and staples, sutures and TA (and there may even be SSI risk reduction in the latter), AB-S and N-AB-S of epidermal closure, nor monofilament and multifilament sutures for buried sutures. There is evidence to support the use of antibacterial sutures for the prevention of SSIs. Since the choice of wound closure material depends on many factors, outside of the ACSs having an SSI advantage, these other factors will play a larger role in the ultimate choice of wound closure material.
Ambient Temperature
Perioperative or intraoperative hypothermia (approximately 2°C below the normal core temperature) is thought to increase the risk of SSI. 56 WHO recommends that warming devices be used during surgeries to keep the patient normothermic (35.5-36°C or higher) to reduce SSI. 16
However, the evidence supporting this recommendation must be clarified, especially with more up-to-date studies. A 2016 5438-participant Cochrane review concluded that active body warming systems showed a reduction in SSI in abdominal surgeries when compared with controls [4.7% vs 13%; RR, 0.36 (95% CI, 0.20-0.66); P = .008]. 57 Conversely, a 2020 SR-MA reviewing perioperative body temperature maintenance and SSI was less conclusive, indicating that the available evidence is insufficient to prove that warming methods prevent SSIs. Despite their conclusion, the authors recommend normothermia during the perioperative and intraoperative periods. 58 Finally, a 2023 retrospective review of 49,067 cases, including ambient temperature and relative humidity of operating rooms in 3 hospitals performing a variety of surgeries, revealed no relationships between intraoperative temperature and room humidity and increased risk of SSI when analyzed as independent variables. 59 Interestingly, the study results showed that when the low temperature was combined with high humidity, there was an associated lower risk of SSI. 59
Climate is another temperature-related factor that has been reviewed as a risk for increasing SSIs. Elevated temperatures may increase the risks of SSIs. 60 Furthermore, an increase in maximum daily precipitation and humidity also increased SSI risk. 61 The seasonal variation of SSI rates in the northern hemisphere, peaking during July and bottoming out in December, is consistent with prior studies. 62 With climate-related temperature and humidity changes, the estimate is that there would be a 3% increase in SSIs by 2060 in the Southeast region of the USA. 61
These studies are not specific to D-S, which, with inherent low risks of SSI, may not lend itself well to the same conclusions as applied to other surgical procedures. Not only are further studies specific to D-S in regard to ambient temperatures required, but the examination of extremes in weather that come with climate change, including freezing temperatures, especially in places such as Canada, and its effect on SSI from D-S is warranted.
Irrigation
The WHO suggests using an aqueous PVI solution for irrigation of the incisional wound before closure to reduce SSI in clean and clean-contaminated wounds but states that there is insufficient evidence to recommend for or against saline irrigation and does not recommend the use of antibiotic irrigation. 63 A 2017 SR-MA of RCT evaluating prophylactic intraoperative wound irrigation (WI) for the prevention of SSI supported this recommendation. 64 On the other hand, a 2022 meta-analysis (MA) of 24 studies evaluating the effects of WI on the prevention of SSIs found that both antibiotic irrigation (OR, 0.48; 95% CI, 0.36-0.62, P < .001) and aqueous PVI irrigation (OR, 0.40; 95% CI, 0.20-0.81, P = .01) had significantly lower SSIs in all surgical populations compared with saline irrigation or no irrigation. 64
A 2023 SR-MA concluded that there have been many studies showing that the inclusion of antibiotics in the irrigation solution significantly lowers SSIs. Still, these studies are heterogeneous and contain many biases. 65 Potential harms of intraoperative WI may include anaphylaxis, nephrotoxic effects, and systemic contact dermatitis. 66
In summary, there is at most low-level evidence that antibacterial solutions (eg, antibiotic solutions or antiseptic solutions) may lower SSI when used as prophylactic incisional WI, but none of the studies reviewed were specific to D-S. Dermatologic surgeons will need to weigh the risks and additional costs of irrigation against the potential benefits, perhaps in certain procedures with higher risks of SSI due to other factors.
Intra-Incisional Antibiotic Prophylaxis
In dermatologic surgery, one method of SSI reduction is intra-incisional antibiotic prophylaxis. It is currently a less commonly used method of local antibiotic prophylaxis through incisional antibiotics delivered along with local anesthetic right at the incision site. 67
A 2023 RCT with 681 patients (1133 lesions) was treated with buffered local anesthetic (LA) alone (control group), buffered LA with microdosed flucloxacillin, or buffered LA with microdosed clindamycin. The proportion of lesions with clinical SSI was 5.7% in the control group, 5.3% in the flucloxacillin group, and 2.1% in the clindamycin group. 68 Regarding the prescription of postoperative antibiotics during follow-up, there was a significant reduction in the intra-incisional antibiotic groups (clindamycin, 2.1%; flucloxacillin, 4%) compared to the control group (8%). The conclusion was that intra-incisional antibiotics are effective, safe, and cost-effective as an SSI reduction measure in dermatologic surgery. 68 This study’s conclusions are supported by a 2020 review that evaluated 2080 MMS patients from 2 studies published in 1998 (evaluating nafcillin) and 2002 (evaluating clindamycin) who received intra-incisional antibiotic prophylaxis through their LA solution versus placebo. 67 It was shown that there was a significant reduction in SSIs in the treatment groups. While the 2023 RCT recommended routine adoption of incisional microdosed clindamycin for patients undergoing skin cancer surgery due to the magnitude of effect and the absence of adverse effects, since SSI rates are low in routine dermatologic surgery, the clinician’s judgment should be used to balance the benefits or intra-incisional antibiotics with potential risks of bacterial resistance and systemic effects.
Glycemic Control
There are no studies assessing intraoperative or postoperative glycemic control and dermatologic SSI risk. However, a 2018 MA showed that perioperative (intraoperative and postoperative) tight glycemic control (with the upper level of glucose goal ≤8.3 mmol/L) was associated with decreased risk for SSI in cardiac, vascular, gastric, and neurosurgical procedures. 69
Postoperative Factors
Postoperative wound care involves cleaning and dressing the wound, including specific patient instructions (Table 2). These protocols seek to reduce SSIs, comfort, hemostasis, scar reduction, protection from mechanical trauma, and wicking away blood/exudate. 70 Aspects of wound care are reviewed concerning SSI reduction.
Summary of Recommendations for Postoperative Wound Care Factors in Cutaneous Surgery.
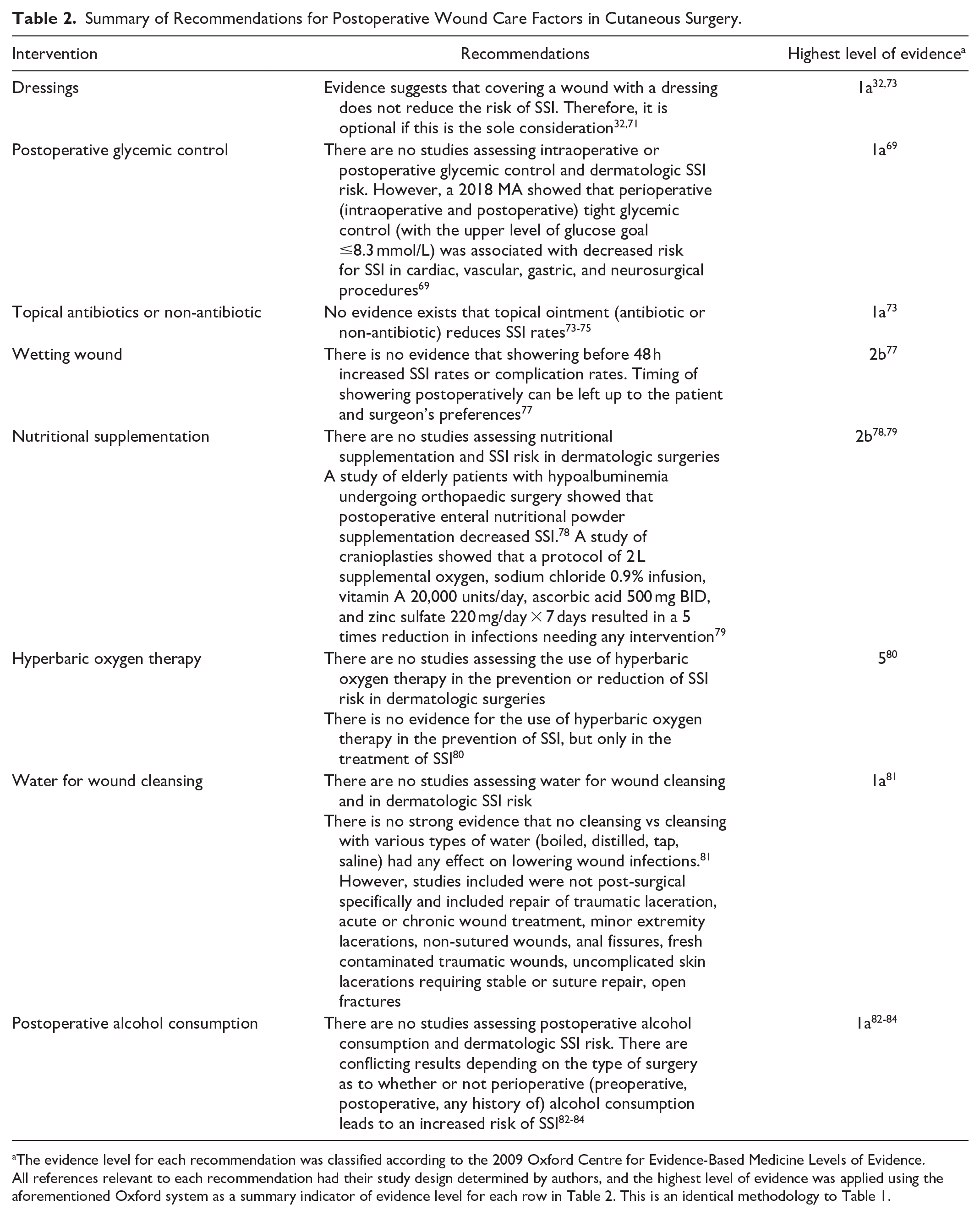
The evidence level for each recommendation was classified according to the 2009 Oxford Centre for Evidence-Based Medicine Levels of Evidence. All references relevant to each recommendation had their study design determined by authors, and the highest level of evidence was applied using the aforementioned Oxford system as a summary indicator of evidence level for each row in Table 2. This is an identical methodology to Table 1.
Dressings
Conventional post-surgical dressing involves an ointment layer, a contact layer, an absorbent layer, a contouring layer, and a securing layer. It is part of the routine postoperative care for reducing SSIs and symptom management. 32 However, a 2016 Cochrane review of 20 RCT concluded that there was no evidence to suggest that covering a wound with a dressing reduced the SSI compared to leaving a wound exposed. 32 Furthermore, there was no evidence that any particular wound dressing is more effective than others in decreasing SSI, improving cosmesis, or reducing pain. A 2022 SR-MA of RCT evaluating immediate air exposure versus dressings following primary closure of 1243 clean and clean-contaminated surgical wounds showed that dressing (gauze dressings, film dressings, and tissue glue as dressings) do not outperform immediate air exposure in terms of SSI risk. The SSI incidence was 11% for the immediate air exposure group and 11.1% for the dressings group when pooled, irrespective of surgery type. 71 These SSI rates are excessive compared to the established D-S risks, likely due to the nature of the surgical procedures studied and the fact that “clean-contaminated” wounds were included. Wound dressing decisions should be made based on other factors such as dressing costs, patient preference, and symptom management of each dressing type. 32
Dressings with Topical Antibiotics or Non-Antibiotics
Ointments are frequently applied after D-S as a first layer in multi-layer dressings. The rationale for ointments may be for a moist wound healing environment, for comfort, or for antibacterial purposes. 72 There are several options, including topical antibiotics and non-antibiotics.
A 2015 SR-MA reviewing topical antibiotic prophylaxis (T-AB-P) for preventing SSIs in D-S did not show a difference between topical antibiotics (T-ABs) and petrolatum/paraffin. 72 A 2021 SR-MA evaluating T-AB-P for SSIs in clean and clean-contaminated surgery (dermatological, ocular, spinal, orthopaedic, and cardiothoracic) did not reveal any differences between T-ABs and non-antibiotic agents. 73 A more recent 2023 MA reviewing T-ABs’ effects on the prevention and management of SSIs had a different conclusion. Their analysis concluded that T-ABs had significantly lower SSIs compared with placebo and antiseptics in persons with uncomplicated wounds. However, the authors recommended that these results be interpreted with caution since the studies they evaluated were of low sample sizes. 73
Of particular concern is the evidence that there is an increased risk of potential harm with the use of certain T-AB ointments. For example, topical gentamicin, as compared to petrolatum for managing auricular wounds, demonstrated a disproportionate number of cases of inflammatory chondritis. 74 In a study evaluating topical mupirocin ointment to surgical wounds before occlusive dressings, there were more scar complications in the mupirocin group due to an increased risk of skin necrosis. 75 In addition to certain increased surgical complications, topical antibiotics can cause ACD and contribute to antibiotic resistance. 34
As for the evidence for T-ABs or topical antiseptics for the treatment of surgical wounds healing by second intention, a 2016 Cochrane review concluded that there is no evidence of the effectiveness of any antiseptic/antibiotic/antibacterial preparation. 76
Based on these studies, there were no advantages to using T-ABs on clean, primarily closed wounds to prevent SSIs, and further studies are required for its use on surgical wound healing by second intention. From an antibiotic stewardship and healthcare savings standpoint, this will have positive benefits while not causing increased infection in patients.
Wound Wetting
Within routine postoperative care, patients are often recommended to avoid wetting the wound for 48 hours. 77 A 2020 systematic review evaluating infections between patients who were allowed to shower on or before postoperative day 2 and those who were prohibited from showering until postoperative day 3 and after revealed no difference in infection rates [P = .45, (−0.0052, 2 × 0.007 95% CI)]. 77 Showering may reduce infection by removing dirt and bacteria but may lead to contamination and wound maceration that may increase infection. 77 The review included only showering in its analysis and did not include water submersion (eg, swimming or bathing), which clinicians often do not advise until 10 to 14 days postoperatively. 77 Based on this evidence, the timing of showering can be left up to the patient’s preference and may lead to better patient satisfaction and earlier socialization post-surgery.
Nutritional Supplementation
There are no studies assessing nutritional supplementation and dermatologic SSI risks. However, a 2019 study of hypoalbuminemic seniors undergoing orthopaedic surgery indicated postoperative enteral nutritional powder supplementation decreased SSIs. 78 A 2023 study of cranioplasties showed that a protocol of supplemental oxygen, saline infusion, vitamin A, ascorbic acid, and zinc resulted in a 5 times reduction in infections needing any intervention. 79
Hyperbaric Oxygen Therapy
There are no studies assessing the use of hyperbaric oxygen in reducing SSI risk in D-S or in any surgeries. 80
Water for Wound Cleansing
There are no studies assessing water for wound cleansing and dermatologic SSI risk. Based on a 2022 Cochrane Review, no evidence exists that no cleansing vs cleansing with various types of water (boiled, distilled, tap, saline) had any effect on lowering wound infections. 81
Postoperative Alcohol Consumption
There are no studies assessing postoperative alcohol consumption and dermatologic SSI risk. A 2014 SR-MA of alcohol consumption and gastrointestinal SSI, and a 2024 SR-MA of alcohol consumption and shoulder arthroscopy SSIs showed no increased risk.82,83 However, another 2024 SR-MA focusing on ankle fracture fixation SSI demonstrated that perioperative alcohol consumption increased the risk for SSIs. 84 All of these studies looked at “perioperative” alcohol consumption which included preoperative, postoperative, and history of alcohol consumption. These conflicting results show that the effect of alcohol on SSI risk may be related to the specific surgical intervention.
Conclusions
D-Ss constitute a routine aspect of clinical practice, constantly emphasizing mitigating potential complications. Among these, SSIs are of critical concern. This review aims to examine the evidence for established cutaneous procedural and wound care practices and to provide an update on their impact on the incidence of SSIs. Certain factors, including cosmesis, healing time, scar strength, patient satisfaction, pain, and exudate, lie outside the scope of this discussion. Adopting these recommendations will be up to the clinician after carefully considering all relevant procedural and individual patient risk factors. This review revealed the necessity for additional research on risk factors specific to D-Ss. We also advocate for further studies into the influence of climate on SSI, with a particular emphasis on the distinctive Canadian weather conditions. By challenging established norms and presenting the latest evidence on SSI risks, we aim to facilitate a more informed decision-making process among dermatologists.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Informed Consent Statement
There are no human participants in this article, and informed consent is not required.