
Abstract
In Canada, there is a maldistribution of dermatologists, with as many as 5.6 dermatologists per 100,000 population in urban areas and as low as 0.6 per 100,000 in rural areas. Considering trends of dermatologists to work in group practices in urban areas, and the low number of rural dermatologists, one solution may be to incentivize dermatologists to practice rurally. Several solutions using the following themes are discussed: dermatology program-specific incentives, dermatology practice-specific incentives, and other indirect incentives. The low number of dermatologists in rural areas in Canada is concerning and has negative consequences for access to care for patients in rural areas, ultimately resulting in worse patient outcomes. Future research is needed to evaluate the impact of these initiatives and assess future access to dermatological care.
Introduction
Access to dermatology is a barrier to care in rural communities. In Canada, there is a maldistribution of dermatologists, with as high as 5.6 dermatologists per 100,000 in urban areas, and only 0.6 per 100,000 in rural/remote areas. 1 Definitions of rurality vary greatly within the literature, but are consistently distinguished by a lower population size, degree of urbanization, and proximity to metropolitan areas. Existing literature on the number of dermatologists needed to service the needs of Canadians estimates an ideal 4 per 100,000. 2 However, previous to this, the Royal College’s 1998 National Specialty Physician Review reported that the catchment area of each dermatologist in Canada was expected to be a population of at least 62,650. 3
For those living in rural and remote communities, the nearest dermatologist may be hours to days away. Diagnoses such as melanoma may be delayed which can have devastating consequences on mortality and quality of life. 4 A study in Ireland found that patients living greater than 90 km away from the nearest dermatologist had median Breslow thicknesses 127% greater than those living less than 3 km away (2.5 mm vs 1.1 mm of median Breslow thickness, respectively). 5 Demographic data indicate that 17.8% of Canadians live in rural areas, with over half identifying as Indigenous. 6 Given the disparities in healthcare resource allocation within rural and Indigenous communities, health outcomes of individuals in rural areas often fall short of those in urban environments. This inequity can be seen in Canadian literature, where the 1 year prevalence of atopic dermatitis in children living on mostly rural First Nations reserves reached as high as 16.5%, with most cases being deemed “moderate to severe.” 7 The present need for rural and remote dermatology should not be understated.
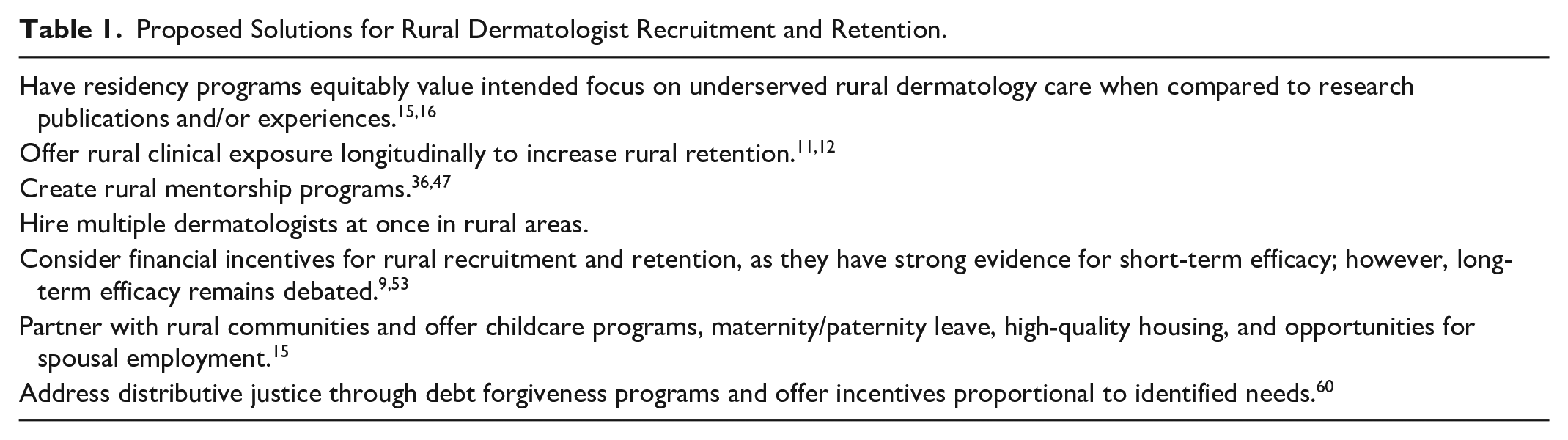
Considering the increased burden of care placed on an already low number of rural dermatologists, alongside an ever-increasing distribution favouring urban and suburban communities, solutions are needed. 8 Table 1 summarizes some of the proposed solutions within the literature for increasing the number of rural dermatologists. Existing reviews have discussed rural incentives in medicine broadly9,10; this review will focus on incentives for rural dermatologists.
Proposed Solutions for Rural Dermatologist Recruitment and Retention.
Dermatology Program-Specific Proposed Solutions
Targeted admission policies
There is strong evidence to support targeted admission policies for those with rural backgrounds, as these students are more inclined to return to their own communities to practice.11,12 An example of this is the Northern Ontario School of Medicine, whereby graduates from their undergraduate medicine program, the majority of which grew up in northern Ontario and/or rural areas were 2.57 times more likely [95% confidence interval (CI) 1.21, 5.44; P = .014] to have practices in rural Ontario. 13 A cross-sectional study of graduates from the Queen’s University family medicine residency program found that physicians raised in rural communities were 2.3 times more likely (95% CI 1.43, 3.69; P = .001) to practice in a rural community, and also 2.5 times more likely (95% CI 1.53, 4.01; P = .001) to be continuing to practice in a rural community at the end of the 4 year study. 14 During dermatology admissions, having programs equitably value intended focus on underserved rural care when compared to research publications may be a solution.15,16
Rural dermatology clinical exposure
Educating and training medical students and residents in rural areas has routinely been a suggested method for rural physician recruitment.17-20 A compelling body of literature supports rural clinical exposure in increasing the likelihood of rural retention.21-30 A survey of 89 primarily family physicians practicing in northern Ontario found that while length of stay and intent to stay were correlated with strong family ties to a rural area, 65.3% of respondents did not have strong family ties and 57.3% did not grow up in a rural setting. 31 While family ties and growing up in a rural area are often important and predictive for future rural practice, other intrinsic motivations to practice rurally can be fostered through rural training track initiatives. 31 Studies have shown that the resultant benefit of establishing rural track training programs can be an immediate and direct positive impact on the health of rural communities.32-34 In the United States, those from medical schools with rural tracks were 1.57 times more likely (95% CI 1.07, 2.26; P = .01) to pursue rural dermatology practice. 35 In a 2023 survey of 11 Canadian dermatology residency programs, 2 had mandatory rural rotations, 2 offered rural electives, and 5 offered both; leaving 2 programs which did not offer any direct opportunities for rural experience. However, in Canadian residency programs, rural electives remain limited, have unknown retention efficacy, and added financial, personal, and educational challenges for dermatology residents. 36
Rural mentorship programs
Mentoring relationships in dermatology play an important role in stimulating interest among residents in a variety of career tracks and leadership pursuits. 37 Mentoring is frequently discussed as having the potential to guide the career direction of a resident. 38 In a survey of 53 dermatology program directors of American residency programs, 81% of respondents deemed mentorship to play a “somewhat” or “very important” role in their own career development. 37 In the same 2009 study, 50% of program directors identified a need for a more structured mentorship program in their residency program. 37 Overall, 85% of program directors noted that a mentorship program had the potential to increase the number of residents pursuing more leadership roles, 37 which are undoubtedly important in rural dermatology.
Rural mentorship has shown promising results in enabling more individuals to consider practicing in a rural area.38-46 As mentorship in dermatology is an important part of becoming a physician, mentorship may be warranted, and virtual rural mentorship considered.36,47 Compared with older dermatologists favouring solo practice, younger dermatologists are more likely to practice in group practices. 48 This may be due to the added level of reassurance of being able to discuss cases with colleagues and establishing mentorship in early practice. An example of existing programs in ancillary specialties to dermatology includes the British Columbia program, Sustaining Pediatrics in Rural and Underserved Communities, a pediatrician-led clinician network offering a network of mentorship opportunities, and rural education to pediatricians. 52
Dermatology Practice Specific Incentives
Group practice hiring
There is a trend toward solo practice dermatologists in rural areas, 48 and group practice dermatologists in urban areas,2,48 and so, hiring more than 1 dermatologist at a time could be a solution to increasing the number of rural dermatologists, particularly in areas with a catchment area large enough for multiple dermatologists. Encouraging retired dermatologists to practice even part-time in rural communities may be a solution, as encouraged in rheumatology. 49 Some dermatologists travel to rural and remote areas for short stays and provide care. A rural locum program to provide care to rural areas of Canada may be warranted, and has shown positive results in pediatrics and otolaryngology.50,51 Dermatologist practice models generally consist of either primarily operating out of an academic centre, solo practice, small group practice (with 1 to 2 other dermatologists), or interprofessional group practice. 2 Each practice type has unique advantages, with solo and small group practices offering increased autonomy, allowing quick decision-making and the ability to modify practice, but with the added burdens of time commitment in running and operating a small business often with high overhead costs. 2 Encouraging various levels of the government to set up a program whose aim was to guide dermatologists toward essential business resources and services (eg, financing, grants, venders, realtors, contractors, etc) could lessen the burden of working in solo or small group practice in rural areas and could be an important step in incentivizing dermatologists to practice rurally.
Financial incentives
Financial incentives may also play a role in increasing the number of rural dermatologists, and as previously discussed, financial incentives to lower overhead costs for dermatologists in rural areas could be a solution. While blanket financial retention incentives have shown to be ineffective for rural family physicians, 52 short-term financial incentives have proven successful in short-term rural physician recruitment. 9 Literature from Québec has found some positive effects from financial incentives in family physicians 53 ; however, Québec’s Plan Régional d’Effectifs Médicaux (PEM) program aimed at increasing staffing in medical specialties based on expressed need, has poor uptake in dermatology, especially in rural areas. 54 Public outpatient dermatology practice in Québec does not only require PEM but also excludes many dermatologists from obtaining hospital privileges, however limited. 55
Other Indirect Incentives
Supporting families of dermatologists
Factors in a dermatologist’s decision to practically rurally may include spouses with independent careers, which constrain their ability to locate in rural areas. 56 A cross-sectional study of American physicians found that compared with other married physicians, physicians with a highly educated spouse were significantly less likely to work in a rural area (4.2% vs 7.2% respectively; 95% CI 2.4, 3.4; P < .001). 56 However, given this small absolute difference, opportunities for spouses of dermatologists may help, but will likely not increase the number of rural dermatologists as much as other solutions. 56
Other ways which could incentivize the families of dermatologists reported in the literature include offering housing, access to education, implementation of childcare programs, and maternity/paternity leave. 15
This review does not discuss teledermatology, which while effective and necessary in providing care to patients in rural areas, 57 contains several clinical, economic, technological, legal, and ethical limitations, which can make it less ideal than an in-person visit.58,59
Upstream solutions
The most upstream solution to this maldistributive inequity is to address the underlying causes of so few rural dermatologists, through a combination of both financial and grassroots efforts aimed at empowering and supporting dermatologists to practice rurally. 60 At a policy level, this may look like debt forgiveness programs, increased investment in allied healthcare professionals in rural areas, and providing incentives which are proportional to the unique needs of each community. 60 Addressing Canada’s rural dermatological care issue is not solely the responsibility of dermatologists, and will require a multidisciplinary approach.
Conclusion
The shortage of dermatologists in rural areas of Canada is a pressing issue that requires urgent attention. Limited access to care in rural areas is associated with increased morbidity, 61 and when applied to dermatology, emphasizes the need for more dermatologists practicing in rural areas. There are a number of ways to address the rural dermatologist shortage. At a residency program level, these changes may include targeted solutions such as equitably valuing intended focus on underserved rural care in residency program admissions, and offering rural-focused electives and rural mentorship programs. Other indirect incentives such as loan forgiveness programs, increased funding for allied healthcare professionals, and the creation of multidisciplinary teams help bridge the gap in access to care, and improve health equity among Canadians. Future studies are needed to evaluate the impact of these initiatives and assess future access to dermatological care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.