
Abstract
Topical photodynamic therapy is a widely approved therapy for actinic keratoses and low-risk nonmelanoma skin cancers with a rapidly growing range of emerging indications for other cutaneous diseases. This review summarizes the best-available evidence to provide a clinical update for dermatologists on the approved and emerging indications of photodynamic therapy. The body of evidence suggests that photodynamic therapy is superior or noninferior to other available treatment modalities for actinic keratoses, low-risk basal cell carcinomas, Bowen’s disease, skin field cancerization, chemoprevention of keratinocyte carcinomas in organ transplant recipients, photoaging, acne vulgaris, and cutaneous infections including verrucae, onychomycosis, and cutaneous leishmaniasis. There is emerging evidence that photodynamic therapy plays a role in the management of actinic cheilitis, early-stage mycosis fungoides, extramammary Paget disease, lichen sclerosis, and folliculitis decalvans but there are no comparative studies with other active treatment modalities. Common barriers to topical photodynamic therapy include procedural pain, costs, and the time required for treatment delivery. There is significant heterogeneity in the photodynamic therapy protocols reported in the literature, including different photosensitizers, light sources, number of treatments, time between treatments, and use of procedural analgesia. Topical photodynamic therapy should be considered in the management of a spectrum of inflammatory, neoplastic, and infectious dermatoses. However, more comparative research is required to determine its role in the treatment algorithm for these dermatologic conditions and more methodological research is required to optimize photodynamic therapy protocols to improve the tolerability of the procedure for patients.
Introduction
Topical photodynamic therapy (PDT) is centred on the interaction between a photosensitizer, the appropriate activating wavelength of light, and oxygen. The resulting photochemical reaction generates singlet oxygen, a highly-reactive chemical species that initiates a series of cellular reactions that culminate in necrosis, apoptosis, and a host immunologic response. 1 The main topical photosensitizers used for PDT are 5-aminolevulinic acid or its ester, methyl aminolevulinate (MAL). These photosensitizers preferentially bind with low density lipoproteins (LDLs), and the resulting complexes are subsequently internalized by LDL receptor-mediated endocytosis and are metabolized into the photoactive protoporphyrin IX (PpIX) within the mitochondria. 2 Premalignant and malignant cells accumulate PpIX due to higher rates of LDL uptake from increased LDL receptor expression to supply these rapidly dividing cells with cholesterol to create membranes for cell division, and increased mitochondrial PpIX synthesis.3,4 Numerous clinical guidelines have approved topical PDT for the treatment of actinic keratoses (AKs) and low-risk nonmelanoma skin cancers (NMSCs).5,6 There is a rapidly expanding number of studies exploring the utility of topical PDT for a spectrum of dermatological conditions. However, topical PDT continues to be underutilized in Canada. Therefore, a review is necessary to update dermatologists on the latest evidence about the clinical applications of topical PDT, with a focus on high-quality comparative studies with other first-line treatment modalities.
This review explores the approved and emerging clinical applications of topical PDT in dermatology to evaluate its role in the treatment algorithm of cutaneous diseases and the barriers to its use. The literature comparing topical PDT and other accepted treatment modalities for the established and emerging dermatological clinical indications for topical PDT are summarized in Table 1. This review preferentially included randomized-controlled trials (RCTs) and meta-analyses of RCTs with quantitative primary outcomes. In the absence of published RCTs and meta-analyses in the context of emerging clinical applications of topical PDT, prospective and retrospective cohort studies as well as case studies and series with quantitative primary outcomes were included. All descriptive studies were excluded.
Efficacy Comparisons Between PDT and Other Accepted Treatment Modalities for the Established and Emerging Clinical Indications for Topical PDT.
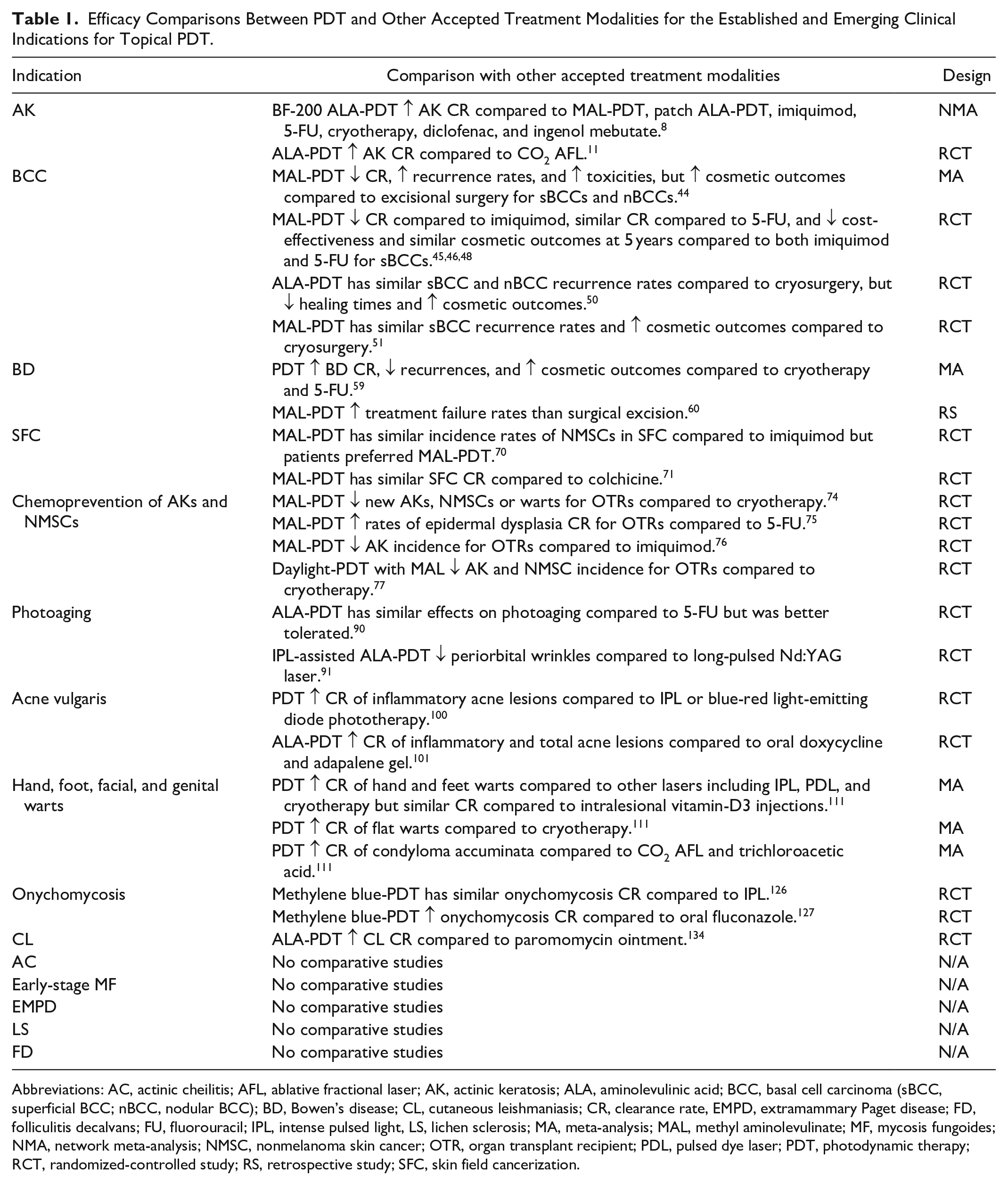
Abbreviations: AC, actinic cheilitis; AFL, ablative fractional laser; AK, actinic keratosis; ALA, aminolevulinic acid; BCC, basal cell carcinoma (sBCC, superficial BCC; nBCC, nodular BCC); BD, Bowen’s disease; CL, cutaneous leishmaniasis; CR, clearance rate, EMPD, extramammary Paget disease; FD, folliculitis decalvans; FU, fluorouracil; IPL, intense pulsed light, LS, lichen sclerosis; MA, meta-analysis; MAL, methyl aminolevulinate; MF, mycosis fungoides; NMA, network meta-analysis; NMSC, nonmelanoma skin cancer; OTR, organ transplant recipient; PDL, pulsed dye laser; PDT, photodynamic therapy; RCT, randomized-controlled study; RS, retrospective study; SFC, skin field cancerization.
Currently Approved Indications
Actinic Keratoses
Topical PDT has been established as an effective approach to treat AKs, common precancerous skin lesions that develop from cumulative sun exposure and may progress to squamous cell carcinomas (SCCs). There are numerous treatment modalities for AKs. Lesion-directed therapies include cryotherapy, lasers, and curettage. Field-directed therapies include topical 5-fluorouracil (FU), imiquimod, and diclofenac. 7 In a network meta-analysis of 25 RCTs of 5562 participants, topical PDT with a nanoscale-lipid vesicle formulation of aminolevulinic acid (ALA; BF-200 ALA-PDT), showed the highest AK clearance rates (75.8%) compared to topical PDT with MAL (MAL-PDT), patch ALA-PDT, cryotherapy, diclofenac, 5-FU, ingenol mebutate, and various imiquimod treatment protocols. 8 Another network meta-analysis of 15 RCTs of 4252 patients with at least 12 months of follow-up found that ALA-PDT had the highest AK clearance rates compared to placebo (Risk Ratio (RR): 8.05; 95% CI: 2.07-31.37), followed by imiquimod 5%, MAL-PDT, and cryotherapy. 9 In a meta-analysis of 4 RCTs with a total of 641 participants, PDT with either ALA or MAL increased AK clearance rates at 3 months compared to cryotherapy (RR: 1.14; 95% CI: 1.11-1.18). 10 ALA-PDT reduced AK quantity at 3 months compared to CO2 ablative fractional laser (AFL) (80% vs 66.7%; P = .0155) in a RCT of 20 patients. 11 MAL-PDT has higher AK clearance rates at 3 months (85.9% vs 51.8%; P < .0001) compared to 3% diclofenac and hyaluronic acid gel in a RCT of 200 patients. 12 In a survey of patient perceptions of PDT, more patients reported a recovery time of 1 week or less after PDT than after cryotherapy (61.5% vs 36.1%; P = .02) and surgical excision (61.6% vs 27.3%; P = .02), and patients preferred PDT over 5-FU (64.9% vs 12.5%; P < .001) and imiquimod (64.9% vs 12.5%; P = .03). 13 However, it is important to note that due to the higher mean costs of PDT, 5-FU was found to be the most cost-effective AK treatment modality in a RCT of 624 participants in the Netherlands comparing 5-FU, imiquimod, ingenol mebutate, and MAL-PDT. 14 Patient tolerability to PDT as an AK treatment modality is limited by procedural pain. Numerous approaches have been shown to reduce PDT-related procedural pain, which include PDT procedural modifications and adjuncts. PDT procedural modifications that improve tolerability without reducing treatment efficacy include non-occlusive photosensitizer application, 15 reduced photosensitizer incubation time,16,17 simultaneous illumination with photosensitizer application, 18 variable pulsed light illumination with short pulse durations, 19 fractional illumination in 2 parts separated by a dark interval in which no light is delivered, 20 and reduced illumination fluency rates (mW/cm2). 21 Cold air analgesia, 22 scalp nerve blocks,23,24 and topical analgesia with a 7% lidocaine and 7% tetracaine self-occlusive cream, 25 are PDT procedural adjuncts with demonstrated efficacy in pain reduction. In a split-face RCT of 22 patients with multiple AKs, applications of a topical ultrapotent steroid (clobetasol propionate 0.05%) before and just after MAL-PDT reduced post-PDT erythema (16% vs 7.6% increased erythema at 24 hours; P = .012) with no significant difference in AK clearance rates compared to MAL-PDT alone. 26
Daylight-PDT, where natural daylight exposure is used instead of an artificial light source, addresses many of the limitations of conventional PDT by reducing clinic visit times associated with the illumination procedure and minimizing procedural pain. Of course, the effectiveness of daylight-PDT is dependent on weather conditions, as limited sunlight could be insufficient to activate the photosensitizer, and cold ambient temperatures may preclude patients from tolerating the necessary time outdoors to receive the optimal dose of daylight exposure. It was found that there was generally sufficient natural sunlight (>8 J/cm2 for at least 2 hours) and a comfortable temperature (minimum temperature of at least 10°C) for outdoor sunlight exposure to treat patients with AKs effectively with daylight-PDT until the middle of September, even in countries in Northern latitudes. 27 This threshold of 8 J/cm2 for at least 2 hours was based on a study that found similar AK clearance rates after daylight-PDT with MAL at light doses of 8 to 70 J/cm2 and that 1.5 and 2.5 hours of daylight exposure resulted in similar AK clearance rates.28,29 From our experience in an Eastern Canadian climate, daylight-PDT remained effective well into the month of October with temperatures remaining above 10°C. Daylight-PDT was noninferior to conventional PDT for grade I to II AKs (RR: 0.97; 95% CI: 0.91-1.04) but was less effective for thick and hyperkeratotic grade III AK lesions (RR: 0.87; 95% CI: 0.81-0.94) in a meta-analysis of 6 RCTs with a total of 369 patients. 30 This meta-analysis also showed that daylight-PDT reduced maximal pain scores (mean difference: 4.51; 95% CI: 3.89-5.12) and lowered the risk of adverse events (RR: 0.7; 95% CI: 0.58-0.85) compared to conventional PDT. More patients were satisfied with daylight-PDT compared to conventional PDT (RR: 4.001; 95% CI: 2.017-7.938) in a meta-analysis of 5 RCTs with a total of 318 patients. 31 These findings align with our experience treating a 72-year-old male with chronic facial actinic damage and AKs with 4 repeated sessions of daylight-PDT with MAL (Figure 1). There have been some methodological studies to guide the selection of a daylight-PDT AK treatment protocol. Patients undergoing pre-treatment curettage, which is thought to enhance photosensitizer penetration, had similar AK clearance rates at 3 months compared to the non-curettage group. 32 Comparisons between the ALA and MAL photosensitizers found that daylight-PDT with BF-200 ALA improved AK clearance rates at 3 months and at 12 months.33-35 No difference in AK clearance rates were found in a study comparing a single treatment and 2 treatments of daylight-PDT with MAL; however, the second treatment increased pain (P = .04) and the severity of local skin reactions (P < .01). 36 Pre-treatment with super-potent corticosteroids and the use of brimonidine tartrate, a highly selective α2-adrenergic receptor agonist with potent vasoconstrictive activity, 24 hours after daylight-PDT significantly reduced post-treatment erythema with similar AK clearance rates compared to the untreated group. 37
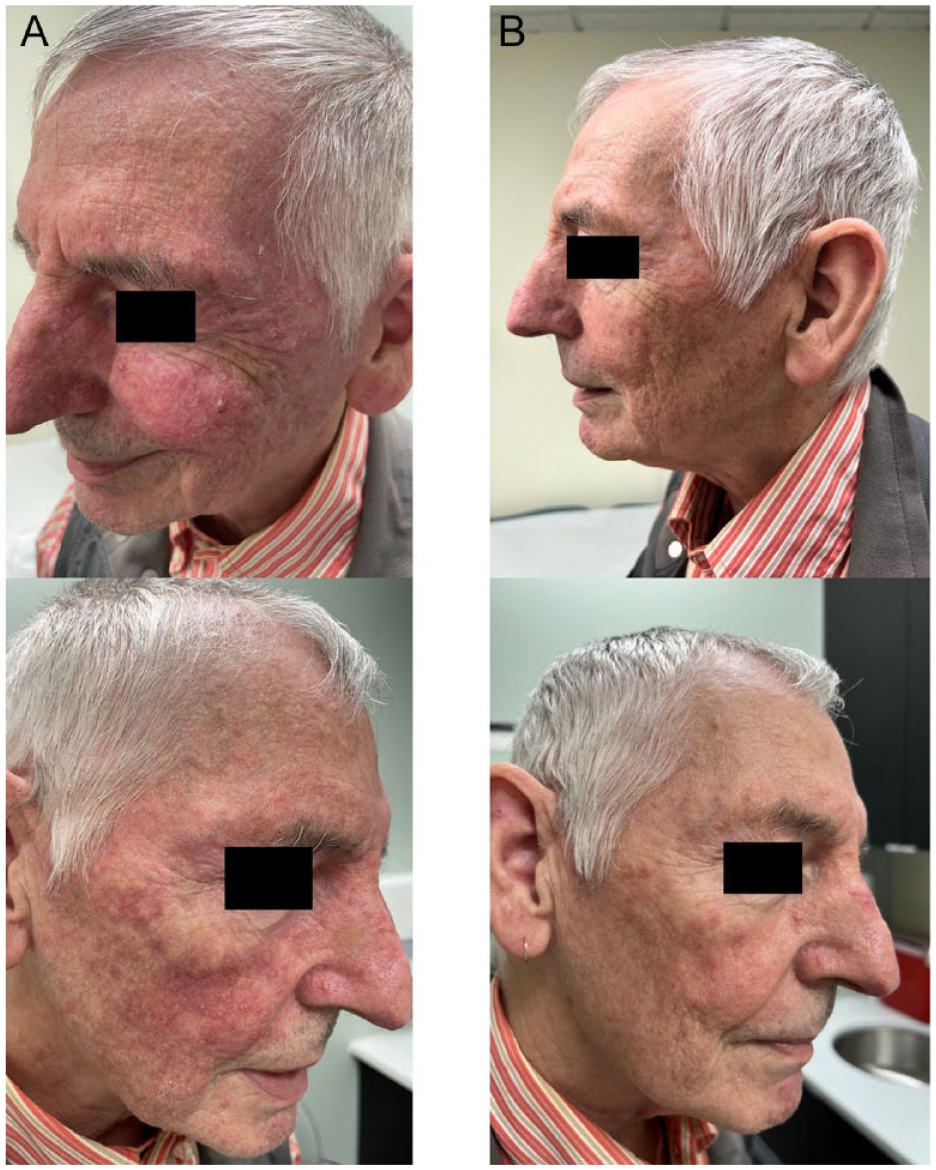
Facial photographs (A) pre- and (B) post-daylight MAL-PDT for a 72-year-old male with chronic actinic damage and numerous AKs on the bilateral cheeks, forehead, and nose. After 4 treatments with daylight MAL-PDT, marked improvement was noted with no significant procedural side effects. AKs, actinic keratoses; MAL-PDT, methyl aminolevulinate photodynamic therapy.
There is evidence that treatment modalities to improve photosensitizer penetration such as micro-needling and lasers enhances the efficiency of PDT. In a meta-analysis of 4 RCTs with a total of 240 participants, laser-assisted PDT with CO2 or Er:Yag AFL improved AK clearance rates compared to PDT monotherapy (RR: 1.33; 95% CI: 1.24-1.42) with no increased procedural pain. 38 In a meta-analysis of 5 RCTs with a total of 213 participants, the combination of micro-needling and ALA-PDT increased AK clearance rates compared to ALA-PDT monotherapy (mean difference: 6.01; 95% CI: 0.84-11.17), with no increased procedural pain. 39
Pre-treatment with topical treatments may improve photosensitizer accumulation and enhance PDT treatment outcomes. Similar AK clearance rates were reported for patients undergoing 1 session of MAL-PDT pretreated with 40% urea (60.8%), 10% salicylic acid (61.4%), or curettage (68.5%), but pre-treatment with urea and salicylic acid increased procedural pain in comparison to curettage (P < .05). 40 ALA-PDT with pre-treatment with 5-FU cream twice daily for 7 days showed increased AK clearance rates of 100% versus 82.6% (P = .0002) at 12 months compared to ALA-PDT alone. 41 A meta-analysis of 10 RCTs with a total of 277 participants found that the combination of PDT with topical treatments including imiquimod, 5-FU, ingenol mebutate, tazarotene, and calcipotriol increased complete clearance rates (RR: 1.63; 95% CI: 1.15-2.33) compared to PDT alone. 42 The evidence suggests that daylight-PDT is first-line for the treatment of grade I to II AKs and that conventional PDT is first-line for managing grade III AKs, but more work is required to clarify the role of combination PDT treatments with micro-needling and lasers in AK management.
Basal Cell Carcinomas
Basal cell carcinomas (BCCs) are keratinocytes malignancies and are the most common cancers worldwide. 43 Surgical excision definitively manages BCCs, but these procedures are time consuming, and may be associated with significant cosmetic and functional limitations. There are different subtypes of BCCs, including superficial, nodular, morpheaform, infundibulocystic, pigmented, and fibroepithelioma of Pinkus BCCs. PDT is approved for the treatment of low-risk, superficial BCCs (sBCCs). A meta-analysis of 7 RCTs involving 1339 patients and 1568 BCCs and 1 retrospective study involving 108 BCCs found that MAL-PDT has inferior 3-month (RR: 0.93; 95% CI: 0.89-0.97) and 12-month (RR: 0.90; 95% CI: 0.85-0.95) clearance rates compared to surgery, with an increased 12-month recurrence rate (RR: 10.43; 95% CI: 1.98-55.03) and more toxicities (RR: 2.12; 95% CI: 1.46-3.09). 44 However, MAL-PDT had superior cosmetic outcomes compared to excisional surgery (RR: 1.99; 95% CI: 1.5-2.63). It is important to note that excisional surgery is rarely employed in the clinical management of sBCCs. The more common treatment options for sBCCs include 5-FU, imiquimod, and cryosurgery. Imiquimod was superior to 2 sessions of MAL-PDT and 5-FU was noninferior to MAL-PDT in a RCT of 601 patients with sBCCs after 1 and 3 years.45,46 A follow-up cost-effectiveness analysis of this study cohort showed that imiquimod and 5-FU were more cost-effective than MAL-PDT for sBCC management. 47 A follow-up analysis of the cosmetic outcomes 5 years post-treatment showed modest improvements in the number of recurrence-free patients with good and excellent cosmetic outcomes after MAL-PDT when compared to imiquimod and 5-FU. However, due to the increased risk of sBCC recurrence in the MAL-PDT treatment group that may have required re-treatment with surgical excision, there were ultimately no statistically significant differences in cosmetic outcomes between the 3 treatment groups. 48 However, a subgroup analysis of this study cohort showed that MAL-PDT was superior to imiquimod in 1 subgroup of lower extremity sBCCs on patients > 60 years, which may be explained by functional barriers that elderly patients experience when applying topical medications on the lower extremities. 49 ALA-PDT had similar rates of histological recurrence of sBCCs at 12 months compared to cryosurgery (25% vs 15.4%; P > .05), but shorter healing times and improved rates of excellent cosmetic outcomes (50% vs 8%; P < .001). 50 Similarly, MAL-PDT showed statistically comparable sBCC recurrence rates at 5 years and improved rates of excellent cosmetic outcomes compared to cryosurgery (60% vs 16%; P = .00078). 51
Some studies have demonstrated value for PDT in the treatment of nodular BCCs (nBCCs). 52 Though MAL-PDT has inferior sustained nBCC complete response rates at 5 years compared to excisional surgery (76% vs 96%; P = .01), MAL-PDT increased the rate of good or excellent cosmetic outcomes (87% vs 54%; P = .007). 53 These findings were reinforced in other studies comparing PDT with surgical excision for nBCCs.54-56 Laser pre-treatment may enhance the efficacy of PDT for nBCCs by increasing the penetration of the photosensitizer. Pre-treatment with a Er:YAG AFL increased complete response rates for thin (≤2 mm) facial nBCCs at 3 months (82.4% vs 50%; P = 0.026) and lowered the recurrence rate at 12 months (6.3% vs 55.6%; P = .006). 57 The cumulative evidence suggests that though imiquimod is the first choice non-invasive treatment for sBCCs, PDT may be considered first-line for treating sBCCs on the lower extremities of elderly patients and for patients with nBCCs with contraindications for surgery.
Bowen’s Disease
Cutaneous SCC is the second-most common form of skin cancer, with an increasing worldwide incidence. 58 PDT -in some instances- can be used for the treatment of SCC in situ, otherwise known as Bowen’s disease (BD). Other treatment options for BD include surgical excision, 5-FU, imiquimod, and cryotherapy. In a meta-analysis of 4 RCTs with 292 patients, PDT had higher complete response rates (RR: 1.36; 95% CI: 1.01-1.84), reduced recurrence (RR 0.53; 95% CI 0.3-0.95), and improved cosmetic outcomes (RR 1.34; 95% CI: 1.15-1.56) compared to cryotherapy and 5-FU. 59 However, in comparison with surgical excision with a 5 mm safety margin, PDT has higher rates of treatment failure in a retrospective study of 608 patients with a median follow-up of 18 months (Hazard Ratio (HR): 2.71; 95% CI: 1.52-4.83). 60 It should also be noted that in a long-term follow-up study of MAL-PDT outcomes for BD, a sizeable recurrence rate of 71% at 5 years was noted and risk factors for recurrence included tumour size >300 mm2, upper extremity location, and age <70 years old. 61 There is some evidence that laser-assisted PDT enhances PDT therapeutic efficacy for BD. Pre-treatment with CO2 or Er:YAG AFLs improved BD clearance rates and reduced recurrence rates at 1 year (6.7% vs 31.6%; P = .022), 2 years (12.5% vs 63.6%; P = .006), and 5 years (9.3% vs 41.38%) compared to MAL-PDT alone.62-64 In addition, laser-assisted ALA-PDT improved BD clearance rates at 6 months compared to CO2 AFL alone (90.9% vs 63.63%; P < .05). 65 The body of evidence suggests that PDT is the non-invasive treatment of choice for patients with BDs who are poor surgical candidates.
Emerging Indications
Skin Field Cancerization
Skin field cancerization (SFC) is a process that occurs in areas of the skin that have undergone genomic alterations induced by ultraviolet radiation, with AKs being the product of this environment. PDT has shown promise in treating SFC. In a placebo-controlled RCT of patients with AKs and a history of NMSC, ALA-PDT delayed the mean time of appearance (9.86 months vs 7.14 months) and reduced the total number of new AK lesions at 12 months (14 vs 30; P < .001). 66 With respect to PDT treatment regimens for SFC, studies have shown that pulsed dye laser (PDL)-assisted MAL-PDT has inferior SFC clearance rates compared to conventional MAL-PDT (10.3% vs 44.9%; P < .01) and that 2 MAL-PDT sessions showed similar SFC clearance rates as 3 sessions held 1 month apart (85.4% vs 89.5%).67,68 There is some disagreement in the literature regarding the value of combining CO2 AFL to increase PDT efficiency for SFC clearance. The combination of CO2 AFL and MAL-PDT showed similar total numbers of new AKs and mean times of occurrence of new lesions in comparison with MAL-PDT alone. 69 SFC clearance with 2 sessions of daylight-PDT with MAL was significantly higher after CO2 AFL pre-treatment, in comparison with daylight-PDT with MAL alone, or in combination with micro-needling and micro-dermabrasion pre-treatment at 1 month (P = .002) and 3 months (P = .034) post-treatment, but no significant difference was seen at 6 months (P = .441). 70 The differences in treatment response observed in these studies may be related to patient selection, as the first study included patients with severely photodamaged skin with BCCs and SCCs, while the second study excluded patients with concomitant malignant lesions. This suggests that the combination of PDT with CO2 AFL is less efficacious in the cases of more severe cases of SFC. A few studies have compared PDT to active comparators for the treatment of SFC. In a RCT of patients with SFC, MAL-PDT and 5% imiquimod had comparable NMSC incidence rates at 12 months (16 vs 22, P = .157); however, more patients preferred MAL-PDT to imiquimod (59.1% vs 40.9%). 71 One session of MAL-PDT and twice-daily applications of 0.5% colchicine cream for 10 days had similar SFC clearance rates of the forearms at 60 days (19% vs 17%; P = .76 total clearance and 67% vs 44%; P = .07 partial clearance). 72 The body of evidence suggests that PDT is noninferior to other SFC treatment approaches, but more research is required to determine the role of combined CO2 AFL and PDT for SFC management.
Chemoprevention of AKs and NMSCs
There is growing interest in PDT to prevent AKs and NMSCs in high-risk immunosuppressed organ transplant recipients (OTRs). OTRs have a 65 to 140 times greater risk of developing SCCs, which account for 5% of all-cause mortality in OTRs. 73 PDT showed promise for the primary prevention and treatment of SCCs in OTRs; a meta-analysis of 3 RCTs with a total of 148 solid OTRs found that PDT reduced the incidence of AKs/SCCs (risk difference: 0.14; 95% CI: 0.08-0.19) and a separate analysis of 4 RCTs with 78 solid OTRs showed that PDT increased AK/SCC complete response rates (risk difference: 0.5; 95% CI: 0.22-0.79). 74 Numerous RCTs have compared PDT to other lesion or field treatment options including cryotherapy, 5-FU, and imiquimod. A RCT of OTRs showed that 2 MAL-PDT treatments, 1 week apart, reduced the incidence of new AK, NMSC, or wart lesions (65 vs 103; P = .01) at 3 months in comparison with lesion-directed cryotherapy, but the effect was not significant at 27 months (253 vs 312; P = .06). 75 Compared with a 3-week course of 5-FU, 2 cycles of MAL-PDT, 1 week apart, achieved higher rates of complete resolution of epidermal dysplasia (89% vs 11%; P = .02) in a RCT of OTRs. 76 Two cycles of MAL-PDT increased AK clearance rates (78% vs 61%; P < .001) and reduced the incidence of AKs (0.7 vs 1.5; P = .04) at 3 months for OTRs compared to a 4-week course of imiquimod. 77 Daylight-PDT with MAL reduced the incidence of AKs and NMSCs in OTRs at up to 15 months compared to lesion-directed cryotherapy (3 vs 4.8; P = .02). 78 However, there is one negative published study of the chemopreventative effect of PDT in OTRs. An RCT of 40 OTRs showing that 1 cycle of ALA-PDT did not reduce the incidence of SCCs at 2 years (15 vs 10; P = .81) on the PDT-treated forearms and hands compared to the contralateral untreated forearms and hands of the OTRs and another. 79 More research is necessary to clarify the optimal PDT protocol for the chemoprevention of AKs and NMSCs in OTRs, and to compare prophylactic PDT with other established NMSC chemoprophylaxis protocols including oral retinoid therapies.
Photoaging
Chronic prolonged sun exposure induces photoaging, a process by which the skin undergoes changes that can manifest as rhytids, telangiectasias, increased skin laxity, hyperpigmentation, lentigines, ephelides, volume loss, poikiloderma, and cutaneous dysplasia. Prevention of photoaging is centred around sun protection, and treatment options for photoaging include topical retinoids, 5-FU cream, chemical peels, micro-needling, neuromodulators, and laser resurfacing procedures. PDT is an emerging treatment modality in photorejuvenation. A placebo-controlled RCT showed that 2 treatments of MAL-PDT, 2 to 3 weeks apart, improved fine lines, course lines, mottled pigmentation, tactile roughness, sallowness, erythema, and sebaceous hyperplasia at 1 month post-treatment (P < .05). 80 In 2 placebo-controlled RCTs, 3 intense pulsed light (IPL)-assisted ALA-PDT treatments at 1 month intervals improved global photoaging scores, fine lines, mottled pigmentation, and coarse wrinkles as well as improved investigator cosmetic evaluations and subject satisfaction scores.81,82 Similar findings were observed in a study of photoaged skin of the dorsal hand, which found that IPL-assisted MAL-PDT reduced wrinkle size and skin roughness. 83 Studies have shown that PDT could be a valuable adjunct to micro-needling and laser therapies for photorejuvenation. In a split-face RCT of patients with photodamaged skin, micro-needling-assisted MAL-PDT significantly improved mottled pigmentation, coarse wrinkles, fine lines, roughness, and sallowness compared to MAL-PDT alone (P < .05). 84 Combined ALA-PDT and IPL treatments showed superior global aesthetic improvement scale results at 24 weeks compared to ALA-PDT alone (2.89 vs 3.57; P < .001) in a RCT of patients with moderate to severe photodamage of the chest. 85 In another RCT of patients with photodamage of the chest, the combination of 1927 thulium laser and MAL-PDT improved skin texture (P < .05) but did not improve overall photodamage, mottled pigmentation, or rhytids. 86 Less encouraging results were observed in another RCT of patients with photodamage of the chest; the combination of 1927 nm thulium laser and ALA-PDT did not improve skin wrinkling and texture compared to ALA-PDT alone, but increased the severity of adverse events including erythema, burning/stinging sensation, and edema. 87 One of the barriers of PDT for photoaging is procedural pain. A study of 18 patients with diffuse facial photodamage found that pre-treatment with 40% urea or 3% lidocaine hydrochloride creams had no impact on ALA-PDT treatment pain. 88 A split-faced RCT showed that indoor daylight-PDT with a polychromatic white light-emitting diode (LED) lamp had comparable improvements in tactile roughness and facial erythema compared to conventional PDT for patients with face and scalp photoaging, but reduced pain and inflammation (P < .0001). 89 There is limited evidence of the comparative efficacy of PDT for photorejuvenation relative to other active treatment modalities. ALA-PDT showed comparable global improvements in photoaging signs to 5-FU (50% for ALA-PDT with blue light illumination; 58% for ALA-PDT with pulsed dye light illumination; 67% for 5-FU) but was better tolerated with reduced erythema, crusting, and erosions. 90 In comparison with the long-pulsed Nd:YAG laser, IPL-assisted PDT with a 0.5% ALA liposomal spray showed improved Fitzpatrick Wrinkle Classification System scores for lateral periorbital wrinkles (mean score reduction of 0.9 vs 0.3; P < .05). 91 More research is required to compare PDT with other treatment modalities for photoaging.
Acne Vulgaris
Acne vulgaris is a common inflammatory disorder of the pilosebaceous unit. Early studies have demonstrated that photosensitizer preferentially accumulates in the pilosebaceous unit due to their lipidic cytoplasms and involvement in skin lipid and hormone control that facilitate uptake of the hydrophobic photosensitizer molecule, which facilitates the selective phototoxicity, anti-bacterial and anti-inflammatory effects of PDT at the culprit site of acne vulgaris. 92 In a meta-analysis of 13 RCTs involving a total of 701 subjects, PDT with ALA, MAL, and liposomal methylene blue significantly reduced inflammatory acne lesion counts (15.97%, P < .00001) compared to controls. 93 There is a growing number of methodological studies to inform optimal PDT parameters for acne, including choice of photosensitizer, light source, and procedural adjuncts. In a split-face trial of 15 patients with inflammatory facial acne, there was no significant difference between the MAL and ALA photosensitizers; however, the ALA-PDT treated area had more frequent and severe treatment adverse events. 94 Dose-finding studies showed that PDT with 10% and 15% ALA cream maximized treatment effectiveness and minimized adverse events such as erythema and pigmentation relative to PDT with 5% and 20% ALA cream.95,96 Similar treatment effects were observed in a split-face trial comparing the use of red light to IPL as MAL-PDT activators; however, red light showed a faster response time with better response after the first of 3 total treatment sessions. 97 There was no additional benefit observed in patients pretreated with 2 passes of non-ablative 1550 nm fractional erbium glass laser prior to daylight-PDT. 98 Daylight-PDT or a multi-step irradiance schedule represent approaches to reduce the procedural pain associated with PDT for acne vulgaris. Daylight-PDT with ALA was as efficacious as conventional ALA-PDT for acne but markedly reduced downtime (1.4 days vs 4.1 days; P = .001) and adverse reactions including erosions, erythema, pain, and pustules. 99 A 3-step irradiance schedule for ALA-PDT had similar acne clearance rates but significantly reduced pain (Visual Analogue Scale 1.61 vs 3.14; P < .0001) compared to a 2-step irradiance schedule with the same total irradiance dose of 84 J/cm2. 100
A comparative RCT found that ALA-PDT resulted in superior clearance rates of inflammatory acne lesions compared to IPL or blue-red LED light-based therapies (92% vs 58% or 44%; P < .01). 101 In a RCT of patients with moderate inflammatory facial acne, 2 sessions of ALA-PDT performed 2 weeks apart significantly reduced inflammatory lesions (84% vs 74%; P = .02) and total lesions (79% vs 67%; P = 0.026) at 12 weeks compared to patients that received daily oral doxycycline 100 mg and 0.1% adapalene gel. 102 Other studies have demonstrated that PDT is a valuable adjunct to oral antibiotics or retinoids. Patients who received 4 sessions of ALA-PDT, 1 week apart, combined with daily oral minocycline 100 mg had a greater reduction of inflammatory (74.4% vs 53.3%; P < .001) and noninflammatory (−61.7% vs −42.4%; P < .001) lesions and dermatology life quality index (DLQI; 4.4 vs 6.3; P < .0001) compared to the minocycline alone group at 8 weeks. 103 There is also evidence that PDT is a valuable adjunct to isotretinoin. The combination of 3 sessions of ALA-PDT, 2 weeks apart, and oral isotretinoin 10 mg twice daily for 3 months resulted in greater overall effectiveness rate at 12 weeks (94.1% vs 78.8%; P = .007) and reduced recurrence rate after 6 months (7% vs 24%; P < .05) for patients with acne vulgaris compared to ALA-PDT alone. 104 The literature supports the use of PDT to treat inflammatory acne vulgaris, but there is a need for more comparative research between PDT and current recommended therapies for acne vulgaris such as topical benzoyl peroxide, topical and oral retinoids, and topical and oral antibiotics.
Hand, Foot, Facial, and Genital Warts
Verrucae, or cutaneous warts, are a common skin condition caused by epidermal infection with human papilloma virus (HPV). Treatments for verrucae include topical keratolytics, cryotherapy, electrosurgery, laser therapy, cantharidin, imiquimod, sinecatechins, and intralesional treatments such as bleomycin and Candida antigen. PDT has been proposed as an effective treatment for warts. This is because of the propensity of photosensitizer accumulation in more rapidly dividing HPV-infected cells, resulting in the selective destruction of HPV+ skin cells in warts. A meta-analysis of 19 RCTs found that PDT improved the clearance rate of hand and feet warts compared to placebo (RR: 2.5; 95% CI: 1.13-5.51), other lasers including IPL and PDL (RR: 2.11; 95% CI: 1.47-3.02) and cryotherapy (RR: 1.57; 95% CI: 1.12-2.19), but had a similar cure rate compared to intralesional vitamin-D3 injection (RR: 1.03; 95% CI: 0.82-1.3). 105 The same meta-analysis found that PDT had superior cure rates for flat warts comparted to placebo (RR: 20; 95% CI: 2.83-141.24) and cryotherapy (RR: 1.29; 95% CI: 1.07-1.55). PDT has also been established as an effective adjunct to first-line keratolytic treatment for warts. A study demonstrated that combining standard keratolytic treatment with 30% salicylic acid daily for 8 days with 3 cycles of MAL-PDT at 1 week intervals reduced wart area compared to keratolytic treatment alone (48.4% vs 18.4%; P = .021). 106 Work has also been done to optimize PDT treatment protocol to reduce procedural pain and adverse events. Three cycles of daylight-PDT with ALA and conventional ALA-PDT at 1 month intervals had comparable rates of excellent response in children with flat facial warts at 24 weeks (73.3% vs 80%). 107 A dose-finding RCT of patients with recalcitrant flat facial warts found that PDT with 5% ALA had lower complete response rates compared to 10% ALA (33.3%) and 20% ALA (26.3%). As well, 20% ALA increased post-treatment hyperpigmentation (33.3%) compared to 5% ALA (15.6%) and 10% ALA (12.9%). 108 These findings suggest that PDT with 10% ALA offers the best efficacy and safety profile for the treatment of flat facial warts. Modifying the delivery vehicle of the photosensitizer may also enhance outcomes; PDT with methylene blue delivered within a transferosome nano-vesicular system had a higher rate of complete resolution of plantar warts relative to free methylene gel (86.67% vs 53.57%) and required a lower number of cycles (2.2 vs 4.14). 109
Condyloma acuminata (CA) is a sexually transmitted cutaneous infection of the anogenital region caused by certain variants of HPV. A number of studies have demonstrated that PDT improves outcomes in CA treatment. Traditional treatment for CA include topical trichloroacetic acid, imiquimod, cryotherapy, CO2 AFL, and surgical excision, but cure rates are around 50% with high recurrence rates. 110 In a meta-analysis of 6 RCTs, PDT had similar CA clearance rates to CO2 AFL (RR: 0.98; 95% CI: 0.95-1.00) and trichloroacetic acid (RR: 1.04; 95% CI: 0.59-1.83). 105 Another meta-analysis of 20 RCTs found that ALA-PDT reduced the recurrence rate of CA at 2 weeks compared to CO2 AFL (RR: 0.26; 95% CI: 0.2-0.35) and cryotherapy (RR: 0.49; 95% CI: 0.28-0.87). 111 There is also evidence that the combination of PDT with locally destructive therapies such as cryotherapy or CO2 AFL enhances CA clearance rates. The utility of PDT as an adjunct to cryotherapy was demonstrated in a RCT that showed that ALA-PDT immediately after cryotherapy in 2 treatment sessions separated by 7 days increased CA clearance rates in the urethral meatus (100% vs 54.5%; P < .05) and external genitals (94.2% vs 50.5%; P < .05) when compared to cryotherapy alone. 112 Conversely, adjuvant ALA-PDT after CO2 AFL showed similar CA recurrence rates at 12 weeks compared to adjuvant placebo-PDT after CO2 AFL (50% vs 52.7%; P = .72). 113 A clinical analysis was performed to assess the efficacy of 5 CA treatment methods: cryotherapy, CO2 AFL, ALA-PDT, ALA-PDT immediately after cryotherapy, and re-treatment ALA-PDT after lesion clearance from cryotherapy or CO2 AFL. In all PDT groups, ALA-PDT was administered in 4 cycles, 1 week apart. This study found that the optimal treatment approach for CA depends on lesion size; ALA-PDT alone is preferred if the lesion was <0.5 cm, ALA-PDT immediately after cryotherapy was preferred if the lesion was between 0.5 and 2 cm, and re-treatment ALA-PDT after lesion disappearance from cryotherapy, or CO2 AFL, was preferred if the lesion was >2 cm. 114 A series of studies have identified approaches to reduce procedural pain and enhance patient acceptability of PDT for CA. One approach is to use a 2-step protocol, which starts with a low fluence rate to reduce the pain associated with the subsequent higher fluence rate, resulting in photobleaching of PpIX and reduced tissue inflammation. A RCT comparing a 2-step protocol using a low fluence rate of 40 mW/cm2 for 8 minutes followed by a high fluence rate of 80 mW/cm2 for 16 minutes with an equivalent 1-stop protocol at 80 mW/ cm2 for 20 minutes, found that the 2-step protocol significantly reduced pain scores when compared to the 1-step control (P < .001). 115 Other studies have found that the 2-step procedure was more effective than procedural pain control with cold compresses (P < .0001), with no difference in cure rates. 116 The evidence suggests that PDT should be considered as an efficacious treatment of recalcitrant hand, foot, facial, and genital warts.
Onychomycosis
Onychomycosis is a fungal nail infection that can be difficult to treat and often requires the protracted administration of systemic antifungals which have important side effects such as hepatotoxicity. 117 In vitro studies have demonstrated that Trichophyton rubrum, the dermatophyte primarily responsible for onychomycosis, metabolizes ALA to PpIX, and that PDT inhibits dermatophyte growth. 118 With the growing issue of anti-fungal resistance, an alternate form of therapy may be a welcome option or adjunct to current standards of care for onychomycosis. Case series and single-arm clinical trials show that PDT is generally effective for the treatment of onychomycosis, but a wide range of treatment effects were reported, which may be related to the heterogeneous PDT protocols assessed in the studies. One study reported a cure rate of 43.3% at 12 months of ALA-PDT for toenail onychomycosis, which reduced to 36.6% at 18 months. 119 In a single-arm clinical trial of PDT with an aluminum-phthalocyanine chloride nanoemulsion, clinical cure was reported in 60% of treated lesions, but only 40% achieved mycological cure. 120 In a case series of 62 patients treated with methylene blue and toluidine blue-PDT for onychomycosis, complete and partial clearance was observed in 45% and 40% of patients, respectively. 121 Another study exploring the utility of methylene blue-PDT found that the clinical response is dependent on onychomycosis severity, with a 100% clinical response rate for mild-to-moderate onychomycosis and a 63.6% response rate for severe onychomycosis. 122 The choice of photosensitizer appears to strongly influence the effectiveness of PDT for onychomycosis. The evidence suggests that topical PDT with the MAL and ALA photosensitizers have limited clinical utility in the treatment of onychomycosis. A placebo-controlled RCT found that MAL-PDT with 40% urea pre-treatment resulted in comparable rates of clinical and microbiological cure compared to 40% urea alone with placebo-PDT. 123 An open-label comparative study showed that patients with onychomycosis treated with laser-assisted ALA-PDT had similar mycological clearance rates compared to the laser-assisted 5% amorolfine nail lacquer control group. 124 In a comparative study of methylene blue-PDT and MAL-PDT, the methylene blue-PDT group had a complete cure rate of 70% at 40 weeks, compared to 40% in the MAL-PDT group. 125 These findings suggest that methylene blue-PDT is more effective than MAL-PDT and ALA-PDT for onychomycosis, but more research is required to compare the photosensitizers. Several RCTs have compared PDT with other accepted treatment modalities for onychomycosis. In a RCT of 40 patients with great toe onychomycosis, methylene blue-PDT was found to be comparable with IPL, with 70% and 80% achieving complete cure, respectively. 126 A study comparing weekly methylene blue-PDT to 300 mg oral fluconazole for 24 weeks found that methylene blue-PDT increased clinical and mycological cure rates when compared to fluconazole (90% vs 45%; P < .001), especially in patients who required nail plate abrasion. 127 In an RCT of 51 patients with onychomycosis, pre-treatment CO2 AFL followed by 6 sessions of methylene blue-PDT with IPL resulted in the greatest percentage improvement in proximal nail diameter (52.94% ± 20.24) compared to CO2 AFL (43.82% ± 21.03) or methylene blue-PDT with IPL (35.29% ± 17.0) alone. 128 There was no significant difference in mycological cure rates between the 3 groups (64.7% for methylene blue-PDT with IPL; 76.5% for CO2 AFL; 88.2% for combined CO2 AFL and methylene blue-PDT with IPL). The evidence suggests that methylene blue-PDT may be superior to oral fluconazole and comparable in efficacy to IPL for onychomycosis, but larger-scale RCTs are necessary to compare the efficacy of PDT with other treatment modalities for onychomycosis.
Cutaneous Leishmaniasis
Old world cutaneous leishmaniasis (CL) results from cutaneous parasitic infection of dermal macrophages with Leishmania spp., which are spread by the bite of Phlebotomus sand flies that are endemic to parts of Asia, Africa, and Europe. The other main forms of leishmaniasis are visceral leishmaniasis, which causes fever, anemia, weight loss and hepatosplenomegaly, and mucocutaneous leishmaniasis, which leads to lesions affecting the mucous membranes of the mouth, nose, and throat. CL results in significant morbidity, due to secondary infections, ulceration, and disfiguring scars, and high rates of failure with traditional treatment options. 129 Treatment choices for CL include intralesional or intravenous sodium stibogluconate and meglumine antimonate, amphotericin B, paromomycin, cryotherapy, excision, curettage, and electrodessication. 130 PDT has been shown to reduce parasite load in CL by depopulating infected macrophages and initiating the host immune response to enhance parasite clearance. 131 Topical PDT has shown efficacy in treating CL, typically caused by Leishmania major and L. tropica; however, topical PDT is not suitable for the management of mucocutaneous or visceral leishmaniasis associated with L. braziliensis and L. donovani, respectively. ALA-PDT has demonstrated efficacy in treating CL, with a case series of 11 patients reporting excellent clearance of amastigotes and a considerable reduction in size and thickness of the CL lesions from L. major after 1 to 2 treatments. 132 There are very few comparative studies between PDT and other available treatment modalities for CL. One case report comparing the efficacy of twice-weekly MAL-PDT to daily 15% paromomycin ointment for 4 months in 1 patient with 10 CL lesions from L. donovani found that all 5 PDT-treated lesions resolved, while only 2 of the paromomycin-treated lesions resolved. The other 3 paromomycin-refractory lesions responded to adjunct MAL-PDT. 133 There is only 1 published RCT, which found that weekly ALA-PDT increased complete clinical improvement rates (93.5% vs 41.2%; P < .001) and pathological cure rates (100% vs 64.7%; P < .001) of CL lesions from L. major compared to twice-daily applications of 15% paromomycin ointment for 4 weeks. 134 In a proof of concept study for the use of daylight-PDT for the management of CL, an overall cure rate of 89% was found in a sample of 31 patients (11 with lesions from L. major and 20 with lesions from L. tropica), as well as comparable efficacy between supervised daylight-PDT in the hospital garden and self-administered home daylight-PDT. 135 One study looked at a fractional illumination PDT strategy in patients with CL lesions caused by L. tropica and found that the fractional MAL-PDT group receiving 3 illumination fractions had improved complete response rates compared to conventional MAL-PDT with an equivalent total dose of 90 J/cm2 over 3 sessions (91.4% vs 76%). 136 They also found marked reductions in pain and burning sensation for the fractional MAL-PDT group. The evidence suggests that PDT is superior to paromomycin in the treatment of CL, but more RCTs are required to compare PDT with the other available CL treatment options and to optimize PDT protocols for CL clearance and patient tolerability.
Actinic Cheilitis
Actinic cheilitis (AC) is a premalignant lesion of the lip that requires early treatment to terminate its progression into lip SCC. Traditional treatment strategies include cryotherapy, surgical or CO2 laser vermilionectomy, and topical treatments with 5-FU, imiquimod, or topical diclofenac in hyaluronic acid. To date, there are no comparative studies between PDT and other AC treatment strategies. However, in a systematic review of 49 studies, PDT had lower AC complete response rates (68.9%) in comparison with the 100%, 93.8%, and 75% overall complete response rates reported with surgical, laser, and topical 5-FU treatments, respectively. 137 There is evidence that daylight-PDT is as efficacious as conventional PDT for AC with a better adverse event profile. In a systematic review of 19 studies, daylight-PDT had comparable AC clinical response rates (76.7%) to conventional PDT (80%) and ALA patch-PDT (65.1%), but is better tolerated with more painless patients (daylight-PDT: 87.1%; conventional PDT: 31.25%) and reduced rates of moderate and severe local phototoxic reactions (daylight-PDT: 0%; conventional PDT: 47.78%; ALA patch-PDT: 21%). 138 There has also been some emerging research on combination PDT treatment options for AC. The combination of MAL-PDT followed by a 4-week course of 5% imiquimod cream 3 days per week showed an AC complete response rate of 80%, with only 2 recurrences in a single-armed study of 34 patients. 139 One session of Er:YAG AFL-assisted MAL-PDT showed superior AC complete response rates at 3 months (92% vs 59%; P = .04), and reduced recurrence rates at 12 months (8% vs 50%; P = .029) compared to 2 sessions of MAL-PDT alone. 140 Though there may be promise in the combination of topical PDT with lasers, the overall quality of evidence regarding the role of topical PDT in the management of AC is poor. In addition, in view of the reduced AC complete response rates with topical PDT compared to other treatment modalities and the high risk of AC progression to SCC of the lip, the evidence suggests that topical PDT should not be considered first-line in the management of AC.
Early-Stage Mycosis Fungoides
Mycosis fungoides (MF) is a monoclonal proliferation of CD4+ or CD8+ mature T lymphocytes and is the most common type of cutaneous T-cell lymphoma. MF presents as localized patches or plaques in early stages and often has an indolent course, but may progress to more aggressive tumours and become erythrodermic or metastasize in advance stages. PDT has shown promise in the treatment of early-stage MF; however, there are no placebo-controlled studies exploring the efficacy of PDT with MAL or ALA. In a systematic review of 8 case reports/series with a total of 44 patients found that 67.3% with Stage 1A MF affecting a wide range of body surface areas from 1 to 154 cm2 achieved complete response after PDT (MAL was used in 97.7% of the cases) with a mean of 9.5 treatment cycles. 141 ALA-PDT may be less effective than MAL-PDT for the treatment of early-stage MF. Objective response rates to ALA-PDT every week for up to 6 cycles were only found in 36.4% of patients with refractory MF, defined by failure of at least 2 skin-directed therapies or 1 systemic therapy, with no patients achieving complete remission. 142 A case series showed that 4 to 12 treatments of CO2 AFL-assisted MAL-PDT resulted in complete remission of all 4 patients with Stage 1A MF affecting a body surface area of 8 to 154 cm2 on various sites of the body including the inguinal region, buttocks, cheek, and thigh. 143
Hypericin is an emerging photosensitizer for PDT that is preferentially absorbed by malignant cells and inhibits the proliferation and induces the apoptosis of malignant T lymphocytes. 144 In a phase II placebo-controlled study of patients with patch or plaque MF, twice-weekly hypericin-PDT treatments for 6 weeks resulted in a response rate at 41.7% and 55.6%, with 0.1% and 0.25% hypericin, respectively. 145 In a phase III RCT of patients with Stage 1A or 1B MF, 6 weeks of hypericin-PDT improved index lesion response rates of at least 50% relative to placebo (16% vs 4%; P = 0.04), with only mild local skin and application-site adverse events noted. Patients that received two and three 6-week hypericin-PDT treatment cycles had further improvements in index lesion response rates compared to a single treatment cycle of hypericin-PDT (49% after 3 cycles and 40% after 2 cycles vs 16% after 1 cycle; P < .001). 146 In phone interviews of patients treated with MAL-PDT for Stage 1A or 1B MF refractory to topical chemotherapies, patients reported a higher mean satisfaction score for MAL-PDT compared to topical chemotherapies (6.8 vs 4.8; P = .0271). 147 In addition, the study found that if patients were given a choice, 82% preferred MAL-PDT to topical chemotherapy. There are no comparative studies that assess the efficacy of PDT relative to other treatment options for MF including skin-directed therapies such as topical corticosteroids, nitrogen mustard, carmustine, retinoids, and phototherapy (ie, psoralen with UVA and narrow band-UVB), and systemic treatments such as interferon-alpha, oral retinoids, histone deacetylase inhibitors, and brentuximab. The evidence suggests that PDT can be considered in the management of early-stage MF, but there is a need for placebo-controlled studies and comparative studies between hypericin-PDT, MAL-PDT, ALA-PDT, and other active treatment options for early-stage MF.
Extramammary Paget Disease
Extramammary Paget disease (EMPD) is a rare intraepithelial neoplasm that classically presents as erythematous, ill-defined, pruritic, scaly plaques in the anogenital region. The accepted standard of care for EMPD is surgery with either wide-local excision or Mohs micrographic surgery, and non-surgical approaches including laser therapy, topical imiquimod, 5-FU, and radiotherapy have also been utilized. EMPD has a high local recurrence rate even after the gold-standard surgical approaches. A systematic review and meta-analysis of 27 studies, reported recurrence rates of 7.3% and 26.6% after Mohs micrographic surgery and wide-local excision, respectively. 148 A recent systematic review of 30 case series and reports of 177 patients with 211 EMPD lesions found that ALA-PDT and MAL-PDT have complete response rates of 57.7% and 27.4%, respectively; however, they had high recurrence rates of 40% and 35%, respectively. 149 PDT was found to be a valuable adjunct to imiquimod, laser, and surgical therapeutic strategies, with complete response rates of 100%, 60%, and 100% and recurrence rates of 0%, 8.3%, and 25.6% respectively. Since the publication of that systematic review, a case report showed that 6 sessions of MAL-PDT at 4-week intervals followed by topical 5% imiquimod every other day for 4 months resulted in the sustained remission of perianal EMPD during a 2-year surveillance period. 150 Another case series reported that photodynamic diagnosis, which also uses a photo-excitable compound, was valuable to guide tumour excision by forecasting the EMPD tumour margins and that 2 to 4 cycles of ALA-PDT intra- and post-operatively resulted in no local reoccurrences in a mean follow-up of 2.9 years. 151 There is some preliminary evidence that PDT should be considered for patients with EMPD who are poor surgical candidates or as an adjunct to surgical excision, but there is need for comparative studies between PDT and other treatment modalities for EMPD.
Lichen Sclerosis
Lichen sclerosis (LS) is a chronic inflammatory skin disease that typically involves the anogenital areas of postmenopausal women, with the main symptoms being vulvar itch, pain, and dyspareunia. Various treatment modalities have been described in the management of LS including topical corticosteroids, calcineurin inhibitors, estrogens, retinoids, and cryotherapy. Numerous case reports and series have supported the role of ALA-PDT in the treatment of recalcitrant LS of the vulva and penis, with gradual resolution of the burning, pruritis and pain, improved DLQI scores, and reduced lesion sizes.152-155 These findings were concordant with observational studies with a total of 213 patients with LS. Treatment with PDT resulted in LS clinical remission rates of 51% to 100%.156-159 One of the primary limitations of PDT for LS is the significant procedural pain. In 1 case report, the patient refused to be re-treated with MAL-PDT after clinical relapse of her vulvar LS due to the intense pain during the illumination sessions and the distressing experience of local anaesthetic administration. 160 One potential approach to reduce PDT procedural pain is to illuminate with a green light instead of the standard red light source. In a case series of 11 patients, ALA-PDT with green light illumination was efficacious for LS with complete resolution of erosions in all 5 patients who previously had visible vulvar LS erosions and pruritis in 81.8% of patients at 2 months after topical PDT; in addition, no patients complained of severe pain during the sessions that required analgesia or stopping the illumination. 161 A small number of case studies have explored the utility of laser-assisted PDT. The combination of 1927 nm thulium fibre laser followed by MAL-PDT resulted in the complete clearance of recalcitrant LS of the penis in 2 patients and PDL-assisted MAL-PDT improved clearance of extragenital LS lesions compared to PDL alone.162,163 There is evidence that PDT has a role in the management of LS, but there is a need for studies that compare the efficacy of PDT with other accepted treatment approaches for LS.
Folliculitis Decalvans
Folliculitis decalvans (FD) is a rare primary scarring alopecia characterized by painful, recurrent perifollicular pustules resulting from neutrophilic inflammation of the scalp. Combined topical and oral antibiotics, topical and intralesional steroids and oral retinoids are used to manage FD; however, relapses are frequent. 164 PDT has shown some efficacy in the management of FD. Two case reports reported that 3 cycles of MAL-PDT and 4 cycles of ALA-PDT resulted in sustained remission of FD for 1 year without any adjunctive therapy.165,166 These encouraging findings were corroborated by a prospective study showing that 4 sessions of MAL-PDT resulted in a clinical response for 9/10 patients with FD, with 6 patients exhibiting disease remission, and a retrospective study showing that 9/13 patients with FD undergoing 3 sessions of ALA-PDT were well-controlled with no recurrence at 12 months.167,168 However, the literature includes some conflicting results, with 1 case series reporting treatment failure for 3 patients with recalcitrant FD treated with a mean number of 11 MAL-PDT sessions. 169 The evidence suggests that PDT should be considered for refractory FD, but the available studies had small sample sizes and lacked control groups and thus comparative research is required to establish the role of PDT amongst the other treatment options for FD.
Conclusion
Topical PDT is a widely approved therapy for AKs and low-risk NMSCs with a rapidly growing range of emerging indications for other neoplastic, infectious, and inflammatory cutaneous diseases. There is evidence that PDT is superior or noninferior to many other available treatment modalities for AKs, low-risk BCCs, BD, SFC, the chemoprevention of AKs and NMSCs in OTRs, photoaging, acne vulgaris, and cutaneous infections including verrucae, onychomycosis, and CL. There is emerging evidence that PDT plays a role in the management of AC, early-stage MF, EMPD, LS, and FD but there are no comparative studies with other accepted treatment modalities for these conditions. More high-quality, larger-scale RCTs are required to compare topical PDT with active comparators for all approved and emerging indications to support and guide evidence-based clinical decision-making. There is significant heterogeneity in the topical PDT protocols reported in the literature, and more methodological research is required to address the commonly observed barriers to PDT including procedural pain, postprocedural skin reactions, cost of the procedure, and the time spent in the office to complete the PDT therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent
Consent was obtained for publication of the images.