
Abstract
Psychodermatology pertains to the relationship between the skin and brain. This review aims to summarize the evidence of the mind body connection in four psychophysiological conditions: rosacea, atopic dermatitis (AD), acne vulgaris (AV), and psoriasis. A literature search was conducted using several English language databases. All four conditions share similar psychiatric co-morbidities, including but not limited to anxiety, depression, and suicidality. In rosacea, the upregulation of transient receptor potential vanilloid type 1, Toll like receptor 2, and Th17 cells releases downstream products that are simultaneously implicated in mood disorders. Stress exacerbates AV through the hypothalamic-pituitary-adrenal (HPA) system, which alters functioning of sebocytes and Cutibacterium acnes. In AD and psoriasis, the HPA axis influences Th1, Th2, Th22, and Th1, Th17 immune mediated responses, respectively. This leads to the secretion of pro-inflammatory cytokines which are also involved in the pathogenesis of anxiety and depression. Neurotransmitters implicated in mental illness, such as gamma-aminobutyric acid and serotonin, may also play a role in the development of AD and psoriasis. The management of cutaneous disease may mitigate psychological distress, and future research may show the corollary to also be true.
Introduction
Psychodermatology is the interaction between dermatology and psychiatry. 1 -3 The connection between the two disciplines lies within the neuroendocrine and neuroimmune systems, collectively known as the neuro-immuno-cutaneous system (NICS). 1,2 Approximately 30 to 60% of dermatologic conditions have psychiatric aspects. 1 Although dermatologists have an increased awareness about the psychological aspects of skin conditions, many psychiatric co-morbidities are still undiagnosed and left untreated. 1 This underscores the need for a multi-disciplinary approach.
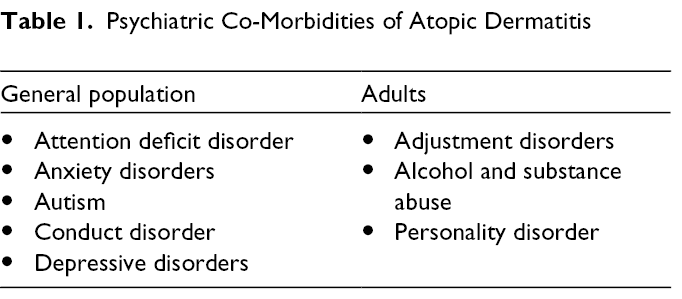
Psychodermatology is classified into three categories: psychophysiological conditions, primary psychiatric and secondary psychiatric disorders (Table 1). Psychophysiological disorders are skin conditions caused by or exacerbated by stress and other emotional factors. 1 -4 Primary psychiatric disorders are characterized as self-induced cutaneous manifestations that arise from underlying psychiatric conditions. 1,3,4 Conversely, individuals with secondary psychiatric conditions experience mental health issues that are a result of pre-existing skin conditions. 1,3,4 This review focuses on four psychophysiological disorders: rosacea, acne vulgaris (AV), atopic dermatitis (AD), and psoriasis. We hypothesized that psychiatric co-morbidities are attributable to shared pathomechanisms involving the NICS, and that modification of dermatologic conditions with drugs and cognitive therapies may have a parallel effect on mental health issues.
Psychiatric Co-Morbidities of Atopic Dermatitis
Methods
An English language literature review was conducted between October 2021 and February 2022 using variations of MeSH and key terms: “dermatitis, atopic,” “psoriasis,” “rosacea,” “acne vulgaris,” anxiety disorders,” “depressive disorder,” “cytokines,” “inflammation,” and “psyc*.” PubMed, Scopus, Medline and Google Scholar databases were utilized with no restriction on the year of publication. The Cochrane database was also searched but yielded no additional results.
Results
Rosacea
Psychiatric co-morbidities
Among all psychiatric co-morbidities, Chung et al. found that rosacea patients exhibit the highest risk for phobic disorder, followed by obsessive-compulsive disorder, major depressive disorder (MDD), and bipolar disorder. 5 Rosacea patients are at least twice the risk to develop anxiety and depression compared to the general population, with approximately 20% and 15% of patients having concurrent depression and anxiety, respectively. 6,7 Many patients experience a diminished quality of life (QoL) in terms of social outcomes, such as being hired for work and developing relationships with others. 5
Pathophysiology mechanism of the skin-brain Axis
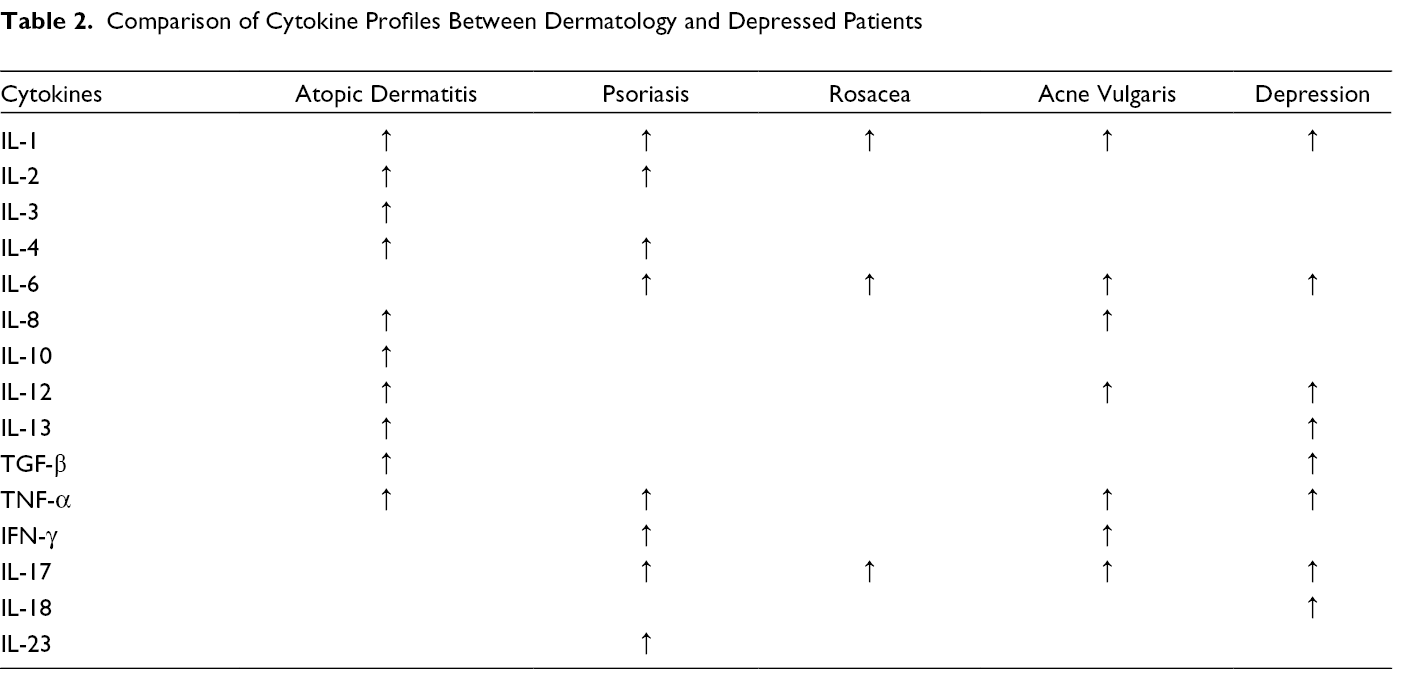
Several investigators have found an overexpression of the transient receptor potential vanilloid type 1 (TRPV1) channel in rosacea patients. 7 -9 TRPV1 functions as a primary sensor of thermal and chemical stimulation in the skin. When stimulated, it modulates vasodilation, inflammation and the sensation of pain. 8,9 After exposure to various rosacea triggers, TRP receptors become overexpressed and release neuropeptides including calcitonin gene-related peptide (CGRP), pituitary adenylate-cyclase-activating polypeptide and substance P (SP). 8 These neuropeptides act directly on endothelial and muscle cells to mediate vascular effects and degranulation of mast cells, 7 resulting in the characteristic flushing, erythema, and inflammation seen in rosacea. 8 Mast cell degranulation releases secretory granules including tryptase, which induces migration of matrix metalloproteinases (MMPs) to the skin. 8 In rosacea, increased MMP activity leads to the degradation of the extracellular matrix, contributing to erythema, telangiectasia, and inflammation. 8,9 Of interest, some investigators have documented higher levels of MMPs among depressed patients, suggesting this may be a shared mechanism linking rosacea to mental health issues. 10,11 In addition, keratinocytes of rosacea patients express increased Toll-like receptor 2 (TLR-2), which activates kallikrein related peptidase 5, which in turn cleaves human cathelicidin antimicrobial protein into the antimicrobial protein cathelicidin, LL-37. 12 LL-37 recruits leukocytes and mast cells, inducing angiogenesis and vasodilation, and releasing various cytokines, for example, IL-1 and IL-6. 12 Of note, circulating serum levels of LL-37 are also higher in bipolar and depressed patients who do not have cutaneous disease compared to healthy subjects. 13,14 Finally, both rosacea patients and depressed individuals may express increased numbers of Th17 cells, with animal models linking increased Th17 cells to depression-like behaviors (Table 2). 8 A main cytokine secreted by Th17 cells, IL-17, can also induce expression of MMP-9 and dysregulate or enhance the expression of LL-37. 15
Comparison of Cytokine Profiles Between Dermatology and Depressed Patients
Behavioural and pharmacological interventions
Cognitive-behavioral therapy (CBT) techniques has been shown to reduce social anxiety and depressive mood, and increase sense of control in rosacea patients. 16,17 However, a study utilizing the Dermatology Life Quality Index (DLQI) found that rosacea patients with a shorter duration of disease were more likely to have higher DLQI scores. 18 Therefore, offering psychological treatment earlier may enhance the patient’s chance for a response.
Treatment of rosacea patients with refractory erythema and flushing has been explored using intradermal botulinum toxin (BoNT) injection. 9,19 BoNT modulates blood vessel dilatation while also exerting an anti-anxiety and anti-depressant effect. 19 -22 Doxycycline, minocycline and metronidazole have been shown to exhibit anti-inflammatory effects and reduce the erythematic appearance of rosacea. 8,23 A recent clinical trial of minocycline and metronidazole have also shown positive effects in humans with depression and rats with anxious-depressive behavior, respectively, 24,25 while doxycycline has exhibited antidepressant effects in animal models of depression. 26,27 Finally, in an animal model of LL-37 induced rosacea, aspirin was shown to reduce erythema and telangiectasia by decreasing the expression of chemokines and cytokines, such as IL-1α and IL-1β, and suppressing the Th17 immune response. 28 However, aspirin’s ability to treat depression, anxiety and stress related disorders in humans has garnered mixed results. 29 -31
Gaps in knowledge and future research
Comparative outcomes across studies are difficult to assess due to heterogenous methods of reporting psychological symptoms and diagnoses. Development of a standardized screening tool specific to rosacea would be of interest for future use. Currently, no data exists to indicate antidepressants or anti-anxiety medications can improve rosacea and there is limited evidence that psychotherapy will mitigate the symptoms of rosacea. Although there is emerging evidence that IL-17 has a shared role in the skin-brain axis, the actual mechanism of IL-17 in mental illnesses is largely unexplored. As such, IL-17 inhibitors may play a role in the management of refractory rosacea, especially those with depression.
Further study of doxycycline, minocycline and metronidazole is necessary to investigate the direct effect on the psyche of rosacea patients, as well as patients with anxiety and depression alone. Whether topical anti-inflammatory medications, such as azelaic acid and ivermectin can mitigate concurrent psychological symptoms has yet to be explored.
Acne Vulgaris
Psychiatric Co-morbidities
Acne vulgaris is associated with low self esteem, anxiety, depression, and suicide. 32 The latter is especially prevalent among adolescents with acne. 32 Severe acne can result in hospital admission for anxiety, adjustment, personality, and substance use disorders. 33 A recent study identified acne patients to be at particularly high risk for developing post-traumatic-stress-disorder during the COVID-19 pandemic compared to individuals without acne. 34 AV heavily disrupts an individual’s personal and professional life, and reduces their QoL. 32,35
Pathophysiology of the skin-brain axis
Stress triggers the hypothalamic-pituitary-adrenal (HPA) system to produce stress-related neuropeptides and neurotransmitters which impact peripheral target organs, including the skin. 35 Recent studies have shown that sebocytes express functional receptors for corticotropin releasing hormone (CRH), β-endorphin, vasoactive intestinal polypeptide, neuropeptide Y and CGRP. 36 These ligands signal the local production of inflammatory cytokines and induce androgen metabolism and lipogenesis in sebocytes. 36 This may in turn further lead to proliferation of Cutibacterium acnes. 36 It is of interest to note that dysregulated levels of androgens are also implicated in the development of anxiety and depressive disorders. 36
C. acnes has been shown to activate inflammasomes within sebaceous glands, inducing them to release pro-inflammatory cytokine, IL-1β. 37,38 C. acnes also binds TLRs 2 and 4 on keratinocytes to increase levels of IL-8 and IL-12. 39 This simultaneously stimulates the NF-kβ signaling pathway, leading to a downstream expression of IL-1β, TNF-α, IL-1α, IL-6 and IFN-γ. 39,40 Wachowska et al. confirmed that depressed individuals have raised serum levels of IL-1 and IL-6 compared to healthy individuals. 41 Further, the results of a meta-analysis noted there were increased levels of IL-6, TGF-β, TNF-α and IFN-γ in suicidal patients compared to non-suicidal controls. 40 Furthermore, C. acnes activates Th1 and Th17 lymphocytes which then produce IL-17 within acne lesions. 39 In mice, cumulative stress may lead to long-lasting depressive symptoms through the upregulation of IL-17, 42,43 and administration of IL-17A alone may precipitate depression-like behavior. 44 Along with elevated Th17 cells, depressed patients can also exhibit elevated serum IL-17 levels. 8,45
Behavioural and pharmacological interventions
Psychotherapeutic interventions, such as relaxation techniques and visualization, have been shown to reduce depression and social phobia in acne patients, and can improve the skin too. 36 Some investigators have reported the greatest reduction in both psychological and skin disease was achieved with oral isotretinoin therapy. 36 Isotretinoin has been linked to depression, suicide, psychosis and mania, 36,46 but a recent population-based study found no increased risk of psychiatric disorders associated with this drug. 47 As isotretinoin can reduce expression of MMPs, the reduction in depressive symptoms in acne patients may be explained in part through this anti-inflammatory effect. 48 Although the role of MMPs in acne lesions is not as well understood as it is in rosacea, tetracycline antibiotics such as doxycycline and minocycline can also target MMP activity. 49,50
Oral contraceptive pills (OCP) and spironolactone diminish acne through their anti-androgen effects. 51 While spironolactone has potential anti-depressant effects, results for the modulation of depressive symptoms with use of OCPs is unclear. 52 -55
Gaps in knowledge and future research
Studies exploring the use of anti-anxiety or anti-depressant medications of acne patients’ cutaneous symptoms may be warranted. No study has explored the effect of IL-17 inhibitors on acne and the psyche. As well, future research investigating the inhibition of the other cytokines identified in acne, such as IL-1, IL-6 or TNF-α may be of value. Continued cytokine sampling from acne lesions at different stages in animal and clinical studies is necessary. Finally, further research on the impact of hormonal treatments on the skin and psyche would be of interest.
Atopic Dermatitis
Psychiatric co-morbidities
Atopic dermatitis is associated with many psychological co-morbidities in all age groups and includes attention deficit disorder, depression and anxiety (Table 1). 56 -58 AD impairs the sleep quality of affected individuals and their caregivers too. 58,59 This, along with pruritus, social isolation, and stigmatization contributes to the mental distress associated with AD.. 56,57,59
Pathophysiology mechanism of the skin-brain axis in atopic dermatitis
Up to 70% of AD patients experience an emotional stressor before an onset of AD. 59,60 Stress induces the release of cortisol, adrenocorticotropin, and β-endorphin from the HPA-axis. 56 Acute high stress hormone levels can exert an immunosuppressive effect on Th1 cells while mediating differentiation of T-helper cells to Th2 cells. 56,59 -61 Th2 cells proceed to induce immunoglobulin class switching from IgM to IgE. 59 -61 IgE antibodies then bind to mast cells and induce degranulation of lipid mediators, chemical and protein mediators, and pro-inflammatory cytokines (TNF-α, TGF-β, IL-1-4, IL-8-13 etc.) resulting in eczematous skin lesions. 59 -61 Previous studies have found that anxiety was positively correlated with serum IgE and IL-4 levels and negatively correlated with Th1/Th2 ratio in AD patients. 61,62 Of interest, individuals with depression also share a similar cytokine profile with AD patients (Table 2). 63
Anxiety and stress may also worsen AD through the serotonergic system. Rasul et al. found higher levels of serotonin 5-hydroxytryptamine (HT) 1A receptor and serotonin transporter protein (SERT) expression in skin lesions of AD patients, while higher 5-HT2A expression was observed in non-lesional skin. 64 Investigators found that stimulation of 5-HT1A activates monocytes and inhibits their apoptosis. 65,66 In skin, serotonin is involved in inflammation, immunomodulation, vasodilation and pruritus. 67 -69 For example, serotonin may promote secretion of pro-inflammatory cytokine, IL-16, recruit and activate T cells, and activate TRPV receptors. 67 -70 Serum levels of serotonin in AD patients have been shown to adversely correlate with depression scores, and its dysregulated levels are well known to facilitate the pathogenesis of several psychiatric disorders, including anxiety and depression. 64,67,71
There is further evidence for stress-induced neurogenic inflammation in AD. AD patients may have high serum levels of nerve growth factor, SP, neurotrophin-4, and brain-derived neurotrophic factor (BDNF), all of which have roles in neuronal survival, inflammation, pruritus and psychiatric disorders (Table 3). 9,72 Affected skin can display a high density of SP- and CGRP-positive nerve fibers that have increased contact with mast cells under stress exposure. 9,73 A mouse model demonstrated that mental stress can worsen AD through SP-dependent neurogenic inflammation and local Th2 related cytokines. 9 Clinical studies have confirmed that the amount of SP detected in AD patients’ serum is correlated with disease severity, suggesting neuropeptides released from nociceptors in skin lesions promote itching and scratching. 73 Additionally, investigators propose that SP may serve as a biomarker and therapeutic target for depression and anxiety disorders. 74,75 In animal models, its administration can elicit depressive and anxious behaviors. 74,75 Elevated levels of SP have also been observed in individuals with MDD compared to healthy controls, and levels subsequently drop after they receive treatment for depression. 74
Neurotropic Factors, Neuropeptides and Enzymes Implicated in Neurogenic Inflammation of Atopic Dermatitis
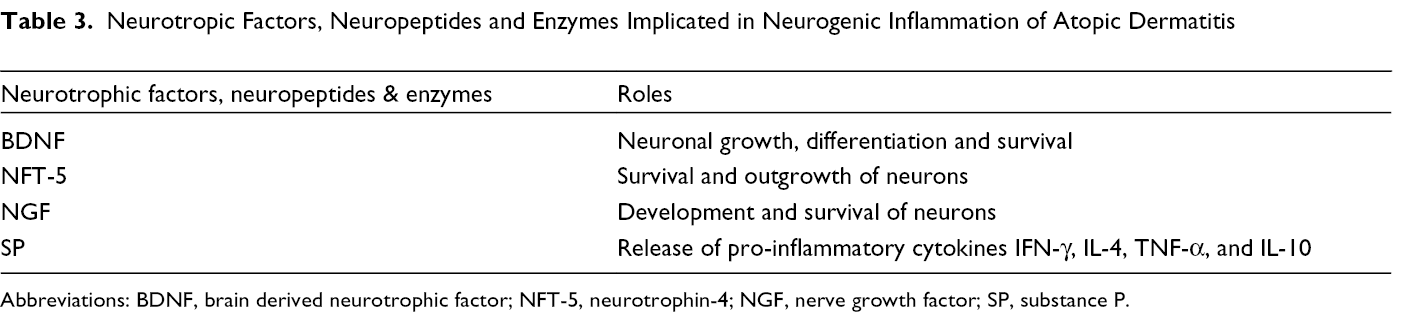
Abbreviations: BDNF, brain derived neurotrophic factor; NFT-5, neurotrophin-4; NGF, nerve growth factor; SP, substance P.
Finally, high BDNF levels in AD patients have been correlated with disease activity, potentially due to its immunomodulatory effects including chemotaxis, inhibition of eosinophil apoptosis, and localization of eosinophils to sensory nerve fibers. 76,77 Yeom et al. reported that anxious and depressive-like behavior in AD mice was associated with increased BDNF striatal levels and activation in the reward circuitry. 72,78,78
Behavioral and pharmacological interventions
Supplementing dermatological treatment with psychotherapy, such as CBT, can improve both skin and mental health in patients. 59,79 -81 However, compliance with therapy limit this benefit because some AD patients may lack the motivation to continue with treatment. 81 For chronic anxiety and depression, low to moderate (10 to 50mg depending on the specific medication) doses of tricyclic antidepressants and selective serotonin reuptake inhibitors (SSRI) are a safe and effective option, although they take several weeks to take effect. 57,79,82,83 Li et al. found that administration of fluoxetine ameliorated both cutaneous and anxiety and depressive-like behavior in an AD mouse model. 84 Tetracyclic antidepressants, such as mirtazapine, are not only reported to reduce psychological symptoms at low to moderate doses (15 to 45mg), but also to improve sleep and pruritus at low doses (7.5 to 30mg). 58,85 -88
In AD, dupilumab, has been shown to reduce symptoms of anxiety and depression as early as 2 weeks through inhibition of pro-inflammatory cytokines (IL-4, IL-12) and IgE. 89 Tralokinumab (anti IL-13) has been linked to overall QoL improvement in AD patients due to its proposed anti-pruritic, anti-depressant, anti-anxiety, and sedative effects. 90,91 While no study has demonstrated any anti-depressant or anti-anxiety effects of JAK-inhibitors on AD patients, these small molecules have been shown to improve anxious-depressive behavior in animals and can improve the mental health of patients living with chronic illnesses, such as rheumatoid arthritis. 92,93
In future, pharmacologic interference of SP-mediated neurogenic inflammation may be a promising alternative therapeutic target utilizing the NK-1 receptor antagonist BIIF 1139 Cl. 9 Clinical studies reported NK-1 receptor antagonists reduced pruritus in AD patients, while animal studies observed a decrease in IgE levels and density of SP-positive nerve fibers in skin lesions. 9,94 NK-1 receptor antagonists have been demonstrated to reduce anxiety and depression in both animal models and patients with MDD and moderately high anxiety levels. 95,96
Gaps in knowledge and future research
Research on biologics and small molecule medications, for example, tralokinumab, should continue to determine if they can not only improve the skin and psychological symptoms associated with AD but as well reduce anxiety and depression in those who do not have skin disease. Further study of anxiolytic and antidepressant mechanisms underlying NK-1 receptor antagonism is encouraged. Several bidirectional theories suggest psychological distress can induce AD, while cutaneous AD symptomatology can induce mental illness through cytokines and neurotrophic factors. Why this occurs in some AD patients and not others is unclear. Longitudinal animal studies are not available and may be the next suggested step.
Psoriasis
Psychiatric co-morbidities
There is a high prevalence of depression, anxiety, suicidality, and sleep disorders in psoriatic patients. 97 -99 A strong correlation exists between the level of stress and disease severity. 100 Psoriasis can be a debilitating and stigmatizing condition that often leads to social isolation and adversely impacts sleep and work. 101
Pathophysiological mechanism of the skin-brain axis
External stress stimuli can induce keratinocytes to produce several pro-inflammatory cytokines, for example, TNF-α, IFN-γ, IL-1β and IL-6. 102 The activation of inflammatory dendritic cells (DC) and their subsequent release of pro-inflammatory cytokines is largely considered a major contributing factor in the pathogenesis of psoriasis. 102,103 Elevated levels of pro-inflammatory cytokines (IL-1, IL-6, TNF-α, etc.) in psoriatic patients is analogous to the profile seen in people with depression who do not have other systemic inflammatory diseases (Table 2). 104,105
Moreover, DCs produce high levels of IL-23, which activates Th17 cells. 102,104 In turn, Th17 cells produce high levels of IL-17A and other cytokines, which have direct effects on keratinocytes. 102 -104 A feed-forward inflammatory cycle is established whereby T cells are perpetually being activated. 102 -104 IL-17 and other cytokines are subsequently released into systemic circulation causing further inflammatory responses in perfused tissues. 102,103 Paralleling peripheral effects, IL-17 has been implicated in neuronal cell death and neuronal toxicity. 106 Among psoriasis patients with elevated levels of IL-17A, an increased risk for anxiety and depression disorders has also been reported. 106
There has been further evidence of increased expression of MMP genes in human psoriatic lesions and human keratinocytes cultured with IL-17. 107,108 Specifically, elevated levels of MMP-9 and pro-MMP-1 levels were observed in patients’ serum, and MMP-3 was further correlated with cytokines IL-4, IL-17A, TNF-α in psoriatic patients. 107,109,110
In addition, the HPA axis may be implicated in psoriasis. 104 CRH has been shown to be involved in a number of cutaneous roles including stimulation of IL-6 and IL-11 production and activation of pro-inflammatory complex protein of NF-kβ, ultimately priming keratinocytes for a pro-inflammatory state. 104 Skin biopsies of psoriatic patients show higher CRH levels compared to healthy skin. 104 As well, IL-1, IL-6, TNF-α, and IFN-α all increase central levels of CRH, adrenocorticotropic hormone (ACTH) and cortisol, and downregulate negative feedback on this stress response by decreasing expression of glucocorticoid receptors. 104 A hyperactive HPA-axis can then promote negative mood symptoms. 104
There is copious evidence for the involvement of gamma-aminobutyric acid (GABA) in the pathogenesis of most psychiatric disorders, such as schizophrenia, bipolar disorder and MDD. 111 More recently, its cutaneous role in psoriasis is being highlighted. Matiushenko et al. reported GABA levels are decreased among psoriatic patients in the acute stage with concurrent psychological disorders. 112 Conversely, Nigam et al. observed an increased number of GABA-positive inflammatory cells and increased GABA-A receptor activity in psoriatic individuals’ skin, which positively correlated with pruritus. 113 Investigators speculate GABA may modulate the activity of immune cells and regulate cytokine release, such as IL-2 and TNF-α. 113,114
Furthermore, the serotonergic system may play a role in the development of psoriasis in addition to AD. Investigators report that psoriatic patients tend to have elevated serum levels of serotonin and higher SERT expression in their lesions. 67,112,115 Higher SERT-positive DCs in lesions also positively correlate with psoriatic severity. 115
Behavioural and pharmacological interventions
There are many options available to treat the psychological symptoms of psoriasis. Escitalopram, an SSRI, combined with psychotherapy showed greater reduction in depression, anxiety, pruritus and Psoriasis Area Severity Index (PASI) scores compared to psychotherapy only in psoriatic patients. 116 However, other psychotropic medications, fluoxetine, bupropion, and lithium, can exacerbate psoriasis.The exact reasons remain unclear and other studies have not found this association. 117,118 Generally, there is evidence that antidepressants, such as SSRIs, tricyclic antidepressants and serotonin norepinephrine reuptake inhibitors, can reduce the risk of psoriasis in patients with MDD. 118 Of interest, mindfulness meditation has been demonstrated to significantly improve psoriasis but without a reduction in stress levels. 119 Another study demonstrated that CBT significantly reduced anxiety, depression, and PASI scores: 64% of psoriasis patients achieved PASI 75 at a 6-months compared to 23% in controls. 120
Moreover, TNF-α antagonists, anti-IL-12/23 antibodies (ustekinumab), and anti-IL-17 antibodies (brodalumab and ixekizumab) were shown to reduce both the severity of psoriasis and depressive symptoms. 4,101,106,109,121,122 A boxed warning regarding the risk of suicidal ideation and behavior was previously issued for brodalumab; however, a subsequent meta-analysis did not find any significant association. 123 Cutaneous disease and depression, particularly seasonal depression disorder, can be managed with phototherapy. 124 -126 Psoriasis is often treated with ultraviolet (UV)-B or psoralen plus UV-A therapy, whereas bright light therapy is used for depression. 124,125 The therapeutic benefit of phototherapy in psoriasis is largely attributed to its anti-inflammatory effects. 125 This is also part of the proposed mechanism for its effectiveness in depression, along with increasing vitamin D levels and stimulating the production of serotonin. 124,126 However, the exact mechanisms through which light therapy improves mood remain unclear, and further research is warranted. 124,126 Additionally, the impact of UV therapy on depression in patients with psoriasis is variable, with some studies reporting a positive effect on mood, while others finding no significant effect or even an exacerbation of depression. 127,128 Finally, a case report found treatment with gabapentin and pregabalin improved an individual’s psoriasis; however, larger studies have not been conducted. 129
Gaps in knowledge and future research
Tzeng et al. have suggested antidepressants could be used as a preventative measure for MDD patients against the development of psoriasis. 118 Further research is necessary to confirm this and to investigate the effect of these medications on established psoriasis. Questions remain as to whether biologics could be used to treat depression in patients who do not have psoriasis. As phototherapy alone seems to offer no benefit on co-existing anxiety and depression, this highlights the complexity of underlying skin-brain pathophysiology. Emphasis on integration of a more holistic treatment approach for psoriasis may be especially necessary. Further pre-clinical study is required to understand the order of events, and the role that inflammation plays in the co-occurrence of psychiatric conditions.
The Interrelationship Between Psychotherapy and the Neuroimmune System
Psychosocial interventions can reduce both psychological and dermatologic symptoms across the four conditions discussed in this review. While the exact mechanism remains unclear, a recent systematic review found a significant correlation between psychotherapy and an improved immune function. 130 Psychotherapy has been shown to consistently reduce pro-inflammatory cytokine levels and increase immune cell counts. 130 These associations were most consistent for CBT and multiple combined psychotherapies. 130
In addition, psychotherapy has been shown to reduce 5-HT1B and increase 5-HT1A receptor binding effect in patients with MDD, indicating that serotonin modulation may be a contributing factor in the therapeutic effect. 131,132 Linz et al. observed that there was no difference in BDNF levels after participants completed a 3 month mindfulness-based mental training program. 133 Similarly, Sanacora et al. reported that CBT did not affect cortical GABA concentrations in depressed individuals. 134 However, most psychotherapy research has centered on the effects of cortisol levels. For example, mindfulness-based art therapy, mindfulness meditation and CBT all reportedly reduce cortisol levels. 135 -140 These effects were only observed in individuals who experienced significant improvement in their cognitive and affective symptoms of depression. 141 In particular, females who do not respond well to CBT have significantly higher cortisol and ACTH basal plasma concentrations, which investigators suggest may serve as a predictor of psychotherapy outcome. 142 Despite the growing body of evidence, research of the effects of psychotherapy on the NICS system is still distinctly nascent.
Limitations
This review has several limitations including limited scope, lack of data synthesis and analysis, and lack of quality appraisal of evidence. Only four dermatological conditions were included to highlight the inter-dependence of the mind and skin, although many others exist (Figure 1). Studies generally included have small sample sizes, inconsistent psychiatric evaluation, and heterogeneous inflammatory markers and timepoints. Additionally, exploration of the gut-brain-skin axis was outside the scope of this review. The breadth and depth of the literature was managed using a carefully designed search strategy and librarian consultation.
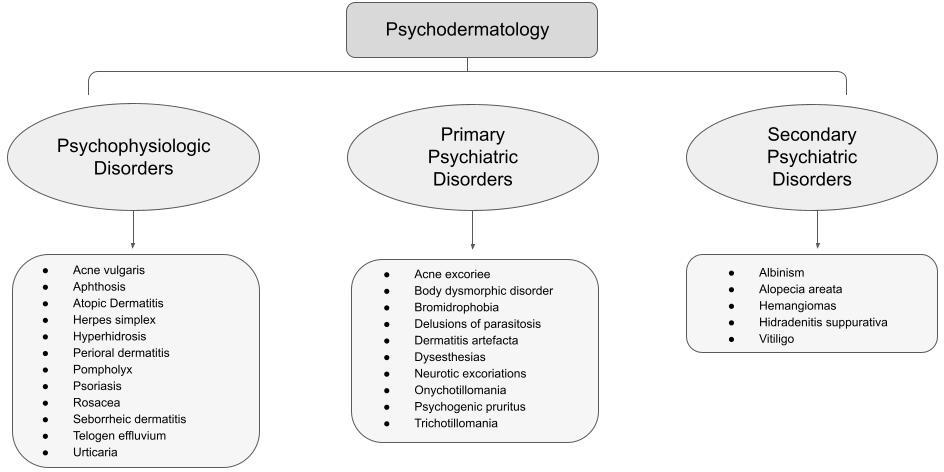
Psychodermatology disorders. psoriasis, trichotillomania and vitiligo are just a few examples of common psychodermatologic conditions. This list is not exhaustive.
Conclusion
The psychological distress caused by rosacea, AV, AD, and psoriasis are well known to clinicians. Common co-morbidities include anxiety disorders, mood disorders, sleep disorders, and suicidal thoughts and attempts. Although the stigmatization of mental illness has decreased, barriers remain for patients to access mental health services, and many individuals are reluctant to seek treatment. 143 A combined treatment approach that addresses both the psychological and cutaneous disease state would be welcomed by patients. Clinical management may gradually evolve from a purely dermatological lens to one that is more multi-disciplinary in approach. Development of a standard psychiatric screening tool relevant to psychodermatologic conditions is necessary. Dermatologists may then easily and rapidly administer screening questionnaires for certain patients. Evidence of shared pathomechanisms between the skin and brain present dual targetable therapeutic opportunities. Further coordinated care through the use of psychotherapy and psycho-pharmacologic agents may provide an additional benefit in the management of cutaneous diseases. In future, and in a complementary fashion, drugs used in cutaneous disease may also prove of benefit for the management of primary psychiatric states.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Neither honoraria nor other form of payment was made for authorship.