
Abstract
Intravascular B-Cell Lymphoma (IVBCL) is a rare type of extranodal large B-cell lymphoma where clonal B-cells selectively home to and replicate in the lumen of small vessels. Random skin biopsy (RSB) of uninvolved skin is a reputable tool to diagnose this protean entity and thus dermatologists are involved in its diagnosis. A literature review was completed to derive an approach to RSB in these patients to maximize diagnostic yield of IVBCL and minimize morbidity. Based on this review, data from 27 patients where clinical signs and symptoms and results of investigations were able to be linked to a positive diagnosis of IVBCL from RSB from 11 papers from 2003 to 2021 were analyzed. Following this analysis, RSB should be considered when there are no clinical skin findings and there is an elevated lactate dehydrogenase in the absence of lymphadenopathy and presence of fever of unknown origin, thrombocytopenia, anemia, and ferritinemia. Three to four RSBs from the thigh, abdomen and/or posterior upper arm should be performed via either incisional or telescoping punch biopsies and should include senile/cherry angioma(s) if present. If RSB results in a diagnosis of IVBCL, hematology should be consulted for further management. Consideration of a false negative biopsy or alternative diagnoses should be explored if RSB is negative for IVBCL. Following a standard approach for RSB in these patients will increase diagnostic yield of IVBCL while decreasing the risk of harm to the patient.
Keywords
Introduction
First described in 1959 1 intravascular B-Cell Lymphoma (IVBCL) is a rare type of extranodal large B-cell lymphoma characterized by the selective growth of clonal B-cells in the lumen of the small vessels of various organs including the liver, spleen, lungs, brain, kidney, and skin in the absence of lymphadenopathy. It is an aggressive, rapidly fatal neoplasm with protean signs and symptoms, causing it to appear on a myriad of differential diagnosis and making it a challenge to diagnose. The incidence is less than 1 case in 1 million per year worldwide 2 with a median age of onset of 70 years 3 .
There are two sub-types: a classical (or Western) variant and an Asian (or Eastern) variant. 4 The Western variant manifests more often with neurological and dermatological changes 5 including morbilliform eruptions, plaques, nodules, hyperpigmented areas, telangiectasias, palpable purpura, ulcers and infiltrative peau d’orange changes. 6 The Eastern variant is usually accompanied by hemophagocytic lymphohistiocytosis and typically does not have skin involvement. 4 Exceptions to this separation have been noted in case reports 7 and case series. 8
When the diagnosis is suspected, various areas may be targeted for a biopsy including the brain, lung, bone marrow and skin, with or without signs of cutaneous disease. 2,4,5,9,10 Over the last 20 years, there have been studies 3,11 -26 noting the utility of random skin biopsy (RSB) in the diagnosis of IVBCL with many of these touting the relatively minimally invasive nature of RSB. As a result of the sensitivity (77.8%), specificity (98.7%) and positive and negative predictive values (96.6% and 90.6%, respectively) put forth by Matsue et al 3 and the ease of cutaneous biopsy, dermatologists have become part of the care team responsible for the diagnosis of IVBCL. Several studies have put forth clinical and biochemical criteria 3,15,22 which may aid in patient selection for RSB when IVBCL is a consideration, however there is currently no approach in the literature which defines when to perform RSB in these patients, which method of RSB provides the highest sensitivity and specificity while minimizing morbidity and what steps to take following RSB. To address this, a literature review was conducted to derive an approach to RSB in patients where IVBCL is a consideration with the aim of preventing unnecessary RSB and a technique which may provide the best opportunity of diagnosing IVBCL in patients with the disease.
Methods
A comprehensive literature review was performed. PubMed and Google Scholar were searched with keywords and terms including normal appearing skin, random skin biopsy, blind skin biopsy combined with intravascular lymphoma and intravascular B-cell lymphoma. For this review RSB means taking a skin biopsy from normal appearing skin. One author searched for articles and subsequently reviewed them to ascertain their relevance. Titles and abstracts were screened, and the following were excluded: non-English abstracts, articles where IVBCL was diagnosed by using methods other than RSB, duplicates, conference proceedings or if the publication was inaccessible (i.e., could not be obtained through interlibrary loans or was not available online). Reference lists were reviewed to retrieve additional articles and to ensure available data were adequately collected. Patients from the literature review were only included in the analysis of demographics, signs and symptoms and investigations if it could be ascertained whether that patient had a diagnosis of IVBCL made from RSB of normal appearing skin. Papers where patients were used as part of a patient group in subsequent papers were also eliminated from our analysis. Patient data from Arai et al, 27 Asada et al, 28 Matsue et al, 18,29 and Yamada et al 24 were excluded from our analysis for these reasons.
Results and Discussion
Papers Included and Demographics
Based on the data generated from these papers, presented in Tables 1 and 2, and discussed more in-depth below, Figure 1 gives an overview of a proposed approach of when and how to perform RSBs in patients suspected of having IVBCL and steps to take following RSB results. Patients from 11 papers from 2003 to 2021 were included in the analysis of clinical and laboratory characteristics of patients diagnosed with IVBCL via RSB and are summarized in Table 1. 11,15,17,19,21,22,26,30 -33 Overall, 27 patients, 19 men and 8 women, had a positive diagnosis of IVBCL from RSBs and had an average age of 65.3 (48, 83) years. Four of the 11 studies took place outside of Asia, two in the United States of America, one in Argentina and one in Australia comprising one Asian, one white and two patients of unknown ethnicity (T1 in Supplemental Material). Of the remaining 23 patients, 2 were Japanese and 21 were of unknown ethnicity with 11 and 10 patients enrolled in Japan and Thailand, respectively. Table 2 summarizes the number of RSBs needed to diagnose IVBCL. Data were generated from a subset of 9 of the 11 papers discussed above, comprising 24 patients, where the number of RSBs completed on each patient and the number of these RSBs that were positive were reported. 17,19,21,22,26,30 -33
Signs, Symptoms, and Investigations in Patients Who Have a Random Skin Biopsy From Normal Skin Positive for Intravascular B-Cell Lymphoma (IVBCL). Values Indicate Presence of Sign, Symptom, or Investigation Result Over Total Number of Patients in Each Study.
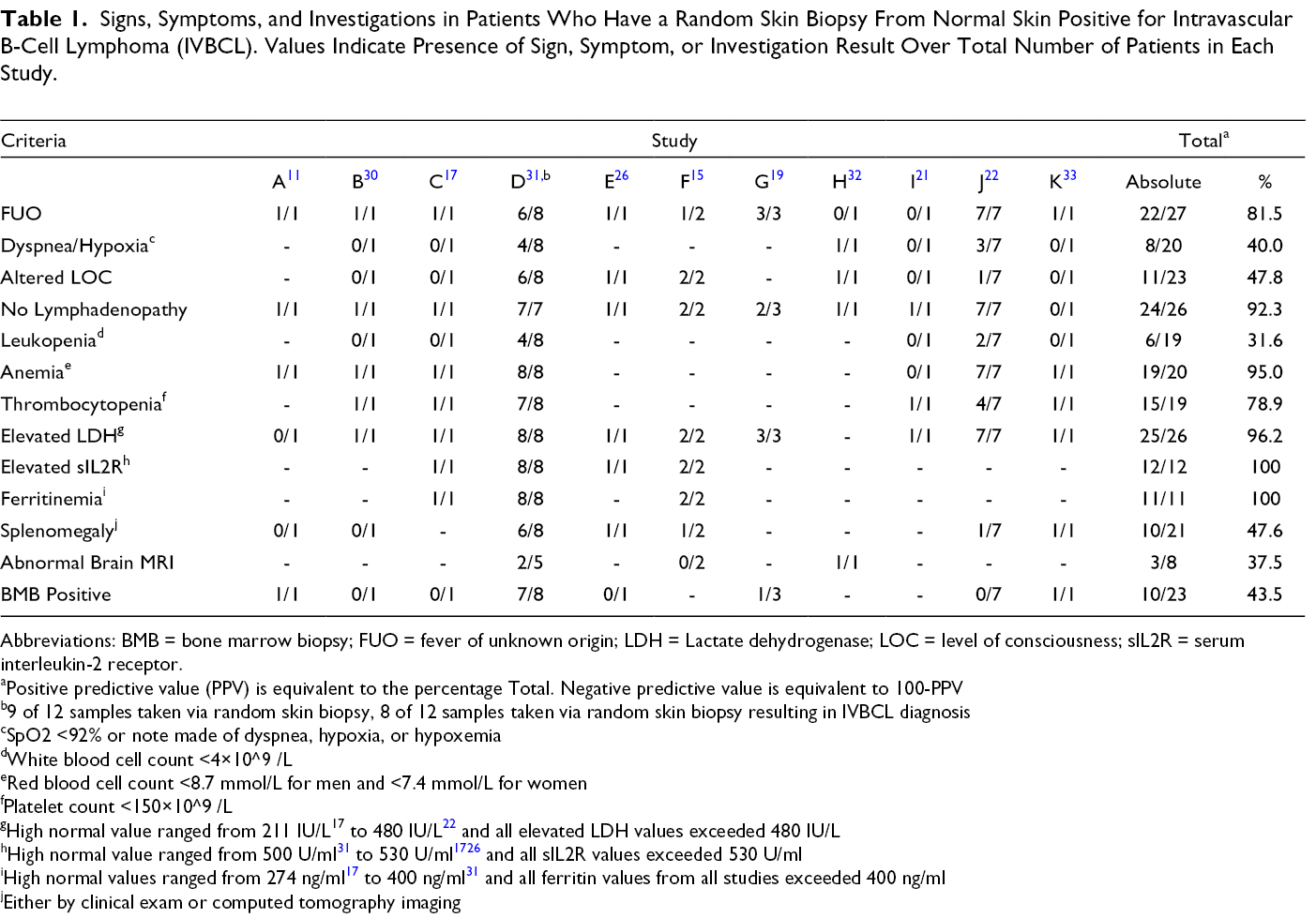
Abbreviations: BMB = bone marrow biopsy; FUO = fever of unknown origin; LDH = Lactate dehydrogenase; LOC = level of consciousness; sIL2R = serum interleukin-2 receptor.
aPositive predictive value (PPV) is equivalent to the percentage Total. Negative predictive value is equivalent to 100-PPV
b9 of 12 samples taken via random skin biopsy, 8 of 12 samples taken via random skin biopsy resulting in IVBCL diagnosis
cSpO2 <92% or note made of dyspnea, hypoxia, or hypoxemia
dWhite blood cell count <4×10^9 /L
eRed blood cell count <8.7 mmol/L for men and <7.4 mmol/L for women
fPlatelet count <150×10^9 /L
gHigh normal value ranged from 211 IU/L17 to 480 IU/L 22 and all elevated LDH values exceeded 480 IU/L
iHigh normal values ranged from 274 ng/ml 17 to 400 ng/ml 31 and all ferritin values from all studies exceeded 400 ng/ml
jEither by clinical exam or computed tomography imaging
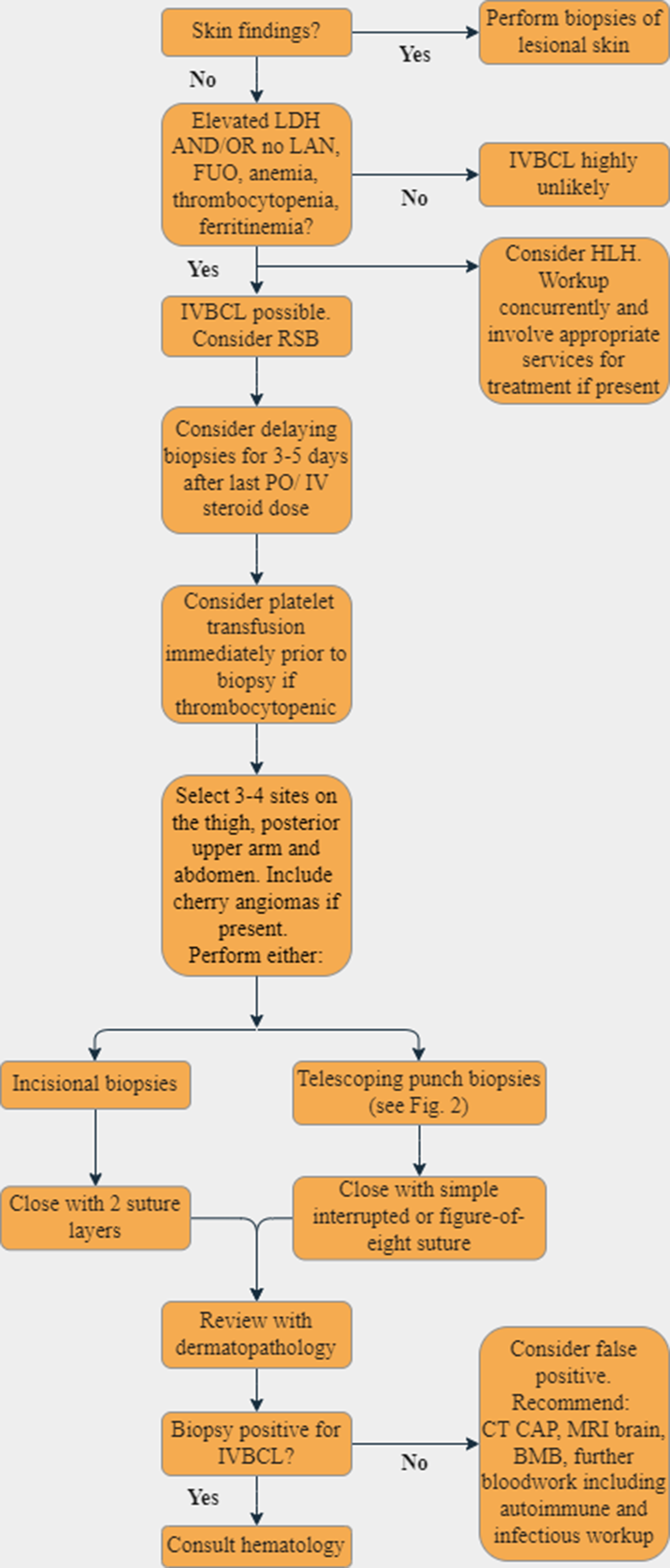
Approach to random skin biopsy in patients where intravascular B-cell lymphoma (IVBCL) is a consideration. BMB = bone marrow biopsy, CT CAP = CT chest, abdomen, pelvis, FUO = fever of unknown origin, LAN = lymphadenopathy, LDH = lactate dehydrogenase.
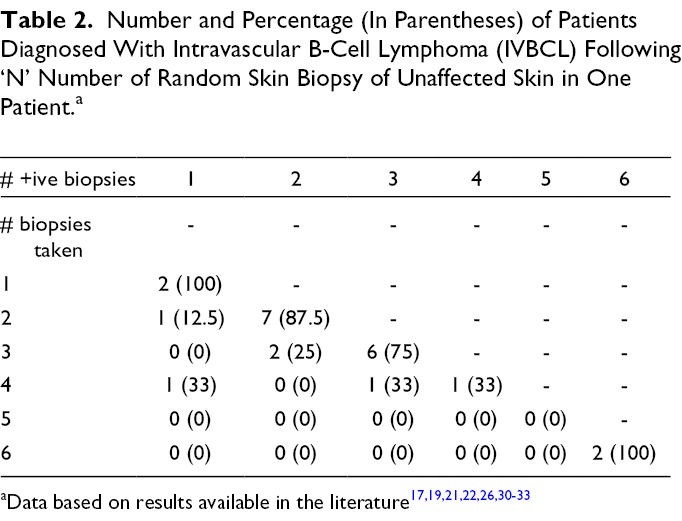
Number and Percentage (In Parentheses) of Patients Diagnosed With Intravascular B-Cell Lymphoma (IVBCL) Following ‘N’ Number of Random Skin Biopsy of Unaffected Skin in One Patient. a
To Biopsy or Not Biopsy?
The incidence of skin lesions in IVBCL approaches 40%, especially in the Western variant and the lesions can vary in morphology including morbilliform eruptions, purpura, telangiectatic macules and subcutaneous nodules. 2 If there is a suspicion of IVBCL and skin lesions are present, they should be biopsied in lieu of RSBs. If there are no skin lesions and IVBCL is a consideration, several studies have put forth criteria which may help in patient selection. Higashi et al 15 recommended to perform RSBs in patients suspected of having IVBCL with various nonspecific central nervous system manifestations, hematocytopenias, elevated levels of lactate dehydrogenase (LDH) and no lymphadenopathy. Sitthinamsuwan et al contend RSB is a reliable method of diagnosing IVBCL in patients without lymphadenopathy, hepatosplenomegaly, or bone marrow abnormality with fever of unknown origin (FUO) and any of the following: hematologic abnormalities with or without unusual neurologic symptoms, elevated LDH, and/or hypoxemia. In addition to patients having FUO and hypoxia, Matsue et al 3 further defined elevated levels of LDH to be most closely associated with a positive diagnosis of IVBCL when greater than 800 U/L. Like these studies, based on data aggregated in Table 1 from literature review, prior to performing RSB on a patient suspected of having IVBCL, determining whether a patient has an elevated serum LDH, ferritinemia, anemia, and no lymphadenopathy is key as these features occurred in 96.2% (25/26), 100% (11/11), 95.0% (19/20), and 92.3% (24/26) of patients in our analysis, respectively. If none of these characteristics are present, especially elevated serum LDH as it is more specific than other features listed above for a hematologic malignancy, then RSB has almost no yield for detection of IVBCL as there is likely another diagnosis. FUO and thrombocytopenia occurred less frequently, 81.5% (22/27) and 78.9% (15/19), in patients in our analysis than is suggested in the literature. Nevertheless, these patient characteristics should still be assessed prior to performing a RSB. Further, elevated beta-2 microglobulin 9,20,21 and hypoalbuminemia 18 have also been shown to be present in patients with IVBCL, but were only captured for patients in two 21,30 and one 33 paper(s), respectively (T1 in Supplemental Material). Occurring in less than 50% of patients with IVBCL diagnosed via RSB in our analysis is dyspnea or hypoxia, altered level of consciousness, leukopenia, splenomegaly, abnormal brain MRI and a positive bone marrow biopsy (BMB, Table 1). Other patient characteristics captured in only a small subset of patients and seeming to have no bearing on a whether a patient with IVBCL would have a positive RSB are C-reactive protein, erythrocyte sedimentation rate, fibrinogen, and triglycerides (T1 in Supplemental Material). Though Higashi et al 15 and Matsue et al 3 recommend performing RSB in patients with an elevated sIL2R and it was noted in 100% of patients (12/12) in four studies we reviewed, 15,17,26,31 it is an not available at many hospital laboratories and may be elevated in a number of other conditions like infections, autoimmune and other inflammatory diseases and hemophagocytic lymphohistiocytosis. 34 Therefore, we have not included it as part of our decision tree (Figure 1). If a center does have access to sIL2R testing, then it could be considered as a biochemical feature of a patient who may have IVBCL and RSB could be considered if the patient has no skin lesions and no lymphadenopathy. It should be noted that many clinical and biochemical features of IVBCL also overlap with HLH and consideration should be given to the latter diagnosis when approaching a patient where IVBCL is a possibility due to HLH potentially being rapidly fatal.
Biopsy Method
No standard biopsy method exists in the literature. Consideration of biopsy delay should occur if the patient was treated with oral or intravenous steroids in the previous three 3 to five 24 days as it increases the risk of false negatives. 3,24 IVBCL lesions in RSB are most consistently present in small vessels in the subcutaneous fat 12 -14 . RSB does carry an inherent risk of bleeding, especially in this patient population where thrombocytopenia is common and in one case report 25 incisional biopsy (6 in total completed) may have contributed to hemorrhagic shock and death of a patient due to blood loss. This patient was profoundly thrombocytopenic (2.3 × 104 /L) with no note made of pre-procedure coagulopathy correction. Another study of 25 patients with 82 incisional biopsies noted no post-procedure hemorrhagic complications, but recommended coagulopathy correction, if necessary, based on local guidelines. 14 In 114 incisional RSB specimens from 111 patients in Matsue et al, 3 the sensitivity, specificity and positive and negative predictive values were 77.8%, 98.7%, 96.6% and 90.6%, respectively.
Some authors have questioned the diagnostic utility of using a superficial 4 mm punch biopsy for RSB to consistently diagnose IVBCL 10,12 -14 citing that these 4 mm punch biopsies sample the superficial 4-5mm of skin and do not sample a deep enough section of subcutaneous fat 10 where the diagnosis of IVBCL via RSB is more consistently made. 13,14 Some authors have championed incisional biopsy down to the fascial plane noting 37% of IVBCL lesions were present only if the subcutaneous tissue had a minimum depth of 5 mm from the skin surface to the lesion. 14 Long axis and width of the incisional biopsy with positive diagnosis of IVBCL has ranged from 1 cm x 0.5 cm 15 , 19 to 2 cm x 0.5 to 1 cm 25 .
Winge et al. recommend telescoping punch biopsies (Figure 2) with 6 mm and then 4 mm punches to obtain adequate subcutaneous tissue, followed by suturing using a figure of 8 closure. 23 This publication was a Clinical Image with no accompanying data on sensitivity and specificity, however did manage to achieve 12.8 mm depth of biopsy, likely conferring similar diagnostic yield to incisional biopsy as biopsy depth is comparable. 13,14 Others have noted telescoping punch biopsies may increase the risk of unintended prolonged post-procedure bleeding. 13
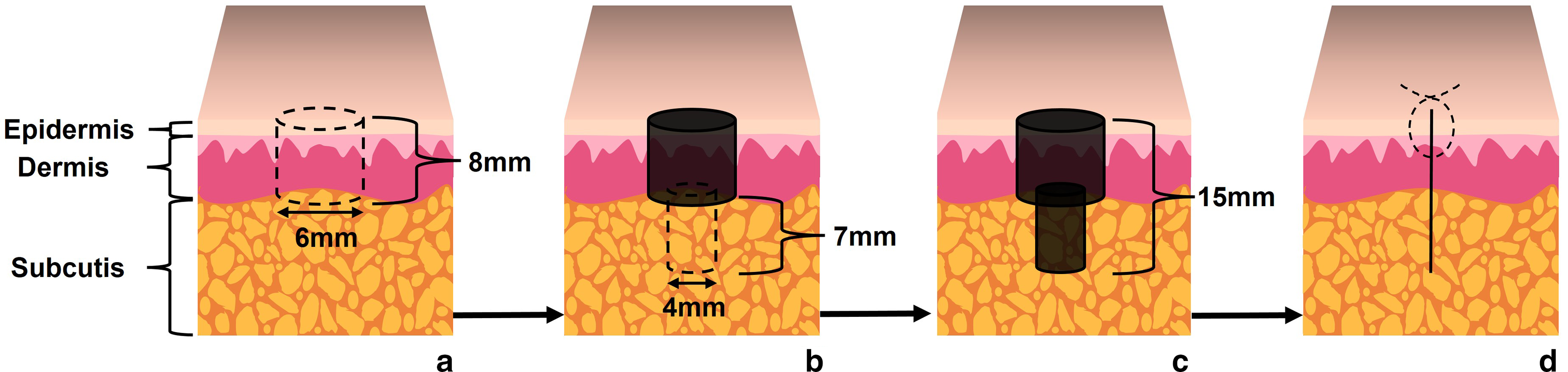
Illustration of telescoping punch biopsy. A. First, a 6 mm punch biopsy is performed (dotted cylinder), which confers 8 mm depth into tissue. B. Second, a 4 mm punch biopsy (dotted cylinder) is completed subjacent to the 6 mm punch biopsy (black cylinder) and allows for an additional 7 mm depth to be achieved. C. The entire telescoping punch gives 15 mm depth for the completed biopsy (black cylinders). D. The defect is then closed with interrupted (dotted lines) or figure-of-eight sutures.
Site selection of RSB is also an important consideration. Owing to the depth of the biopsy needed for consistent diagnosis of IVBCL, the thigh, abdomen, and posterior upper arm are suitable sites for biopsy 3,14,22,23,25 with some studies opting to perform RSB on all three sites. 17,21 A number of case reports have noted IVBCL colonizing senile/cherry angiomas. 20,35 -37 Therefore, if these lesions are noted on the thigh, abdomen, or posterior upper arm, they should be incorporated into the RSB biopsy.
Number of RSB Samples
The optimum number of RSB samples needed to increase diagnostic sensitivity and minimize morbidity has not been determined. Most studies have opted for one 17,21 to six 26,31 with recommendations on the number of RSBs to complete ranging between 1 to 3 33 , 2, 22 3 15 and at least 3. 19 Based on Table 2, data would suggest diagnosis of IVBCL via RSB in a patient suspected of having IVBCL requires anywhere between 1 and 6 RSBs. A RSB was positive for IVBCL in all patients regardless of how many RSBs were taken in 78.2% of cases and a patient who was diagnosed with IVBCL via RSB had one RSB negative for IVBCL no matter how many RSBs were taken in 17.4% of cases. In one patient 4 RSBs were taken and resulted in only one sample yielding a diagnosis of IVBCL (Table 2). 31 If only 3 RSBs were taken in this patient, the diagnosis of IVBCL may have been missed. Therefore, though sample sizes in our analysis are likely too small and the techniques used between studies too varied in the literature to draw concrete conclusions, data in Table 2 would suggest needing at least 3 RSBs per patient in most cases and 4 RSBs in some cases to maximize sensitivity. More study is needed, in particular using incisional or telescoping punch biopsies to reach layers of subcutaneous fat more likely yield a diagnosis of IVBCL, to increase the sensitivity of detecting IVBCL via RSB when the disease is present while minimizing patient morbidity by not taking more RSBs than needed to make the diagnosis of IVBCL. Finally, all cases where RSB has been performed should be reviewed with a dermatopathologist to ensure appropriate staining and deeper levels are cut, if necessary, to increase the diagnostic yield of RSB in a patient who has IVBCL.
Finishing the Consult
If RSB yields a diagnosis of IVBCL, hematology, if not already consulted, should become part of the patient’s circle of care. In cases where a diagnosis of IVBCL has not been made via RSB, thought should be given to the potential of a false negative RSB, particularly if the patient had been treated with oral or intravenous steroids within three 3 to five 24 days prior to biopsy. In addition, further investigations should be considered as the patient may have IVBCL that is not yet present in the skin. A number of cases exist in the literature where RSB was negative and the patient was diagnosed with IVBCL through the biopsy of another organ and if not already completed, a CT scan of the chest, abdomen and pelvis and MRI brain should be considered as IVBCL can present in organs of the thorax and abdomen and in the central nervous system. 2,4,5,9,10 In certain cases a PET CT may be considered. Further, though a random skin biopsy from normal-appearing skin is more sensitive than a BMB for the diagnosis of intravascular lymphoma as evidence would suggest in this analysis (Table 1) and the literature, 27 several studies have demonstrated BMB as diagnosing IVBCL when RSB was negative. 3,29,31 Shimada and Kiyoi recommend work-up by both RSB and BMB if IVBCL is suspected. 38
Another diagnosis may also be responsible for the patient’s presentation. Review of studies where RSB did not yield a diagnosis of IVBCL revealed numerous other neoplastic, auto-immune, and infectious etiologies of a patient’s symptomatology including various other types of lymphoma, acute disseminated encephalomyelitis, Schnitzler syndrome, adult-onset Still’s disease, neuro-Behcet disease, sarcoidosis, graft-versus-host disease, POEMS syndrome, systemic lupus erythematosus, polyarteritis nodosa, bacterial infection and tuberculosis. 15,18 -20,22 Investigations for such etiologies should be the responsibility of the patient’s home or other consult services, particularly if the patient has no cutaneous findings.
Limitations
The number of patients where clinical data and data from investigations for individual patients where IVBCL was diagnosed from RSB were low with 27 patients identified from 11 studies. In addition, the majority of patients, 88.9%, in this review had either Asian ethnicity or the study was conducted in Asia with unknown ethnicity. These patients likely had the ‘Eastern’ variant of IVBCL where absence of skin disease is more common than in the ‘Western’ variant, though there are exceptions to these phenotypic correlations. 7,8 Thus, for patients without Asian ethnicity or when IVBCL is suspected in a patient outside of Asia, RSBs may not be needed as the patient has an increased likelihood of having clinical cutaneous manifestations of IVBCL and the proposed approach (Figure 1) would have less utility. Further, data collected for this review were not generated at the same lab and the papers analyzed spanned almost 20 years. This presents the possibility of differences in measurement of biochemical and radiographic parameters in patients in different studies. However, by determining the presence or absence of a patient sign, symptom, or abnormal finding on investigation from each study rather than applying the same criteria across all patients from all studies, this was hopefully mitigated.
Conclusion
When there is suspicion of IVBCL and the patient has no skin findings, RSB should be performed if certain clinical characteristics and biochemical perturbations are present like an elevated serum LDH with or without FUO, no lymphadenopathy, thrombocytopenia, anemia, and ferritinemia. Following a standard approach for RSB in these patients, like the one proposed here, should increase diagnostic yield while decreasing the risk of harm to the patient. In addition, a standard approach may allow for better comparison of which signs and symptoms and investigation abnormalities are present in patients with IVBCL without signs of skin lesions. Further study of the optimal number of RSB for the diagnosis of IVBCL is required to prevent unnecessary skin biopsies, yet ensure IVBCL is diagnosed, if present. In addition, there is a future need to compare the sensitivity and specificity of elliptical excision versus telescoping punch biopsy contrasted against the relative morbidity of each so an even more standard approach to RSB in patients where IVBCL is a consideration can be achieved.
Supplemental Material
Supplementary Material 1 - Supplemental material for Recommendations for an Approach to Random Skin Biopsy in the Diagnosis of Intravascular B-Cell Lymphoma
Supplemental material, Supplementary Material 1, for Recommendations for an Approach to Random Skin Biopsy in the Diagnosis of Intravascular B-Cell Lymphoma by Michael L. MacGillivary and Kerri S. Purdy in Journal of Cutaneous Medicine and Surgery
Footnotes
Acknowledgements
Statistical support from Ms. Kara Matheson is greatly appreciated.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.