
Abstract
Introduction
Hidradenitis Suppurativa (HS) is a chronic inflammatory disordercommonly affecting body folds. It can significantly impair quality of life due to the physical, psychological, and socialturmoil experienced by patients. Treatment remains a challenge.Limited data on the HS patient experience, such as self-treatment exists.
Methods
This was a single-center cross-sectional study, utilizing a paper-based survey. Surveys were mailed out to all HS patients from the dermatology clinic and completed on a voluntary basis. Demographics, disease characteristics, medical and family history, treatments tried, and life quality were documented.
Results
The response rate was 49.4% (41/83), with a female predominance (26/41). Eighty-five percent (35/41) were Caucasian with an average age and BMI of 39.0 ± 16.78 and 30.71 ± 7.02, respectively. In total, 24.4% (10/41), 56.0% (23/41), and 19.5% (8/41) had Hurley I, II, and III, respectively. Lesions affected the genital region (75.6%), thigh/groin (68.2%), and axilla (46.3). Almost half (49%) of patients experienced an average of 1-2 flares per month. The most bothersome symptoms were pain (92.7%), discharge (68.3%), malodor (63.4%), and itch (61%). Depression (53.7%), severe facial acne (14.6%), and hypertension (14.6%) were the most common co-morbidities. Treatments used included antibiotics (82.9%) and surgical excision (34.2%) were. Over 90% of patients reportedself-treatment of lesions by squeezing (80.5%), soaking (53.7%), and lancing (41.4%).
Conclusions
This study provides insight into the patient perspective of HS. We identify itch as a symptom that is not frequently associated with HS and reveal how commonly patients utilize various types of self-treatment in their experience of disease.
Introduction
Hidradenitis Suppurativa (HS) is a chronic, relapsing inflammatory skin condition characterized by painful cutaneous nodules and abscesses in the body folds, which may result in sinus tracts and scaring. 1 In the Western world, HS has a prevalence of 0.05% to 4%, with the incidence continuing to increase. 2 Associations with female sex, obesity, smoking, and family history have been previously described. 3
The painful and recurrent nature with subsequent disfigurement can be highly distressing to patients. The average onset of disease has been described to be in the second decade, 4 affecting young adults during a vulnerable transition period of life. Pain has been consistently reported as one of the most distressing symptoms of HS, with the majority of patients rating their pain as a 4-10 out of 10 on the Numerical Rating Scale-11. 5 Malodorous discharge is another bothersome symptom that is associated with decreased quality of life (QoL), as it causes stained clothing and contributes to social isolation and failed relationships. 6,7 In addition to physical factors, impacts on psychological and emotional wellbeing further contribute to the disease burden in HS patients. Higher levels of loneliness, alexithyma, andemotional fragility have been linked to patients with HS. 8 -10 When compared to psoriasis, HS patients have significantly lower QoL and higher levels of anxiety and depression. 11
Furthermore, due to its chronic relapsing/remitting course and potential for severe scarring, treatment remains a challenge to both dermatologists and surgeons. Current evidence supports antibiotic treatment with combinations of clindamycin, rifampicin, and tetracyclines. 12,13 Biologic anti–tumour necrosis factor (TNF) therapies such as Adalimumab and Infliximab have also been shown to be effective. 12,13 In addition to medical management, surgical techniques and carbon dioxide laser treatments are available; however, data on the outcomes of these approaches are more limited. 12 While elaborate treatment algorithms have been proposed, a significant portion of HS patients continue to be poorly controlled as demonstrated by the high frequency ofemergency department visits and inpatient hospital admissions. 14 It was found that HS patients utilize these high cost resources more often than patients with psoriasis or other chronic cutaneous inflammatory diseases. 14,15
Despite the significant disease burden and established negative effects on QoL, there is limited data on the patient experience of HS. We conducted a survey-based cross sectional study to better understand the patient perspective of disease. These data will compliment our current knowledge of HS and can serve as a guide for physicians to better counsel HS patients and optimize their management.
Methods
Study Design
This was a single-center cross-sectional study, utilizing a paper-based survey containing the Dermatology Life Quality Index (DLQI). Ethics compliance was received from the Queen’s University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board.
Participants
All patients with a diagnosis of HS from the Kingston General Hospital Dermatology Clinic during the years 2015 to 2017 were identified and received a paper copy of the survey. A letter of information and a consent form were included in the survey package. Participation was voluntary and patients had the option of receiving a monetary reward to partake in the study. Patients that signed the consent form and mailed the survey back to the primary investigator were included. Incomplete surveys were excluded.
Survey
The survey comprised 43 questions in addition to the Dermatology Life Quality Index (DLQI). It was sent to participants through the Canada Post mail service and inquired about patient demographics (gender, ethnicity, age, body mass index), disease characteristics (Hurley score, DLQI, age of symptom onset, years from symptoms to diagnosis, most bothersome symptoms, number of flares, lesion location), treatments used, past medical history and comorbidities, family history, and smoking history (Supplemental Appendix 1).
Outcome Measures
The primary outcome measures were focused on the patient experience of disease including most bothersome symptoms, comorbidities, disease management, duration of flares, and the overall QoL as depicted by the DLQI.
Statistical Analysis
Data collected from the surveys were compiled into a centralized database designed specifically for the study using Microsoft Excel. The data were summarized in table format using descriptive analysis (means, standard deviations, ranges). Categorical variables were reported as frequencies and relative frequencies. Continuous variables were reported as means and standard deviations.
Results
There were 83 patients identified with HS from the dermatology clinic that received the survey. Of these, there was a response rate of 49.4% (41/83), with a majority of female respondents (26/41). Eighty-five percent (35/41) of responders were Caucasian with an average age and BMI of 39.0 ± 16.78 (15-85) and 30.71 ± 7.02 (18.2, 50.6), respectively. There was a positive family history of HS and personal smoking history in 24.4% (10/41) and 53.7% (22/41) of patients, respectively (Table 1).
Patient Demographics.
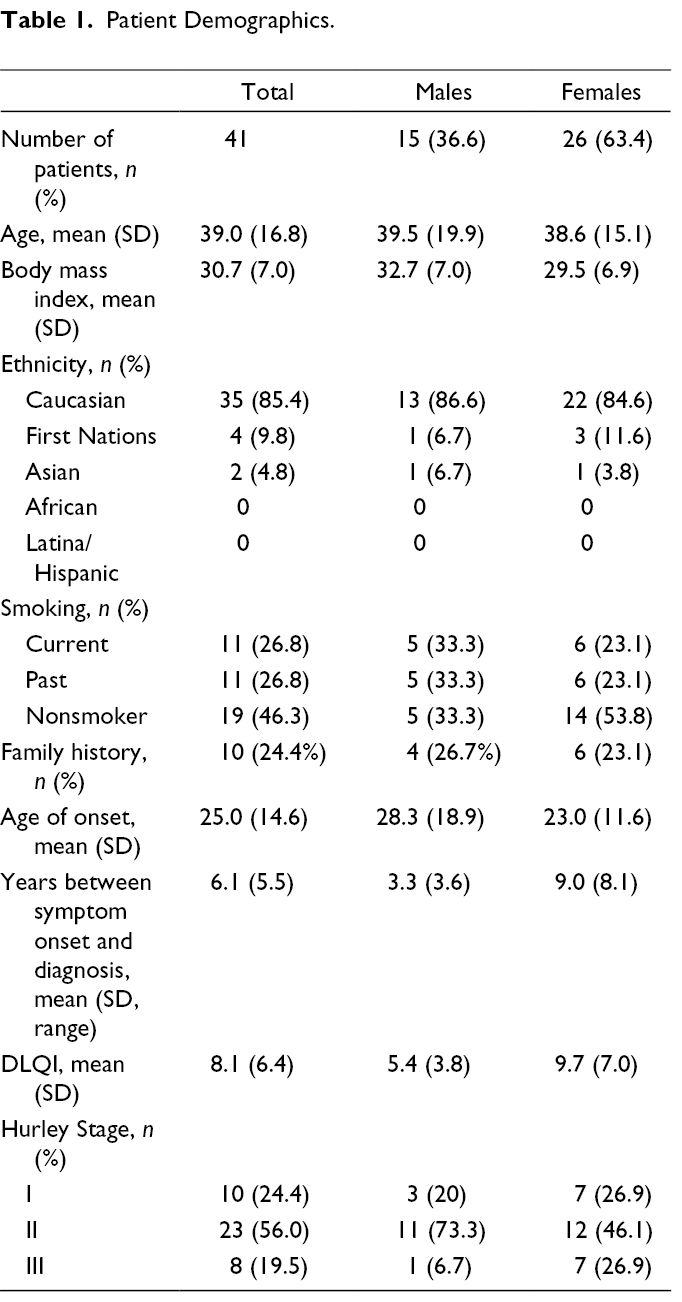
In total, 24.4% (10/41) of patients demonstrated Hurley I, while 56.0% (23/41) and 19.5% (8/41) had Hurley II and III, respectively. The average age of symptom onset was 25.0 ± 14.6 (10, 83) years and the average time between symptom onset and diagnosis was 6.1 ± 5.5 (0, 39) years. Females experienced an earlier disease onset (23.0, 28.3 years, P = .27) and a longer time period between symptom onset and diagnosis (9.0, 3.3 years, P = .01). The average DLQI of all patients was 8.15 ± 6.35, with statistically higher scores in females (9.7, 5.4, P = .03) (Table 1).
HS lesions were mainly affecting the genital/gluteal region (75.6%), thigh/groin (68.2%), axilla (46.3%), and inframammary region (36.6%) (shown in Figure 1a). Close to half (49%) of patients experienced an average of 1-2 flares per month (range: 0-6 per month) (shown in Figure 1b). The most bothersome symptoms reported by patients included pain (92.7%), discharge (68.3%), malodor (63.4%), and itch (61%). Swelling and fever were reported in less than 10% patients (shown in Figure 1c). Depression (53.7%), severe facial acne (14.6%), hypertension (14.6%), and inflammatory bowel disease 9.8% (4/41) were the most common co-morbidities reported bypatients. Other co-morbidities included diabetes, dyslipidemia, polycystic ovarian syndrome, arthritis, and eczema. (shown in Figure 2).
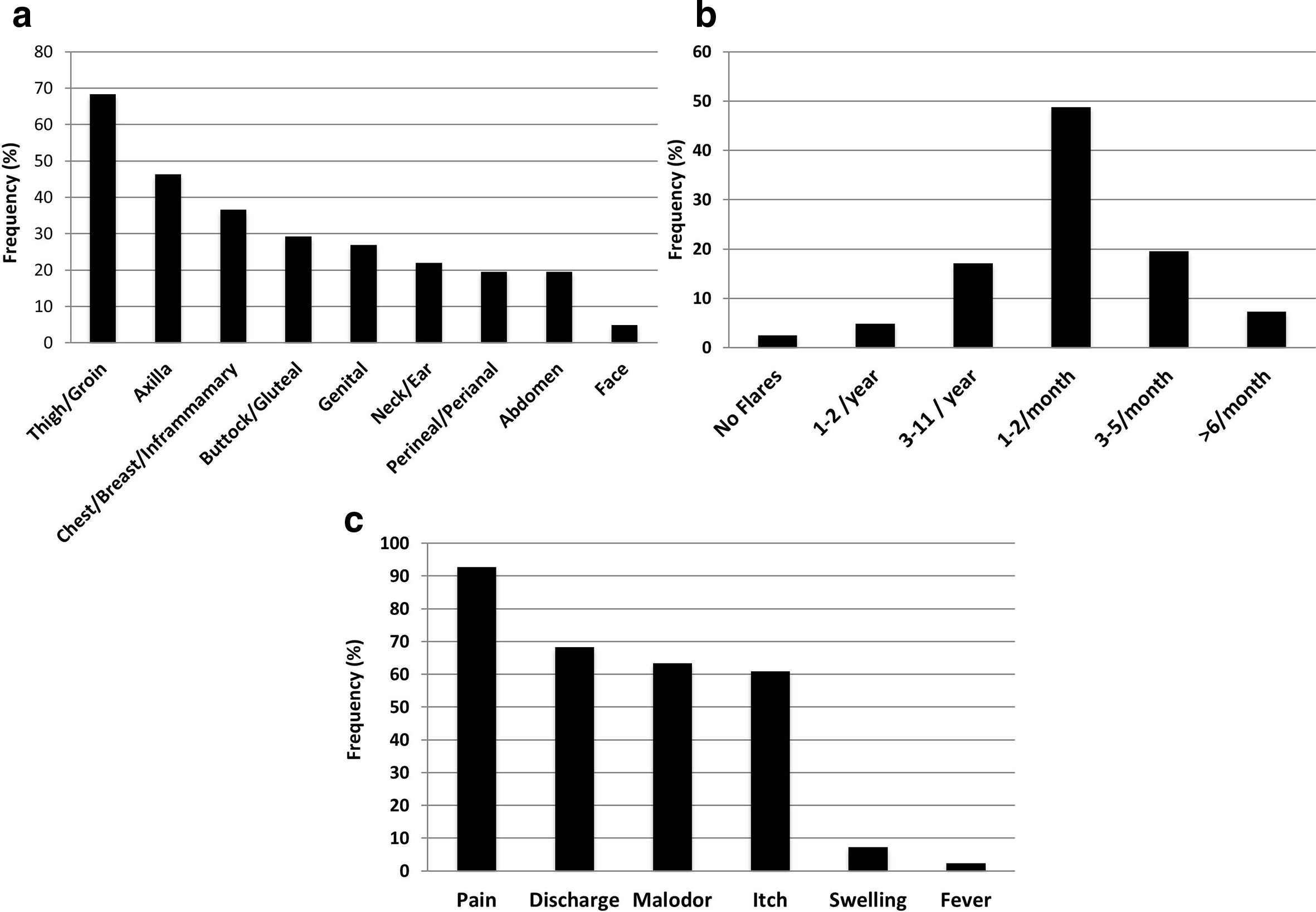
Details of HS disease burden. (
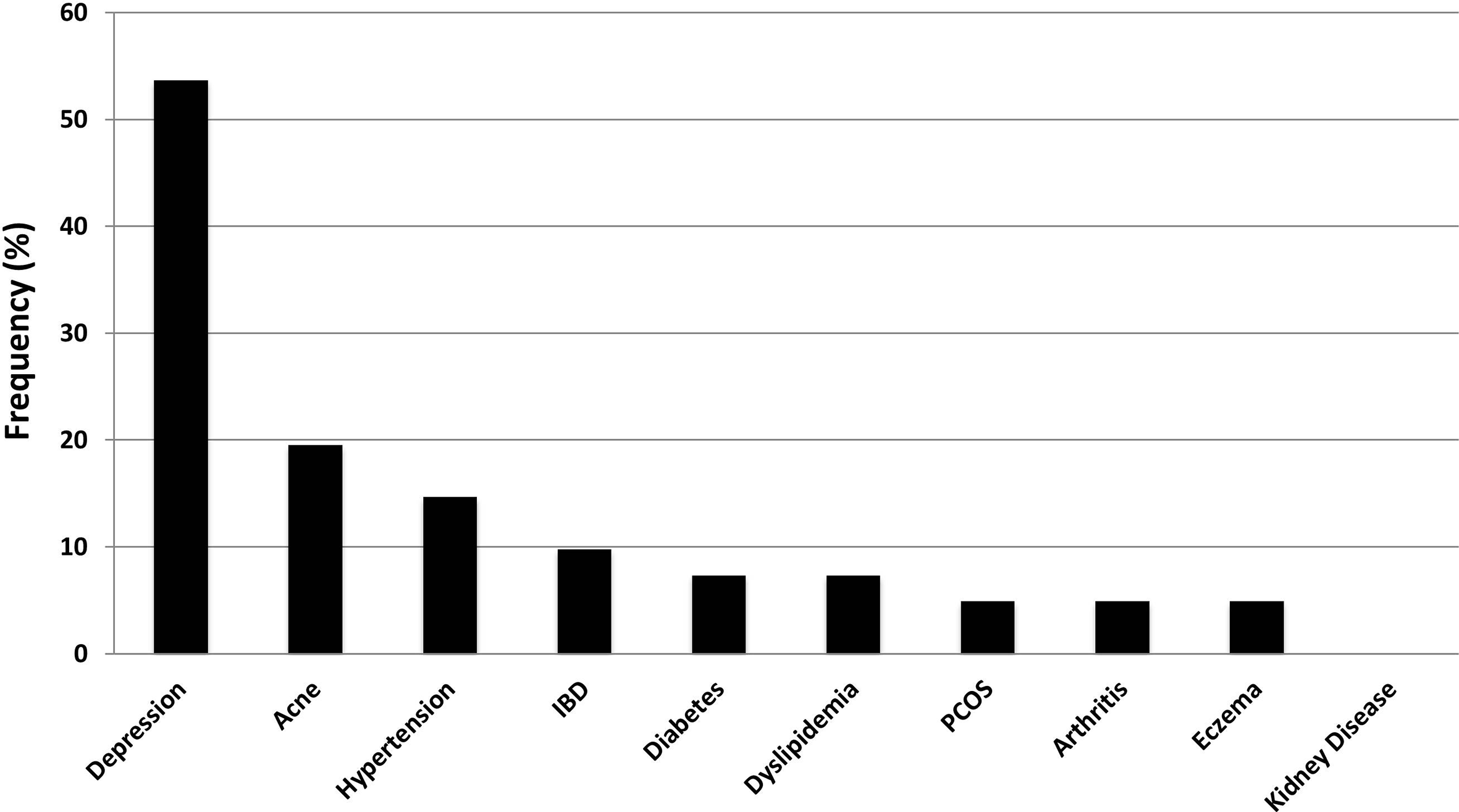
Frequency of co-morbidities reported in HS patients.
There were 63.5% (26/41) of patients on multiple treatment modalities.Antibiotics were the most common (82.9%), followed by surgical excision (34.2%). Systemic steroids and retinoids were used by 24.4% (10/41) and 9.8% (4/41), respectively. Anti-TNF biologics werea treatment modality for 4.9% (2/41) of patients and lasers wereused by 2.4% (1/41) (seen in Figure 3a). In addition to prescribed treatments, over 90% of patients reported self-manipulation or treatment of their lesions. There were 80.5% (33/41) that squeezed, 53.7% (22/41) that soaked, 41.4% (17/41) that lanced, 29.3% (12/41) that used ice compression,14.6% (6/41) that used herbal remedies, and 9.8% (4/41) used warm compressions for their lesions (seen in Figure 3b).
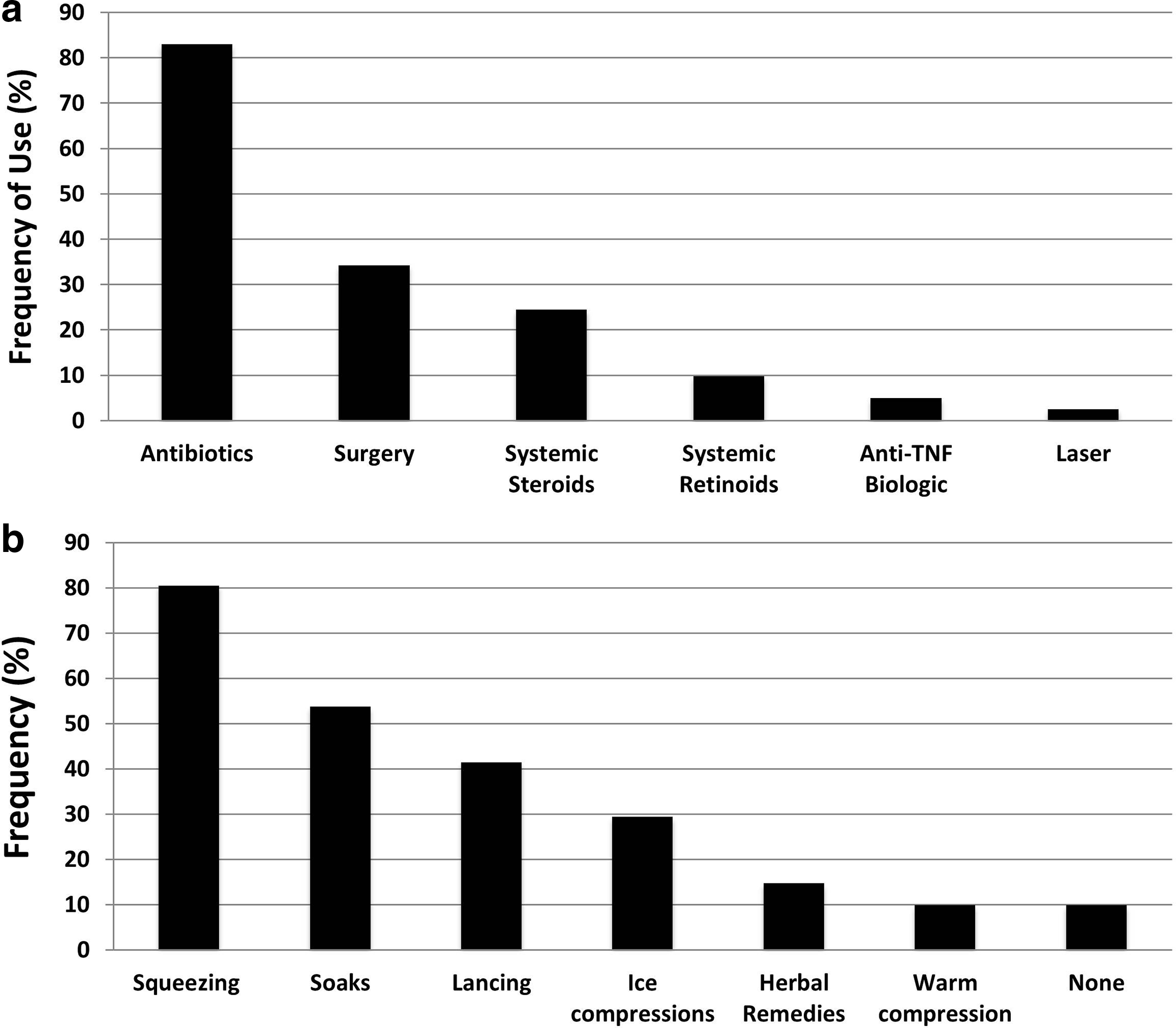
Treatment for HS. (
Discussion
While the understanding of disease factors and treatments for HS is continuously evolving, there is limitedliterature focusing on the patient experience of disease. By considering patient factors that may not be clearly evident during the HS assessment, physicians can provide better patient care. The present studyoffers valuable insightsinto how patients experience and treat their disease, which can guide physicians to optimize their management of HS patients.
The first important finding from our study was that pain was the most bothersome symptom (92.7%), followed by discharge (68.3%), malodor (63.4%), and itch (61%). Pain has been well established as one of the most debilitating and unbearable aspects of HS. 16 In a large cross sectional study, pain in HS was been found to be worse than psoriasis, skin tumors, eczema, and acne. 17 A recent review characterized HS-related pain into acute and chronic, both of which can be present concurrently. 18 While acute pain presents with neuropathic burning, stinging, shooting, and stabbing sensations, chronic pain is more stimulus-dependent, characterized by gnawing, aching, tenderness, and throbbing. 18 Due to the multifactorial components of HS pain, a biopsychosocial approach has been widely accepted.
A malodorous discharge has also been frequently reported as a common symptom of HS. As nodules evolve, abscesses form which will break through the skin causing sinuses and a malodorous purulent or seropurulent discharge. The malodorous discharge and staining of clothing is a source of embarrassment, low self-esteem, social stigma, and a barrier to interpersonal relationships in these patients. 19,20 A Canadian study also reported that the severity of odor from lesions predicts the Skindexscore, another measure of QoL. 21
Lastly, itch is a problematic but relatively under-studied symptom of HS. In our cohort, 61% of patients reported pruritus, slightly higher than an incidence of 57.3% found in a previous cross-sectional study. 22 Pruritus appears to be moderate to severe in intensity, and was found to be associated with increased body regions affected by HS, female sex, the intensity of suppuration, and the presence of comorbid Crohn’s disease. 23 Furthermore, pruritus has been implicated as an important player in insomnia and decreased sleep quality in HS patients, 24 which may further contribute to decreased QoL. Recognizing the most bothersome symptoms for patients and how they contribute to QoL is key to optimizing patient care and satisfaction.
The next major finding was the comorbidities reported by patients. As HS is a chronic and incapacitating skin disease, it is important for clinicians to be well informed on concurrent diseases that may impact the patient. Depression was reported by over half of our patients. This was an alarming result given past studies showing a prevalence of 16.9% to 26.6% 25 -27 in HS patients. Two recent systematic reviews/meta-analyses both demonstrated higher odds of depression in HS patients as compared to the general population with odds ratios of 2.54 and 1.84, respectively. 25,27 Furthermore, a large-scale study utilizing the Danish National Registries revealed that HS patients had an increased risk of completed suicides and suicidal behavior, after adjusting for confounding factors. 28 When compared to psoriasis, HS patients had a 2-fold greater risk of suicide. 29 Considering the evidence for the prevalence and severity of depression in HS patients, it is not surprising that HS has also been shown to be associated with higher levels of anti-depressant use. 27,28 Of note, other psychiatric conditions such as anxiety, bipolar disorder, psychosis, schizophrenia, and alexithymia have also been shown to be higher in HS patients than healthy counterparts. 9,25 -27 Given the high rates of psychiatric comorbidity seen in HS patients, early recognition and referral to psychiatry specialists have been recommended. However, with fast paced dermatology clinics, efficient strategies for psychological screening are still warranted. In addition to psychiatric issues, dermatologists may also have a role in screening for other skin and systemic-related comorbidities associated with HS. 30
Lastly, our study reports the prevalence and techniques of self-treatment of HS lesions. With increasing attention to HS over the last several years, our understanding of treatment approaches continues to grow. Currently, there are over 9 treatment guidelines with overlapping recommendations developed by various expert organizations worldwide. 31 Despite comprehensive treatment algorithms, over 90% of our patients were self-treating their lesions, regardless of Hurley stage. The most common methods were squeezing (80.5%), soaking (53.7%), lancing (41.4%), and icing lesions (29.3%). Self-treatment was mainly used in conjunction with prescribed medical therapy, however 3 of our 41 patients relied on self-treatment as monotherapy. There were 14.6% (6/41) of patients who reported using non-prescribed herbal remedies as self-treatment. Cannabis for mucocutaneous disease has been suggested for acne, psoriasis, dermatitis, kaposi’s sarcoma, pruritus, skin cancer, and systemic sclerosis. 32 Cannabis has also been described to have a role in the treatment of chronic pain. 33 As chronic pain is one of the most significant symptoms in HS, 18 future studies investigating the efficacy of cannabis in HS pain management could be beneficial. To our knowledge, there are currently only a few publications describing self-manipulation/treatment of HS. The common practice of self-treatment in conjunction with the majority of patients experiencing at least 1-2 flares monthlyin our study may suggest that HS patients are undertreated in our cohort. Our result further supports previous studies that demonstrated high amounts of emergency department visits and admissions due to poor control. 14 This highlights the importance of the patient perspective of disease when assessing treatment response and disease control.
Limitations
This study may have some limitations. Firstly, the use of a survey may have introduced recall bias as questions required patients to document experiences and feelings from the past. Additionally, as surveys were anonymous, descriptions of disease involvement rated by the patient could not be validated with a clinical assessment by the dermatologist. However, previous chart reviews completed in the same center demonstrated similar Hurley Stage ranges. While the authors aimed to capture important demographics and disease characteristics, factors such as alcohol/substance abuse were not assessed due to the limited number of questions acceptable in a survey. Secondly, there may have been an element of selection bias due to the use of a paper survey and the monetary reward offered for participation. The inconvenience of mailing surveys back to the investigators may have deterred patients from participating. Meanwhile, offering a reward for participation may have selected for a certain group of patients. Lastly, the single center design within a new dermatology practice limited our sample size. Although this study offers valuable information regarding the patient experience of HS, future studies with larger sample sizes across multiple centers are required to confirm our findings.
Conclusion
Our cross-sectional study provides insight on the patient perspective of HS. The most bothersome symptoms reported were pain, malodorous discharge, and pruritus. Depression was the most prevalent comorbidity and may be more common than reported in previous studies. This highlights the need for effective psychological screening in dermatology clinics and the importance of multidisciplinary care. Lastly, the majority of patients reported self-treatment/manipulationof their lesions for symptom control, regardless of Hurley stage and/or prescribed medical treatments. This finding suggests that patients may be undertreated and reminds physicians that Hurley staging does not represent disease control or patient satisfaction. As HS has significant impacts on QoL, aspects of the patient’s disease experience are essential to consider in providing optimal patient care.
Supplemental Material
Online supplementary file 1 - Supplemental material for Hidradenitis Suppurativa From a Patient Perspective Including Symptoms and Self-Treatment
Supplemental material, Online supplementary file 1, for Hidradenitis Suppurativa From a Patient Perspective Including Symptoms and Self-Treatment by Christina M. Huang and Mark G. Kirchhof in Journal of Cutaneous Medicine and Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mark Kirchhof – Abbvie, Novartis- Speaker, Advisory Board Member, Consultant; Janssen, Leo Pharma, Pfizer, Sanofi-Genzyme, UCB – Speaker, Advisory Board Member; Celgene, Eli Lilly – Advisory Board Member.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.