
Abstract
Nail matricectomy is indicated in the management of painful onychodystrophies, including recalcitrant onychocryptosis, onychogryphosis, onychauxis, and refractory onychomycosis. Although many matricectomy methods have been described, with phenolization being the best studied, no one method has clearly emerged as superior. We present a series of 14 patients who underwent a total of 18 matricectomies with either phenolization or electrodessication (ED) in a private dermatology office, and describe a simple and effective variation of the ED technique using a modified hyfrecator tip. A video demonstration of this technique is included. We also describe ED matricectomy in the context of a review of the literature, ascertaining recurrence rates, complication rates, healing time, and patient satisfaction. The nuances of technique specifics (such as the use of adjunct methods and antibiotics), as well as outcome predictors and measurements have been highlighted. We found ED to be comparable to other forms of matricectomy, with the advantages of ease of use, minimal complications, and good satisfaction rates.
Introduction
Matricectomy is indicated in the management of painful onychodystrophies, including recalcitrant onychocryptosis (most commonly), onychauxis, onychogryphosis, and refractory onychomycosis. 1 Matricectomy refers to the excision or destruction of the nail matrix, with the aim of achieving permanent nail loss. 2 It may be partial or total. 2 Simple onychectomy without matrix destruction has been shown to have a high recurrence rate in cases of onychocryptosis. 3
The use of electrodessication (ED) in matricectomy, first described in 1938, 2 is considered a simple and effective option. 4,5 It is one of the numerous methods of matricectomy, which include surgical excision, chemical ablation (with phenol, sodium hydroxide, or trichloroacetic acid), cryotherapy, carbon dioxide laser, and curettage. 4 While there has been no consensus as to which surgical technique is optimal, healing time as well as recurrence and complication rates are universally important outcomes in nail matricectomy. 4,6
This article examines the use of ED in matricectomy with a case series of 18 procedures comparing ED with a modified hyfrecator tip (Figure 1) to phenolization, as well as a review of the electrosurgery techniques described in the literature.
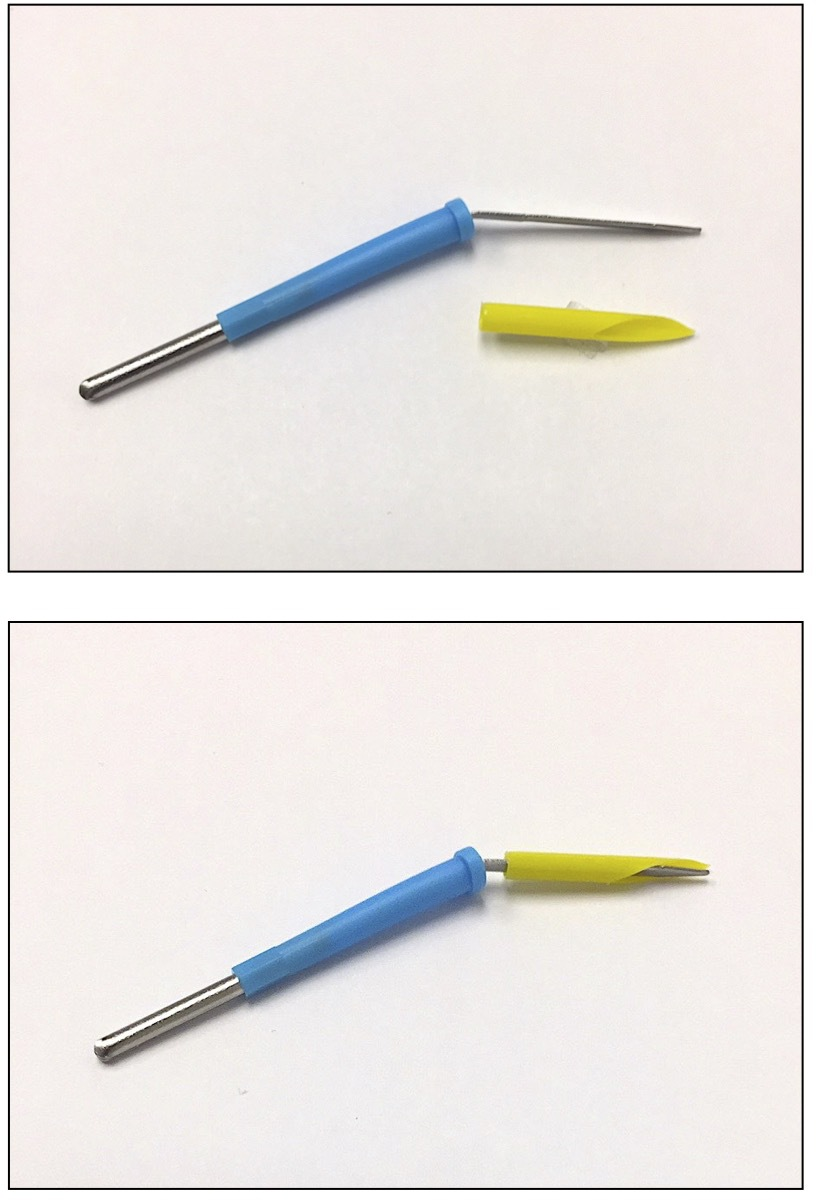
Modified hyfrecator tip.
Case Series Using an ED Technique With a Modified Hyfrecator Tip
A retrospective case series was conducted on 14 patients who underwent a total of 18 matricectomies in a private dermatology office from August 2016 to December 2020 (Supplemental Table S1). Indications included onychocryptosis and onychogryphosis. A total of 16 nails were involved, of which 2 required a repeat procedure due to recurrence (18 procedures total). The procedures were all performed by one dermatologist, were either partial or total, and consisted of curettage followed by either phenolization or ED using a modified hyfrecator tip. Chart review and follow-up phone calls were carried out to ascertain the following outcomes: recurrence rate; infection rate; healing time (return to activities and time to complete healing); and patient satisfaction (4 = very satisfied, 3 = somewhat satisfied, 2 = somewhat unsatisfied, 1 = very unsatisfied). Informed consent was obtained from patients whose identifiable data (including but not limited to video footage) are included in the study.
The ED matricectomy technique employed in the case series featured a modified hyfrecator tip, demonstrated here in a patient who underwent a total matricectomy for painful onychogryphosis (Figure 2 and Video 1 [accessible online at https://journals.sagepub.com/doi/full/10.1177/12034754211024124]). The skin was first cleansed. A distal ring block was performed with 1% lidocaine without epinephrine. A digital tourniquet was applied. The entire nail plate was then elevated, released, and avulsed. The matrix was curetted and then electrodessicated with a Bovie A950 (Aaron, USA) set to 20 in monopolar fulguration mode, with careful attention paid to the lateral matrix horns. Resection of the proximal nail fold to optimize visualization of the nail matrix is sometimes indicated. The plastic covering of the needle was preserved at the tip, cut at an angle such that the dorsal side would be insulated and therefore protect the overlying proximal nail fold. A dressing with petrolatum and tube gauze was applied. Wound care instructions were provided to patients in a handout (see Supplemental Handout) as part of their pre- and post-operative care. Neither antibiotics nor antiseptic treatments were prescribed.
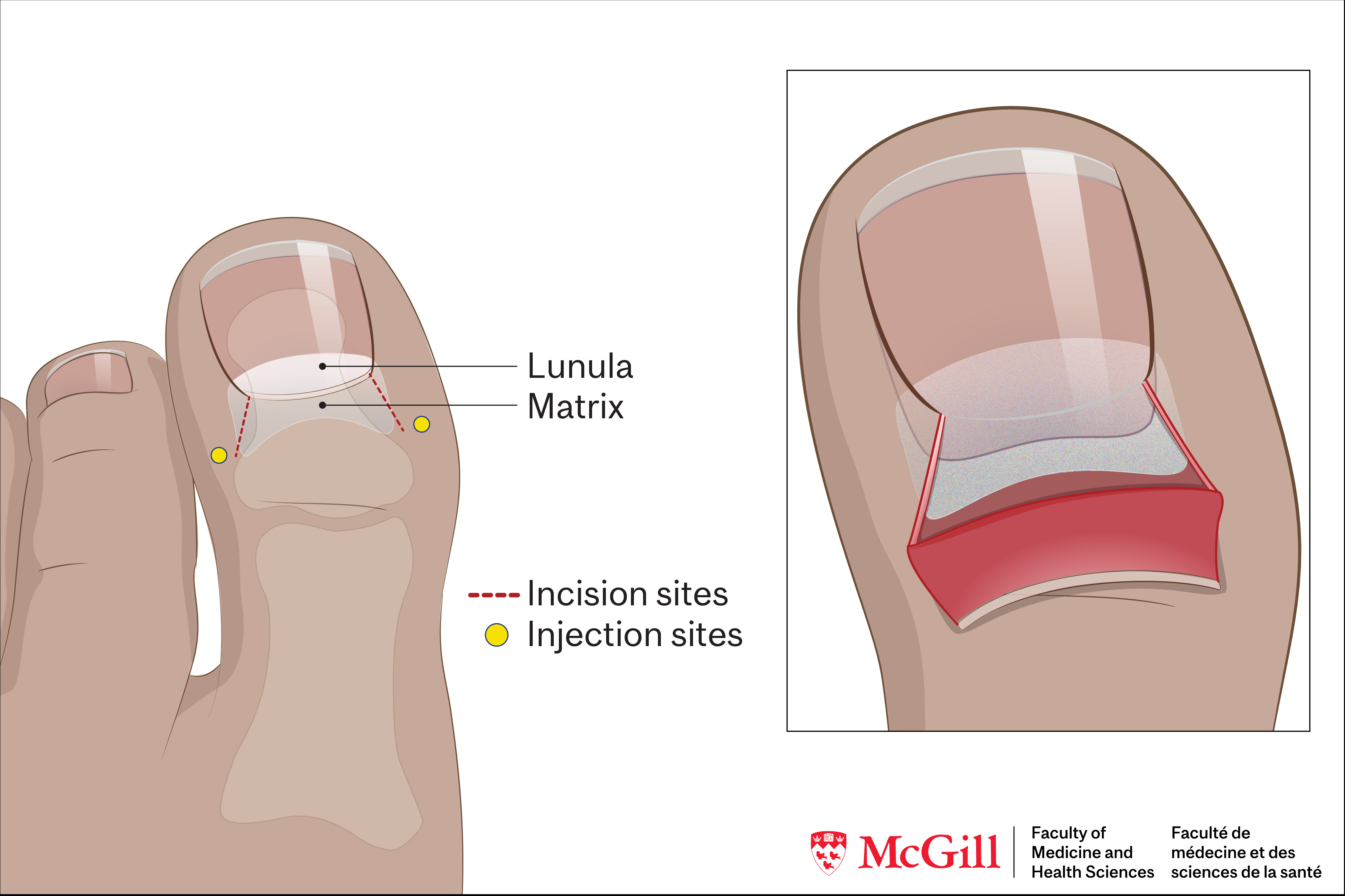
Nail anatomy.
Case Series Using an ED Technique With a Modified Hyfrecator Tip: Results
Following curettage, ED was performed in 9 initial procedures, and phenolization in 7. There was 1 recurrence with each technique. Both recurrences were re-treated with ED, resulting in a total of 11 ED procedures. One patient was lost to follow-up.
Of the 11 ED procedures: recurrence occurred in 1 (9.1%); infection in 1 (9.1%); median time to return to activities was 2.5 weeks in 10 reported outcomes (ranging 2 days to 8 weeks); and median time to complete healing was 4 weeks in 10 reported outcomes (ranging 1 to 16 weeks). Nine of 11 responses (81.8%) regarding satisfaction indicated the patients were “very satisfied” following an ED procedure. The remaining 2 of the 11 procedures (18.2%) yielded outcomes with which the patients were “somewhat unsatisfied,” with one complaint pertaining to the nail’s esthetic appearance.
Of the 7 phenolization procedures: recurrence occurred in 1 of 6 reported outcomes (16.7%); infection in none (0%); median time to return to activities was 3.5 weeks in 6 reported outcomes (ranging 3 to 8 weeks); median time to complete healing in 4 reported outcomes was 7 weeks (ranging 4 to 12 weeks); and 5 out of 5 patients (100%) who reported their level of satisfaction were all “very satisfied.”
Review of the Literature
Searches were conducted across EMBASE, MEDLINE via PubMed, CINAHL, Cochrane, Web of Science, and Scopus in December 2020 using the search terms matrixectomy/matricectomy, matricectomy procedure(s), matricectomy technique(s), electrosurgery, electrocautery, electrodessication, electrofulguration, diathermy, nail bed ablation, nail procedure, and nail surgery. Corresponding subject headings and all possible subheadings were applied where available. Reference lists were also reviewed. Articles were then manually screened for eligibility.
Eleven original articles describing the use of ED in ablative matricectomy were included in the present study, with sample sizes ranging from 1 to 302 patients (averaging 89 per study), and the number of matricectomy procedures performed ranging from 10 to 353 (averaging 90 per study) (Supplemental Table S2). The outcomes of a total of 753 nail matricectomy procedures using ED were ascertained over an average follow-up period of 9.47 months (with an overall range of 3 to 15 months).
Nine of the 11 studies stated onychocryptosis as their primary indication for matricectomy 4,6 -13 but the procedure was also used in the management of onychogryphosis 14 and pachyonychia congenita. 15 Most matricectomy procedures are partial in the management of onychocryptosis. 4,6 -13
Review of the Literature: Technique
ED following nail avulsion has been described as a standalone technique in 4 studies, 6,7,9,11 as an adjunct to curettage in 2 studies, 10,15 and as an adjunct to another form of matrix excision in 4 studies. 4,8,13,14 One study used ED to supplement both matrix excision and curettage. 12
The electrosurgery set-ups described in the literature varied, including: bipolar electrosurgical units set at 50 W 4,14 ; monopolar electrosurgical units on a medium setting 8,10 or at 50 V 6 ; and radiowave output frequency set to 3.8MHz. 12 Total duration of ED was reported to range from 2 seconds up to 60 seconds in partial and total matricectomy. 4,6 -8,10,12,14
Tourniquets are commonly used to provide a dry surgical field, 4,7,8,10,11,13,14 but not always. 12 Excessive granulation tissue is either excised 8,10 or curetted. 6 A curette may be used to remove residual nail fragments and/or the nail matrix. 10,12 Sutures may be used to approximate the nail plate with the external fold of the digit 4,8,9 but are not part of routine practice.
Oral antibiotics were used in a total of 2 studies for pre-operative nail infections 10,12 and prophylactically in a total of 5 studies. 4,7 -9,14 Prophylactic topical antibiotic or antiseptic solutions were used in a total of 6 studies as part of post-operative wound care. 4,6,7,10,13,15 Three studies used more than one form of antibiotic and/or antiseptic treatment, either prophylactically or to treat a pre-existing toe nail infection. 4,7,10 Only 1 study did not use any form of antibiotic or antiseptic treatment. 11 Pain was controlled by over-the-counter analgesics. 4,12,14
Review of the Literature: Results
Recurrence rates a following ED procedures ranged from 0% to 44.8%: 0% in 5 studies 4,7,8,14,15 ; 1% to 5% in 2 studies 12,13 ; 10% to 15% in 2 studies 9,11 ; and 26.7% and 44.8% in the 2 outlier studies reporting the highest recurrence rates. 6,10
Infection rates following ED procedures ranged from 0% to 10.3%: 0% in 6 studies 7,8,11,12,14,15 ; and 1.8%, 8.0%, and 10.3% in the 3 studies reporting post-operative infections. 4,9,13
Healing time was reported on average to be less than 10 days in 2 studies, 7,8 but more than 10 days in 4 studies, up to 4.5 weeks. 4,10,13,14
Good patient satisfaction was reported in 5 studies, 8,11,12,14,15 and ease of technique in 2 studies. 11,15
Discussion
Various nail disorders may necessitate matricectomy—onychocryptosis being the most common, with many predisposing factors including improper hygiene, hyperhidrosis, poorly fitting shoes, trauma, and certain comorbidities and medications. 3 Surgery is indicated in severe cases; scarring, cellulitis, osteomyelitis, and amputation are rare but possible complications of onychocryptosis. 3 Surgery may also be indicated in cases of onychogryphosis, where there is no therapeutic modality available to normalize the nails. 14 The purpose of matricectomy is to remove or destroy all or part of the nail matrix, with the goals of pain relief, resolution of recurrent infections, and regaining the ability to wear normal footwear. Bilateral partial matricectomy preserves the functional and cosmetic role of the nail. 2,16 Nail plate extraction alone has been associated with high recurrence rates ranging from 64% to 83%. 6
The matricectomy method using ED is a technique with a good learning curve and that produces consistent results. 5,9 ED uses electric current to generate heat and cause tissue dehydration and superficial destruction, thereby inducing coagulation necrosis and carbonization of cells, which are then ultimately removed via a combination of enzymatic degradation and phagocytosis. 13,17 The amount of ED needed can be reduced when most of the matrix tissue is first removed by an adjunct method such as dissection or curettage. 13
Recurrence rates following ED from the 11 studies in this review ranged from 0% to 44.8%, however, 7 out of the 11 studies reported a recurrence rate of 0% to 5%, and 2 out of the 11 studies, 10% to 15%. Our case series reported 1 recurrence out of 11 ED procedures (9.1%), which falls within the described range. The recurrence rates reported in studies using ED are likely comparable to those of phenolization, which have been reported to range from 0.6%, 1.1%, and 4.3% in study samples of 350, 537, and 948 patients (respectively), up to 18% in a study of 520 patients. 3 In addition, in 4 comparative studies, ED yielded recurrence rates that were clinically similar to those of phenolization, cryotherapy, and curettage. 4,6,9,10 Similarly, in our case series, the recurrence rates following ED and phenolization appeared to be comparable (9.1% and 16.7%, respectively).
ED may also further decrease recurrence rates when used to supplement other matricectomy methods; one study reported significantly less recurrences when ED was used in combination with surgical excision of the matrix. 8 Furthermore, 2 studies noted that when recurrences were re-treated with ED, there were no further recurrences, 8,13 which is in-keeping with the findings from our case series.
In the 9 ED studies that reported infection rates, they ranged from 0% (in 6 studies) up to 10.3% (in 3 studies). Of the 3 studies reporting post-operative infections, 1 study had prophylactic oral antibiotics prescribed, 1 used a prophylactic topical antibiotic/antiseptic cream, and 1 used both. 4,9,13 In our case series, despite the lack of routine prophylactic antibiotic or antiseptic treatments, the infection rates following ED and phenolization were similar at 9.1% and 0%, respectively. The use of routine prophylactic antibiotics is also not recommended in the literature, unless there is evidence of cellulitis. 16,18 It appears the use of antibiotics does not prevent post-operative infections.
In the 6 studies that reported healing times following ED procedures, there was considerable variation, and the data published were often imprecise; while one study reported an average of 7.5 days (with neither post-operative ooze nor pain by day 4), 7 another reported “at least 10 days” 10 and other studies, up to 4.5 weeks. 13,14 One study found that healing time following ED was significantly longer than that of phenolization, 10 however, phenolization has been associated with more pain secondary to unpredictable tissue damage, delayed scar healing, and exudative drainage for up to 6 weeks. 3,4,7,16 Another study found ED to have similar healing times to curettage. 4 Significant healing time variation was also reflected in our case series’ findings: complete healing for ED procedures ranged from 1 week to 16 weeks, and for phenolization procedures, 4 weeks to 12 weeks. Although the presence of infections likely skews these outcomes, the variation may also be in part explained by the differing criteria used to define healing time. Notably, however, there was an absence of prolonged post-operative discharge in the nails treated with ED, a common complication of chemical matricectomy. 3,4,16
Although none of the original studies reported long-term complications directly related to the use of ED in nail surgery, theoretical risks have been described. Given that a lot of heat may be delivered to the tissue in order to ensure that no matrix remains, severe post-operative inflammation and thermal periostitis with long-term pain may occur, 3,9 which may further explain the potentially prolonged healing times reported. The study comparing ED to phenolization established 60 seconds of ED application time—the longest reported of all articles included in the review—and healing time was found to be significantly longer than that of phenolization. 10 The use of a modified hyfrecator tip as demonstrated in this case series, although protective of surrounding tissues in theory, did not appear to significantly decrease healing time; however, this remains inconclusive due to small sample size.
Overall patient satisfaction following matricectomy with ED appears to be good. 8,11,12,14,15 Reasons for patient dissatisfaction appear to pertain to cosmesis—a relevant outcome in our case series—and/or recurrence. 8,13
Although many matricectomy methods have been described, of which phenolization remains the best studied, no one method has clearly emerged as superior. 3,18 Perhaps most attributable is the lack of comparative evidence, as the matricectomy procedures and techniques outlined in the literature vary significantly. The type of digital block, electrodes, sutures, antibiotics, dressings, and adjunct matricectomy methods such as curettage and excision are inconsistently used and/or differ, as do the electrosurgical unit settings and application descriptions, which in addition are often not well specified. Furthermore, the distinction between the various forms of electrosurgery used in the articles is unclear; the terms electrofulguration, electrodessication, electrocautery, diathermy, radiofrequency, and radiowave are often used interchangeably. Thus, there is great potential for technique variation, which is likely contributory to the variation in the recurrences, infections, and healing times reported. Moreover, there is a discrepancy in the way recurrences are presented; some articles report recurrences and nail spicule formations separately. 6,12 -15 It is also possible that outcomes are more dependent on the surgical skills and experience of the physician rather than the matricectomy method itself.
Potential but important confounders that may further contribute to the outcome discrepancies reported in the literature include concomitant comorbidities and/or co-existing nail disorders such as onychomycosis. One study excluded patients who were smokers or known for diabetes, and reported a 0% infection and recurrence rate, as well as a mean of 9 days of healing time. 8 Another study had an exclusion criteria entailing autoimmune disease, severe toe nail deformity, and a history of previous recurrences, and yielded a 13.8% and 10.3% recurrence and infection rate, respectively. 9 Another study comparing ED to phenolization suggested the absence of comorbidities was associated with a lower risk of recurrence in both treatment groups. 10
Finally, the comparison of nail matricectomy techniques is often solely contingent upon recurrence rates. Other important outcomes including infection rates and healing times are inconsistently reported, and even lesser commonly reported outcomes include cosmesis and patient satisfaction. Better understanding of said outcomes may help determine the most appropriate matricectomy technique for a given patient.
Conclusion
Matricectomy is an important technique for addressing painful onychodystrophies. Proponents of ED as a method of matricectomy report low recurrence rates, low infection rates, ease of use, minimal post-operative discharge, and good satisfaction rates. Although there is significant variation in the technique specifics and outcomes reported in the literature, ED is comparable to the other forms of matricectomy methods described.
Neither antibiotic nor antiseptic treatments appear to affect healing outcomes. Cosmesis and recurrence are the main reasons implicated in patient dissatisfaction. Concomitant comorbidities and/or nail disorders may be important predictors of outcomes. Healing time, complication rate, and patient satisfaction are outcomes in addition to recurrence that warrant further study.
Although the generalizability of our case series is limited as a small, retrospective, single-center study with recall bias and loss to follow-up, our findings are consistent with the literature. The innovation of a modified hyfrecator tip is a simple-to-use and effective variation.
Supplemental Material
Online supplementary file 1 - Supplemental material for Electrodessication Matricectomy With Modified Hyfrecator Tip: Case Series and Literature Review
Supplemental material, Online supplementary file 1, for Electrodessication Matricectomy With Modified Hyfrecator Tip: Case Series and Literature Review by Janet Chan and Kevin Pehr in Journal of Cutaneous Medicine and Surgery
Supplemental Material
Online supplementary file 2 - Supplemental material for Electrodessication Matricectomy With Modified Hyfrecator Tip: Case Series and Literature Review
Supplemental material, Online supplementary file 2, for Electrodessication Matricectomy With Modified Hyfrecator Tip: Case Series and Literature Review by Janet Chan and Kevin Pehr in Journal of Cutaneous Medicine and Surgery
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.