
Abstract
Background
A lack of representation of skin of color (SoC) in dermatology curricula is well-documented across North American medical schools and may present a barrier to equitable and comprehensive undergraduate medical education.
Objectives
This study aims to examine representation in dermatologic educational materials and appreciate a link between bias in dermatologic education and student diagnostic ability and self-rated confidence.
Design
The University of Toronto Dermatology Undergraduate Medical Education curriculum was examined for the percentage photographic representation of SoC. A survey of 10 multiple-choice questions was administered to first- and third-year medical students at the University of Toronto to assess diagnostic accuracy and self-rated confidence in diagnosis of 5 common skin lesions in Fitzpatrick skin phototypes (SPT) I-III (white skin) and VI-VI (SoC).
Results
The curriculum audit showed that <7% of all images of skin disease were in SoC. Diagnostic accuracy was fair for both first- (77.8% and 85.9%) and third-year (71.3% and 72.4%) cohorts in white skin and SoC, respectively. Students’ overall self-rated confidence was significantly greater in white skin when compared to SoC, in both first- (18.75/25 and 17.78/25, respectively) and third-year students (17.75/25 and 15.79/25, respectively) (P = .0002).
Conclusions
This preliminary assessment identified a lack of confidence in diagnosing dermatologic conditions in SoC, a finding which may impact health outcomes of patients with SoC. This project is an important first step in diversifying curricular materials to provide comprehensive medical education.
Introduction
A lack of diversity in dermatology education is a well-documented concern. 1,2 Upon review of dermatology practice in Canada, there are gaps in knowledge of the management of common skin conditions in SoC. 2 Toronto is one of the most multicultural cities in the world with nearly 50% of residents identifying as a visible minority, necessitating educational resources that are reflective of the city’s inhabitants. 3
The Fitzpatrick skin phototype (SPT) scale is used to describe skin types based on their reactivity to ultraviolet radiation. According to this system, “SoC” includes SPT IV through VI, skin that tans readily and rarely burns on sun exposure. SPT I through III, includes “white skin,” skin that almost always burns with sun exposure. 4 For the purposes of this paper, SPT I-III skin will be referred to as “white skin” while SPT IV-VI skin will be referred to as “SoC.”
Dermatologic conditions are among the most common reasons for presenting to primary care; however, disparities exist in the identification, treatment, morbidity and mortality of many skin conditions on the basis of skin color. 5 -7 Barriers to accessing healthcare are compounded by variation in presentation in SoC when compared to white skin (Figure 1), presenting a diagnostic challenge, as there is a relative paucity of educational materials for dermatology in SoC. From 1996 to 2005, only 2% of the total teaching events at the annual meetings for the American Academy of Dermatology were devoted to SoC. 1 In a review of popular dermatology textbooks, at most, 19% of pictures were of patients with SoC. 1 Gaps in physician education may contribute to patients’ lack of education about their own risks of various skin conditions. 4,8
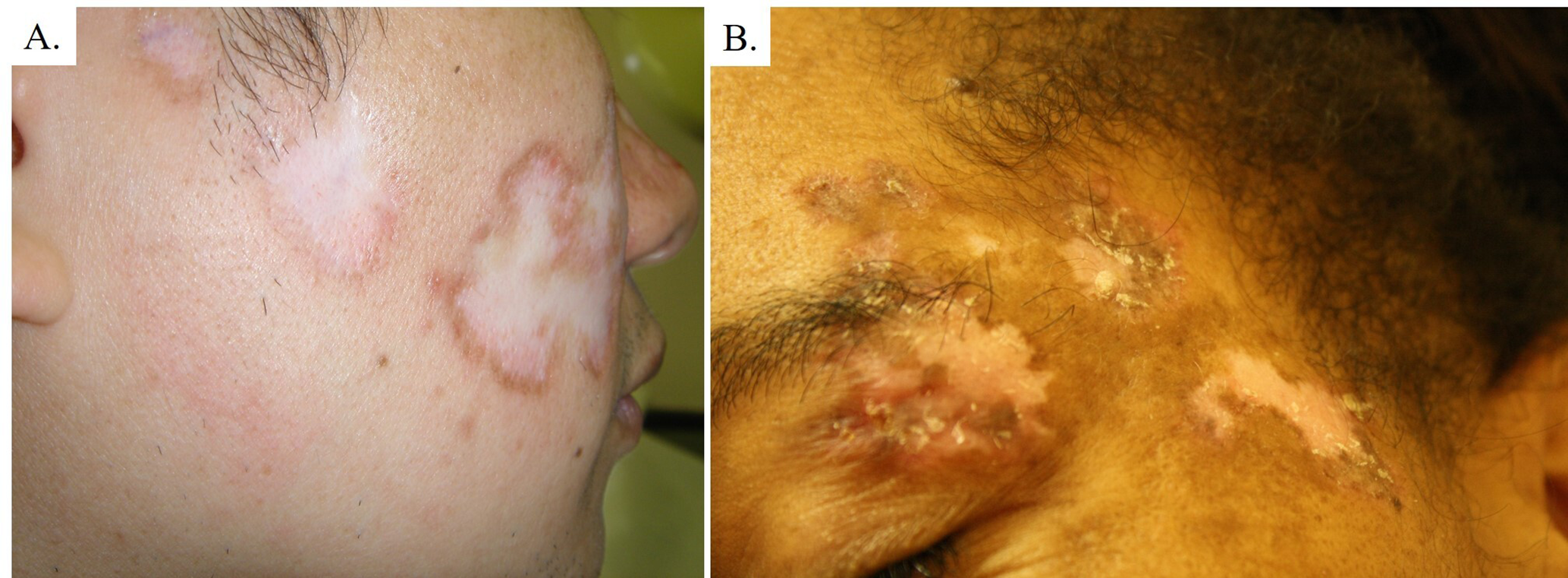
Sample of pictures presented in the survey, highlighting differences in presentation of lupus, represented. (a) White skin (SPT I-III) and (b) skin of color (SPT IV-VI).
This needs assessment project aimed to uncover knowledge gaps in undergraduate medical education with emphasis on common skin conditions in SoC. Our research is important and timely as there is a call to action to improve diversity in dermatology teaching and the field of dermatology. 2
Materials and Methods
This study was conducted at the University of Toronto Temerty Faculty of Medicine which offers a 4-year, undergraduate medical program, like most North American medical schools. Dermatology teaching is administered as a 1 week course in first year, followed by a 1-day patient viewing session at the start of clinical placements (clerkship) in third year. 9 Our study consisted of an audit of the dermatology curriculum followed by a survey assessing diagnostic accuracy and self-rated confidence of medical students when diagnosing dermatologic conditions.
Ethics
This work was completed as a needs assessment project for the purposes of redesigning curriculum. A proposal was submitted to the office of the Research Ethics Board (REB) manager who determined this work did not meet criteria for formal REB review. Demographic data, aside from the year of medical school, was not collected. Participants provided written consent prior to participating in the survey. All data were collected and stored anonymously and analyzed in aggregate. Only members of the study team had access to the collected data.
Study Population
The study population was pre-clerkship medical students at the University of Toronto. This study was conducted in the 2019/2020 academic year and was administered to the first- and third-year cohorts after completion of their respective dermatology curricula.
Curriculum Audit
An audit was performed to determine representation of SoC in the 2019/2020 curricula. Two authors (K.O.A. and E.B.) independently reviewed all images presented in the curriculum and classified them as Fitzpatrick Type I-III (white skin) or Fitzpatrick Type IV-VI (SoC), based on comparison with standardized reference images. 10 Criteria for categorization was developed collaboratively and agreed upon. Images of dermatologic conditions in SoC were reported as a percentage of the total number of images. Images from non-mandatory learning resources were not included in the audit.
Survey
Students were invited to participate in an online, voluntary 20 question survey following the dermatology block for first-year students and following a 1-day transition to clinic dermatology course for the third-year students. The survey consisted of 10 multiple-choice questions, each paired with a corresponding 5-point Likert item assessing the students’ confidence in diagnosis. Likert-item options included: “Unsure,” “Somewhat Unsure,” “Neutral,” “Somewhat Confident,” and “Confident.” Five common dermatologic conditions (psoriasis, lupus, basal cell carcinoma, atopic dermatitis, and molluscum contagiosum) were represented in both white skin and SoC.
Diagnostic accuracy was quantified by assigning a value of 1 to each correct answer and 0 to each incorrect answer. The maximum possible score for overall diagnostic accuracy was 5/5 for SoC or white skin. Each option on the Likert item was assigned a value from 1 (Unsure) to 5 (Confident), with a maximum score on each item of 5. The 5 Likert-items for each dermatologic condition in white skin or SoC summed to a maximum possible score of 25/25 for each skin type.
Students were asked to provide feedback about specific curriculum changes that could be used to enhance instruction of dermatologic conditions in skin of color. They were able to select from a menu of options (photos embedded into in-class lectures and self-learning modules, online image bank, live patient viewing led by dermatologists) and were encouraged to provide their own suggestions (free text). Students were also asked to rate their agreement with a statement “There was adequate representation of dermatological conditions in SoC (ie, olive, brown, black skin tones) in my dermatology educational materials.” on a 5-point Likert-item from “Agree” to “Disagree.”
Data Analysis
All statistical analyses were completed in GraphPad Prism. The relationship between skin type, cohort, diagnostic accuracy and overall self-rated confidence were analyzed with the use of a 2-way ANOVA. The interaction between skin type and diagnostic accuracy on individual survey questions was analyzed with the use of Fisher’s exact test. The interaction between skin type and self-rated confidence on individual survey questions was analyzed with a χ2 test. For the purposes of this analysis, the 5-point Likert item for self-rated confidence was condensed to a 3-point scale (summing the “Confident” and “Somewhat Confident” categories and the “Unsure” and “Somewhat Unsure” categories). A P value of <.05 was considered significant.
Results
Curriculum Audit
The first-year dermatology curriculum at the University of Toronto Temerty Faculty of Medicine consists of in-class lectures (10 hours), online video modules (1.75 hours), small group case-based learning (2.5 hours) and small group clinical teaching sessions (4 hours). The curriculum audit revealed that of 513 images represented in dermatology teaching materials, 19 (3.7%) displayed conditions in SoC. The third-year dermatology curriculum consists of online self-learning modules and dermatologist-led patient viewing (7 hours). Of the 198 pictures included in this curriculum, 12 (6.06%) displayed dermatologic conditions in SoC.
Survey Response
For the first-year cohort, responses were received from 101/268 students (38%). For the third-year cohort, responses were received from 76/261 students (29%).
Diagnostic Accuracy
Students in the first-year cohort had a mean diagnostic accuracy of 3.89/5 (77.8%) for skin conditions presented in white skin and 4.30/5 (85.9%) in SoC. Students in the third-year cohort had a mean score of 3.57/5 (71.3%) for skin conditions presented in white skin and 3.62/5 (72.4%) in SoC (Figure 2). There was a significant interaction effect between skin type and cohort, prompting a post-test analysis (P = .0367). First-year students performed significantly better overall in diagnosis of skin conditions in both skin type groups when compared to third-year students (P < .05). Within the first-year cohort, students were significantly less accurate in their diagnosis of dermatologic conditions in white skin than in SoC (P < .05). Within the third-year cohort, there was no difference in diagnostic accuracy between skin type groups (P > .05).
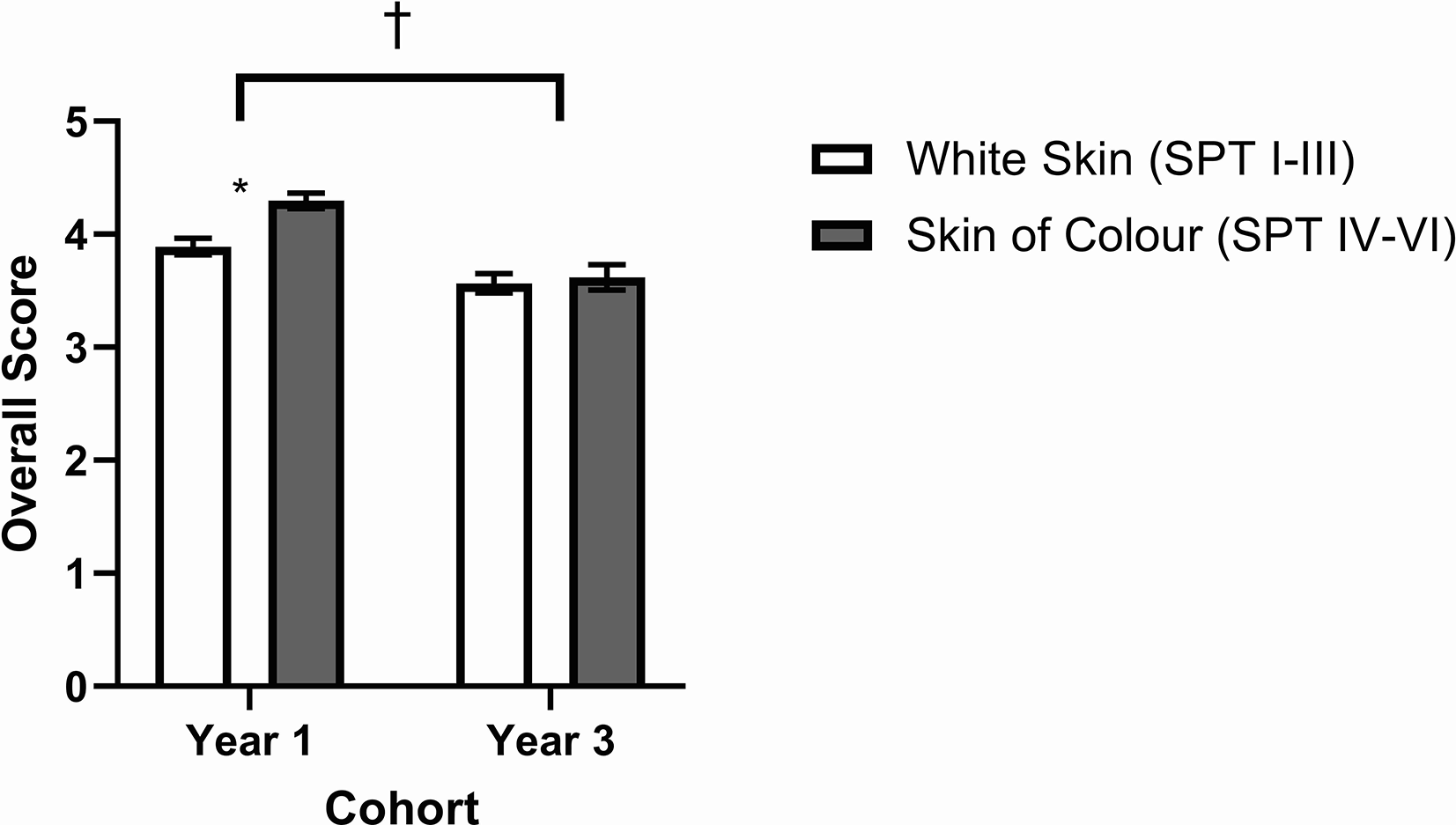
Overall diagnostic accuracy of first-year and third-year medical students for photographs of 5 common dermatologic conditions in white skin (SPT I-III) and skin of color (SPT IV-VI). * Denotes a significant difference between skin types. †Denotes a significant difference between cohorts. Year 1 N = 101, Year 3 N = 76. P < .05 was considered significant. Data presented as mean ± SEM.
Within the first-year cohort, there were no statistically significant differences in accuracy based on skin type when diagnosing psoriasis (P > .05), lupus (P > .05), basal cell carcinoma (P > .05) and atopic dermatitis (P > .05) (N = 101). Third-year students were equally accurate in their diagnoses of psoriasis (P > .05), lupus (P > .05), and atopic dermatitis (P > .05) across skin types (N = 76). When diagnosing basal cell carcinoma, third-year students were significantly more accurate in white skin than in SoC (N = 76, P = .0049). First- and third-year students were significantly more accurate in their diagnosis of molluscum contagiosum in SoC than in white skin (N = 101, P < .0001; N = 76, P = .0467) (Figure 3A and B).
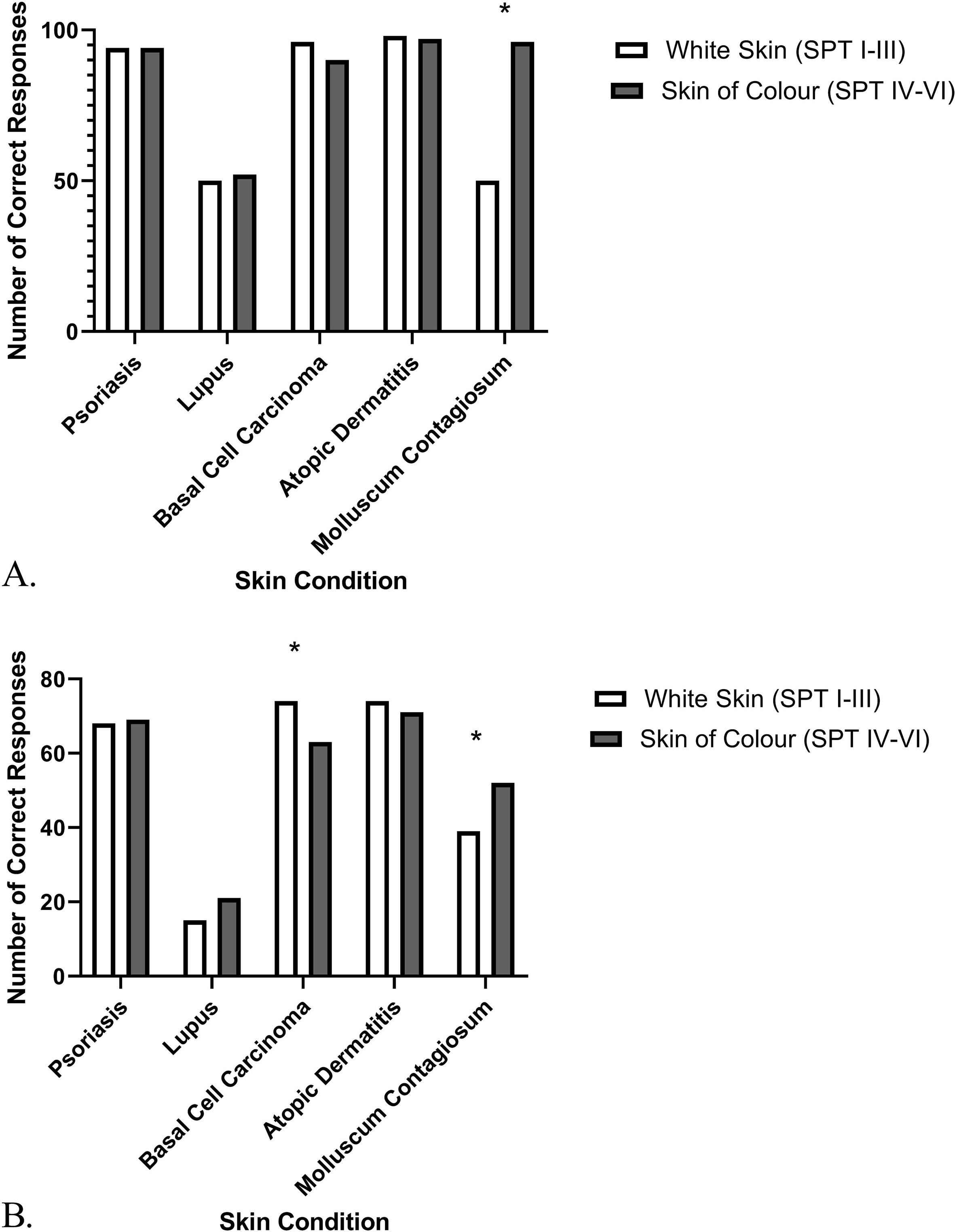
Diagnostic accuracy of (a) first-year and (b) third-year medical students in assessing photographs of 5 common skin conditions in white skin (SPT I-III) and in skin of color (SPT IV-VI). *Denotes a significant difference between skin types. (a) Year 1 cohort, N = 101. (b). Year 3 cohort, N = 76. P values < .05 were considered significant. Data presented as number of responses.
Self-Rated Confidence
Students in the first-year cohort had a mean self-rated confidence of 18.75/25 when diagnosing skin conditions presented in white skin and 17.78/25 in SoC. Students in the third-year cohort had a mean self-rated confidence of 17.75/25 when diagnosing skin conditions presented in white skin and 15.79/25 in SoC (Figure 4). Overall, first-year students were significantly more confident in their diagnoses than third-year students (P = .0001), but both cohorts were significantly less confident in diagnosis of skin conditions in SoC than in white skin (P = .0002).
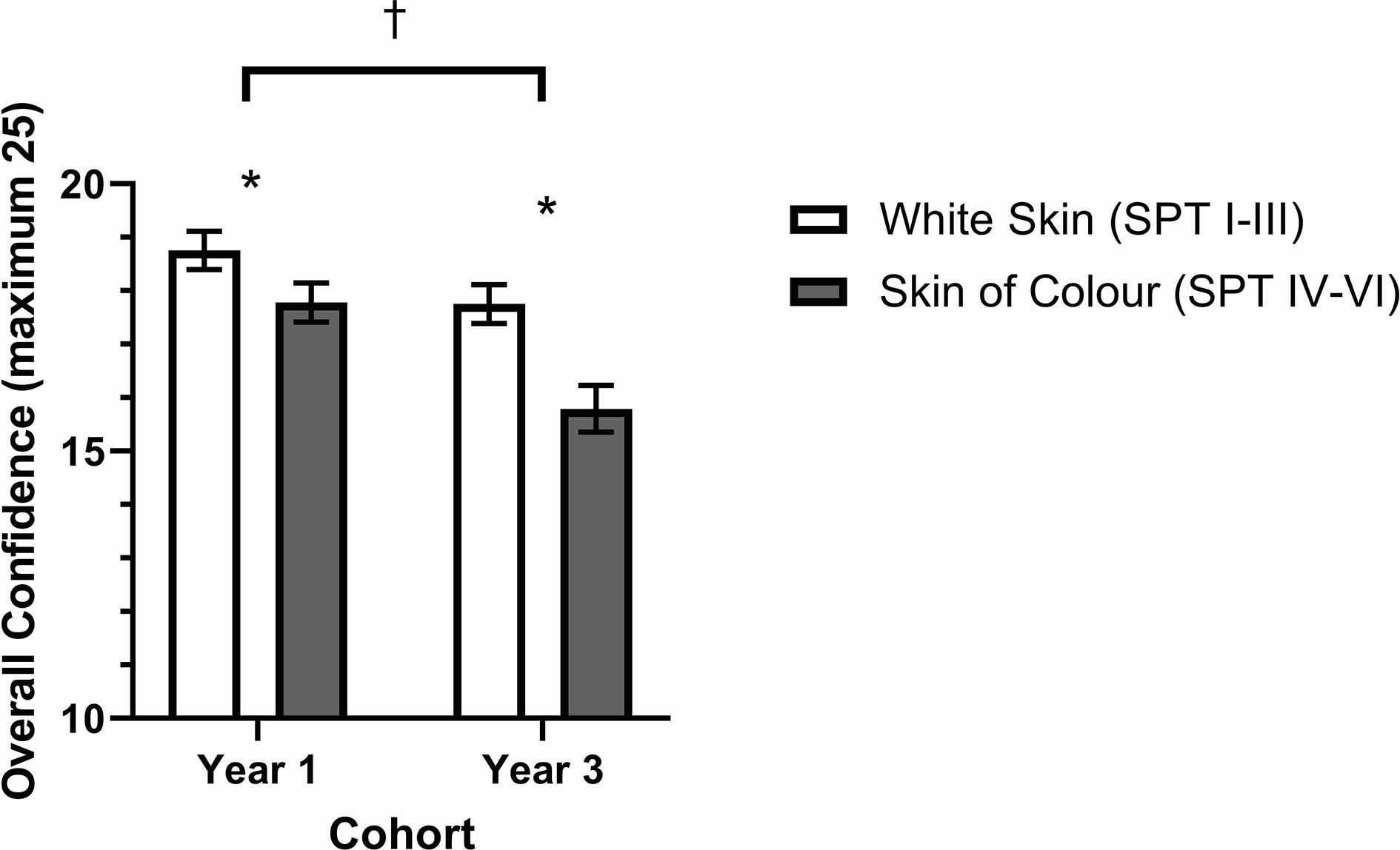
Overall self-rated confidence in accuracy of diagnosis in first-year and third-year medical students across 5 common conditions assessed in white skin (SPT I-III) and skin of color (SPT IV-VI). Year 1 N = 101, Year 3 N = 76. * Denotes a significant effect of skin type. †Denotes a significant effect of cohort. P values < .05 were considered significant. Data presented as mean ± SEM.
Among first-year students, there was no difference in the distribution of self-rated confidence in diagnosis of psoriasis (P > .05, degrees of freedom (df) = 2), lupus (P > .05, df = 2), and atopic dermatitis (P > .05, df = 2) between white skin and SoC (N = 101). First-year students trended significantly toward confidence in their diagnosis of basal cell carcinoma in white skin (N = 101, P = .0024, df = 2), while the reverse was true for molluscum contagiosum, with the distribution of responses indicating greater confidence in SoC (N = 101, P < .0001, df = 2) (Figure 5A). Self-rated confidence of third-year students did not vary with skin type in the diagnosis of psoriasis (N = 76, P > .05, df = 2) and molluscum contagiosum (N = 76, P > .05, df = 2). Third-year students trended to be more confident in diagnosing lupus (P value = .0410, df = 2), basal cell carcinoma (P < .0001, df = 2), and atopic dermatitis (P = .0235, df = 2) in white skin than in SoC (N = 76) (Figure 5B).
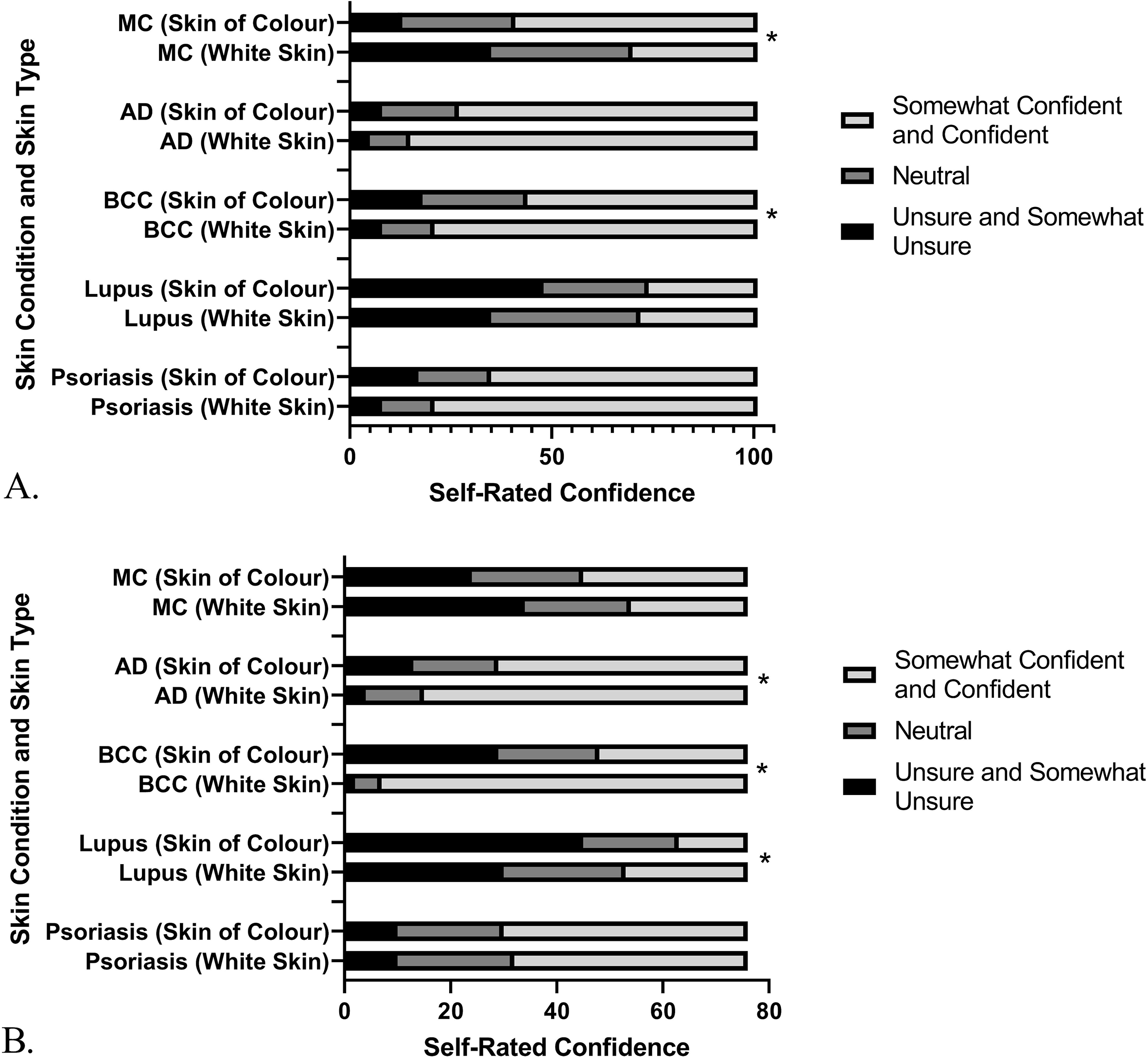
(a) First-year and (b) third-year medical students self-rated confidence in diagnosis of 5 common skin conditions in white skin (SPT I-III) and skin of colour (SPT IV-VI). Year 1 cohort, N = 101. Year 3 cohort, N = 76. *Denotes a significant effect of skin type. P values < .05 were considered significant. Data presented as number of responses. AD, atopic dermatitis; BCC, basal cell carcinoma; MC, molluscum contagiosum.
Curriculum Modification Feedback
Qualitative feedback highlighted a desire for more exposure to educational materials that display dermatological conditions in SoC. The majority of first-year students identified that photos embedded in lectures and self-learning modules would be most helpful, while third-year students suggested photos be added to lectures, in addition to an online image bank for independent review and live patient viewing led by a dermatologist (Table 1). Unfortunately, there was minimal free-text feedback from students about how to modify the dermatology curriculum. When asked if the curriculum provided adequate coverage of SoC, 49 students (48.5%) in the first-year cohort and 36 students (47.4%) in the third-year cohort, selected “Disagree” or “Somewhat Disagree” (Figure 6).
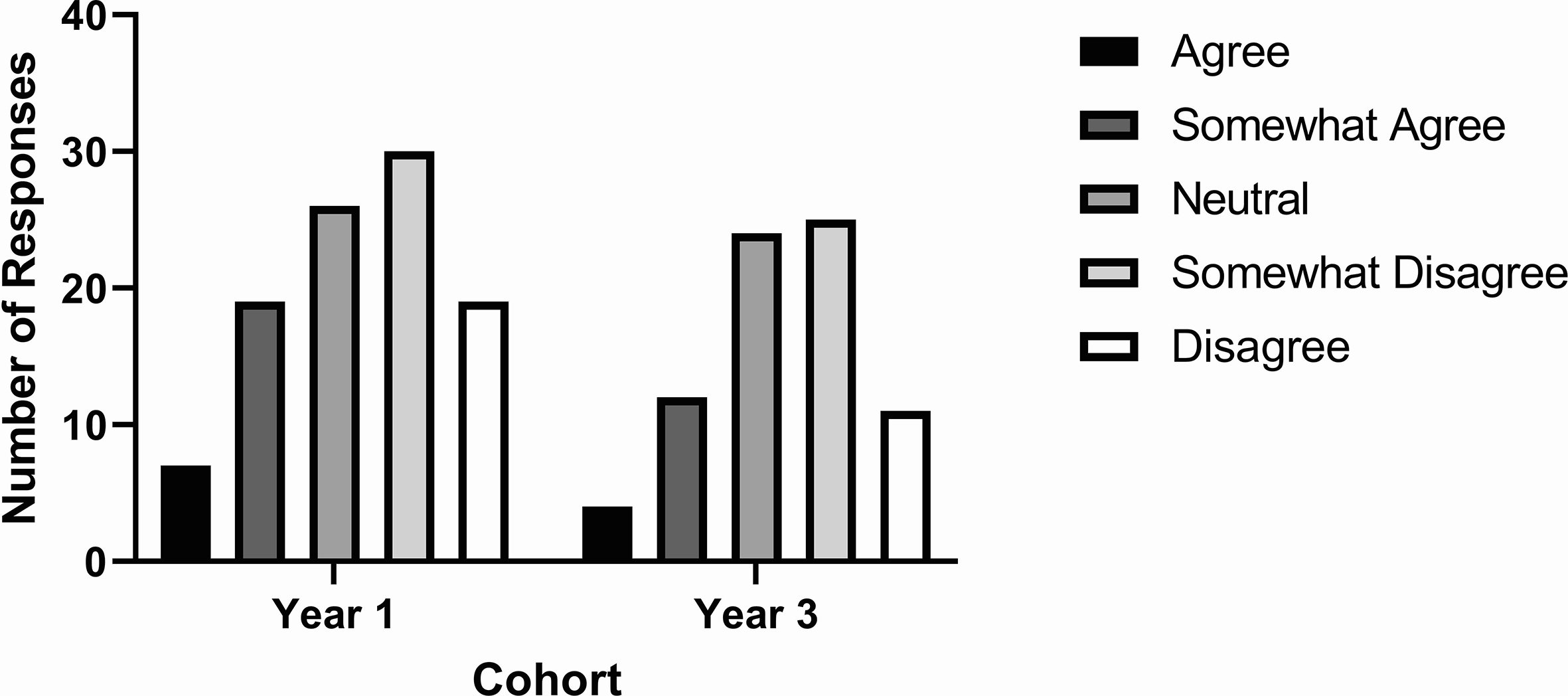
First-year and third-year medical students’ agreement with the statement “There was adequate representation of dermatological conditions in skin of color (ie, olive, brown, black skin tones) in my dermatology educational materials.” as measured on a 5-point Likert-item. Year 1 cohort, N = 101. Year 3 cohort, N = 76. Data presented as number of responses.
Student Suggestions for Curriculum Modification.
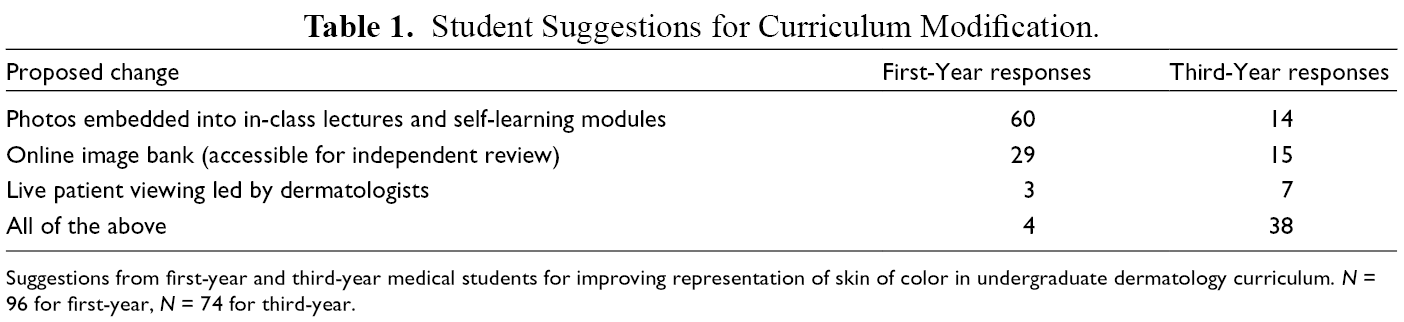
Suggestions from first-year and third-year medical students for improving representation of skin of color in undergraduate dermatology curriculum. N = 96 for first-year, N = 74 for third-year.
Discussion
Our curriculum audit revealed an underrepresentation of dermatologic conditions in SoC. Only 3.7% of all images presented in first-year, and 6.06% of those presented in third-year, were in skin of color. This finding is lower than rates seen in medical curricula at other North American medical schools. 11 -13 Discrepancy between these rates may be due to demographic differences between Canada and the United States, as our data were compared with curricula from American medical schools. In addition, the province of Ontario does not collect race-based health data as rigorously as is done in the United States. Critics have highlighted that this lack of data may have myriad implications for the equitable distribution of healthcare resources and evaluating the efficacy of health promotion strategies. 14 Perhaps this paucity in race-based health data may contribute to a corresponding dearth of diversity in medical education. In addition, the negative implications for patient care due to a lack of ethnic diversity in the field of dermatology have been explored. 15 A lack of diversity in the field of dermatology may also contribute to a lack of diversity in educational materials. A similar needs assessment of dermatology texts at several of the top medical schools in the United States found an underrepresentation of skin of color at both a chapter and topic level. 11 -16 A lack of representation of SoC in medical education contributes to pre-existing health disparities, affects trainees’ well-being and limits the provision of equitable dermatologic care. 16 These long-standing absences of tonal diversity in educational materials must be addressed to reflect a racially and ethnically diverse population.
In both the first- and third-year cohorts, diagnostic accuracy was above 70%, irrespective of the Fitzpatrick phototype. A similar study performed by Fenton et al. at 2 U.S. medical schools found that students diagnosed some conditions well regardless of phototype, whereas accuracy in others differed by skin type. Notably, first-year students in our study were significantly more accurate than their third-year peers in diagnosing skin conditions in both white skin and SoC. This disparity between first- and third-year classes could be due to a recency bias, as the survey was administered to first-year students on the final day of their week-long dermatology block. Aldridge et al. found that dermatologic diagnostic accuracy in undergraduate medical students increased 10 days after beginning undergraduate teaching and when diagnostic accuracy was reassessed 12 months later, half of this effect had disappeared. 17 This result highlights the role of information retention after didactic dermatology teaching, which is also demonstrated in our study results.
The first- and third-year participants were significantly less confident overall in their diagnoses of dermatologic conditions in SoC. Our finding provides nuance into the previously uncovered lack of confidence in medical trainees’ ability to diagnose dermatologic lesions. 18 -20 Trainee research has shown a low correlation between confidence and diagnostic accuracy in a number of clinical procedures, but this research fails to explore how this low correlation may impact racialized health care disparities and inequities. 19,20 It is possible, that a medical student who lacks confidence in diagnosing conditions in SoC avoids further clinical exposure during training, ultimately risking a deficiency in their patients’ care. Chiang et al. postulate the role of additional clinical exposure to various dermatologic conditions to improve the confidence of medical learners in diagnosing skin lesions, while Fenton et al. suggests presenting all dermatologic conditions in both light skin and SoC as part of a comprehensive dermatology curriculum. 18,21
Despite significant differences in self-rated confidence, we did not identify major dermatologic condition-specific differences in diagnostic performance. It is most interesting to consider the discrepancy between a lack of self-confidence, yet fair diagnostic accuracy. While some research indicates a strong positive relationship between self-rated confidence and diagnostic accuracy, other findings suggest a lack of correlation. 19,22 Diagnostic accuracy may have been falsely elevated in this survey due to the cueing effect seen with multiple-choice questions. While multiple-choice greatly increased the feasibility and implementation of this survey, the use of free-response questions may have provided a more accurate assessment of students’ diagnostic ability. 23 Despite a lack of association seen here between diagnostic accuracy and self-rated confidence, a lack of self-rated confidence in the diagnosis of dermatologic conditions in SoC presents unique implications beyond medical education. A medical student unsure of their diagnosis may symbolize a lack of confidence in the medical system when interacting with a racialized patient. 16 The potential implications of a lack of visual representation of SoC in dermatology education are numerous and must be considered when developing curricula.
Students in our study suggested curriculum additions to increase ethnic representation. By increasing diversity in medical education and encouraging students to reflect on the context in which they are learning, students may improve their critical-thinking skills and become more able to adapt to the myriad challenges faced in healthcare. 24 All Faculties of Medicine should aim to provide contextual diversity in their curricula, especially when teaching the visual specialty of dermatology.
There were several limitations in our study. Our study was conducted in a single urban academic center and was not administered in a proctored environment. Participation bias may have influenced the results, thus, limiting the generalizability of the results to all medical students. We were unable to randomize the question order due to limitations in our survey platform. The dermatologist authors (Drs. R.A.B., E.D., and M.J.) worked collaboratively to select pictures of similar diagnostic difficulty for SoC and white skin, but it is possible that anatomic lesion site, photo quality, and lighting introduced confounders on the survey results (basal cell carcinoma and molluscum contagiosum). Finally, while anonymity of the survey responses likely encouraged participation, it also made assessment of participant population demographics unreasonable.
Results from this survey indicate that pre-clerkship students at the University of Toronto are accurate in diagnosing dermatologic conditions across skin types; however, their self-rated confidence drops significantly when diagnosing dermatologic conditions in SoC. Our curriculum audit of the undergraduate dermatology curriculum at the University of Toronto highlighted a lack of diversity, like deficiencies found at other North American institutions. 11 -13,25 Most concerning about this finding is that Toronto is one of the most multicultural cities in the world, suggesting that students training here are not receiving a curriculum that reflects the population they will serve. This work will inform curriculum renewal initiatives to improve SoC teaching in undergraduate medical education at the University of Toronto.
It is the hope of the authors that these findings support curriculum improvement and further research, that will ultimately help to address this gap and ensure that the next generations of physicians are able to accurately, equitably and confidently diagnose and treat patients of all skin types.
Footnotes
Acknowledgments
We would like to acknowledge faculty members at the University of Toronto who were instrumental in this study’s design and execution: O.N. for her support and guidance in the inception of this process; J.N-Y. for her encouragement; P.B. for her support in connecting us with resources.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.