
Abstract
Background:
There are no current instruments to facilitate population screening for rosacea.
Objective:
To develop and evaluate a screening instrument for rosacea applicable for population surveys.
Methods:
A rosacea-specific screening instrument (Rosascreen), consisting of a subject-completed questionnaire and screening algorithm, was developed based on current diagnostic criteria for rosacea. Three iterations were pilot tested and refined for clarity and sensitivity in adult outpatients with and without rosacea.
Results:
Three subject groups were consecutively evaluated with iterations of the questionnaire at each centre (overall N = 121). The final version had a sensitivity of 93% to 100% for key diagnostic criteria, and use of the algorithm had a sensitivity of 100% for detection of rosacea and specificity of 63% to 71%. Most subjects found the questionnaire easy to understand and complete.
Conclusion:
Rosascreen, a subject-completed questionnaire and diagnostic algorithm, is a highly sensitive screening instrument that may facilitate estimation of rosacea prevalence in general populations.
Rosacea is an inflammatory facial dermatosis with characteristic clinical features. Prevalence estimates range from less than 1% (in residents of the Faroe Islands of Denmark) to more than 20% (in an Estonian population).1-5 However, direct comparisons are difficult due to differences in case ascertainment, types of populations, and sociocultural perceptions.
Prior to the publication of the National Rosacea Society (NRS) criteria in 2002, 6 the study of rosacea was hindered by the absence of diagnostic criteria. These defined criteria include primary features (transient erythema or flushing, fixed/nontransient erythema, inflammatory papules/pustules, telangiectasia) and secondary features (burning, plaque, edema). Furthermore, the NRS described 4 subtypes: erythematotelangiectatic (persistent central facial erythema), papulopustular (facial erythema with transient papules and/or pustules), phymatous (including skin thickening), and ocular. 6
Most recent studies have found erythematotelangiectatic rosacea to be the most common, followed by papulopustular; phymatous was the least common.2,5,7 Ocular rosacea may be associated with 50% of cases of cutaneous roscaea. 8 Nevertheless, epidemiological information on rosacea remains sparse, with few general population prevalence studies. 9
Estimation of disease prevalence in a population can be facilitated by using a screening instrument followed by confirmatory evaluation of positive responders by clinical experts. A similar approach was used previously in screening for chronic obstructive pulmonary disease and heart failure.10,11 The absence of a screening instrument for rosacea based on the NRS criteria is a current shortcoming in estimating population prevalence. Accordingly, the purpose of this study was to develop and evaluate the operating characteristics of a screening instrument for rosacea based on a self-administered questionnaire and algorithm (Rosascreen).
Methods
This 2-centre study involved 1 centre in Canada and 1 centre in Sweden and was conducted in accordance with the Declaration of Helsinki and Good Clinical Practices. The study was performed in compliance with local regulatory requirements and was reviewed and approved by local ethics committees. All subjects provided their written informed consent before participation.
English and Swedish versions of the self-administered screening questionnaire and the evaluative algorithm were developed prior to patient testing. Testing of questionnaires was performed at the clinical practices of 2 dermatologists with expertise in rosacea. For each cycle of questionnaire testing, each centre enrolled approximately 20 subjects attending routine consultations or follow-up visits (10 with and 10 without rosacea). Subjects completed the questionnaire just prior to the consultation. Male and female subjects aged between 18 and 65 years old were eligible.
Cycles of questionnaire testing were performed until optimal phrasing and sensitivity were achieved (Figure 1). Each cycle included questionnaire administration for self-completion by subjects; investigator evaluation for rosacea signs and symptoms and dermatological diagnoses including confounders for rosacea; identification of discrepancies between subject responses and investigator assessment; and clarification of discrepancies by the investigator to evaluate clarity and phrasing with subject input.
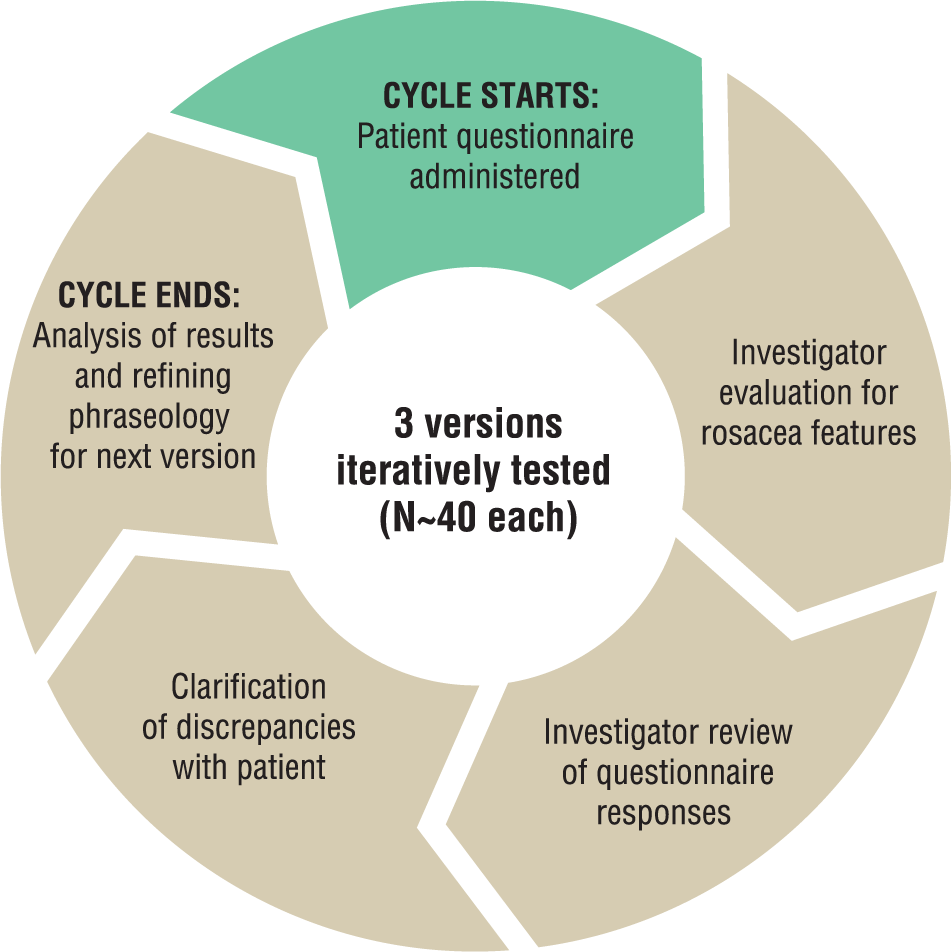
Questionnaire testing cycles.
After each cycle, the questionnaire was analyzed by rosacea experts (including the 2 study investigators) for improvements in phrasing as needed. The next version was then tested on another group of subjects and repeated until sensitivity rates were optimized.
The questionnaire included domains regarding demographics, acceptability (time required and ease of completion), other facial dermatoses, treatment history, and 7 key items relevant to rosacea. The latter were developed from NRS expert consensus criteria for diagnosis of rosacea. 6 Photographic examples were provided showing characteristic clinical features with images of various severities to assist subject comprehension; these remained unchanged across the tested versions.
An algorithm was developed for rosacea case finding defined as the presence of at least one of the following: rhinophyma; central facial persistent erythema; facial warmth/stinging burning for darker phototypes (IV to VI); and/or a previous diagnosis of rosacea. This was developed from a review of the literature and the input of the investigators and rosacea experts regarding criteria of highest sensitivity. Papules/pustules and ocular symptoms were not included in the algorithm due to their high prevalence in other conditions not associated with rosacea, such as acne vulgaris and allergic conjunctivitis, respectively.
Data collected were descriptively summarized, and missing values were not replaced (observed data). Analysis of the measurement properties of the questionnaire (sensitivity and specificity) was performed for the key items (flushing, erythema, facial warmth and/or stinging/burning, papules/pustules, telangiectasia, rhinophyma, and ocular manifestations) and the algorithm.
Sensitivity, or the proportion of subjects with rosacea, shows the ability of the test to identify true rosacea patients and was targeted to approach 100%. Specificity is the ability of the test to identify patients without rosacea. The questionnaire was developed with the aim of achieving the highest sensitivity (primary objective) based on subject comprehension.
Results
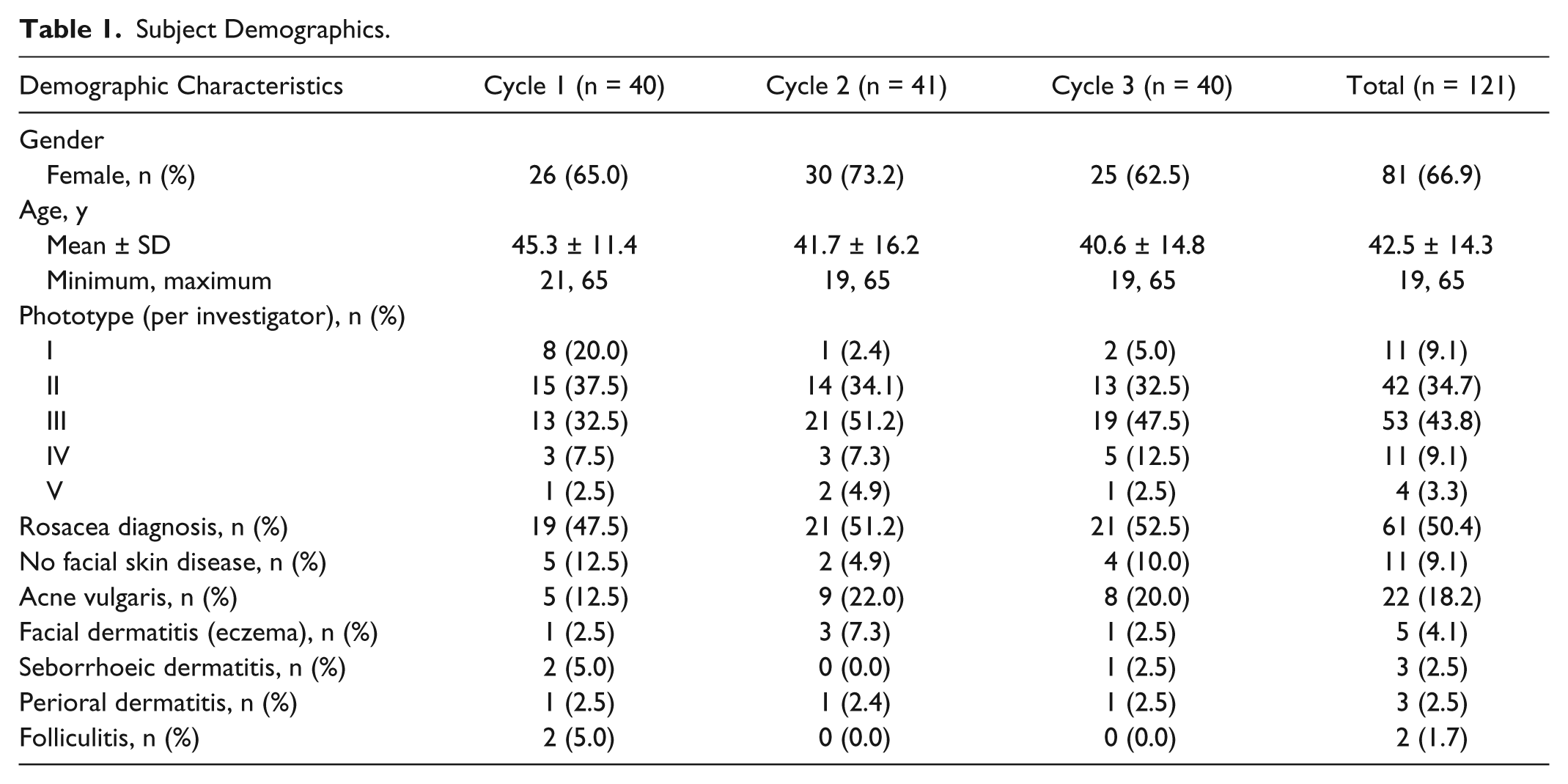
Between May and December 2012, a total of 121 subjects (61 in Canada and 60 in Sweden) were recruited, with approximately 40 subjects in each of the 3 cycles of questionnaire testing. The cohorts in each cycle were demographically similar (two-thirds female, mean age 43 years, predominantly phototype II-III), except for a slightly higher proportion with phototype I in cycle 1 (Table 1). Half were diagnosed by the investigators with rosacea (47.5%, 51.2%, and 52.5% for cycles 1, 2, and 3, respectively, and 50.4% overall) with the remainder having mainly acne vulgaris (18%) or no facial dermatosis (9%) (see Table 1). Amongst those with investigator-diagnosed rosacea, associated signs and symptoms were persistent facial erythema (~92%), facial warmth or stinging/burning (77%), papules/pustules (74%), telangiectasia (64%), ocular manifestations (31%), and rhinophyma (10%) (Figure 2).
Subject Demographics.
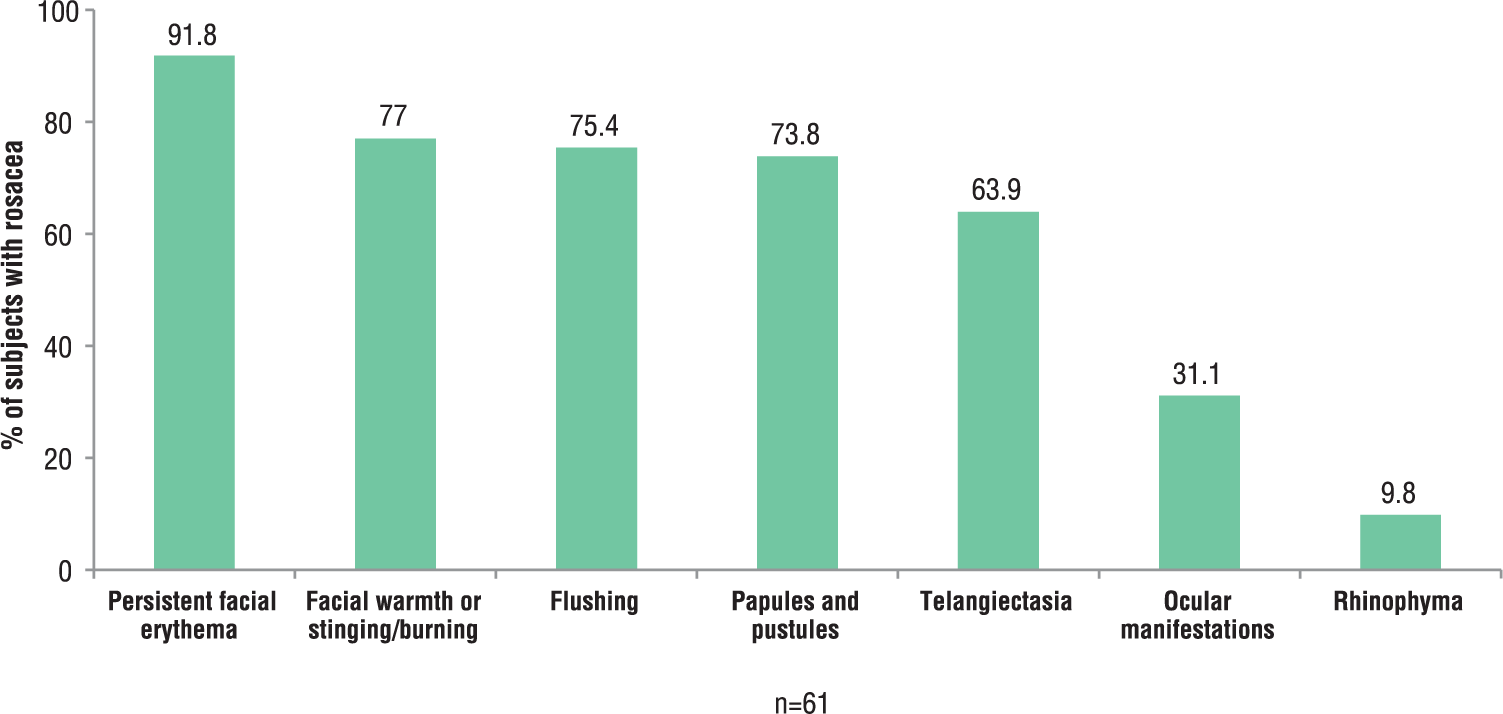
Investigator-reported signs and symptoms for subjects with rosacea.
For all 3 phases of testing, 90% of subjects indicated that the questionnaire was easy to understand and complete. All indicated that the time required to complete the questionnaire was acceptable.
Table 2 includes the sensitivity and specificity for each of the key items for the 3 cycles of testing. For key items, sensitivity ranged from 95% to 100%. The question regarding rhinophyma achieved 100% sensitivity in the first cycle and did not necessitate revision, whereas the remaining 6 items required modification (including the question regarding erythema, which was modified twice). Table 3 shows optimized phrasing for each of the key items.
Measurement Properties of Rosacea Key Signs and Symptoms and Rosacea Diagnosis Based on Questionnaire Version a .
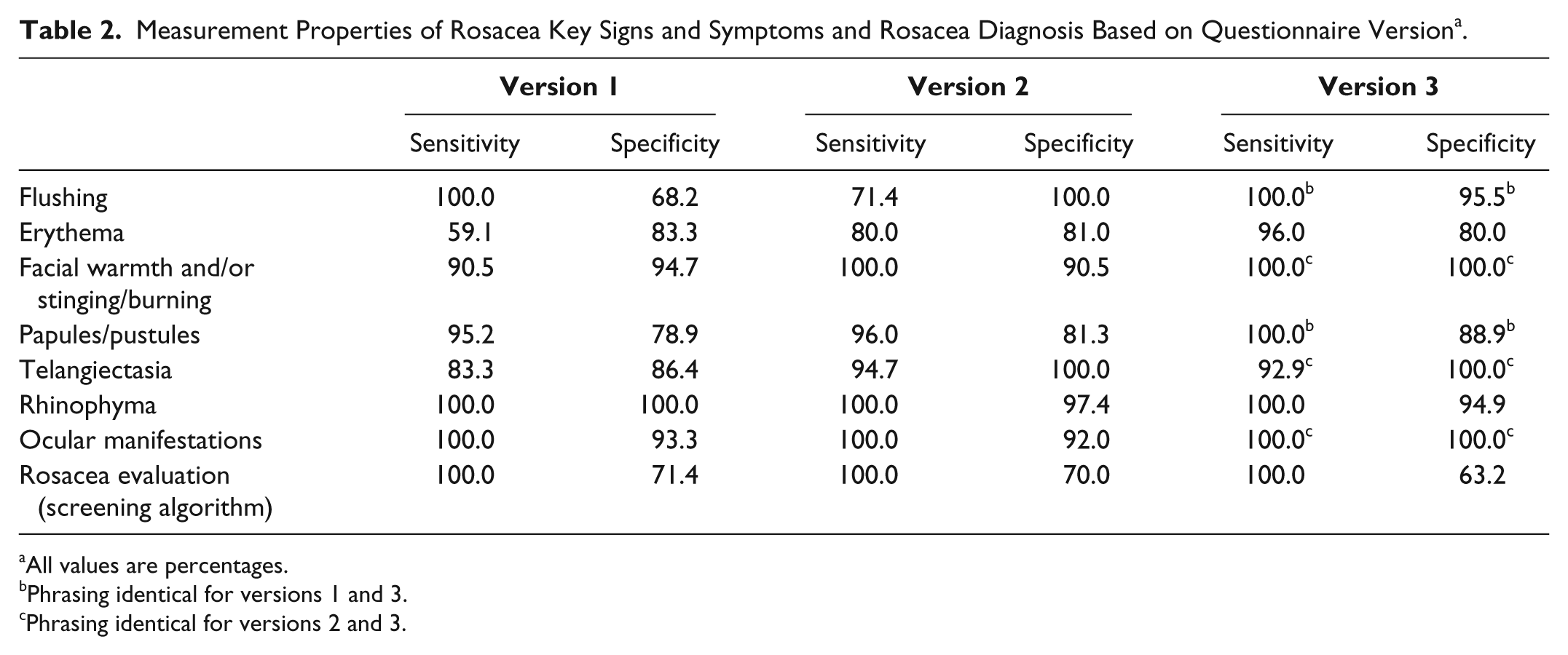
All values are percentages.
Phrasing identical for versions 1 and 3.
Phrasing identical for versions 2 and 3.
Excerpt of Questionnaire: Key Items, Showing Select Photographs. a
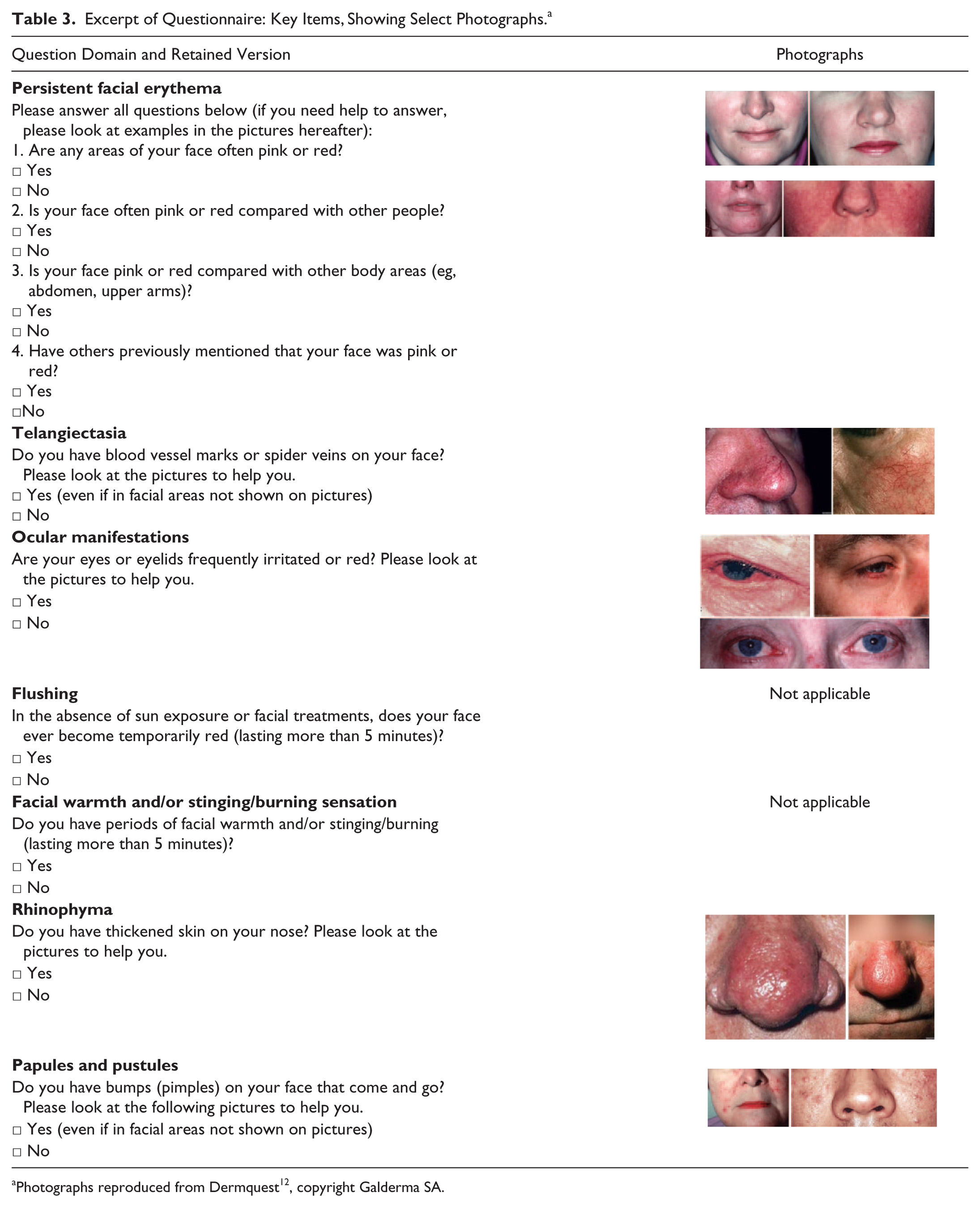
Photographs reproduced from Dermquest 12 , copyright Galderma SA.
As persistent facial erythema was the symptom expected by experts to be the most frequent and sensitive for rosacea patient selection, it was essential to maximize sensitivity. In the first cycle with the question “Do you experience redness on all or part of your face all the time?” sensitivity was 59% and specificity 83%. The modification for the second cycle comprised a positive response to either of “Are any areas of your face always red?” or “Is your face red compared with other people?” and achieved sensitivity of 80% and specificity of 81%. For the third cycle, a positive response to any of “Are any areas of your face often pink or red?” or “Is your face often pink or red compared with other people?” or “Is your face pink or red compared with other body areas?” or “Have others previously mentioned that your face was pink or red?” achieved sensitivity of 96% and specificity of 80%.
Rosacea was defined as present on screening if at least 1 of the following was positive: rhinophyma, central facial persistent erythema, facial warmth or stinging/burning for darker phototypes (IV to VI), and/or previous diagnosis of rosacea. The algorithm achieved 100% sensitivity across all 3 versions, regardless of the sensitivity of key question phrasing, with a specificity that only varied slightly from about 63% to 71%. The final version of the algorithm had a specificity of 63%, which was deemed acceptable since the level of sensitivity remained 100% and included the highest sensitivity for the item regarding erythema.
Discussion
The wide range of reported rosacea prevalence from similar regions in Europe illustrates the need for harmonization in screening and case finding based on currently accepted diagnostic criteria. Accordingly, the rosacea screening instrument described herein, consisting of a questionnaire and algorithm, was derived directly from NRS criteria. 6 The screening instrument exhibited good measurement properties as it attained 100% sensitivity in pilot testing, thereby fulfilling the prime criterion for a screening method. Furthermore, these criteria were operationalized into layman’s language and patients indicated that the questionnaire was easy to understand and undertake. These are both important features for a general public screening instrument. 13 As rosacea is a relatively uncommon disease, direct diagnosis of the general population by dermatologists is impractical. Accordingly, this instrument should facilitate case finding in population studies whereby only screen-positive subjects would proceed to further dermatological evaluation.
High sensitivity was the objective of this instrument to maximize detection of true-positive cases. Reasonable specificity was achieved as confounding diagnoses were largely addressed by exclusion of papules/pustules and ocular symptoms. Their inclusion would have reduced specificity due to their high prevalence in other conditions, such as acne vulgaris and allergic conjunctivitis, respectively.
The majority (92%) of patients with rosacea were assessed by investigators to have persistent facial erythema and were also highly affected by facial warmth or stinging/burning, papules/pustules, and telangiectasia. The selection of the first 2 of these signs and symptoms in the algorithm was thus pertinent. Although rhinophyma and stinging/burning in darker skin were not differentiated in our results due to low prevalence in the pilot study population, they are anticipated to be relevant for the detection of rosacea presentations when screening larger general populations. High levels of sensitivity were achieved on all key item questions of the survey and for the algorithm.
Limitations of this study include development in English and Swedish, so other languages will require linguistic and cultural validation. Also, cohorts (rosacea or nonrosacea subjects) in this pilot study were not matched for age, gender, or other sociodemographic characteristics. However, the cohorts in each cycle were demographically similar.
In conclusion, Rosascreen is a subject-completed questionnaire and screening algorithm that is highly sensitive for detecting rosacea, suggesting its potential for application in case finding with subsequent dermatologist verification in general population surveys. The acceptability of Rosascreen by patients in this pilot study suggests that it may be practical for use with the general public.
Footnotes
Acknowledgements
The authors thank other members of the Rosacea International Study Group (RISG) committee for their expert input. Writing assistance was provided by Galadriel Bonnel, PhD, who is a freelance medical writer.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Galderma R&D.