
Abstract
Background:
By combining existing Global Burden of Disease (GBD) data with the economic conditions of different regions, we can better understand disease trends and make more accurate estimations, facilitating effective public health interventions. Medical institutions can consequently allocate resources more efficiently. For patients, this helps lower disease risk and reduce the overall disease burden in affected areas.
Methods:
We analyzed health patterns in 204 countries using GBD 2021 methodologies and conducted separate analyses of disease burden in China and worldwide. We estimated incidence, prevalence, and years lived with disability (YLDs). We further assessed disease status by incorporating Socio-Demographic Index (SDI) values. In addition, we used Mendelian randomization to identify factors leading from falls to thoracic rib fractures, and we investigated the key protein involved in thoracic rib fractures through detection of 4907 plasma proteins.
Results:
From 1990 to 2021, the age-standardized incidence rate (ASIR) and age-standardized prevalence rate (ASPR) generally showed an upward trend, although male ASIR, and ASPR displayed a slight decline. In China, however, ASIR and ASPR reached a turning point in 2000, dipped in 2005, then trended upward again. Morbidity and prevalence were negatively correlated with SDI. Based on Mendelian randomization analyses, falls leading to thoracic rib fractures were linked to education level and osteoporosis. Moreover, HAMP was identified as the key protein in thoracic rib fractures.
Conclusion:
As global populations age, analyzing the global burden of thoracic rib fractures caused by falls from 1990 to 2021 can help guide the development of effective public health prevention strategies and optimize the allocation of existing medical resources.
Introduction
This study provides a comprehensive analysis of the global burden of thoracic rib fractures resulting from falls. Demographic aging poses a significant challenge for developed societies, as the proportion of older adults continues to rise. Advanced age is a high-risk factor associated with multiple morbidities, including falls that lead to various disease outbreaks. 1 Among the elderly, falls are the primary injury mechanism and a major cause of severe trauma. Individuals aged 75 years and older will soon constitute the largest segment of patients experiencing major trauma, with rib fractures occurring in approximately 10% of these cases—often resulting in considerable morbidity. About one-third of rib fracture complications involve pneumothorax, followed by hemothorax, pulmonary contusion, and flail chest. Younger individuals frequently lack awareness of fall prevention due to limited maturity, while many working-age adults face occupational fall risks. Older adults may be unaware of or deny their susceptibility to falls due to underlying health conditions. 2
Studies based on the Global Burden of Disease (GBD) offer important advantages, as they use consistent estimates, analytical methods, and model specifications over the same observation periods, facilitating cross-regional and international comparisons. 3 Furthermore, socio-economic characteristics of a region or country are critical indicators for evaluating disease burden. Leveraging 2021 GBD database data, this study aims to (1) quantify and compare the burden of fall-related sternal rib fractures in China and worldwide, stratified by gender, age, and region; (2) examine the trends in disease burden from 1990 to 2021; and (3) elucidate the relationship between falls and thoracic rib fractures by incorporating social and economic factors. The findings will help inform the development of public health strategies.
Materials and Methods
Data Sources
Data on falls resulting in chest and rib fractures were obtained from the GHDx (Global Health Data Exchange) query tool (https://vizhub.healthdata.org/gbd-results/).4 -6 These data included incidence and prevalence rates, enabling the estimation of age-standardized incidence (ASIR) and prevalence (ASPR) for fall-related sternal rib fractures across 21 regions and 204 countries from 1990 to 2021.7 -9 The Socio-Demographic Index (SDI) is a regional development indicator based on the average educational attainment of individuals aged 15 years and older, the total fertility rate among those under age 25, and per capita income. A higher SDI value corresponds to a higher socio-economic level. Incorporating SDI and age helps further clarify the health losses associated with fall-related chest rib fractures.
Joinpoint Regression Analysis
The Joinpoint regression model is a widely used linear statistical approach for analyzing temporal changes in disease trends, particularly for fall-induced sternal rib fractures in this study. By identifying specific points (joinpoints) where the slope of the trend changes significantly, it provides a more refined view of how disease burden evolves over time. The Grid Search Method (GSM) and Monte Carlo Permutation Test were employed to optimize the model, while Bonferroni correction helped maintain the overall asymptotic significance level. 10 The model outputs include the Annual Percent Change (APC), calculated within each segment defined by these joinpoints. The analysis starts with the minimum number of joinpoints, and additional joinpoints are tested sequentially to confirm their statistical significance. 11 Through this approach, the Joinpoint regression model ensures that every detected inflection point accurately reflects a real trend shift in the data.
Age-Period-Cohort Analysis
The Age-Period-Cohort (APC) model is a valuable tool for examining temporal trends in disease incidence and disentangling the influences of age, calendar period, and birth cohort on fall-induced sternal rib fractures. In this study, incidence rates were computed both over 5-year intervals and as cumulative incidence for different age groups, followed by model fitting using the Epi package. 12
Within the APC framework, the age effect typically represents the biological and physiological changes occurring at different life stages, making age the most critical factor for understanding the risk of fall-induced fractures. The period effect captures changes that occur during specific periods, such as early detection programs or significant improvements in treatment that could alter the disease incidence or severity. Finally, the cohort effect reflects the influence of varying exposures to risk factors across different birth cohorts, where shifts in lifestyle or environmental factors can lead to distinct differences in disease incidence over time. 13 Mathematically, the APC model can be expressed as: Y = log(M) = μ + αX₁ + βX₂ + γX₃ + ε where Y is the log-transformed incidence, M is the observed incidence, X₁, X₂, and X₃ represent the age, period, and cohort groupings, respectively. The parameters α, β, and γ correspond to the age, period, and cohort effects, μ is the intercept, and ε is the random error term assumed to follow a normal distribution. 14 By jointly modeling these 3 effects, the APC approach offers a nuanced view of how age, temporal trends, and generational changes all contribute to the burden of fall-induced sternal rib fractures.
Decomposition Analysis
Disaggregated analysis separately examines the impacts of population growth, shifts in age structure, and changes in disease trends on the overall number of patients. By parsing out these components, researchers can determine the unique contribution of each factor, thereby gaining a clearer understanding of how they collectively shape the disease burden. This detailed perspective is essential for informed public health planning, enabling targeted interventions and more effective resource allocation. 15
Prediction of Disease Development
The ARIMA (p, d, q) model was employed to project the incidence and prevalence of fall-induced rib fractures from 2021 to 2036, where p represents the order of autoregression, d is the degree of differencing, and q is the order of the moving average. 16 This approach accounts for both past observations and linear dependencies over time, enabling a more reliable prediction of future disease trends.
Additionally, frontier analysis was performed to establish benchmarks for the burden of fall-induced rib fractures. By incorporating Years Lived with Disability (YLDs) and the Socio-Demographic Index (SDI), “effective differences” were calculated for each country. 17 Statistical significance was defined as a 2-tailed P-value < .05. Since this study focuses on the long-term trend of the disease burden of thoracic and rib fractures in the world and China, we selected GBD data from 1990 to 2021 to systematically analyze the incidence rate, prevalence, and YLDs.
Mendelian Randomization
Independently from GBD data analysis, we utilized large-scale plasma proteomics screening combined with Mendelian randomization (MR) method and found that HAMP was significantly downregulated in fracture patients, suggesting that its role in bone metabolism and thoracic rib fractures deserves further investigation. All traits were obtained from the IEU Open GWAS project (https://gwas.mrcieu.ac.uk/). HAMP protein data comes from the FinnGen project (Finnish database). The pQTL data set, encompassing 4907 plasma proteins, was derived from 35 559 Icelandic individuals through deCODE genetics. Mendelian Randomization (MR) analysis was then conducted to identify key proteins associated with the risk of rib and sternum fractures (9995 cases; 395 649 controls).18,19 To ensure robust and independent findings, the following screening criteria were applied: P < 5 × 10−8, R2 < .01, and a clumping distance of 10 000 kb. Moreover, we performed an additional functional validation to clarify the role of HAMP, also known as hepcidin, in bone metabolism. Our Mendelian Randomization (MR) approach indicated that lower HAMP expression might correlate with reduced iron regulation, subsequently affecting osteoclast activity and bone microarchitecture.
Results
Time Trends in Disease Burden
To gain insight into the global burden of chest and rib fractures caused by falls, we examined both their time trends and sex-specific differences. In China, incidence and prevalence showed a decline from 2002 to 2005 (Figure 1A and B). In contrast, worldwide trends from 1990 to 2021 indicate a rise in overall incidence and prevalence, though in some intervals incidence showed a slight downturn (Figure 1C and D). When stratifying by 5-year age groups, both China and global data revealed that incidence and prevalence escalate notably with advancing age. Notably, age 70 emerged as a pivotal threshold, with a relatively modest increase observed prior to 70 and a rapid surge thereafter (Figure 1E-H).20,21

Trends of ASIR and ASPR in both sexes. (A) In China, ASIR for both sexes rose before 2000, declined before 2005, and rebounded thereafter. (B) Similarly, ASPR in China increased before 2000, dipped before 2005, then resurged after 2005. (C) Globally, the incidence among both sexes is increasing, yet ASIR continues to decline. (D) Worldwide prevalence is on the rise, whereas ASPR remains on a downward trajectory. (E) In China, incidence among individuals aged over 70 has grown in both sexes. (F) Likewise, prevalence among those over 70 has increased in both sexes in China. (G) Globally, incidence among individuals over 70 has also risen. (H) Worldwide, prevalence among those over 70 has similarly increased.
Disease Burden by Age and Gender
In 1990, disease incidence among men in both China and globally was primarily concentrated in younger age groups, while prevalence was notably higher in middle-aged men. By contrast, the incidence among women in China also centered on younger individuals, whereas globally, female incidence was more evenly distributed. Meanwhile, female prevalence in China showed a relatively balanced distribution, compared to the global landscape where prevalence was highest among older women (Figure 2A-D). By 2021, disease incidence and prevalence in China and worldwide indicated that men were predominantly affected in middle and older age groups, whereas women were mostly affected in later age groups (Figure 2E-H). These findings suggest that the disease is increasingly shifting toward older populations in China. Furthermore, as China’s economy has developed, the underlying causes of these fractures appear to have evolved.22,23

Differences in disease burden by age group. (A) In 1990 China, the highest incidence was observed among individuals aged 20 to 24. (B) In 1990 China, prevalence peaked in men aged 35 to 39 and in women aged 65 to 69. (C) In 1990 worldwide, men experienced their highest incidence at ages 20 to 24, while women peaked at 75 to 79. (D) In 1990 worldwide, men’s prevalence was highest at ages 55 to 59, while women peaked at 75 to 79. (E) In 2021 China, the largest incidence for men occurred at 30 to 34, while it was 80 to 84 for women. (F) In 2021 China, men’s prevalence was highest at 55 to 59, whereas women’s incidence peaked at 65 to 69. (G) In 2021 globally, men showed the largest incidence at ages 30 to 34, whereas women’s incidence peaked at 80 to 84. (H) In 2021 globally, men’s prevalence was highest at 65 to 69, and women’s incidence was highest at 80 to 84.
Joinpoint Regression
According to the Joinpoint regression model, China’s age-standardized incidence rate (ASIR) demonstrated a declining trend from 2001 to 2005, with female, and male annual percent changes (APCs) of −8.35 and −7.73, respectively (Figure 3A and B, Supplemental Figure S1A). Between 2010 and 2021, however, the ASIR rebounded markedly (female APC = 5.41; male APC = 5.24). In contrast, the global ASIR showed an overall downward trajectory (Figure 3C and D, Supplemental Figure S1B). A similar pattern was observed in China’s age-standardized prevalence rate (ASPR): it declined from 2001 to 2005 (female APC = −8.9; male APC = −7.73) and then rose significantly between 2010 and 2021 (female APC = 5.21; male APC = 5.13; Figure 3E and F, Supplemental Figure S1C). Meanwhile, the global ASPR continued to decline (Figure 3G and H, S1D). 24

Joinpoint analysis of ASIR and ASPR (1990-2021) in China and globally. (A) For Chinese women, the ASIR progressed through 4 intervals: 1990 to 2001 (APC = +0.75, P < .05), 2001 to 2005 (APC = −8.35, P < .05), 2005 to 2010 (APC = +1.27), and 2010 to 2021 (APC = +5.41, P < .05). (B) Among Chinese men, the ASIR showed 4 intervals: 1990 to 2001 (APC = +0.49, P < .05), 2001 to 2005 (APC = −7.18, P < .05), 2005 to 2010 (APC = +1.07), and 2010 to 2021 (APC = +5.24, P < .05). (C) For women globally, the ASIR was subdivided into 6 intervals: 1990 to 1994 (APC = −0.44, P < .05), 1994 to 2000 (APC = −0.08), 2000 to 2005 (APC = −0.79, P < .05), 2005 to 2010 (APC = −0.01), 2010 to 2018 (APC = −0.82, P < .05), and 2018 to 2021 (APC = −0.23, P < .05). (D) Among men worldwide, the ASIR showed 6 distinct segments: 1990 to 2000 (APC = −0.35, P < .05), 2000 to 2005 (APC = −1.08, P < .05), 2005 to 2010 (APC = −0.58, P < .05), 2010 to 2014 (APC = −1.24, P < .05), 2014 to 2018 (APC = −0.83, P < .05), and 2018 to 2021 (APC = −0.03). (E) For Chinese women, the ASPR was split into 4 intervals: 1990 to 2001 (APC = +0.47, P < .05), 2001 to 2005 (APC = −8.90, P < .05), 2005 to 2010 (APC =+0.82), and 2010 to 2021 (APC = +5.21, P < .05). (F) For Chinese men, the ASIR progressed through 4 intervals: 1990 to 2001 (APC = +0.29, P < .05), 2001 to 2005 (APC = −7.73, P < .05), 2005 to 2010 (APC = +0.49), and 2010 to 2021 (APC = +5.13, P < .05). (G) Among women globally, the ASPR included 6 phases: 1990 to 1993 (APC = −0.42, P < .05), 1993 to 2000 (APC = −0.20, P < .05), 2000 to 2005 (APC = −0.83, P < .05), 2005 to 2010 (APC = −0.13, P < .05), 2010 to 2017 (APC = −1.10, P < .05), and 2017 to 2021 (APC = −0.38, P < .05). (H) Finally, for men worldwide, the ASPR was subdivided into 6 periods: 1990 to 2000 (APC = −0.44, P < .05), 2000 to 2005 (APC = −1.18, P < .05), 2005 to 2010 (APC = −0.76, P < .05), 2010 to 2014 (APC = −1.53, P < .05), 2014 to 2018 (APC = −0.97, P < .05), and 2018 to 2021 (APC = −0.00).
Influence of Age, Period, and Cohort on Incidence
In China, the ratio of long versus cross relative risks (RR) rose with advancing age, whereas globally it showed a decline. The remaining indicators closely mirrored global trends (Figure 4A and B). Regarding morbidity and mortality by age in 1992, 2002, and 2012, the incidence in China increased sharply after age 70, whereas globally, it rose more markedly after age 60. Incidence rates climbed over time in almost all age groups, with the highest levels observed among older individuals. Additionally, birth cohort data indicated a strong correlation between increasing age and higher incidence, suggesting that more individuals are diagnosed as they age. Overall incidence patterns in China and worldwide were largely comparable (Figure 5A and B). 25

APC (Age-Period-Cohort) analysis the age effect is illustrated by both the longitudinal and cross-sectional age curves. Age deviations integrate these 2 curves (represented as Long vs Cross RR) and capture any non-linear effects, akin to observing linear age trends. The period effect is shown via Fitted Temporal Trends, Period RR, and Period deviations. Fitted Temporal Trends depict incidence or mortality for a reference cohort after deviations are corrected—similar to age-standardized rates. Period deviations combine these Fitted Temporal Trends with any non-linear influences identified by Period RR, approximating linear trends across different time periods. Finally, the birth cohort effect is represented by Cohort RR and Local Drifts, with cohort deviations integrating non-linear aspects of Cohort RR and local drift, again resembling linear trends. (A) Among the same birth cohort in China, mortality gradually increases with age. Based on the Period RR, mortality has risen more slowly in recent years. (B) Globally, mortality also increases with age within the same birth cohort. However, the Period RR indicates a decline overall. Specifically, mortality rises for individuals born before 1930, then gradually decreases for those born after 1930.
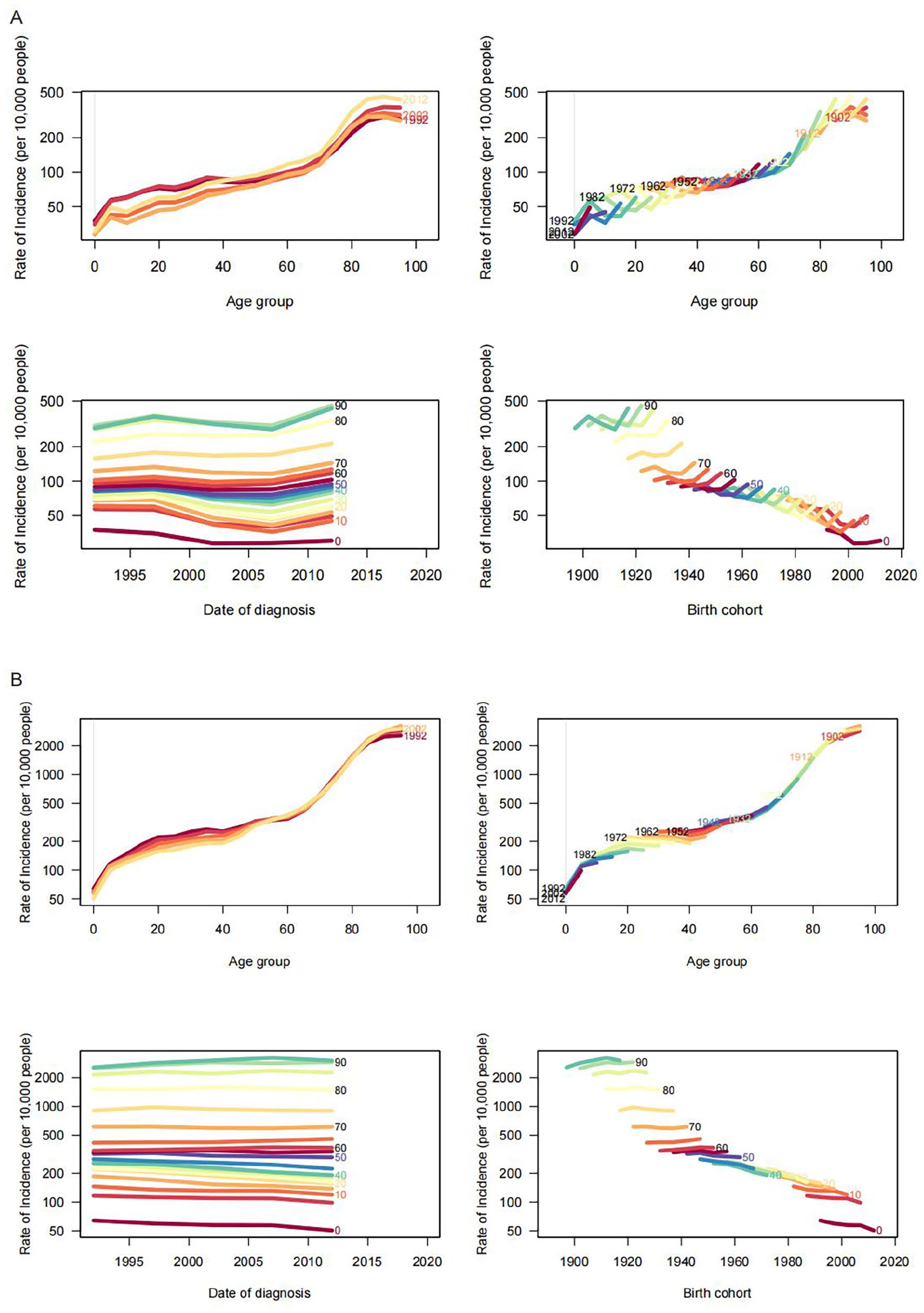
Age-specific APC analysis. This figure presents age-specific incidence data across varying time periods, birth cohorts, and age groups. Each row covers a 10-year span of age-specific incidence. (A) Thoracic rib fracture incidence from falls in China. (B) Thoracic rib fracture incidence from falls globally.
Changes in Population Age Structure, Growth and Epidemiological Trends
The decomposition analysis visually highlights the shifting factors driving sternal rib fractures from driving-related falls between 1900 and 2021. In China, age-standardized incidence (ASIR) and prevalence (ASPR) suggest that changes in disease epidemiology are the main contributors, whereas on the global scale, population size accounts for a greater share of the burden. Meanwhile, Chinese YLDs point to population aging as a key driver, while global YLDs show that population size again plays a more prominent role (Figure 6A-F).

Decomposition of disease drivers. (A) In China, epidemiological changes are the largest contributor to ASIR. (B) Epidemiological changes also dominate ASPR in China. (C) Aging plays the most significant role in China’s YLDs. (D) Globally, population shifts emerge as the primary driver of ASIR. (E) For global ASPR, epidemiological changes account for the largest share. (F) Similarly, epidemiological changes remain the major factor influencing global YLDs.
Future Development Trend
Using the ARIMA predictive model, researchers forecast disease trends for the next 15 years to better understand the burden of disease and guide regional responses. In China, the age-standardized incidence rate (ASIR) for men is expected to decline notably, whereas women will likely see a downward trend until 2031, followed by an upswing (Figure 7A and B). Globally, both men and women show a slower, steady decline in ASIR (Figure 7C and D). For age-standardized prevalence rates (ASPR), Chinese men and women are projected to experience a decrease up to 2031, then an increase thereafter (Figure 7E and F), while the global ASPR for both sexes continues to trend downward (Figure 7G and H). 26

Projected Disease Trends Over the Next 15 years (A) ASIR among men in China. (B) ASIR among women in China. (C) ASIR among men globally. (D) ASIR among women globally. (E) ASPR among men in China. (F) ASPR among women in China. (G) ASPR among men globally. (H) ASPR among men globally.
ASIR, ASPR, and Frontier Analysis by Region
High-income regions—including Australia, high-income Asia, North America, and Western Europe—exhibit elevated age-standardized incidence (ASIR) and prevalence (ASPR), likely reflecting the impact of advanced industrial development, where well-established industrial conditions can exacerbate chest rib injuries resulting from falls (Figure 8A-D). Frontier analyses further reveal that countries with higher Socio-demographic Index (SDI) scores are better equipped to handle disease burdens and improve outcomes in the future (Figure 8E and F). 27

Disease burden by region. (A) ASIR across 22 regions. (B) ASPR across 22 regions. (C) ASIR across 204 countries. (D) ASPR across 204 countries. (E and F) Frontier analysis.
Disease Causation and Plasma Protein Prediction
Using MR analysis, we further investigated the underlying factors contributing to the disease burden. Results indicate that education is a critical component: in highly industrialized regions with elevated SDI, education proves pivotal in mitigating fall risk and enhancing individual protective measures (Figure 9A). Personal attributes also play a substantial role, with osteoporosis notably increasing the likelihood of sustaining chest-rib fractures from falls (Figure 9B). Among the 4907 plasma proteins evaluated, HAMP emerged as a key regulator, as its expression decreased significantly following disease onset (Figure 9C). Functional enrichment revealed that TGFβ-related pathways are closely involved in the disease process (Figure 9D and E).28 -30 HAMP was identified as a key protein in thoracic rib fractures, showing significantly decreased expression following disease onset, suggesting its regulatory functions in bone remodeling, and iron homeostasis.

MR Analysis (A) A causal relationship between education and fall-induced sternorib fractures. (B) A causal relationship between osteoporosis and fall-induced thoracic rib fractures. (C) Screening of 4907 plasma proteins highlights key proteins involved in fall-related rib fractures. (D) GO enrichment analysis of key proteins. (E) KEGG enrichment analysis of key proteins.
Discussion
The age-standardized incidence (ASIR) and prevalence (ASPR) rates for Chinese men and women have shown a marked decline since 2000, whereas global rates for women remained relatively unchanged and those for men showed only a gradual decrease. This suggests that while China’s social development advanced rapidly, global progress continued at a steadier pace. Over the last 2 decades, China’s rapid development appears to have significantly shifted the age distribution of thoracic rib fractures caused by falls, implying that the factors triggering these falls have also changed markedly against the backdrop of accelerated social growth.
Compared with 1990, when young and middle-aged adults predominated among patients in China, older adults now make up a higher proportion of cases in 2021—a clear sign of population aging. Beyond societal advancements, expanded access to education, and economic growth, many older individuals have underlying health conditions that further increase their vulnerability. Although most rib fractures result from direct trauma to the chest wall, even minor trauma can lead to a single rib fracture in older adults. 31 Aging also diminishes physical, cognitive, and sensory capacities, and factors such as reduced physical activity, environmental hazards, cardiovascular disease, and mental health issues can all lead to falls. 32
Raising awareness of fall risks—through education and personal risk assessment—can help individuals adopt safer lifestyles and mitigate the burden of rib fractures. Educating people about the possibility of sustaining chest and rib fractures from falls allows us to evaluate both the effectiveness and limitations of existing prevention measures and adapt these strategies to minimize such injuries. Bone mineral density (BMD) is a known risk factor for fractures; lower BMD increases the likelihood of experiencing high-energy trauma leading to fractures. Early identification of osteoporosis is therefore essential to prevent rib and sternal fractures. 33 TGF-β is critical for bone-resorption processes and bone coupling, 34 and TGF-β–driven wound healing involves a complex cascade of cell migration and inflammation, fibroblast proliferation, granulation, extracellular matrix deposition, and scar tissue remodeling. 35 HAMP (hepcidin) is a key regulator of iron metabolism, primarily produced by the liver. It binds to ferroportin, promoting its internalization and degradation, thereby reducing iron release into the bloodstream. High hepcidin levels, often triggered by iron overload or inflammation, limit free iron availability. Conversely, low hepcidin levels during deficiency enhance iron release. Hepcidin also plays a critical role in innate immunity by restricting iron access to pathogens. Abnormal hepcidin regulation is linked to conditions such as hereditary hemochromatosis, anemia of chronic disease, and iron overload or deficiency. Its dysregulation significantly impacts both healthy iron homeostasis and disease states. These findings underscore HAMP’s potential as a therapeutic or diagnostic marker for fall-related thoracic rib fractures. HAMP’s role in iron homeostasis may influence osteoclast activity and fracture healing; thus, interventions targeting HAMP or its downstream pathways could offer novel strategies to prevent or mitigate rib fractures, especially among older adults or those with osteoporosis.
This study has several limitations. First, insufficient data may affect the accuracy of the burden estimates, though improvements in data reporting over time should lessen this effect. Second, the disease burden might be underestimated in less developed regions, whose limited diagnostic and management capacities also affect data reliability. 36 Despite these constraints, our research examines shifts in the global and Chinese burden of rib fractures caused by falls from 1990 to 2021, explores their underlying causes, and employs MR to identify key proteins involved—laying the groundwork for future investigations. In low- or middle-income countries constrained by limited resources, preventive care is crucial. As such, policymakers can combine public health education with robust, preventive healthcare interventions to significantly reduce the burden of thoracic rib fractures triggered by falls.
Supplemental Material
sj-docx-1-bec-10.1177_11795972251350223 – Supplemental material for Rib and Sternum Fractures From Falls: Global Burden of Disease and Predictions
Supplemental material, sj-docx-1-bec-10.1177_11795972251350223 for Rib and Sternum Fractures From Falls: Global Burden of Disease and Predictions by Zhanghao Huang and Jun Zhu in Biomedical Engineering and Computational Biology
Supplemental Material
sj-jpg-2-bec-10.1177_11795972251350223 – Supplemental material for Rib and Sternum Fractures From Falls: Global Burden of Disease and Predictions
Supplemental material, sj-jpg-2-bec-10.1177_11795972251350223 for Rib and Sternum Fractures From Falls: Global Burden of Disease and Predictions by Zhanghao Huang and Jun Zhu in Biomedical Engineering and Computational Biology
Footnotes
Abbreviation
ASIR: age-standardized incidence rate
ASPR: age-standardized prevalence rate
GBD: Global Burden of Disease
YLDs: years lived with disabilities
SDI: socio-demographic index
Ethical Considerations
Not applicable.
Author Contributions
ZH: Data curation, Investigation, Software, Methodology, Project administration, Resources, Validation, Writing—original draft, Writing—review and editing. JZ: Resources, Writing—original draft, Conceptualization, supervision, visualization, Data curation, Software, Funding aquisition.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Postgraduate Research & Practice Program of Jiangsu Province (KYCX23_3427).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available on request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.