
Abstract
Retroclival epidural hematoma (EDH) is a rare form of intracranial hemorrhage located between the clivus and the dura mater, predominantly affecting pediatric patients due to the anatomical vulnerability of the craniocervical junction. This case report describes a 4-year-old boy involved in a motorcycle accident who presented with facial trauma and was found to have a retroclival EDH and multiple mandibular fractures. Despite the hematoma measuring 8.7 mm in thickness and 3 cc in volume, the patient remained neurologically intact with a Glasgow Coma Scale of 15. He underwent surgical repair for the mandibular fractures while the retroclival EDH was managed conservatively. The patient recovered fully without neurological deficits at follow-ups extending to 6 months. A comprehensive literature review reveals that retroclival EDH in children is commonly associated with high-energy trauma such as motor vehicle accidents and often results from tectorial membrane stripping injury. While clinical presentations vary, many cases, like the one described, show minimal neurological signs despite the presence of significant hematomas, emphasizing the importance of high clinical suspicion and appropriate neuroimaging. Computed tomography is the initial diagnostic tool, but magnetic resonance imaging is superior for identifying associated ligamentous injuries and differentiating from subdural hematomas. Most pediatric retroclival EDH cases are managed conservatively with excellent outcomes, reserving surgical intervention for cases involving brainstem compression or craniocervical instability. This report reinforces the favorable prognosis of isolated retroclival EDH in neurologically stable pediatric patients and underscores the critical role of imaging and clinical vigilance in trauma assessment.
Introduction
Retroclival epidural hematoma (EDH) is an uncommon form of intracranial hemorrhage, distinguished by its location between the clivus and the dura mater. While retroclival EDH has been documented in adults, often linked to trauma or spontaneous causes such as coagulopathy or pituitary apoplexy, it is predominantly recognized as a pediatric pathology. 1 The higher incidence in children is attributed to the unique anatomical and biomechanical characteristics of the developing craniocervical junction (CCJ), including greater ligamentous laxity, a relatively larger head-to-body ratio, and horizontally oriented occipital condyles, which predispose this region to injury from hyperflexion or hyperextension mechanisms. 2 Motor vehicle accidents (MVAs) are the most frequently reported cause of traumatic retroclival EDH in the pediatric population. 3 The pathophysiology of pediatric retroclival EDH is often linked to the stripping of the tectorial membrane from the clivus, leading to hemorrhage from the basilar venous plexus or associated small bridging veins. 1 Clinically, retroclival EDH can present with a wide spectrum of symptoms, from neck pain and minor neurological signs to severe deficits including cranial nerve palsies—most commonly affecting the abducens nerve—and altered consciousness. However, a benign neurological status, as seen in our patient, can occur despite the presence of a significant hematoma, potentially leading to underdiagnosis. Diagnosis relies on neuroimaging, with computed tomography (CT) being the initial modality in acute trauma, and magnetic resonance imaging (MRI) offering superior delineation of the hematoma and associated soft tissue or ligamentous injuries. Conservative management is often successful for isolated retroclival EDH in clinically stable pediatric patients, leading to favorable outcomes.
This paper presents a case of a 4-year-old boy who sustained a traumatic retroclival EDH and multiple mandibular fractures following a motorcycle accident, managed conservatively with an excellent outcome. We also review the existing literature to discuss the nuances of this rare traumatic entity in the pediatric context.
Methods/Literature Search
A comprehensive literature search was undertaken to identify reported cases of retroclival epidural hematoma, with primary emphasis on the pediatric population and inclusion of adult cases for comparative purposes. Searches were conducted in PubMed, Scopus, and Google Scholar, encompassing all available years through May 2025. The search strategy employed combinations of the keywords “retroclival epidural hematoma,” “clivus hematoma,” “pediatric,” and “trauma.” Reference lists of all relevant publications were manually reviewed to capture additional cases. Eligibility criteria for the pediatric cohort included case reports, case series, and reviews describing retroclival epidural hematomas in patients aged ≤18 years with traumatic etiology confirmed by clinical history and imaging. Non-traumatic cases, non-English publications without accessible English abstracts, and reports lacking sufficient clinical or imaging details were excluded. For completeness, adult cases (>18 years) meeting similar clinical and imaging criteria were also compiled.
Reported Cases of Retroclival Epidural Hematoma in Pediatric Population
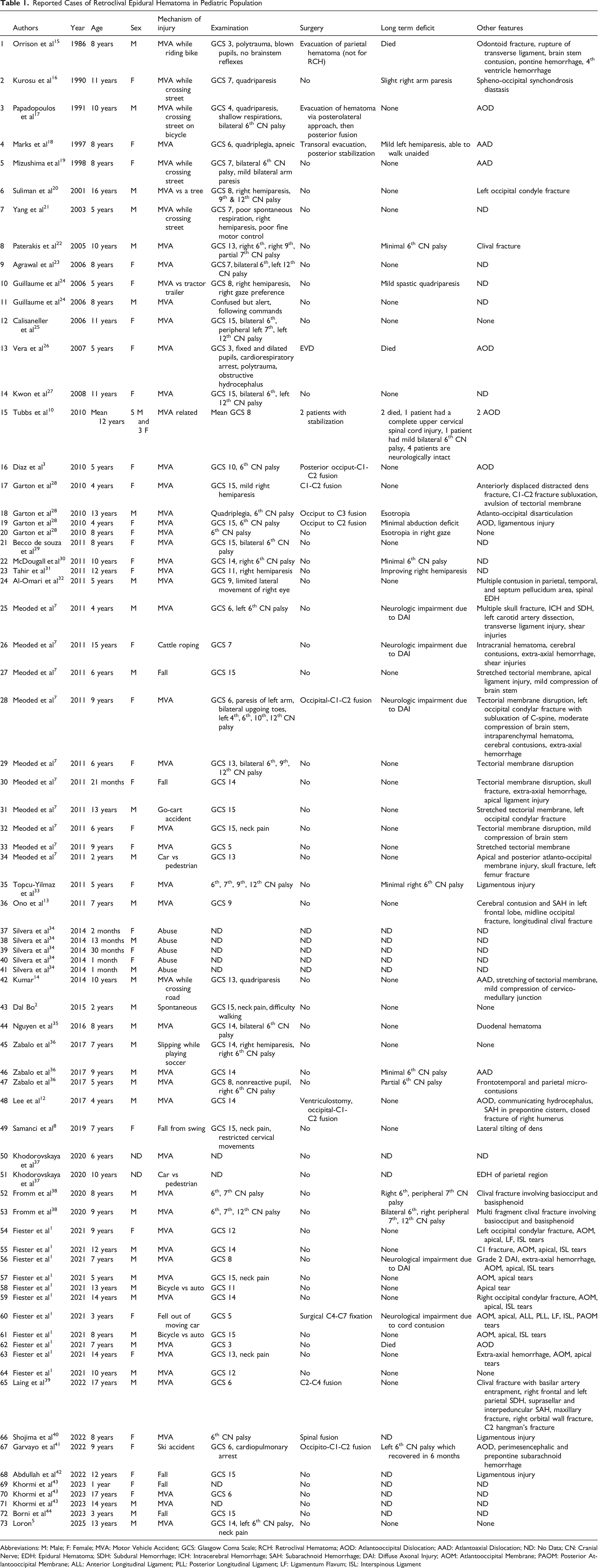
Abbreviations: M: Male; F: Female; MVA: Motor Vehicle Accident; GCS: Glasgow Coma Scale; RCH: Retroclival Hematoma; AOD: Atlantooccipital Dislocation; AAD: Atlantoaxial Dislocation; ND: No Data; CN: Cranial Nerve; EDH: Epidural Hematoma; SDH: Subdural Hemorrhage; ICH: Intracerebral Hemorrhage; SAH: Subarachnoid Hemorrhage; DAI: Diffuse Axonal Injury; AOM: Atlantooccipital Membrane; PAOM: Posterior Atlantooccipital Membrane; ALL: Anterior Longitudinal Ligament; PLL: Posterior Longitudinal Ligament; LF: Ligamentum Flavum; ISL: Interspinous Ligament
Reported Cases of Retroclival Epidural Hematoma in Adult Population

Abbreviations: M: Male; F: Female; MVA: Motor Vehicle Accident; GCS: Glasgow Coma Scale; RCH: Retroclival Hematoma; AOD: Atlantooccipital Dislocation; ND: No Data; CN: Cranial Nerve; EDH: Epidural Hematoma; SDH: Subdural Hemorrhage.
Case Presentation
A 4-year-old boy was brought by his family to the Emergency Department (ED) 8 hours after sustaining injuries in a traffic accident. The patient was a passenger on a motorcycle, not wearing a helmet, and was seated on his father’s lap, who was operating the motorcycle. The motorcycle collided with another motorcycle approaching from the opposite direction, causing the patient to be thrown forward, with his face impacting the asphalt first. According to the patient’s father, there was a loss of consciousness for less than 5 minutes, after which the patient regained consciousness. There were no reported episodes of vomiting, seizures, or discharge from the nose or ears.
Following stabilization of his airway, breathing, and circulation, the disability assessment revealed an initial Glasgow Coma Scale (GCS)
4
score of 15. His pupils were round, isochoric, equal in size at 3 mm/3 mm, and there was no lateralization. Physical examination of the facial area revealed multiple contusions accompanied by edema and crepitation in the mandibular region. A head CT scan showed a hyperdense lesion in the retroclival area, with a thickness of 8.7 mm and a volume of 3 cc (Figures 1C–E). Additionally, a 3D CT scan identified multiple fractures in the mandibular area (Figures 1A,B). Non-contrast Head CT Scan. (A, B) Anterior and Right Lateral Views of the 3D Reconstruction Show Multiple Mandibular Bone Fractures. (C) Axial View Reveals a Retroclival EDH (White Arrow). (D) Coronal View Shows the Retroclival EDH (White Arrow). (E) Sagittal View Demonstrates the Retroclival EDH (White Arrow)
The patient promptly underwent open reduction, repositioning, and internal fixation with miniplates for a left segmental parasymphysis mandibular fracture and a right corpus mandibular fracture, performed by the plastic surgery team. Conservative management was implemented for the retroclival EDH. The patient received symptomatic treatment, including intravenous analgesia with paracetamol 200 mg and fentanyl 100 mcg, and intravenous antiemetic ondansetron 15 mg. He was hospitalized for 5 days, during which no signs of increased intracranial pressure, such as restlessness, projectile vomiting, seizures, or a decline in consciousness, were observed. During follow-up assessments at 1 week, 3 months, and 6 months post-accident, the patient remained in stable condition and was able to perform daily activities effectively, with no identified deficits or limitations.
Discussion
Retroclival EDH is an uncommon yet significant type of intracranial hemorrhage, characterized by blood accumulation between the clivus and the dura mater. Its occurrence is notably rare, constituting a small fraction of all epidural hematomas (approximately 1.2%–12.9%) and posterior fossa epidural hematomas. While retroclival EDH can occur in adults, often secondary to trauma but also spontaneously due to factors like coagulopathy or pituitary apoplexy, it is predominantly observed in the pediatric population. This pediatric predilection is a consistent finding across multiple studies, including a systematic review by Loron et al 5 which identified 64 individual pediatric cases of posttraumatic clival/retroclival hematoma, and the narrative synthesis of 73 pediatric cases presented in Table 1. The presented case of a 4-year-old male aligns with this established demographic predisposition. Piccirilli et al 6 suggest that retroclival EDH are likely underdiagnosed in adults. A summary of reported adult cases of retroclival EDH is provided in Table 2. As our methodology was not systematic, these findings should be interpreted descriptively rather than as quantitative estimates of incidence or outcome.
Pathophysiology
The mechanism underlying retroclival EDH in children is closely linked to the unique anatomical and biomechanical properties of the pediatric craniocervical junction (CCJ). Children possess a relatively larger head-to-body ratio, weaker neck musculature, horizontally oriented and smaller occipital condyles, and increased ligamentous elasticity compared to adults. These factors contribute to a less stable CCJ, making it more susceptible to injury from hyperflexion or hyperextension forces, typically encountered in high-impact trauma such as motor vehicle accidents (MVAs). Review of pediatric cases, including those in Table 1, confirms MVAs as the most frequent cause. The patient in this report sustained injuries in a motorcycle accident, a common etiology for retroclival EDH. The reported face-first impact suggests a significant flexion or extension moment at the CCJ. Such forces can lead to the detachment or stripping of the tectorial membrane from the clivus. The tectorial membrane, the cranial extension of the posterior longitudinal ligament, is firmly attached to the clivus and incorporates the basilar venous plexus. Injury to this plexus, or tearing of small bridging veins between the dura and the clivus, is considered the primary source of hemorrhage in retroclival EDH. Fiester et al 1 strongly proposed that retroclival EDH in the pediatric population is a direct result of significant flexion-extension forces leading to a stripping injury of the tectorial membrane from the posterior clivus and subsequent tearing of the basilar venous plexus. All patients in their study who underwent cervical MRI after retroclival EDH identification on CT showed evidence of tectorial membrane stripping injury. Meoded et al 7 also highlighted that tectorial membrane disruption is a key factor in retroclival EDH formation, seen in 70% of their pediatric cases. While MRI was not performed in our case due to the patient’s stability and good GCS, the mechanism of injury aligns with this hypothesis. Although high-energy trauma is typical, low-energy injuries, such as a fall from a swing as reported by Samanci et al 8 or even minor trauma in adults as noted by Izumida et al 9 can also lead to retroclival EDH, emphasizing the vulnerability of this region, particularly in children.
Clinical Presentation
The clinical presentation of retroclival EDH can be varied and may not always correlate directly with the hematoma size or initial GCS scores. Patients might present with symptoms ranging from neck pain, headache, and vomiting to severe neurological deficits such as cranial nerve palsies (most commonly the sixth cranial nerve), hemiparesis, quadriparesis, or altered levels of consciousness. Our patient presented with an initial GCS of 15 and a brief loss of consciousness (<5 minutes), without vomiting, seizures, or focal neurological deficits other than those attributable to his significant mandibular fractures. This relatively benign neurological status despite an 8.7 mm thick blood highlights the potential for retroclival EDH to be initially overlooked if not specifically sought, especially in polytrauma settings where other injuries might be more apparent. Table 1 shows a wide range of GCS scores in pediatric retroclival EDH cases, from 3 to 15. The literature supports that retroclival EDH can be underdiagnosed on initial CT scans. Loron et al 5 found that while higher initial GCS scores correlated with general neurological recovery (P < 0.05), no significant difference was found in GCS scores between patients with complete and those with incomplete abducens nerve recovery. The incidence of abducens nerve palsy in the setting of posttraumatic retroclival EDH was reported as 40% by Loron et al 5 and 42.6% by Samanci et al 8 ; this is a common finding in the pediatric cases summarized in Table 1.
Imaging Modality
CT scan is the primary imaging modality for acute head trauma and can reveal retroclival EDH as a hyperdense, biconvex collection anterior to the brainstem and posterior to the clivus. The hematoma in our patient measured 8.7 mm in thickness with a volume of 3 cc. Fiester et al 1 reported a mean anteroposterior dimension of 4.4 mm for retroclival EDH in their series. MRI is often recommended for better delineation of the hematoma, associated ligamentous injuries (particularly tectorial membrane injury), and differentiation from retroclival subdural hematoma. An EDH is typically limited superiorly by the mid-clivus and inferiorly by the mid-body of C2 due to tectorial membrane attachments; subdural hematomas can distribute more rostrally or caudally. Meoded et al 7 found MRI to be more sensitive than CT for tectorial membrane injuries and EDH, identifying retroclival EDH in all 8 children who had MRI vs 9/10 on CT. Samanci et al 8 also noted that retroclival EDH were not easily detected on CT scans and were often identified on MRI only. Piccirilli et al 6 also emphasized MRI’s superiority for identifying these lesions in adults and recommended sagittal reconstructions if using CT. It should be noted that MRI was not performed in our patient due to clinical stability and absence of focal neurological deficits. Nonetheless, this limitation precludes definitive exclusion of ligamentous injury, which is a recognized association with retroclival epidural hematoma.
Management
Conservative management is the mainstay of treatment for most retroclival EDH cases, particularly in neurologically stable patients or those with mild, non-progressive symptoms. This approach typically involves cervical spine immobilization and close neurological observation. Our patient was managed conservatively for the retroclival EDH, with symptomatic treatment for pain and antiemetics, and showed excellent recovery without neurological sequelae at 6-month follow-up. This outcome is consistent with the generally good prognosis reported for conservatively managed pediatric retroclival EDH (Table 1). Steroids, such as methylprednisolone, have been mentioned in the conservative management of some adult and pediatric cases. Surgical intervention, such as hematoma evacuation or craniocervical stabilization, is reserved for cases with significant brainstem compression, progressive neurological deterioration, hydrocephalus, or associated craniocervical instability. For instance, Tubbs et al 10 reported surgical fusion in 2 of their 8 cases of retroclival EDH, both of whom had associated atlanto-occipital dislocation. Marks et al 11 described transoral evacuation in a child with C1-C2 dislocation. Loron et al 5 noted that hematoma evacuation was rare, occurring in only 2 of 64 reviewed cases, while spinal fixation was more common when indicated by associated instability. Lee et al 12 reported a pediatric case where AOD and resulting hydrocephalus necessitated ventriculostomy and occipital-cervical fusion. The data in Table 1 shows that the majority of pediatric patients were managed conservatively.
Associated Injuries
Retroclival EDH can be associated with other significant injuries, including skull base fractures (clival, occipital condyle), cervical spine fractures/dislocations (AOD, AAD), and ligamentous injuries. The presence of multiple mandibular fractures in our patient underscores the severity of the traumatic impact to the craniofacial region. While Fiester et al 1 noted that none of their 11 pediatric patients with retroclival EDH had a clival fracture, and only six had concomitant occipital condylar or cervical spine fractures, the forces required to fracture the mandible can certainly be transmitted to the CCJ. Ono discussed longitudinal clival fractures, often caused by severe head trauma, which can coexist with retroclival EDH. 13 Lee et al 12 described the triad of AOD, retroclival hematoma, and hydrocephalus. Complications such as hyponatremia and delayed traumatic intracerebral hematoma have been reported in adult traumatic retroclival EDH. Therefore, a high index of suspicion for retroclival EDH and associated CCJ ligamentous injuries should be maintained in pediatric patients presenting with significant facial trauma, even if the initial neurological examination is unremarkable. The recommendation by Fiester et al and Kumar et al 14 to perform cervical MRI in pediatric patients with posttraumatic retroclival EDH on initial head CT to evaluate the integrity of the tectorial membrane and other craniocervical ligaments is pertinent, although in our case, the benign clinical course did not prompt this further investigation.
Prognosis and Outcome
The prognosis for pediatric retroclival EDH is generally good, especially with conservative management. Spontaneous resolution of the hematoma typically occurs within weeks to months. Izumida et al 9 reported resolution in an adult by day 8. Loron et al 5 reported a median follow-up of approximately 9 weeks for complete neurological recovery in their systematic review. The rate of complete recovery of abducens nerve function was 73% in the same review, with recovery often occurring within weeks to 14 months. Our patient’s full recovery aligns with these favorable outcomes, as does the majority of cases detailed in Table 1. To our knowledge, this is among the few reported pediatric cases of retroclival epidural hematoma associated with concurrent mandibular fractures. This case reinforces that conservative management can yield favorable outcomes in neurologically intact patients, while also underscoring the importance of considering retroclival EDH in the setting of significant craniofacial trauma.
Conclusion
Retroclival EDH, though rare, is an important diagnostic consideration in pediatric trauma, especially following high-energy impacts. Literature and the presented case highlight its predilection for children, common traumatic etiology (often MVAs), and link to craniocervical junction biomechanics, frequently involving tectorial membrane injury. While clinical presentations vary, and initial GCS may be high, neuroimaging (CT and particularly MRI) is crucial for diagnosis and assessing associated injuries. Our case, showing full recovery with conservative treatment for retroclival EDH despite significant mandibular fractures, aligns with the generally favorable prognosis for isolated retroclival EDH in stable pediatric patients. A high index of suspicion and thorough evaluation for associated craniocervical injuries remain paramount.
Footnotes
Acknowledgements
The authors thank the Department of Neurosurgery at their institution for support in the preparation of this manuscript.
Consent for Participate
Written informed consent for participation was obtained from the patient’s legal guardian.
Consent for Publication
Written informed consent for publication of this case report and accompanying images was obtained from the patient’s legal guardian. A copy of the consent form is available for review by the journal’s editorial office upon request.
Author Contributions
Christopher Lauren: Conceptualization, Data curation, Formal analysis, Project administration, Resources, Supervision, Validation, Writing - original draft, Writing - review & editing. Ida Bagus Gede Adiguna Wibawa: Conceptualization, Project administration, Resources, Writing - original draft, Writing - review & editing. I Gusti Ketut Agung Surya Kencana: Conceptualization, Project administration, Resources, Writing - original draft, Writing - review & editing. Maria Monica: Conceptualization, Project administration, Resources, Writing - original draft, Writing - review & editing. Denny Japardi: Conceptualization, Project administration, Resources, Writing - original draft, Writing - review & editing. Bagus Dwiki Arya Dharma: Conceptualization, Project administration, Resources, Writing - original draft, Writing - review & editing. Joshua Sutikno: Conceptualization, Project administration, Resources, Writing - original draft, Writing - review & editing. Tiffany Tiffany: Conceptualization, Project administration, Resources, Writing - original draft, Writing - review & editing. Ian Adrianto Limansyah Conceptualization, Project administration, Resources, Writing - original draft, Writing - review & editing. Made Ratna Dewi: Conceptualization, Data curation, Formal analysis, Investigation, Project administration, Resources, Supervision, Validation, Visualization, Writing - original draft, Writing - review & editing. Made Gemma Daniswara Maliawan: Conceptualization, Project administration, Resources, Writing - original draft, Writing - review & editing. Tjokorda Gde Bagus Mahadewa: Conceptualization, Formal analysis, Investigation, Project administration, Resources, Supervision, Visualization, Writing - original draft, Writing - review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.