
Abstract
Background
Recently, the United States Food and Drug Administration (USFDA) approved viloxazine extended-release (ER) to manage attention-deficit hyperactivity disorder (ADHD) in pediatric patients of 6–17 years of age.
Objective
To perform a meta-analysis to determine the safety and efficacy of viloxazine ER in the management of ADHD.
Data Source and Methods
A literature search was performed through the databases Cochrane Library, PubMed, and clinicaltrials.gov, for a period from inception to August 2021, with the keywords: viloxazine, SPN-812, ADHD, and randomized clinical trials. The randomized controlled trials published in English language that analyzed the efficacy and safety were included. The risk of bias (RoB) was assessed by RoB tool. The outcomes included in this study were the proportion of patients with a 50% reduction in ADHD-Rating Scale-5 (ADHD-RS-5 responders) and improvement in CGI-I scale and the proportion of patients with at least one adverse event, the incidence of somnolence and Serious Adverse Events (SAEs).
Results
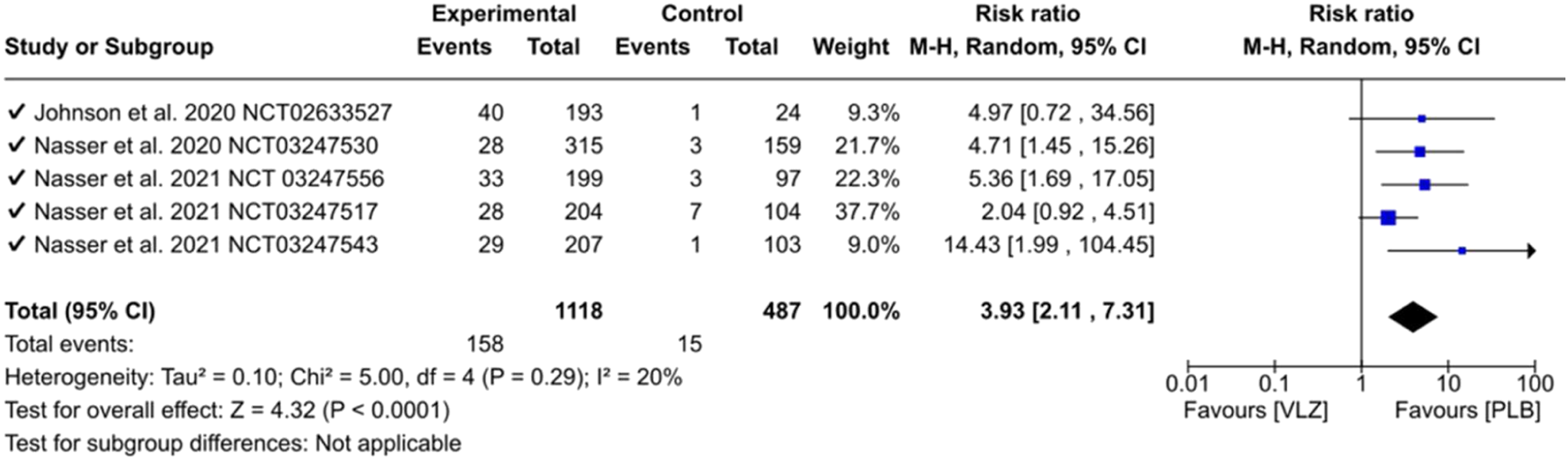
This meta-analysis includes 1605 patients from five randomized clinical trials; all of the trials were at low risk of bias. Viloxazine group had more ADHD-RS-5 responders as compared to placebo; RR = 1.62; 95% CI = 1.36-1.93; P = <.00001. Significantly higher number of patients showed improved CGI-I score; RR = 1.53; 95% CI = 1.32-1.78; P = <.00001. A higher proportion of patients was observed with at least one adverse event (RR = 1.52; 95% CI = 1.24-1.85; P = <.0001), and somnolence (RR = 3.93; 95% CI = 2.11-7.31; P = <.0001) in viloxazine group. The incidence of SAEs was more in viloxazine group (RR = 2.98; 95% CI = .67-13.3; P = .15).
Conclusions
Viloxazine was found to be significantly superior to placebo in both efficacy outcomes. Adverse events and somnolence were significantly more than the placebo. The incidence was SAEs was more in the viloxazine group but was not statistically significant.
Introduction
Attention-deficit hyperactivity disorder (ADHD) is a common neurological disorder in the pediatric population (2–17 years) and is characterized by a persistent and pervasive pattern of inattention and hyperactivity-impulsivity that interferes with functioning or development. 1 The etiology of ADHD is unclear. Among children and adolescents, ADHD is more common in males, with the sex ratio ranging from 2:1 to 10:1. 2 However the sexual predilection of ADHD remains controversial due to the underdiagnosis of ADHD in females. 3 Among school-age children, the prevalence of ADHD ranges from 3% to 10%. 4 In United States, 9.4% of children between 2 and 17 years of age were diagnosed with ADHD in 2016. 5 The worldwide prevalence of ADHD in children and adults is 5.29% and 2.5%, respectively. 6 The prevalence of ADHD in India ranges from 4.7% to 29.2%. 3 ADHD results in poor school performance and difficulty in maintaining the formal relationship with their peers and parents in children. Adolescents with ADHD often present as school dropouts or grade retention, and they are more often associated with substance abuse and earlier sexual engagement. Adults with ADHD often have poorer educational achievement, poor job performance, and emotional instability. They are more prone to traffic accidents, lawbreaking, and substance abuse. 7 The onset of ADHD usually occurs in early childhood, but the diagnosis is generally made in the school-age years. The diagnosis of ADHD is purely clinical supplemented by proper family, gestational, and developmental history. According to the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-V), diagnosis of ADHD in children (<17 years) is made when six or more symptoms are present in either the inattentive or hyperactive and impulsive domains, or both. DSM-5 further divides ADHD into three distinguished presentations, that is, inattentive, hyperactive and impulsive, or combined. 8
Treatment of ADHD involves behavioral therapy and pharmacological management. Behavioral therapy focuses on decreasing distractions and improving time management and organization skills. Pharmacological management encompasses two drug categories—stimulants (methylphenidate and amphetamine) and non-stimulants (ER guanfacine, ER clonidine, and atomoxetine). Stimulants are widely used and highly efficacious, and act faster, whereas non-stimulants are comparatively less efficacious and take much time for their onset of action. 9
When treated with stimulants as monotherapy, the response rate is usually 70%, and the response rate increases up to 90% when two stimulants are concomitantly used. The most common side effects include loss of appetite, sleep disturbances, and cardiovascular events such as hypertension and tachycardia. 10 The alternative approach of non-stimulant treatment is usually less effective. The most common adverse events associated with non-stimulant treatments are sleep disturbances, gastro-intestinal discomfort, and loss of appetite. 11 A novel drug with efficacy, tolerability, and least abuse potential is still sought after.
The United States Food and Drug Administration (USFDA) has approved viloxazine extended-release (ER) capsules (SPN-812) to treat ADHD in pediatric patients between 6 and 17 years of age in 2021. 12 The precise mechanism of action of viloxazine is not known and is claimed to act by inhibiting norepinephrine reuptake. Viloxazine increases serotonin and norepinephrine levels in the prefrontal cortex and causes a minimal increase of dopamine levels in the nucleus accumbens makes it a novel drug for ADHD with the least abuse potential. 13 The median time taken to reach the maximum concentration (Tmax) for viloxazine ranges between 6 and 9 hours while the half-life is 7 hours. Viloxazine is mainly metabolized by CYP2D6, UGT1A9, and UGT2B15 enzymes, and most of the drug has got renal elimination. 14 Considering the novel mechanism and the other factors discussed above and the recent approval by USFDA, the authors set to conduct this study to evaluate the efficacy and safety of viloxazine for treatment of ADHD in pediatric patients between 6 and 17 years of age group.
Methods
The meta-analysis was carried out as per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 15
Search Strategy
A systematic search was conducted on August 16, 2021 of PubMed, Clinical Trial Registry https://clinicaltrials.gov/, and the Cochrane Library database for any included clinical trials published in English language from inception to August 15, 2021. Search terms included the following: viloxazine, SPN-812, ADHD, and randomized clinical trials. The references lists were also explored for additional clinical trials. After excluding duplicate and inapt studies, the abstract of each article was examined by 2 investigators (AS and MB) independently to check whether the study fits into the inclusion criteria. The disagreement, if any, was dealt with among the authors through discussion. The protocol and statistical analysis plan was also checked (available at Clinical Trial Registry) to see if any desirable information was not mentioned in the published article. The search strategy has been depicted in Figure 1 Study selection process.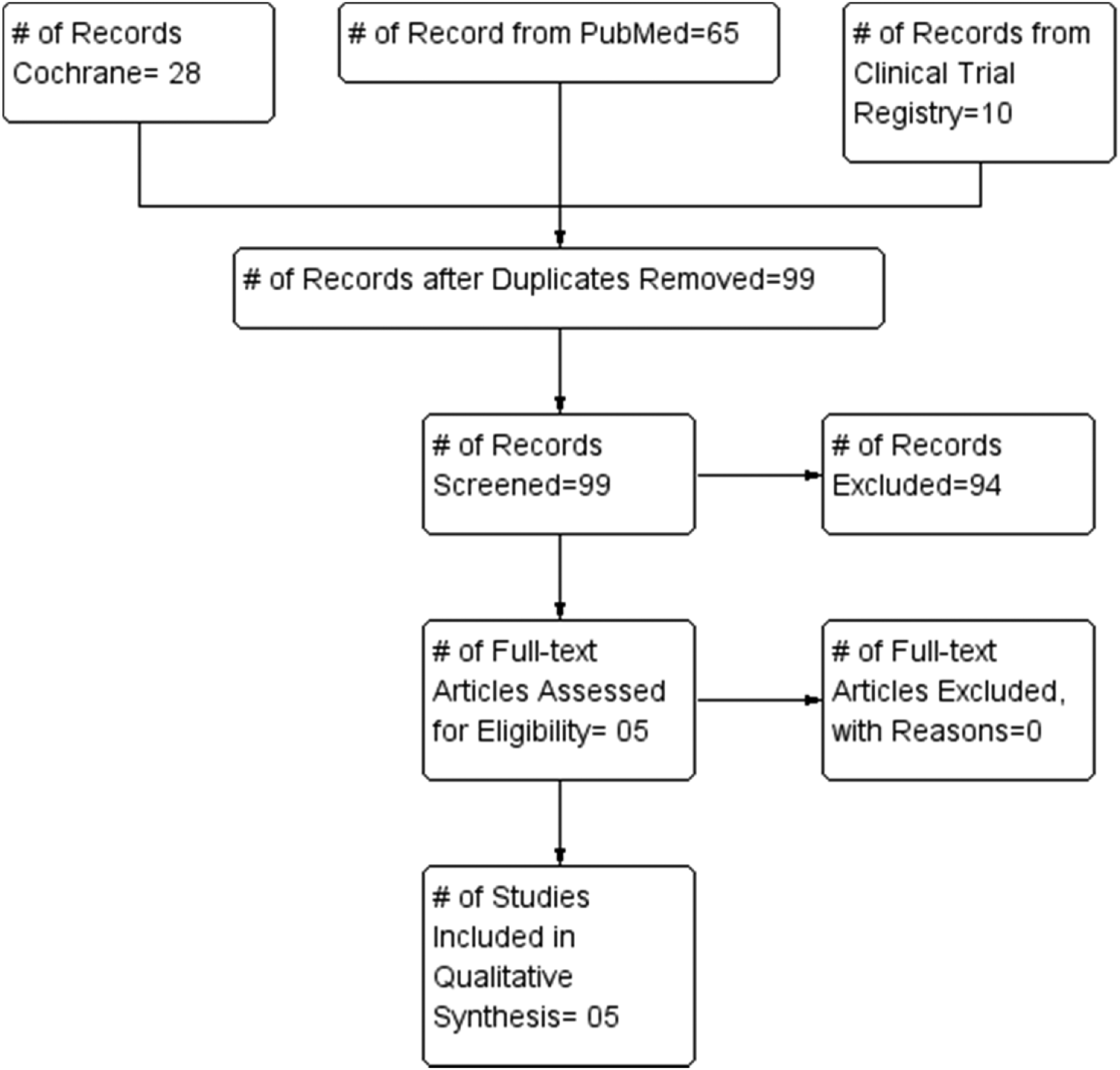
Study Selection
The randomized clinical trials, which involved pediatric and adolescents patients of age group 6–17 years diagnosed with ADHD, compared viloxazine ER with placebo at doses evaluated in phase II/III clinical trials were included for analysis.
Data Extraction
Two investigators performed the data extraction using Microsoft Excel software 2016. The primary demographic information, inclusion and exclusion criteria, and treatment schedule all outcomes (primary and secondary) were analyzed for every research article. A third author checked the data extraction. Subsequently, all the relevant data were entered and analyzed in Review Manager 5.4 for windows. Risk of Bias (RoB 2) assessment tool was used to assess bias and plotted in Review Manager. 16 The biases assessed for each include selection bias, performance bias, detection bias, attrition bias, and reporting bias. Publication bias was checked by preparing a funnel plot for each outcome.
Outcomes
The efficacy and safety endpoints included are as under: • The proportion of patients with 50% reduction in ADHD-Rating Scale-5 (ADHD-RS-5) at the end of the study. • The proportion of patients categorized as “improved” at the end of the study on the CGI-I scale. (defined as a subject who had a CGI-I score of 1 [“very much improved”] or 2 [“much improved”]) • The proportion of patients with at least one adverse event. • Incidence of Somnolence. • Incidence of Serious Adverse Events (SAEs).
Subgroup Analysis
We further analyzed the efficacy endpoints (mentioned above) across the most commonly used doses in included trials, that is, 200 mg per day and 400 mg per day. Review authors also performed indirect comparisons among the doses.
Statistical Analysis
The relative risks (RRs) with their 95% confidence intervals (CIs) were used for dichotomous data. The heterogeneity among the included studies was assessed with the Cochrane Q and the I 2 statistic. If the I 2 was > 50%, the data were considered to be heterogenic. 17 Authors used the Random-effects model to conduct the meta-analysis.
Results
Baseline Characteristics
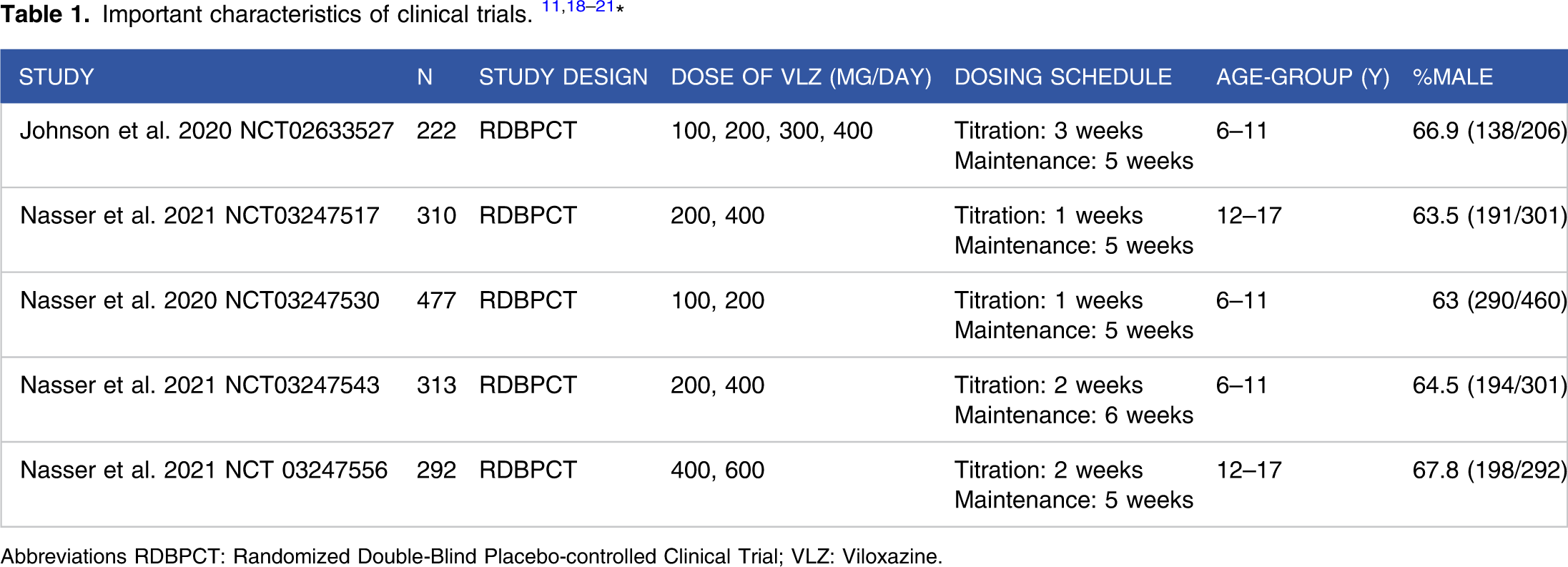
Abbreviations RDBPCT: Randomized Double-Blind Placebo-controlled Clinical Trial; VLZ: Viloxazine.
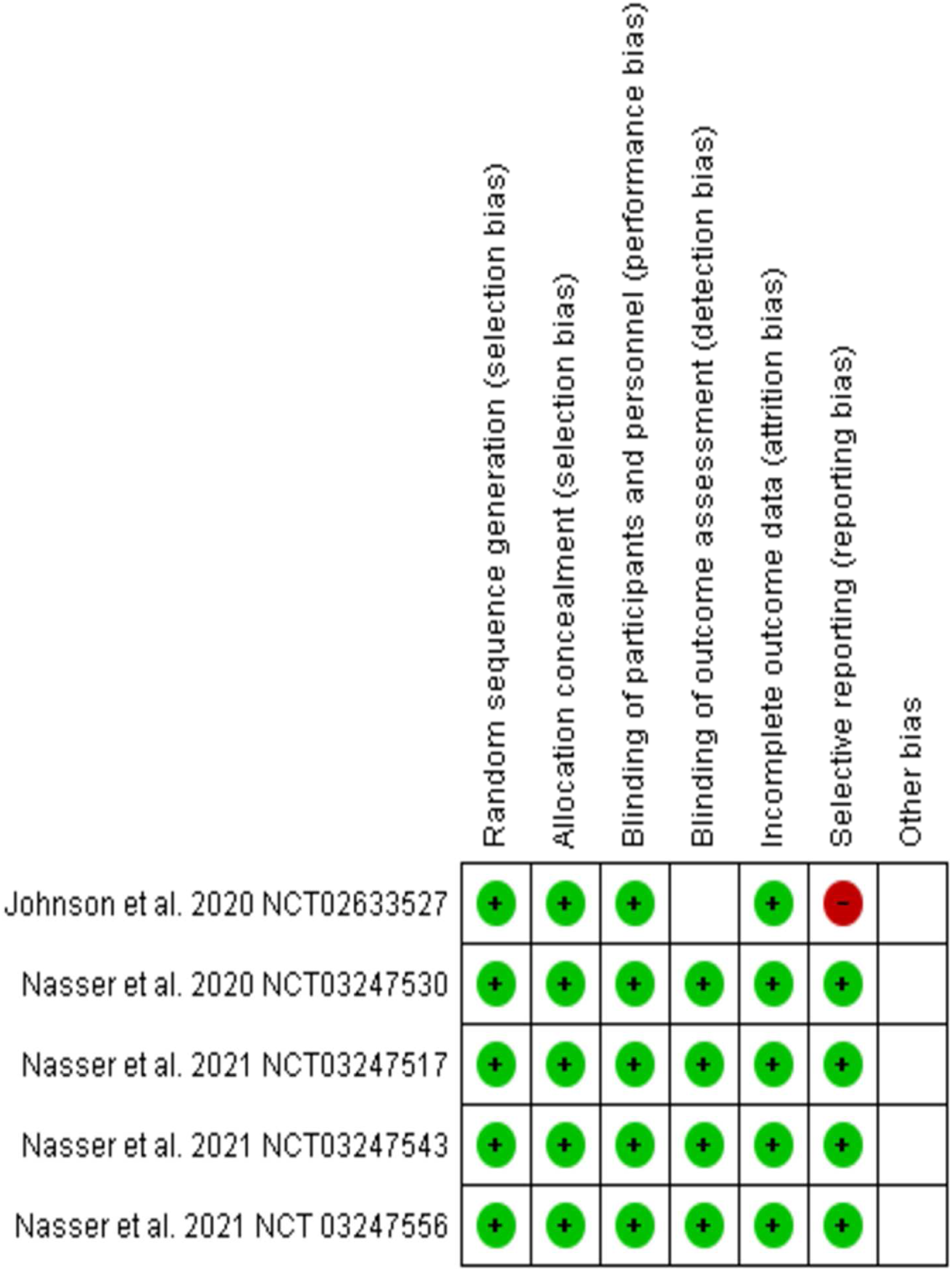
Risk of bias summary.
Efficacy Endpoints
As the funnel plot obtained for the efficacy outcome, the proportion of patients with a 50% reduction in ADHD-RS-5 at the end of the study, was symmetrical; the review authors did not note any publication bias. Further, no heterogeneity was observed (I2 = 0%, P = .72) among these trials. In this endpoint, cumulatively, 41.6% of participants were responders in the viloxazine group, whereas 25.4% of patients responded in the placebo group and viloxazine was significantly superior to placebo; RR = 1.62; 95% CI = 1.36–1.93; P = < .00001. Forest plot for ADHD-RS-5 responders. Forest plot for CGI-I improved scores.

Safety Endpoints
In the safety endpoints, the proportion of patients with at least one adverse event was more in the viloxazine group as compared to placebo (59.2% vs 37.6%), and it was statistically significant; RR = 1.52; 95% CI = 1.24–1.85; P = <.0001. Forest plot for incidence of TEAEs. Forest plot for incidence of somnolence. Incidence of SAEs. Summary of Findings.


Subgroup Analysis
The subgroup analysis was conducted for both efficacy endpoints and a comparison among recommended doses, that is, 200 mg and 400 mg was performed. In the ADHD-RS-5 responders, viloxazine performed better in both doses as compared to placebo (200mg- RR =1.72; 95% CI = 1.37–2.16; P < .00001) (400mg- RR = 1.58; 95% CI = 1.27–1.97; P < .0001). Furthermore, viloxazine 200 mg group was appeared to be better than viloxazine 400 mg group in indirect comparison (17% vs 16.5%). In another endpoint of improved CGI-I score, viloxazine in both doses performed significantly better than placebo (200mg—RR =1.55; 95% CI = 1.29–1.86; P<.00001) (400mg—RR = 1.57; 95% CI = 1.30–1.90; P < .0001). In this parameter, 400 mg viloxazine was better than viloxazine 200 mg group in indirect comparison. (19.5% vs 17.9%) ADHD-RS-5 Responders (200 mg vs 400 mg). CGI-I Improvers (200 mg vs 400 mg).

Discussion
This meta-analysis was performed for recently approved drug for ADHD in pediatric patients of 6–17 years of age and includes 5 studies in which 4 studies mainly contributed to the efficacy parameters while safety parameters included all studies. As the majority of participants were male, this is similar to the usual epidemiological trend. 23 All the trials included had a similar trial protocol, that is, titration phase followed by a maintenance phase, similar duration (6–8 weeks), endpoints and diagnostic criteria, statistical analysis plan, and the majority of participants were white. Though it increases the validity of meta-analysis, a relatively fewer numbers of participants from different ethnicity affect the results being applicable worldwide. The trials included in this study were mainly at low risk of different biases. (Figure 2) Studies with a low risk of biases generate high certainty of the evidence, which helps formulate evidence-based guidelines, eventually improving patient care. 24 Though the analysis includes less number of studies, the evidence appears to be high quality.
Viloxazine has shown significant improvement in both efficacy parameters as compared to placebo. Review authors have chosen the categorical endpoints as both ADHD-RS-5 50% response rate and improvement in CGI-I score has been shown to express clinically meaningful change and are statistically correlated.25-26 The authors had no access to actual trial data and endpoints presented as least-square mean and standard error (ADHD-RS-5 change from baseline, Conner’s 3—Parent Short Form Composite T-score, and Weiss Functional Impairment Rating Scale) were left off. These data would have added more reliability to the current meta-analysis. We assessed the adverse events and most common adverse event (somnolence), which was reported in every trial. The incidence was significantly higher in the viloxazine group compared to placebo, which was expected. 27 Somnolence will be one of the determining factors in the ultimate acceptability of drugs in the general population. The analysis also showed fewer incidences of the SAEs in the viloxazine group. More than one clinical trial reported major SAEs of concern were syncope, suicidal ideation, and suicide attempt.11,20 The RRs of somnolence and SAEs must be interpreted cautiously due to their very wide confidence interval (see table summary of findings and respective forest plots) that indicate little knowledge about the true effect and further exploration is required. ADHD medications have been shown to have placebo and nocebo effects for efficacy outcomes and tolerability respectively; hence the overall results must be analyzed critically. 28 There is a possibility of higher favorable outcome in efficacy and negative outcome in safety parameters. Upon comparing different doses, both doses (200 mg and 400 mg) were superior to placebo in both efficacy parameters. More trials are required to compare the efficacy of different doses regimen. Authors have not performed the meta-analysis of 100 mg and 600 mg of doses due to the paucity of clinical trials with desired endpoints.
The non-responders range from 10-30% when treated with approved stimulant medication (methylphenidate and amphetamine). 29 Many patients cannot tolerate the side effects of the stimulant drugs or may experience deterioration of pre-existing illnesses, or may have conditions that contraindicate their use.30-31 Moreover, both drugs carry the risk of abuse and sudden cardiac death in already existing cardiac disease. The non-stimulant drugs (atomoxetine, guanfacine ER, and clonidine ER) have more variable efficacy than the stimulant medication.32-33 Atomoxetine carries a warning for suicidal ideation, severe hepatic injury, and sudden cardiac in structural heart disease. 34 Clonidine ER is useful in addition to stimulant medication for partial responders. 35 Clonidine has been associated with withdrawal reactions if discontinued abruptly and is more common in pediatric patients. 36 Considering the limitations of already existing drugs, viloxazine (ER) was explored. Upon analyzing the clinical trials, viloxazine also carries the risk of suicidal ideation/attempt and syncope; however, no death was reported in the trial. The apparent advantage viloxazine offers is that it can be given in patients with heart disease as the drug is not likely to cause arrhythmia even in supra-therapeutic doses, and no clinically significant ECG changes were observed at least in those included 5 trials. 37 It does not have the risk of abuse, risk of hepatic injury, and withdrawal reactions and are the advantages over pre-existing drugs. 14 Considering the short duration of trials, long-term safety cannot be established, and it will be evident only in post-marketing surveillance. As of now, two open-label trials are being conducted for the long-term safety of viloxazine.38,39 The order of preference of drugs for management of ADHD is stimulants followed by atomoxetine, guanfacine, and clonidine. Presently viloxazine does not have place in management of stimulant resistant ADHD as it is very recent advancement in pharmacotherapy of ADHD.40-41 The efficacy in non-responders needs further clinical trials either alone or in combination with other drugs.
The important limitations of this analysis are the absolute changes in different scores have not been discussed, a fewer number of studies, and effect size was not compared with the conventional drugs. There is possibility of publication bias as most of the included studies have been conducted by same group of authors.
Conclusion
In this meta-analysis, the use of viloxazine ER in children and adolescent patients was associated with a higher number of ADHD-RS-5 responders and improved CGI-I score. More TEAEs, somnolence, and SAEs were observed in viloxazine group. During the short term use of viloxazine, the risk of somnolence and SAEs should be interpreted cautiously. Viloxazine appears to offer certain advantages over the side effects of existing drugs. More clinical trials are needed to evaluate the efficacy and safety of viloxazine.
Supplemental Material
Supplemental Material - Viloxazine for Attention-Deficit Hyperactivity Disorder: A Systematic Review and Meta-analysis of Randomized Clinical Trials
Supplemental Material for Viloxazine for Attention-Deficit Hyperactivity Disorder: A Systematic Review and Meta-analysis of Randomized Clinical Trials by Alok Singh, Mahesh K B, and Abhishek Singh in Journal of Central Nervous System Disease
Footnotes
Author’s Contribution
AS, AS, and MB have conducted a literature search while AS and MB performed data extraction. AS, AS, and MB jointly drafted the manuscript. Final version was approval by AS.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.