
Abstract
Aim of the study:
Neurofibromatosis type 1 (NF-1) is associated with the development of scoliosis or kyphoscoliosis. The deformity is rapidly progressive in the presence of dystrophic changes producing bone erosion. Vertebral subluxation or dislocation can occur in children with highly dystrophic kyphoscoliosis and carries an increased risk of paralysis. There is no standardised treatment for this extreme deformity with very few patients currently reported in the literature.
Methods:
Retrospective review of a patient with NF-1 who developed a dystrophic upper thoracic kyphoscoliosis with segmental displacement of T2 on T3.
Results:
We report a patient with NF-1 who presented at 8.9 years with a progressive upper thoracic kyphoscoliosis. At 18.8 years, the deformity had deteriorated to scoliosis 65° and kyphosis 78° with fixed segmental rotatory dislocation at T2-T3. He underwent posterior cervico-thoracic fusion with concave pedicle screw/hook/rod instrumentation and iliac crest bone. Minimum correction was achieved due to curve rigidity and inability to reduce the T2/T3 displacement by halo-femoral traction. At 7 months, an elective posterior re-grafting procedure was performed followed by anterior fusion with rib strut grafts between T2-T6 through a midline sternotomy. The patient is now 3.5 years after anterior surgery and remains neurologically intact with stable residual deformity and computed tomographic evidence of circumferential fusion. He has no back pain and resumed non-contact physical activities.
Conclusions:
Patients with NF-1 can develop dystrophic kyphoscoliosis with segmental spinal subluxation/dislocation. Circumferential fusion is a technically challenging procedure which often requires a multi-disciplinary surgical team but produces satisfactory clinical outcome preventing paraplegia.
Neurofibromatosis type 1 (NF-1) is a multisystem genetic condition that affects 1 in 4000 individuals. 1 It is a neuro-cutaneous disorder characterised by the presence of neurofibromas and skin pigmentation abnormalities. Involvement of the musculoskeletal system can occur early with spinal deformities representing the commonest manifestation. 2 Scoliosis has a high prevalence in NF-1, accounting for approximately 2% of all paediatric scoliosis patients. This is characterised by a short-segmented, angular curve affecting usually the thoracic spine.3–5
Evaluation of scoliosis in NF-1 allows the classification of curves into non-dystrophic and dystrophic based on the presence of key radiographic features (Table 1). Non-dystrophic curves are more common resembling idiopathic scoliosis and follow similar management principles. 7 In contrast, dystrophic scoliosis is less common but is characterised by rapid curve progression. It is associated with typical radiographic findings including vertebral body scalloping, rib pencilling, dysplastic pedicles, and severe rotation of the apical vertebrae. Kyphosis often co-exists with dystrophic scoliosis and can significantly contribute to deformity progression. 7
Key radiological features of dystrophic and non-dystrophic forms of NF-1 (neurofibromatosis type 1) scoliosis. 6

Vertebral subluxation or dislocation can occur in children with highly dystrophic kyphoscoliosis.2,8 Marked dural ectasia producing widening of the spinal canal is associated with dystrophic curves. This causes erosion of the osseous structures including the pedicles which contributes towards further instability of the vertebral column leading to subluxation and dislocation.2,7 Despite the development of spinal dislocation, patients with NF-1 may preserve neurological function and this is mainly attributed to the dural ectasia and subsequent canal widening which protects the cord from compression and injury. 7
The principles of treatment in severe dystrophic kyphoscoliosis include early surgical stabilisation usually through an anterior and posterior approach to the spine with instrumentation to prevent curve progression and achieve fusion. The treatment of rotatory subluxation/dislocation of the spine in dystrophic NF-1 is very challenging and remains controversial with 14 surgically treated patients reported in the literature (Table 2). Eight of these patients presented with normal neurology; the segmental displacement was reduced in 7 of these patients with the use of traction and fusion in an anatomical position was performed.4,11–13,17–20 The remaining patients with intact neurological function underwent circumferential fusion in situ with fibular strut graft with no attempt to reduce the dislocated segment. 4
Patients reported in the literature surgically treated with vertebral displacement in dystrophic NF-1 (neurofibromatosis type 1).

Abbreviations: AF, anterior fusion; PF, posterior fusion.
In this report, we describe the natural history and treatment of a patient with NF-1 who was followed through child-life and adolescence into adulthood and gradually developed a severe dystrophic kyphoscoliosis with fixed T2-T3 rotatory dislocation after spinal maturity. We discuss the surgical challenges encountered in the presence of an extreme deformity and the principles of treatment which allowed us to obtain a solid fusion and preserve neurological function.
Case Report
A male patient with NF-1 presented in our clinic at age 8.9 years with a mild right upper thoracic kyphoscoliosis. The scoliosis was measuring 14° from T1-T6 and the kyphosis 40° from T1-T12 (Figure 1). A plexiform neurofibroma lying in the paraspinal region at the thoracolumbar junction was noted on examination and confirmed on magnetic resonance imaging (MRI). The patient had several café-au-lait spots along his body and was asymptomatic with normal neurological examination.
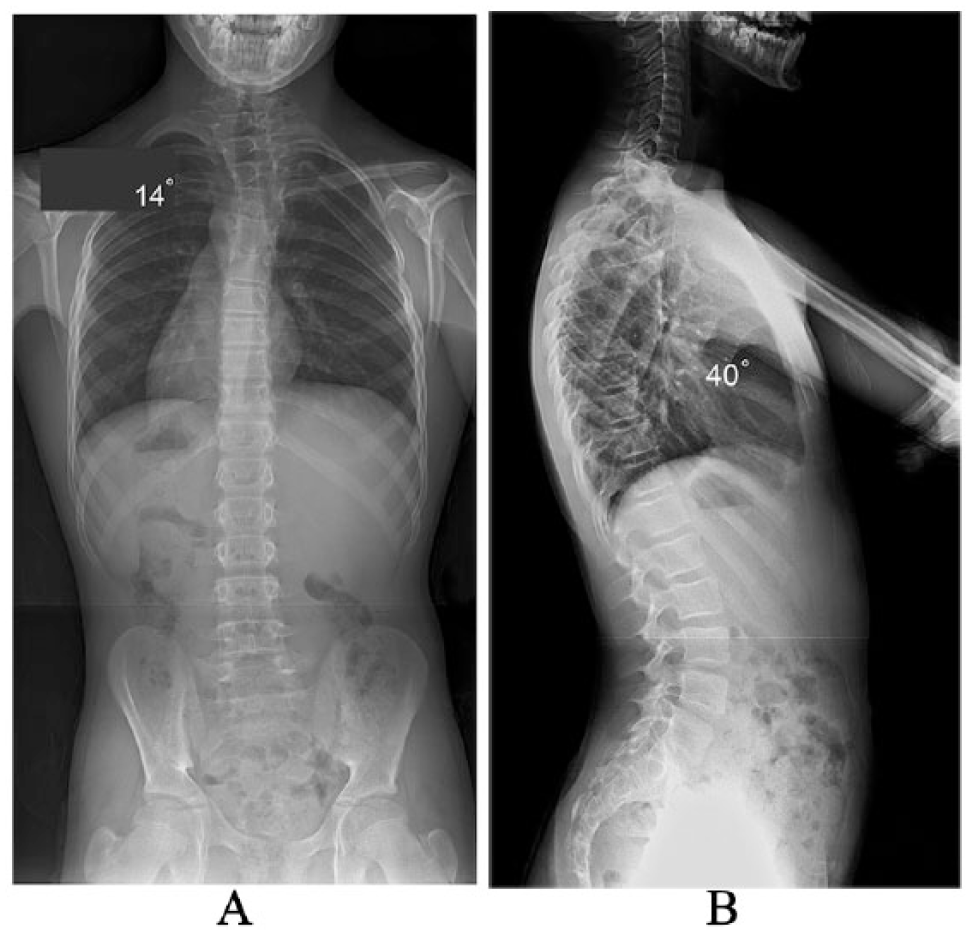
(A) Postero-anterior and (B) lateral radiographs of the spine at initial clinical presentation show a mild right upper thoracic kyphoscoliosis with pencilling of the 2 apical ribs on the convexity of the curve but no other dystrophic changes.
Over the following years, the patient remained under close monitoring. He had no neurological abnormalities and normal range of activities including sports. At age 13.6 years, he had developed dystrophic features on radiographic examination and the deformity had deteriorated to 24° scoliosis and 40° kyphosis. The patient reported intermittent right upper thoracic back pain, which was attributed to a paraspinal plexiform neurofibroma. At that stage and in the presence of a dystrophic deformity which was likely to progress, prophylactic treatment through a posterior spinal fusion was recommended, but the patient and his family did not want to proceed. During the next 3 years, he reported intermittent right upper thoracic discomfort in the area of the paraspinal neurofibroma and his kyphoscoliosis showed evidence of further progression. At age 16.8 years, the patient had completed his spinal growth as the iliac apophysis had fully formed and fused (Figure 2). Posterior spinal fusion was again strongly advised with the aim to stabilise the thoracic spine but was declined by the patient in the absence of any major complaints.

(A) Postero-anterior and (B) lateral radiographs at age 16.8 years show progressing of the deformity in both coronal and sagittal planes and dystrophic changes including rib pencilling, lateral vertebral scalloping, vertebral wedging, and a short-segmented angular curve but no vertebral displacement in the upper thoracic spine.
The patient then failed to attend consecutive appointments in our clinic despite our team contacting the family on multiple occasions. He presented at age 18.8 years with persistent thoracic back pain and reported progression of the deformity. Repeat radiographs confirmed deterioration of his kyphoscoliosis across the upper thoracic region and the cervico-thoracic junction, with the scoliosis measuring 65° and kyphosis measuring 78° (Figure 3). This was despite the fact that the patient had no spinal growth between the ages 16.8 and 18.8 years. A repeat MRI demonstrated extensive dural ectasia in the cervical/thoracic spine producing a very wide spinal canal with marked vertebral body scalloping, thinned pedicles, and hypoplastic apical laminae. A computed tomographic (CT) scan showed rotatory anterior displacement of T2 on T3 at the apex of the kyphoscoliosis (Figure 3). The patient had no neural complaints and a normal neurological examination. He underwent urgent posterior cervico-thoracic fusion extending from C6-T11 with the use of concave instrumentation and abundant autologous iliac crest bone graft harvested from both sides. Preoperative halo-femoral traction failed to achieve reduction in the T2-T3 vertebral dislocation which was fixed. Intraoperative spinal cord monitoring recording transcranial upper/lower limb motor as well as cortical/cervical somatosensory–evoked potentials remained stable throughout surgery. Attention was taken during the posterior approach to avoid plexiform neurofibromas in the right paraspinal region which could increase blood loss. After surgery, he was fitted with an underarm spinal jacket and a hard cervical collar and made an uneventful recovery. After 7 months of index surgery, he underwent an elective posterior re-grafting procedure using autologous ribs supplemented by allograft bone and recombinant human bone morphogenetic protein-2 (rhBMP-2) to reinforce the fusion mass due to the high risk of non-union. At 1 year postoperative follow-up, repeat CT confirmed a solid posterior fusion across the instrumented levels and no change in the degree of upper thoracic rotatory dislocation.
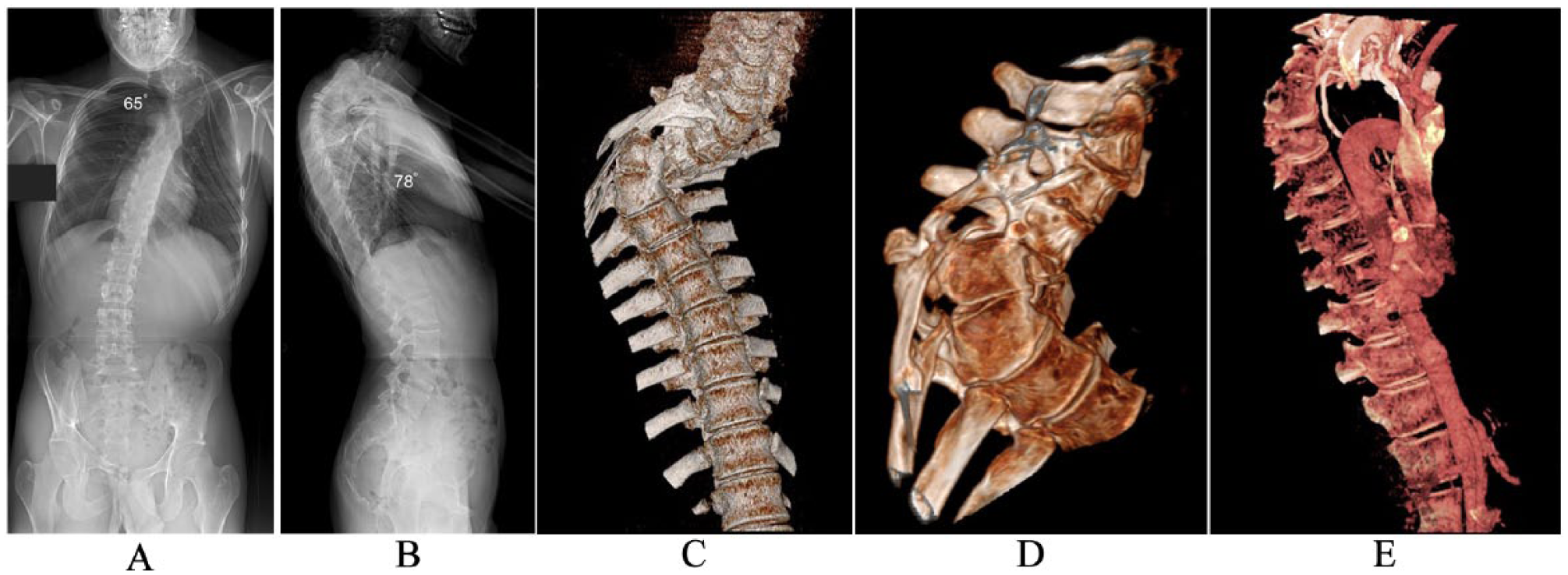
(A) Postero-anterior and (B) lateral radiographs at age 18.8 years show significant deterioration of the kyphoscoliosis associated with rotatory displacement of T2 on T3 (arrow). (C-D) This is better illustrated on the CT scans obtained as part of the preoperative assessment. (E) CT angiography performed before the anterior spinal fusion demonstrates the relationship of the aortic arch and major vascular structures with the apex of the deformity which made the anterior approach to the upper thoracic spine very challenging. CT indicates computed tomography.
The concern at that stage was that due to the highly dystrophic nature of the deformity and the presence of segmental instability at the T2-T3 level, the hypoplastic and weak pedicles could not provide sufficient anterior column support to withstand shear forces despite a solid posterior fusion. In the presence of high risk for further segmental displacement producing paraplegia, a decision was made for additional anterior spinal stabilisation with the use of autologous rib strut grafts. A contrast CT angiogram determined the anatomy of the adjacent vessels in front of the apex of the deformity to allow surgical planning (Figure 3). A joined procedure was performed with our cardiothoracic surgeons. Access to the anterior spine was obtained through a modified clamshell approach with median sternotomy. The major vessels above the aortic arch were mobilised as much as possible and gently retracted to the opposite side to allow access to the anterior aspect of the dislocated T2 vertebra. Rib struts grafts were placed subperiosteally between T2 and T6 in a niche scalloped across the antero-lateral aspect of the vertebral bodies. This procedure was extremely difficult and resulted in 1 blood volume loss (4.5 L) and 6 hours surgical time. Following surgery, the patient developed pericardial and chest effusions and required drainage. He had a stormy postoperative course and remained in the intensive care unit for 6 days and in hospital for 14 days.
The patient is now 3.5 years after the anterior spinal fusion and he has made a remarkable recovery. He remains asymptomatic and neurologically intact and has gradually returned to non-contact physical activities. A repeat CT of the spine confirmed good consolidation of the anterior rib strut grafts and a circumferential fusion (Figure 4). However, due to the highly dystrophic nature of his condition which can still predispose to recurrent bone weakness, he will remain under continuous monitoring in our clinic in the next few years and we have recommended that he should refrain from high-impact sports and any physical job that requires repetitive heavy lifting.
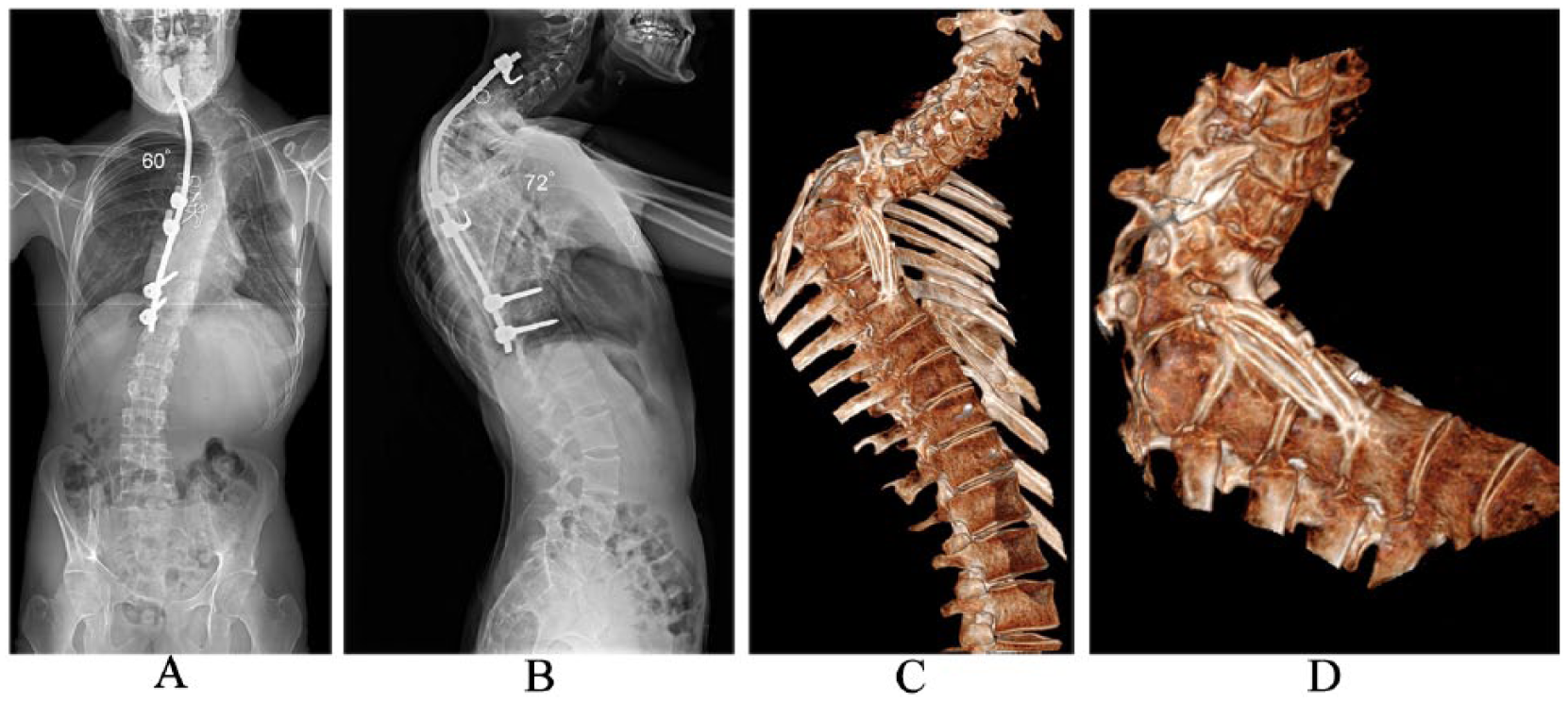
(A) Postero-anterior and (B) lateral radiographs at age 22.3 years show a stable spine with the posterior instrumentation in adequate position and no progression of the deformity. (C-D) Repeat computed tomographic scans show good consolidation of the rib struts across the area of the rotatory T2/T3 displacement providing anterior vertebral column support.
Discussion
To the authors’ knowledge, this is one of very few patients in whom surgical management of fixed thoracic vertebral rotatory displacement associated with dystrophic kyphoscoliosis in NF-1 is reported.4,15 Due to its rarity, there is limited available literature and no established guidelines on optimum treatment. The location of this deformity and segmental rotatory instability in the upper thoracic spine increases the neurological risk, as well as the degree of surgical difficulty and consequent morbidity due to adjacent major vascular structures.
Dystrophic spinal deformities in NF-1 can prove a challenge for treatment. These are often associated with sagittal plane abnormalities with thoracic kyphosis being the commonest finding. The presence of concomitant deformities must be accounted for when planning any surgical intervention. 7 The changes that occur to the bony morphology of the vertebrae contribute to spinal instability. The destruction of the pedicles due to dural ectasia, along with posterior element dysplasia, often results in anterior vertebral displacement. Subsequent biomechanical failure contributes to the development of subluxation or dislocation of the vertebral column.2,21
The goals of treatment in NF-1 are to stabilise the spine and prevent deformity progression. The surgical options include posterior-only or combined anterior/posterior fusion. Posterior-only spinal fusion has been recommended in the presence of a kyphosis less than 95°, whereas combined anterior and posterior spinal fusion to address a kyphosis greater than 95°. 22 Posterior instrumented fusion has also been suggested to achieve satisfactory stabilisation of scoliosis in patients older than 10 years of age. 23 Previous reports highlight the precarious nature of surgically stabilising dystrophic kyphoscoliosis due to anatomical factors which result in a high risk of instrumentation failure. 15 These include difficulty placing segmental pedicle screws due to insufficient pedicle width as the consequence of bony erosion by the dural ectasia and weakening of the vertebral bodies which increases the risk of screw pullout. Sublaminar wires could be an alternative technique in obtaining posterior rod fixation. However, placement of sublaminar wires can increase the risk of cerebro-spinal fluid leak in the presence of dural ectasia resulting in neurological injury. In addition, the existence of thinned laminae increases the risk of wire pullout. Sublaminar wires are also biomechanically poor anchor points proximally in the presence of severe kyphosis. Universal clamps or polyethylene ties can be used as an alternative to sublaminar wires to provide posterior rod stability. Our patient had dysplastic, slim, and elongated pedicles across the apical deformity levels, which precluded the use of pedicle screws. We therefore used a hybrid construct with proximal infra-laminar hook and transverse process wire fixation and distal transverse process hook and pedicle screw stabilisation across anatomically normal pedicles as a salvage solution. A concave construct was used as any attempt to place a convex rod would have ended up in marked instrumentation prominence under the skin in the presence of a fixed and non-correctable deformity. A convex rod would have also limited the space available for bone grafting. Postoperative immobilisation in a spinal jacket and hard cervical collar aimed to limit bending and torsional forces across the instrumented segments and reduce the risk of non-union. As part of informed consent during the index surgery, a subsequent re-grafting procedure was agreed with the patient to reinforce a weak fusion mass.
The second goal of treatment is to obtain a solid fusion across the deformity levels and the unstable spinal segment. The use of autologous iliac crest or rib graft is recommended. Cho et al 12 reported a posterior-only construct achieving a solid fusion with the addition of rhBMP-2. The benefits from the use of rhBMP-2 in achieving spinal fusion in adults are well recognised. Oetgen and Richards 6 reviewed retrospectively 81 patients under 18 years of age and reported few complications following the use of BMP. Local complications such as deep infection, dural fibrosis, and subsequent neurological deterioration result in considering their use on a case-by-case basis. In patients with NF-1, there is reported risk of enlargement of intracranial dural glioma. 6 The use of this bone-enhancing product is currently off-licence in young patients. To ensure a solid fusion, rhBMP-2 was used in our patient during the revision posterior re-grafting procedure along with autologous rib and allograft bone. Bilateral iliac crest autograft harvested during the index surgery provided abundant bone without causing long-term donor site morbidity.
Seven case studies in the literature report segmental displacement reduction and deformity improvement following application of traction.11–13,14–20 In our patient, the rotatory dislocation of T2 on T3 was fixed and did not correct with halo-femoral traction. This may be due to the chronicity of deformity even though the most significant radiographic deterioration of both kyphoscoliosis and vertebral dislocation occurred beyond the end of spinal growth. The gradual onset of rotatory displacement during the years the patient had declined treatment against our strong recommendation and failed to attend follow-up appointments resulted in his severe deformity. We believe that the significant dural ectasia and consequent marked widening of the spinal canal contributed to preservation of his neurological function.
All posterior-only fixation case studies report their success at short-term follow up.11,12,16–20 In addition, these patients achieved reduction in deformity and segmental displacement with preoperative traction, therefore allowing a more stable environment to enhance fusion. In contrast, our patient necessitated a circumferential fusion as the spine was stabilised essentially in situ. There are no studies reporting the risk of failure of posterior-only constructs and fusion in a subluxed vertebral column where a significant biomechanical force is exerted across the posterior bony mass. The aim of the anterior procedure in our patient in the presence of normal neurology was to buttress the area between the displaced T2 vertebral body and the segments below with the use of rib struts placed subperiosteally across a vascular bed that allowed bony consolidation with the aim to achieve long-term vertebral column stability.
During anterior reconstruction in patients with vertebral dislocation associated with NF-1, fibular, or tibial strut grafts have been used.4,10,15 In our patient, we used rib strut grafts to reconstruct and stabilise the vertebral column. These have been reported to be suitable in this group of patients, as graft erosion and deformity progression have not been observed radiologically 10 years following surgery. 24 Therefore, tibial, fibular, or rib strut grafts can be used as long as there is a rich stock of bone struts appropriately placed across the apex of the deformity.4,24 We recommend preservation of a subperiosteal vascular bed to allow incorporation of the rib grafts and achieve fusion. At 3.5-year follow-up, our patient had CT evidence of a solid circumferential fusion. He had no complaints of back pain, had normal neurological function, and had returned to non-contact physical activities. Long clinical and radiographic monitoring is required to confirm maintenance of satisfactory results as the dystrophic changes associated with the underlying condition can progress at longer term follow-up and affect bony fusion as has been demonstrated in patients treated at a young age with circumferential anterior/posterior surgery. 25
Anterior approaches to the upper thoracic spine can be difficult due to the anatomical constraints of the supra-aortic trunks and the transitional thoracic kyphosis. Accessing an upper thoracic vertebra with anterior and rotatory displacement at the apex of a severe kyphoscoliosis can be obtained through a concave antero-lateral exposure to the anterior column which is very challenging. The difficulties that we encountered during the anterior procedure were demonstrated in the preoperative CT angiogram and the trans-sternal approach was our only option. This would not have been possible without the assistance of our cardiothoracic surgeons.
Conclusions
Dystrophic kyphoscoliosis can be associated with segmental displacement of the spine in patients with NF-1 and this produces a very severe deformity with high potential for major neurological complications. Deterioration of the coronal, sagittal, and axial deformity can occur even beyond spinal maturity. This is an unreported feature as all patients in the published literature developed spondyloptosis prior to skeletal maturity, aged 5 to 15 years. In our patient, circumferential stabilisation with the use of posterior instrumentation and anterior rib strut grafting has prevented further progression of the deformity and segmental vertebral displacement. This staged procedure has achieved a 360° fusion and preserved the patient’s neurological function. We believe that this is a useful approach if the vertebral displacement and dystrophic kyphoscoliosis are irreducible where preventing further instability and neurological injury is critical.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AIT contributed to conception and design of the study, critically revising the article, and treating the patient; all authors to acquisition of data, analysis and interpretation of data, and drafting the article.
Informed Consent
Informed consent was obtained by the patient to publish the medical data and images.