
Abstract
Introduction:
Orthopedic ankle injuries are considered among the most common musculoskeletal injuries. A wide variety of modalities and techniques have been used for the management of these injuries, and virtual reality (VR) is one modality that has been examined in ankle injuries rehabilitation.
Purpose:
This study aims to systemically review previous studies evaluating the effect of virtual reality in rehabilitating orthopedic ankle injuries.
Methods:
We searched six online databases: PubMed, Web of Science (WOS), Scopus, the Physiotherapy Evidence Database (PEDro), Virtual Health Library (VHL), and Cochrane Central Register of Controlled Trials (CENTRAL).
Results:
Ten randomized clinical trials met the inclusion criteria. Our results showed that VR had a significant effect on overall balance compared to conventional physiotherapy (SMD = 0.359, 0.009–0.710 P = 0.04), [I 2= 17%, P = 0.30]. Compared with conventional physiotherapy, VR programs significantly improved gait parameters such as speed and cadence, muscle power, and perceived ankle instability; however, no significant difference was detected in the foot and ankle ability measure (FAAM). Additionally, significant improvements in static balance and perceived ankle instability were reported after the use of VR balance and strengthening programs. Finally, only two articles were deemed to have good quality, and the other studies’ quality ranged from poor to fair.
Conclusion:
VR rehabilitation programs can be used to rehabilitate ankle injuries, as they are regarded as safe interventions and have promising effects. However, there is a need for studies with high quality since most included studies’ quality varied from poor to fair.
Introduction
Orthopedic ankle injuries involve injuries of many types, such as lateral ankle sprains (LAS) or functional ankle instability (FAI). Lateral ankle sprains are prevalent among adults and athletes participating in sports that require jumping and frequent changes in direction. 1 Yearly, two million individuals injure their ankles in the US and UK, accounting between 3% and 5% of emergency department visits, and over 700 individuals worldwide suffer LAS daily.2,3 The involuntary twisting of the joint during a sprain has a significant impact on static and dynamic balance, muscle reaction time, muscle strength, and joint proprioception, leaving a painful and swollen joint with limited function.4,5 Those factors combined with insufficient or untimely rehabilitation after the initial injury pose a high risk for re-injury, leading to FAI or chronic ankle instability (CAI). 6 FAI produces a persistent feeling of giving way or instability within the joint during normal daily activities and affects about 70% of LAS patients.7,8 LAI and FAI affect normal biomechanical alignment and body-weight bearing, causing long-term disability, and chronic debilitating health consequences such as osteoarthritis and low quality of life, posing a high socioeconomic burden. 9
According to the 2016 National Institute for Health And Care Excellence (NICE) guidelines, PRICE, an acronym standing for Protection, Rest, Ice, Compression, and Elevation, is the main protocol for dealing with acute ankle injuries and is associated with the early administration of pain-controlled exercises, manual therapy, muscle strength, and balance exercises. 10 Strict adherence to those rehabilitation strategies can prevent the occurrence of FAI. 11 Despite the evident effects of conventional therapy on strength, balance, and other clinical outcomes, it has the disadvantage of being boring, affecting the patients’ compliance, aggravating the condition, and posing a high economic burden. 12 Therefore, ankle rehabilitation has recently encompassed new trends like virtual reality (VR) rehabilitation modalities.
The concept of VR was first developed by Ivan Sutherland in 1960. 13 VR systems offer a window of interaction between users and a computer environment simulating real-life. 13 VR systems can be either immersive or non-immersive, according to the user's level of interaction with the virtual environment and the number of stimulated senses. 13 VR was first adopted in the healthcare field during the 1990s to present compound medical data, especially when planning for surgery. 14 Since then, the use of VR in the healthcare field has grown exponentially to encompass many fields, such as teaching, training, and rehabilitation. 14 Over the last decade, VR use in rehabilitation has surged thanks to its three elements, Interaction, Immersion, and Imagination, which could profoundly enhance motor learning.13,14 VR provides some advantages over conventional therapy. It provides a virtual environment with functional tasks and immediate feedback with proper incentives to encourage patients to increase adherence, and also offers personalized programs for each patient and motivates them to try risky challenges within a safe virtual environment, boosting their capabilities. VR can be used as a home-based program with endless repetitions, thus alleviating work stress for physical therapists, as it requires only mild supervision.15,16
There is an abundance of literature investigating the role of VR in neuro-rehabilitation that shows promising results in patients with stroke, multiple sclerosis, and Parkinsonism.17 -19
Gumaa and Yussef 15 conducted a systematic review to evaluate the efficacy of virtual reality in all orthopedic conditions. For ankle injuries, they reviewed only four studies that included participants with lateral ankle sprain and reported mixed results. Due to the small number of clinical trials they included for the ankle injury, they could not perform meta-analysis. It is evident that there is a need to expand on Gumaa and Yussef’s work and provide the best available evidence in rehabilitating ankle injuries using Virtual Reality systems. Therefore, this study aims to synthesize the evidence for the effect of VR specifically in patients with orthopedic ankle injuries.
Methods
Literature search strategy
This study was registered through PROSPERO, the International prospective register of systematic reviews (CRD42021230879). We conducted and reported this review in accordance with the PRISMA 2020 (the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines). 20
Six databases were searched; namely, Pubmed, Web of Science (WOS), Scopus, the Physiotherapy Evidence Database (PEDro), Virtual health library (VHL), and Cochrane Central Register of Controlled Trials (CENTRAL) from inception till May 17, 2022. The search was conducted using relevant keywords; “virtual,” “virtual reality,” “virtual environment,” “VR content,” “virtual rehabilitation,” “computer-based,” “computer-interface,” “cyberspace,” “artificial intelligence,” “computer simulat*,” “simulator,” “exergam*,” “active video gam*,” “interactive gam*,” “game,” “gaming,” “gamification,” “Xbox Kinect,” “X-box,” “Kinect,” “Nintendo,” “Wii,” “Nintendo Wii,” “ski simulation,” “augmented reality,” “ankle,” “physical therapy,” “physiotherapy,” “training,” “rehabilitation,” “exercise,” “intervention.” We compiled the former keywords using Boolean operators and adjusted the search strategy according to each database. Filters were applied to limit the retrieved studies to English articles with human participants. In addition, we manually searched the reference lists of the included studies to detect any relevant studies.
Eligibility criteria
We set the selection criteria using PIOCS (P-population, I-intervention, C-comparison, O-outcome, S-study design). Included only English randomized controlled trials that (1) recruited adults (⩾18 years old) with orthopedic ankle injuries, (2) used virtual reality rehabilitation techniques either alone or as adjuvant therapy, (3) compared various programs of virtual reality programs or using conventional physical therapy, placebo, or no intervention for the control group, and (4) used any outcome to measure the effect of the intervention. We excluded articles that (1) included patients with neurological disorders and (2) used virtual reality techniques for any other use rather than motor rehabilitation.
Study selection
Two reviewers independently screened the titles and abstracts of the retrieved articles using predetermined eligibility criteria. Any disagreements or discrepancies were resolved by a third reviewer until consensus was reached.
Data extraction
The full texts of the included articles were further analyzed. The following data were extracted: sample size, participant’s age and gender, type, dose of intervention, virtual reality device, diagnosis, outcome measures, and the main results. Any potential conflicts were resolved by a third reviewer.
Quality appraisal
The methodological quality of the included studies was independently assessed by two reviewers using the modified Downs and Black scale for clinical trials. 21 The scale consists of 27 questions rating four categories: (1) reporting, (2) external validity, (3) internal validity, and (4) power. Studies are considered of excellent quality when the final score ranges from 26 to 28, good quality if the score ranges from 20 to 25, fair quality if the score ranges from 19 to 15, and poor if the score is 14 or less. Any disagreements or discrepancies were resolved by discussion till a consensus was reached. The Downs and Black checklist was chosen based on several factors. For example, the checklist has good psychometric properties, such as internal consistency, test–retest reliability, inter-rater reliability, and criterion validity. 21 Importantly, the checklist is a universally accepted tool in evaluating the methodological quality of studies as it provides more interpretable scores, which is essential when completing a systematic review and meta-analysis of intervention studies.
Data synthesis and analysis
Meta-analysis was conducted if at least two studies compared the efficacy of two different programs of VR or examined the effect of VR against traditional intervention, no intervention, or placebo. Standardized mean difference (SMD), 95% confidence interval (CI), and P value were calculated by comparing changes in the outcomes between the VR and the control groups using the random-effect model of analysis. 22 That is, SMD values of 0.2–0.5 are considered small effect size, 0.5–0.8 medium effect size, and >0.8 are considered large effect size. Effect size tells how meaningful the relationship between variables or the difference between groups is. A large effect size means that a research finding has clinical significance, while a small effect size indicates limited clinical applications. In other words, in the context of this study the larger the effect size the stronger the relationship between the variables. Heterogeneity in treatment effect was examined by calculating the I 2 index. The level of significance was set at a P-value of up to 0.05. All meta-analyses were carried out using the comprehensive meta-analysis, version 2.2.064 software package (Biostat, Englewood, New Jersey, USA).
Results
Study selection
Figure 1 represents the flow of the selection process during the study. We conducted an electronic search of six online databases from inception till May 17, 2022. The search strategy retrieved 224 records from PubMed, 74 from PEDro, 1011 from Scopus, 709 from the virtual health library, 199 from the Cochrane library, and 930 from Web of Science. After removing 278 duplicates and including additional 4 RCTs obtained via a manual search, we screened the titles and abstracts of 2873 records. Fourteen articles underwent full-text screening after excluding 2859 records. Two articles23,24 used a mixed population of ankle and other lower-limb orthopedic injuries, and so we contacted their authors for the data of the participants with orthopedic ankle injuries, but no response was received. Thus, we also excluded those two articles from the analysis. In addition, two other studies 25 were excluded due to an inappropriate research design and using a language other than English. Finally, ten RCTs were included in the qualitative analysis,26 -35 and four were included in the meta-analysis.27,31,32,34
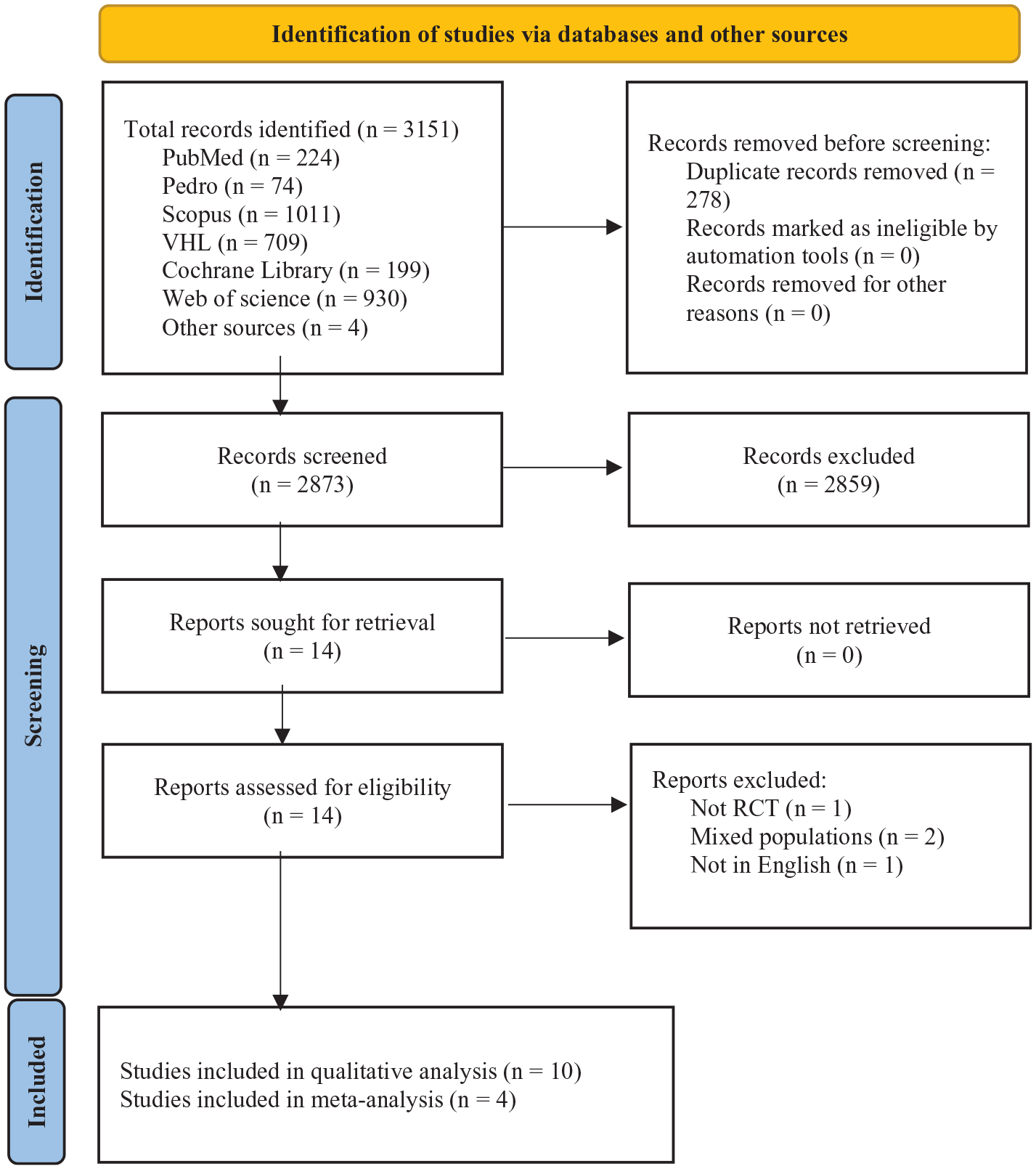
PRISMA flow diagram of the screening and study selection process.
Quality assessment
All ten articles were assessed against the Downs and Black checklist. Four studies29,30,32,34 had a poor quality rating, four26 -28,31 achieved a fair quality rating, and the other two articles33,35 were deemed to be of good quality. The main areas of weakness in the ten studies were in terms of external validity and the power analysis of the Modified Downs and Black scale. Reporting was good among the 10 studies. Finally, internal validity showed a high quality only in two studies.33,35 The complete quality assessment scores can be found in Supplemental file (1).
Characteristics of the included studies
Collectively, the studies included 394 participants diagnosed with functional ankle instability26 -32 and lateral ankle sprain.33,35 The participants’ ages ranged from 16 to 44 years old, and the ten studies were conducted in three countries: seven in South Korea,26 -32 two in Switzerland,33,35 and one in Greece. 12
The included studies used various forms and types of VR to manage orthopedic ankle injuries. Eight studies26 -31,33,35 used the Nintendo Wii Fit Plus device to improve muscle strength and balance. For muscle strength, six studies26 -31 used lunges, single leg extensions, sideways leg lifts, single leg twists, and rowing squats, and for balance, six studies27 -31,35 used ski slalom, table tilt soccer heading, tightrope walking, and snowboard slalom, while the other two studies33,35 added the penguin slide and balance bubble to the previous exercises. An XBK device was also used by one study 34 as a virtual reality method for balance training by playing XbK games such as Rally Ball, Reflex Ridge, River Rush, and 2000 Leaks. Only one study 32 used a visual feedback balance trainer device for balance training in individuals with FAI.
Seven studies26,27,31 -35 compared the efficacy of VR, and investigated its influence on balance using the Biodex Balance System and Biorescue, spatiotemporal gait parameters, on muscle strength using a Biodex isokinetic dynamometer, on physical function using the foot and ankle ability measure (FAAM), on pain using a visual analogue scale (VAS), and on ankle instability using the Cumberland Ankle Instability Tool (CAIT). Three studies28 -30 investigated the efficacy of two VR programs; namely, a balance training VR program and a strength training VR program, and compared their effect on balance using the Biodex Balance System, on muscle strength and ankle proprioception using a Biodex isokinetic dynamometer, and on ankle instability using CAIT. Detailed descriptions of study characteristics, interventions, outcomes, and the main results are given in Tables 1 and 2.
Characteristics of the included studies.
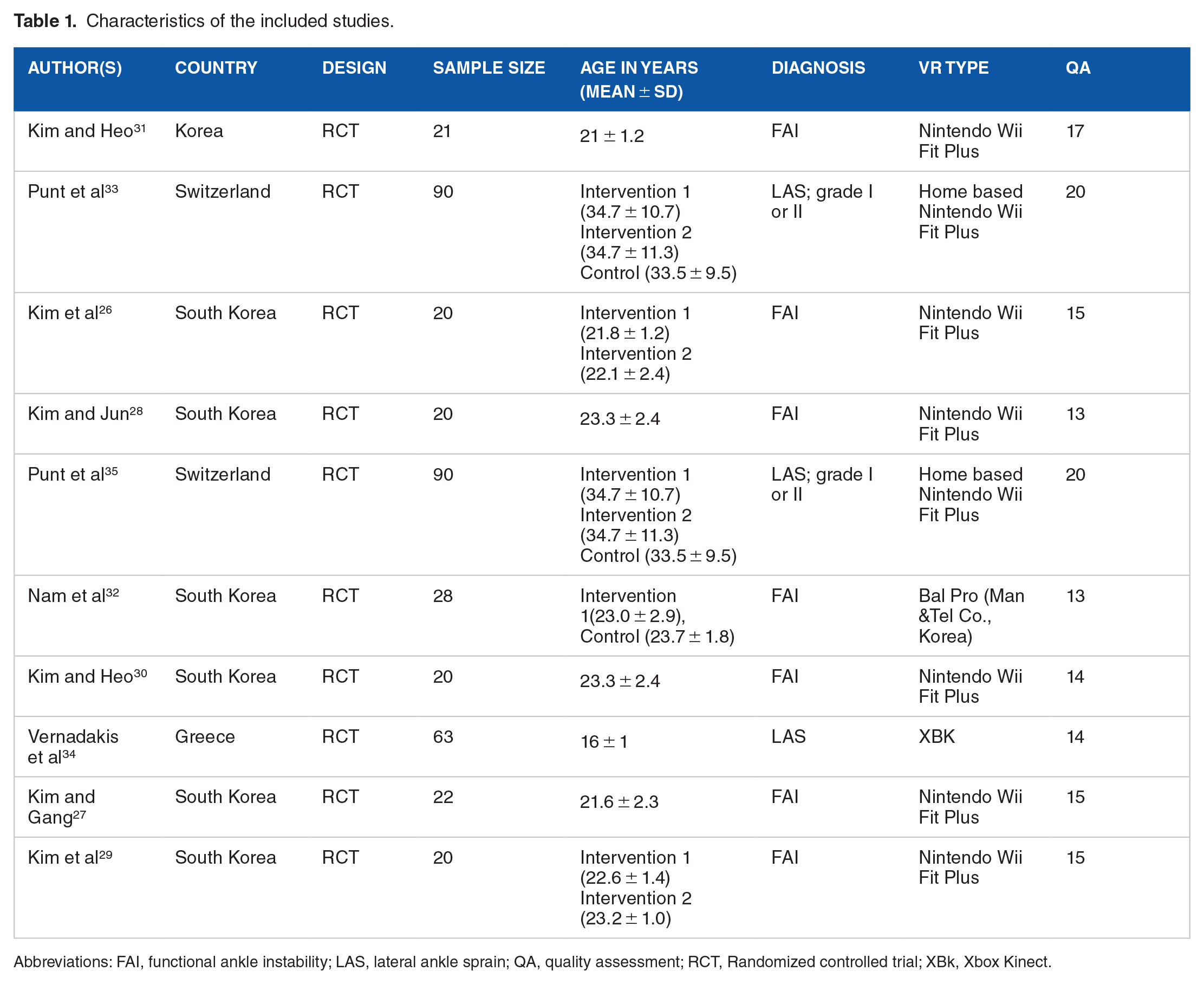
Abbreviations: FAI, functional ankle instability; LAS, lateral ankle sprain; QA, quality assessment; RCT, Randomized controlled trial; XBk, Xbox Kinect.
Summary of the interventions, outcomes, and the main results.

Abbreviations: AP, anterior-posterior; CAIT, Cumberland ankle instability tool; d, day; DF, dorsiflexion DF; FAA, foot and ankle ability; FAAM, foot and ankle ability measure; LOS, limit of stability; min, minutes; ML, medio-lateral; OSI, overall stability index; PF, plantar flexion; TRI, traditional rehabilitation interventions; VAS, visual analogue scale; VR, virtual reality; wk, week; XBk, Xbox Kinect.
Effect of VR on study outcomes
Efficacy of VR compared to conventional physiotherapy or no treatment
Regarding balance, we pooled the results of four studies, and the meta-analysis showed a significant and homogeneous effect of VR on overall balance (SMD = 0.359, 0.009–0.710, P = 0.04), [I 2 = 17. %, P = 0.30], (Figure 2). Subgroup analysis was conducted to investigate the efficacy of VR on static and dynamic balance, and it was concluded that VR significantly improves static balance (SMD = 0.573, 0.095–1.051, P = 0.02), [I 2 = 7%, P = 0.47], while having no significant effect on dynamic balance (SMD = 0.111, −0.404 to 0.628, P = 0.67), [I 2 = 28%, P = 0.25], Figure (2).

Forest plots of mean difference comparing the efficacy of VR compared to conventional physiotherapy or no treatment regarding dynamic and static balance.
Punt et al 33 examined the effect of VR on spatiotemporal gait parameters, and concluded that VR significantly improved gait speed, cadence, step length, single support time, and the symmetry index of single support time. VR did not improve the movement or timing of dorsiflexion or plantarflexion during the swing phase, and there was no significant improvement from VR on spatiotemporal gait parameters in comparison with the conventional physical therapy group or the no-intervention group. 33
Regarding muscle power, Kim et al 26 reported no significant effect from VR on ankle muscle power compared with the traditional exercise group. Regarding perceived ankle stability, using CAIT, Kim and Jun 28 reported a significant improvement from VR. Punt et al 35 reported a significant improvement in FAAM in the VR group; however, no superior effect from VR was reported in comparison with the traditional physiotherapy or no-treatment groups.
Efficacy of VR for balance program compared to VR for strengthening program
Kim and Heo 30 investigated the effectiveness of balance VR programs compared to strengthening VR programs on static and dynamic balance, and reported that both programs effectively improved static and dynamic balance.
Regarding muscle power, the results of one study 35 showed better results in favor of the VR balance training program. Another study 28 found that the VR balance training program improved ankle proprioception, while there was no effect from the VR strengthening training program. Nam et al 32 reported that the different VR programs significantly improved perceived ankle stability as measured by CAIT.
Adverse events and side effects
None of the included studies reported any adverse events or side effects from the virtual reality interventions.
Discussion
Main findings
This systematic review and meta-analysis verified the efficacy of Virtual Reality (VR) training for individuals with ankle joint injuries. A total of ten RCTs were included in the qualitative analysis; however, it was only possible to compare the pooled effects of VR training in relation to dynamic balance and static balance in four studies.
The quality of the included studies was generally moderate, with two studies demonstrating good methodological quality on the Downs and Black scale. 21 In terms of the studied outcomes, all but three of the included studies compared VR with traditional physiotherapy or no intervention. Kim and Heo, 30 Kim and Jun, 28 and Kim et al 29 compared two VR training programs; namely, balance training and strength training.
Overall, the qualitative findings demonstrated that VR rehabilitation programs improved gait parameters, including gait speed, cadence, step length, single support time, and single support time symmetry index. 30 VR balance training exercises improved ankle muscle power and proprioception compared with VR strengthening exercises.28,35
Ankle stability and resting and walking pain also improved after implementing different VR techniques28,32,35; However, the improvements in foot and ankle ability measures were similar to those from traditional rehabilitation. 35
The results from the meta-analysis showed a significant and homogeneous effect of VR on overall balance compared to those receiving conventional physiotherapy or with no intervention. It is worth mentioning that the meta-analysis was based only on four studies with moderate methodological quality. Furthermore, the subgroup analysis revealed that static balance outcomes significantly improved following VR program training. Specifically, VR training showed a significant improvement in post-intervention static balance in the medial-lateral direction. 31 This finding can be explained by the fact that muscle strength training, sideways leg lifts, single-leg extensions, and single-leg twist exercises were performed to improve muscle strength in the medial-lateral direction while maintaining balance. 31
Previous studies evaluating the effects of VR on ankle impairments observed inconsistent results on whether VR training was beneficial for this population. For instance, in their review, based on four studies published before 2017, Gumaa and Yousef 15 concluded that VR is not superior to exercises. However, for this current study, we included four recent RCTs published after 2017 and provided some evidence on the effectiveness of VR for ankle joint rehabilitation. For instance, Nam et al 32 conducted an RCT that included 28 patients with functional ankle instability, and reported a significant improvement in Limit of Stability and Cumberland ankle instability scores for the experimental group. Similarly, Kim and Heo 31 examined the effects of a VR exercise program compared to conventional exercise on balance in a sample of patients with functional ankle instability, and found a significant difference between groups in which VR exercise was more effective in the overall direction (static) and medial-lateral direction (dynamic) of balance than conventional exercise programs.
Contrary to expectations, this study did not find a significant effect of VR training on dynamic balance. Previous literature, however, suggested a significant improvement in both static and dynamic balance of patients with ankle joint injuries after VR applications. For example, Kim and Heo 30 compared the effectiveness of VR balance and strength programs on static and dynamic balance, and found that the two VR programs improved both outcomes. In our study, we did not observe a significant effect of VR on dynamic balance, but this observation may be due to differences in the intervention period, as a significant improvement in dynamic balance parameters may require a longer treatment period and different exercises. 31 These inconsistencies could also be attributable to other biomechanical factors that impact dynamic balance, such as muscle strength, ankle mobility, and functionality of synovial structures that may enhance joint stiffness and thus limit dynamic balance.36 -38 This assumption was also confirmed by Hoch et al 39 in their investigation, where they concluded that a loss of ankle range of motion could negatively affect dynamic balance.
Limitations
A few limitations of this systematic review should be noted. First, only full-text articles published in English were included for this analysis, and therefore we might have missed relevant studies published in other languages. Second, more than half of the included studies were published by the same author and in the same geographical location. Thus, we cannot assure that these studies used different populations. However, other articles were also included to add other critiques and viewpoints. Another methodological limitation in the study is the small individual sample sizes involved, since, with a few exceptions, most of the included studies had recruited small samples of patients that were not based on rigorous sample size calculations. Therefore, a meta-analysis was performed to account for this limitation. Lastly, the majority of the included studies received low scores on their quality assessments. However, these low scores were not because the studies were of poor quality, but rather the problem lay in the quality assessment tools. Although we attempted to use the best available quality assessment tools, these tools shared a common limitation for evaluating VR-related studies. For example, in all the included studies, blinding of participants was not possible due to the nature of VR interventions, and thus the studies missed the score for this item. This limitation was also highlighted in previous reviews, 40 showing that there is a need to develop tools that can specifically assess VR-related studies.
Clinical implications
The findings of this systematic review support the use of virtual reality to complement rehabilitation programs for individuals with ankle injuries, as it significantly improved gait speed, step length, single support time, cadence, and single support time symmetry index without any notable adverse events or side effects. Further, it also improved static balance and perceived ankle instability. All these outcomes are extremely important in fostering ankle joint recovery and rehabilitation after injuries.
Although it was out of the scope of this review, it is interesting to mention that VR systems may improve patient adherence. Research shows that patients’ adherence to physiotherapy is problematic and may adversely affect the success of the entire treatment plan. For example, it has been documented that nearly 10% of patients fail to attend physiotherapy sessions, about 20% do not complete their recommended exercises, and approximately 60% are completely non-adherent to prescribed physiotherapy programs. 41
The problem of non-adherence could be minimized by including VR programs in treatment protocols, as VR has shown a high degree of enjoyment by patients. 15 For instance, as reported by Vernadakis et al, 34 XbK-based balance programs are more enjoyable than traditional physiotherapy programs alone. The roles of enjoyment (the desire to have fun) and intrinsic motivation (the desire to engage and expand one’s skills) have been discussed in the literature as potential predictors of non-adherence to rehabilitation interventions such as exercise. 42 As evidenced by Vernadakis et al, 34 VR systems do a great job in improving enjoyment, and consequently adherence to physiotherapy sessions.
Since VR systems are an emergent technology and relatively new in orthopedic rehabilitation, it is essential to train physiotherapists and clinicians on their use to achieve the desired clinical outcomes for in-patient or institution-based rehabilitation. Notably, VR treatment can also be provided as an unsupervised home-based program. 43 To effectively use VR systems at home, patients have to be educated on how to appropriately use these technologies. This can be a challenging task, because the efficient use of VR systems depends on several factors, such as a patient’s age, technical literacy level, and previous experience. 44 All these considerations should be addressed to achieve the optimal benefits from VR systems. It is also clear that more knowledge-to-action research is needed to effectively integrate VR applications into daily physiotherapy routines.
Conclusion
To conclude, the existing evidence of the efficacy of VR applications for individuals with ankle joint injuries is promising. Based on this systematic review, it is valid to conclude that VR applications are feasible and comparable to other physiotherapy approaches, including exercise, and thus can be considered as a realistic alternative for the rehabilitation of patients with ankle injuries. The results from the meta-analysis of four clinical trials showed a significant and homogeneous effect of VR on static balance compared to conventional or no intervention. For dynamic balance, however, the evidence of the effectiveness of VR applications is somewhat inconclusive. A point of note is that the quality of the reviewed studies must be carefully considered while assessing the results of this systematic review because only two studies were deemed to have good quality, while the quality of the rest varied from poor to fair. Also, only three small studies were included in each meta-analysis, which may imply low power and limited generalizability. In order to effectively inform clinical practice, further clinical trials with larger sample sizes are needed.
Supplemental Material
sj-docx-1-rpo-10.1177_11795727231151636 – Supplemental material for The Efficacy of Virtual Reality Training in the Rehabilitation of Orthopedic Ankle Injuries: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-rpo-10.1177_11795727231151636 for The Efficacy of Virtual Reality Training in the Rehabilitation of Orthopedic Ankle Injuries: A Systematic Review and Meta-analysis by Abd El Rahman Elaraby, Mostafa Shahien, Alhadi M. Jahan, Mohammad Etoom and Amira Hassan Bekhet in Advances in Rehabilitation Science and Practice
Supplemental Material
sj-docx-2-rpo-10.1177_11795727231151636 – Supplemental material for The Efficacy of Virtual Reality Training in the Rehabilitation of Orthopedic Ankle Injuries: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-2-rpo-10.1177_11795727231151636 for The Efficacy of Virtual Reality Training in the Rehabilitation of Orthopedic Ankle Injuries: A Systematic Review and Meta-analysis by Abd El Rahman Elaraby, Mostafa Shahien, Alhadi M. Jahan, Mohammad Etoom and Amira Hassan Bekhet in Advances in Rehabilitation Science and Practice
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.