
Abstract
Purpose:
Literature regarding the WHO’s International Classification of Function, Disability and Health (ICF) has called for research into psychosocial adjustment processes. This project aims to establish the relevance of the Integrative Model of Adjustment to Chronic Conditions (IMACC) as a framework for research and a clinical tool in rehabilitation by linking it with the ICF.
Methods:
The study employed secondary analysis of data from the original IMACC grounded theory study, where 8 women and 2 men with type 2 diabetes mellitus participated. IMACC consists of 3 interconnected parts comprising a total of 13 components. Datasets used for the study consisted of the qualitative data underpinning each IMACC component. Meaningful concepts from each dataset were linked to ICF categories using the updated ICF linking rules.
Results:
Results showed that all 13 IMACC components accommodate ICF category codes from all health and health related ICF components in patterns consistent with the theoretical conceptualisation of each separate IMACC component.
Conclusion:
IMACC maps comprehensively to the ICF framework and provides a framework that may be useful for future ICF related research into biopsychosocial processes in psychosocial adjustment. IMACC provides a clinically applicable intervention for people with psychosocial adjustment difficulties consistent with the ICF framework.
Introduction
The World Health Organization’s (WHO) International Classification of Functioning, Disability and Health (ICF) 1 is a systematic and comprehensive framework for rehabilitation and research. A range of reviews have added detailed information and guidelines for the use of the ICF,2 -5 which is typically used as a common frame of reference for a variety of rehabilitation research.6 -9 This article proposes a strengthening of focus in rehabilitation of the process of individual psychosocial adjustment. After a brief discussion of the nature and importance of psychosocial adjustment, various types of theoretical adjustment models are presented and linked with the ICF. This is followed by the aim of the current project, which is to demonstrate the relevance of the Integrative Model of Adjustment to Chronic Conditions (IMACC) for research and applied rehabilitation within the ICF framework.
Literature relating to WHO’s ICF has called for more research into the process of psychosocial adjustment (referred to as ‘adjustment’ in this article) to chronic long-term conditions (LTCs). 10 Adjustment can be viewed from 2 perspectives. Firstly, adjustment as the state of an individual’s function and wellbeing on a range of parameters and at any given time point after acquiring an LTC. 11 The ICF 1 provides a tool for assessing adjustment by looking at the ICF components body functions and structures (biological aspects), activities and participation, environmental influences and, with a recent addition to the ICF, 5 personal factors (psychosocial aspects). However, the ICF provides primarily an objective, clinical measure of levels of adjustment. Quality of life (QoL), which has traditionally been seen as a measure of adjustment, 7 is a subjective measure and not currently included in the ICF classification system. More to the point, both types of measure can provide information only on the state of adjustment.
The process of changing from one state of adjustment to another is the second perspective on adjustment and, arguably, the more important aspect, if we consider the need to improve clinical interventions aiming to optimise adjustment. 11 A theoretical understanding of the process of adjustment is essential for the development of effective and efficient interventions for individuals, who struggle to adapt to a life with 1 or more LTCs. Furthermore, it could inform future research into development of services and social structures that can optimise support to people with LTCs. This is of great health economic importance as chronic disease management is a major challenge for health services worldwide. 12 In Britain, the Department of Health (DH) claims that an increase in self-management of LTCs is the only sustainable way forward for health and social care services. 13 If that is held up against findings in Scotland, where capability for self-management was only optimal in 13% of a cohort of 9348 patients, 14 we are looking at up to 90% of people with LTCs potentially needing to make improvements to their self-management regimens to keep as well as possible. In the Scottish study, good self-management was associated with the lowest rate of visits to GPs and emergency departments, lowest number of emergency hospital admissions and shorter stays for elective hospital admissions.
Adjustment is a complex concept with many facets. Broadly, adjustment is the psychosocial accommodation of a person to a life-altering event or transition. 15 Looking at the ICF, the aim of adjustment is to optimise the physiological, cognitive and emotional function to allow the best possible level of wellbeing, activity and social participation. 1 From an individual’s perspective, re-appraisal of their lifestyle, health behaviour changes, social and health service support, 12 perceived control and support,16,17 as well as coping with illness stressors 18 and unwanted changes to their life and relationships 12 are just a few of the complex aspects of adapting to an LTC.
The following is a brief overview of different types of adjustment models and how they relate to the ICF. Dekker and de Groot 10 provided an overview of current psychological theories relevant to adjustment in the form of a pathway diagram. They argued that the detailed structure of the ICF is more useful as a measure of health outcomes after adjustment than the traditional QoL measures used in psychology. Finally, they suggested a model linking relevant psychological concepts and theories directly to the current structure of the ICF Model of Functioning and Disability (hereafter called the ICF model). Whereas this is undoubtedly an important step towards integrating psychological adjustment theories into the ICF structure, the model provides limited suggestions as to how these aspects interact to either facilitate or create barriers to adjustment or indeed what the dynamic process of adjustment is.
Mumby and Whitworth 7 explored adjustment processes in chronic aphasia after stroke. They found 5 themes: intervention type, effectiveness, barriers, facilitators and QoL. Arguably, barriers and facilitators are relevant to the personal process of adjustment, QoL is the outcome of the adjustment process, and intervention type and effectiveness are the ‘tools’ that health services and society are continually developing to optimise adjustment in any given population. If these ‘tools’ work well, then they can form part of the facilitators supporting the individual adjustment process. So central to the process of adjustment is the overcoming of barriers to approach or reach an optimal level of function and adjustment. The study linked 5 key barriers to the ICF structure, for instance, ‘overcoming isolation’ was linked to ICF relationships, activity, and participation. Whereas this is useful in terms of integrating adjustment theories with the ICF, the study specifically included the impact of the clinical intervention delivered to the participants and therefore provided limited understanding of the normal process of adjustment in general.
Others18,19 have looked at positive and negative factors impacting the adjustment process and leading to either successful adaptation or adjustment difficulties, respectively. This is useful, for instance, when assessing barriers to adjustment, however, both papers look only at personal cognitive and behavioural factors as barriers and do not include the social and environmental barriers, apart from the historical social impact on the person’s development prior to acquiring an LTC. As with the other models, these factor models do not provide an understanding of the dynamic processes underlying development and maintenance of positive or negative responses to internal and external barriers.
In addition, the above models share the issue that they do not directly point towards systematic methods of intervention that cover the wide range of aspects relevant to adjustment. This makes them difficult to apply directly to clinical practice. Hammond and Hirst-Winthrop 20 proposed the Integrative Model of Adjustment to Chronic Conditions (IMACC), which is a normative process model based on biopsychosocial principles. The model assumes that the process of adjustment is largely similar across conditions, as adjustment is relevant for the whole person, not merely for their condition-specific challenges. The original study focused on type 2 diabetes and the model has since been theoretically verified for applicability to adult-onset epilepsy (IMACC-R1 11 ).
IMACC proposes an understanding of how a person’s pre-condition personality (beliefs, habits and identity), in interaction with their social and physical environment, impacts on their subsequent adjustment process by either hindering (barriers) or facilitating the process. IMACC provides a way of identifying barriers to the normal progression of adjustment and, crucially, it provides a method to understand how and why barriers are maintained over time. IMACC also demonstrates how resolution of barriers are key to the process of behavioural and attitudinal change, which over time will lead to adaptive changes to the person’s identity.
The IMACC model was developed through a grounded theory study using a priori codes from cognitive behavioural theory (CBT). CBT is a widely evidenced theory of psychological processes, typically used to understand maintenance processes in various mental health conditions. 21 The fact that the model has been developed according to CBT principles makes it directly applicable to clinical practice.
IMACC (Figure 1) is a model of a person’s internal process of adjustment. The model consists of 3 interconnected parts comprising a total of 13 components, some of which are divided into sub-components. Pre-condition personality (part 1) factors (beliefs and habits) relevant for adjustment feed into the ongoing adjustment cycle (part 2), where they act as either facilitators or barriers (snags) to adjustment. The ongoing adjustment cycle consists of 5 areas of adjustment, 1 of which (Support) constitutes the social and environmental dimension, where actual and/or perceived external barriers may occur. Barriers to adjustment form triggers for the maintenance cycle (part 3), which is characterised by a cognitive conflict that needs to be resolved. Once resolved (outcome A in Figure 1), this constitutes an adaptive change in thinking and behaviours, which in turn feeds into to positive identity changes. If conflicts are not resolved (outcome B), but rather maintained over time, it leads to adjustment difficulties, and identity changes are typically of a negative nature.11,20 Space does unfortunately not allow for a full presentation of IMACC, for further details please see cited references.

The Integrative Model of Adjustment to Chronic Conditions, first revision (IMACC-R1).
IMACC reflects the normative intrapersonal biopsychosocial processes of change and adaptation.11,20 The interaction with the social/environmental (or extra-personal) dimension is mainly reflected in ‘Support’ (ongoing adjustment cycle), however, as all components reflect aspects of the individual, these are inevitably shaped to a greater or lesser extent by external influences, past or present. Furthermore, such dynamic processes are not likely to fit neatly into the distinct ICF components of body function/structures, activities/participation and contextual factors (environment and personal factors). Rather, all the ICF components are likely to be present throughout the process and mutually influenced in a dynamic way as individuals move from one state of adjustment to another.
This project aims to establish the relevance of the IMACC as a framework for research and a clinical tool in rehabilitation by classifying the datasets from the original study 20 using the ICF classification system. By demonstrating such relevance, this study further aims to propose IMACC as a process model of adjustment central for further ICF research and development.
Method
Design
Framework method 22 can be used to map qualitative data onto a theoretical framework. In this project the method was adapted to allow for mapping of one theoretical framework (IMACC) onto another (ICF).
Ethics and dataset
This study employed analysis of secondary data from the original IMACC grounded theory study.20,23 Approval to conduct secondary analysis was granted by a British University Ethics Committee. The original study 11 was conducted by the first author (LDH) and type 2 diabetes was chosen as the medical condition due to the high levels of incidents of that diagnosis. 24 Using maximum variation sampling, participants were recruited through diabetes support groups and via public advertisement. The sampling criteria were (1) a type 2 diabetes mellitus diagnosis, (2) between 1 and 5 years post diagnosis and (3) capacity to recall and reflect on the experience of adapting to life with type 2 diabetes. Ten participants aged 46 to 63 (8 women and 2 men) consented in writing to take part in either individual interviews or focus groups. In addition to standard data coding, the study made use of a priori theoretical codes 25 from cognitive behavioural theory, 21 which is an extensively evidenced theory used to conceptualise psychological and behavioural processes. For further details please refer to the original publication. 20
As described in the introduction, the model emerging from the original data analysis consisted of 3 distinct but interconnected parts, each of which contained specific components and subcomponents. The full dataset from the original study was used in the present study, however, to allow for mapping of the IMACC onto the ICF, it was necessary to generate new datasets rather than use the original transcripts. These new datasets were generated by merging the data from all nodes (a topical collection of coded data) 26 within IMACC components and sub-components and duplicate data was removed. This resulted in 18 separate datasets, each corresponding to either an IMACC component or a sub-component.
Procedure and analysis
The second author (APF, referred to as the analyst) was trained in the use of the ICF classification system. Using the qualitative analysis software NVivo 12, 27 he identified meaningful concepts from each dataset and linked these to the ICF according to the updated ICF linking rules 3 (referred to as ‘coding’). In addition to the main classification system, 1 the new personal factor classifications 5 were also used. The latter are still under development, however, with IMACC being a model of the intrapersonal change process, it was seen as essential to include personal factors. ICF coding qualifiers were not used, partly to simplify the analysis and partly because severity levels could not reliably be determined.
In parallel, the first author (LDH) was also trained in the use of ICF for the purpose of triangulation 28 of the analysis. Initially, a small pilot analysis was conducted to calibrate the approach. Any discrepancies or questions about classification of, for instance, medical concepts were discussed and agreed with the third author (MS), who is highly experienced in the use of the ICF classification system. The analyst then proceeded with the coding of all transcripts. The analysis allowed for systematic mapping of the IMACC onto the ICF classification structure. Once completed, the coding of all datasets was triangulated by LH and minor inconsistencies corrected.
To keep the coding relatively simple it was chosen to use minimal coding for body functions and body structures. Psychological states like cognition and emotional reactions involve a complex system of neurological and endocrine interactions. Coding of such functions were mainly done by using level 2 ICF codes representing the main functions and structures involved. An exception to this was made in cases where a specific function, like b1304 impulse control, was central to change of health behaviours.
The coding was done on 2 levels; From explicit statements describing, for instance, activities or environmental issues, meaningful concepts were identified and linked to relevant ICF classification codes. In addition, as the original study employed a hermeneutic approach, 29 it was deemed appropriate to take a similar hermeneutic approach when identifying and classifying meaningful concepts in the datasets. A hermeneutic, or interpretative, approach is employed when a deeper understanding of a phenomenon is sought. This understanding is context dependent, in this case we were seeking to interpret the dynamic processes involved in adapting to a life with a chronic condition. Therefore, explicit statements were interpreted by consideration of questions like ‘what does this statement tell us about how the person experienced the described issue?’ This typically involves considering, for instance, the underlying emotional response or the likely attitude of the person uttering the statement. Such statements can obviously be interpreted in several ways; however, such ambiguity is accepted in the hermeneutic tradition. Involving 2 people in the analysis increased the likelihood of broader interpretations. Meaningful concepts arising from these interpretations were similarly linked to relevant ICF codes. Use of this 2-level approach allowed for a richer and more in-depth analysis, thus maximising detailed information relevant to the process of adjustment.
The analysis then proceeded to identify key ICF codes by running frequency reports per dataset. The 20 most frequent codes were listed and included, and a graph produced for each dataset (for an example of this please see Figure 2 in the Results section). The lists of frequent codes were examined to see whether they related to all ICF components; body functions (b), body structures (s), activities and participation (d), environment (e) and personal factors (i). It was then considered whether the constellation of key ICF classification codes linked with each dataset were meaningful in relation to the specifications of each IMACC component or sub-component. These specifications were based on the findings in the original study, 20 which were further developed during the follow-up study on adult-onset epilepsy. 11

Mapping of the IMACC sub-component ‘Learning New Skills’ onto ICF components and specific ICF codes.
Finally, the most relevant key ICF codes from each dataset (IMACC component or subcomponent) were selected and transferred to the ICF model with the purpose of illustrating the relevance of IMACC to the ICS, please see Figure 3 in the Results section for an example.
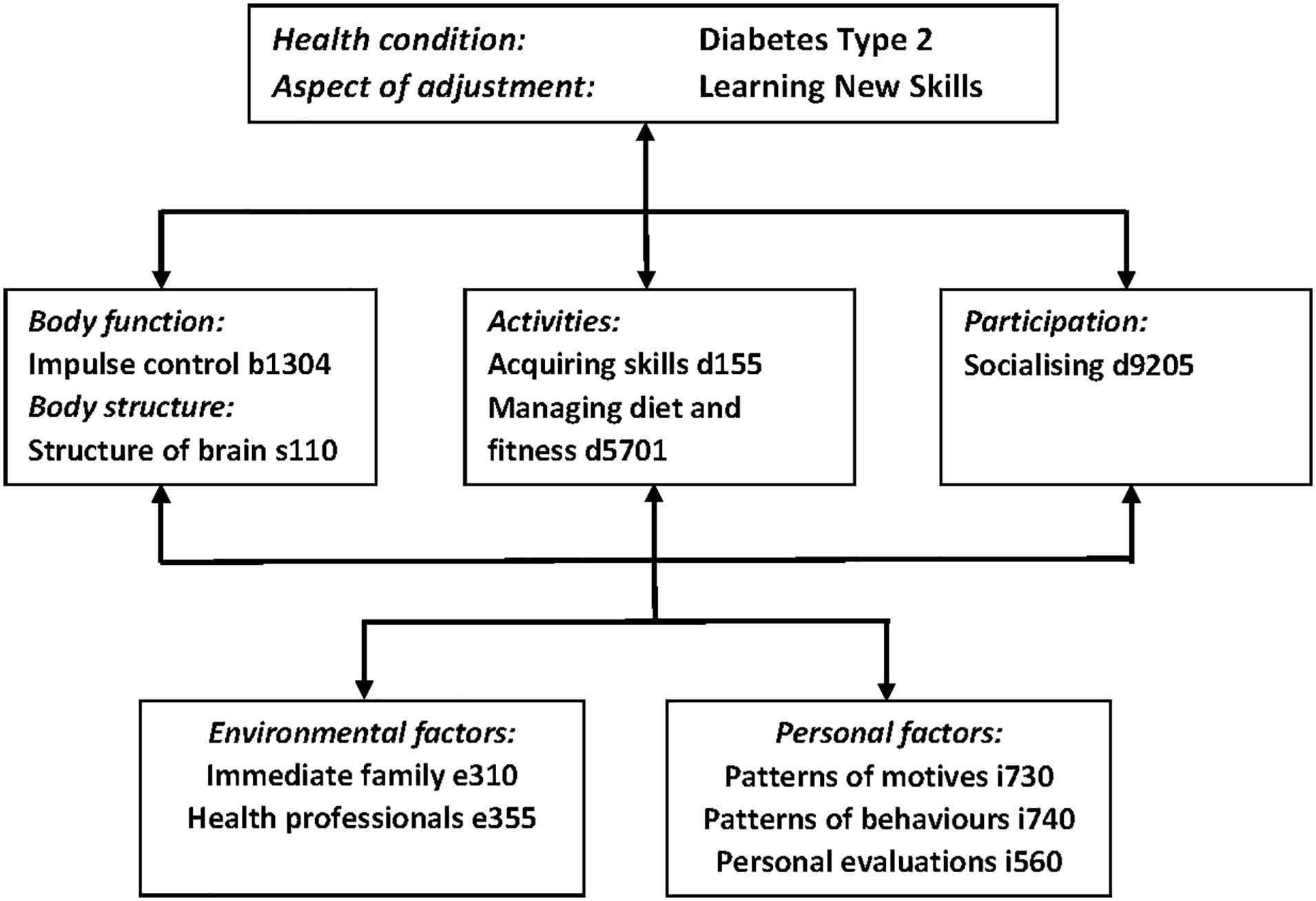
Matching of the ICF component interactions with the IMACC model sub-component Learning New (Skills) using the example of learning the skill of impulse control with regards to sugary/fatty foods that used to be consumed habitually for reward or as part of socialising.
Results
All IMACC components and sub-components accommodated a range of ICF second and third level categories from all health and health related ICF components in patterns consistent with the theoretical conceptualisation of each separate IMACC component.
To illustrate the findings in detail one example has been selected. The IMACC component ‘Learning New’ consists of 3 sub-components: Learning New Knowledge, Learning New Skills and Learning New Attitudes. The second of these sub-components (Skills) was mapped onto the ICF and the graph (Figure 2) with the 20 most frequent codes show that all ICF components (b, s, d, e and i) were applicable.
Further analysis of the specific ICF codes relevant for ‘Learning New Skills’ revealed a pattern consistent with the conceptualisation of the IMACC sub-component, which, as the name describes, is conceptualised as learning new skills relevant to the management of the condition. In the original study this included managing weight, diet, exercise and glucose levels. One skill needed to develop self-management in type 2 diabetes is impulse control. This is used as the example of mapping of IMACC onto the ICF model and the interacting ICF components (Figure 3). Quotes relevant for each ICF code included in the example can be found in Table 1.
Participant quotes illustrating the example of IMACC Learning New (Skills) with ICF codes involved in the task of learning impulse control.

In this example based on the dataset Learning New Skills one body function required for managing weight and diet is b1304 Impulse control. People often reward themselves with food, which can be a particularly challenging habit to change. An internal dialogue (quote no. 1) is used to slow down the automatic habit of rewarding oneself. This involves the body structure s110 Structure of brain as the main structure for cognition and exercise of control.
The two main activities involved in this process is the activity d155 Acquiring skills (quote no. 2), that is part of the learning involved in changing health behaviour, and the activity d5701 Managing diet and fitness (quote no. 3), which is the health behaviour that needs to change to achieve good self-management of the condition.
Mastering the skill of impulse control, and more widely, the skill of diet and weight management, then allows the individual to engage in participatory activities, in this example the activity d9205 Socialising (quote no. 4), without compromising their self-management.
This is facilitated by environmental factors, for instance, e310 Immediate family (quote no. 5). In this case a brother, who supports indirectly by being a source of competition to see, who stays off medication the longest. In addition, e355 Health professionals advising on diet (quote no. 6) support learning by offering information and advice on alternative dietary options.
Finally, personal factors influencing the process of learning include i730 Patterns of motives and handling motives and i740 Patterns of behaviours and handling of behaviours, in this case the motivation to and the habitual behaviour of rewarding oneself with food (quote no. 7). To counteract this habitual motivation, the personal factor i560 Personal evaluation is used to replace the food reward with a positive personal evaluation (quote no. 8).
Discussion
This project aimed to establish the relevance of the IMACC as a framework for research and a clinical tool in rehabilitation by classifying the datasets from the original study 20 using the ICF classification system. The purpose was to propose IMACC as a process model of psychosocial adjustment, something that has been called for in the literature. 10
IMACC is a relatively complex model with multiple components, it was therefore not possible to present all findings within the constraints of a journal article. An example was chosen, the component ‘Learning New’ and its sub-component ‘Skills’. This example was chosen, partly because it was one of the largest datasets with most coding, partly because the process of learning new health-related behaviours is central to rehabilitation efforts. The example demonstrates the interactions between the personal factors, activities of eating healthily, supported by family and health professionals, and the learning of impulse control through working on developing new strategies, like other ways of rewarding oneself. This demonstrates the compatibility of ICF and IMACC, the latter proposing a theory of the missing process of how the ICF components interact.
Adjustment in long-term conditions involve change of health behaviours, and motivation is often seen as key. ICF codes frequently used were the personal factors i730 Patterns of motives and handling motives and i740 Patterns of behaviours and handling behaviours. These were coded with almost equal frequency. Participants typically described their habits and expressed motivation consistent with their habits. There were fewer incidents of clearly expressed motivation to change, hence the lesser use of the ICF code b1301 Motivation. When trying to change habits and behaviour, participants would express a motivation to change and examples of behaviours that would be consistent with that motivation, whilst also sometimes expressing their struggle to maintain the new behaviours. A study into attitudes to healthy eating and dietary behaviour showed a significant relationship between the perceived health of eating habits and the actual level of healthy eating with both interacting to change dietary habits. 30 This seems to be consistent with the findings in this study.
Looking at the article’s example of health behaviour change through use of the ICF model we see a positive result of a process of adjustment, and it informs us of factors that are relevant for learning the skill of impulse control. However, it does not inform us of the dynamic processes that are required during the transition. To understand the journey from inadequate impulse control to good impulse control – or more widely, from poor to appropriate levels of adjustment – it is necessary to use the IMACC model as a whole.11,20 Looking at the 3 superordinate levels of the model we find that personal factors stem mainly from the Pre-condition Personality level. In the Ongoing Adjustment Cycle, we find areas of adjustment, where either personal or environmental factors, and often the interaction of the two, can create barriers to adjustment and challenges for activities and participation. Finally, in the Maintenance Cycle, we find the mechanisms responsible for either maintenance of the problems or development of new ways of coping. The essential principle of this cycle is that people are faced with dilemmas or conflicts that need to be resolved to move on and change behaviours and relevant aspects of identity.
The study demonstrated that IMACC maps comprehensively to the ICF framework in relation to the process of adjustment in chronic conditions. We believe this to be the first study to map a chronic conditions adjustment process model to the ICF framework and IMACC is the first model of adjustment to be shown to comprehensively match ICF span. IMACC provides a framework that may be useful for future ICF related research into biopsychosocial processes related to adjustment and we propose that it could be central for further ICF research and development. Using the IMACC in research has the potential to systematically investigate the processes of health-related behaviour changes and it provides a framework for studying and classifying barriers and facilitators to change and adjustment.
Conversely, the finding that all ICF components are represented in each IMACC component, in ways that are consistent with IMACC component definitions, may strengthen the further development and use of IMACC in rehabilitation practice. Descriptions of IMACC components can be developed, verified, and applied in a highly systematic way by ensuring that definitions and applied formulations include all ICF components.
Cieza et al 3 discussed the issue of the vague association between interventions and outcome measures. As IMACC is directly clinically applicable, it would be possible to use it as a research framework within the wider ICF to develop assessment and/or outcome measures that would link strongly to IMACC as an intervention, all within the overall framework of the ICF. The IMACC also needs to be clinically tested in larger trials. If such testing were linked to established outcome measures consistent with the ICF, a comprehensive tool set for assessment and treatment of psychosocial adjustment difficulties would be available for clinicians.
A weakness of the current study was the use of triangulation of the analysis, rather than a formal inter-rater reliability analysis. However, a more important issue was that it was based on secondary data from a previous study with only few participants and serving a different purpose. To establish the patterns of ICF codes within each IMACC component more systematically, a more targeted study is required. One option could be to investigate each IMACC component in turn, with a focus on identifying facilitative and hindering aspects, and then establish typical patterns by coding relevant data using the ICF classification system. Using the complete IMACC model it could then be established how common barriers are maintained and what aspects need strengthening or support to facilitate optimal adjustment and the best possible levels of self-management of LTCs. Finally, another limitation is the basis of the assumption that IMACC describes the general psychosocial adjustment process, regardless of condition. As the model has only been theoretically verified in diabetes and adult-onset diabetes, a substantial body of work is required to confirm this assumption. However, if this can be empirically demonstrated, the advantages of having a pan-condition psychosocial adjustment model cannot be underestimated.
Facilitation of adjustment is presumably the most important goal for such research. From an individual perspective, poor adjustment can lead to problems like occupational and financial challenges, limiting opportunities and roles in life, stress and anxiety, lower self-esteem, and increased risk of depression and other psychiatric disorders.31,32 The strength of IMACC as that it provides an understanding of the process of change, not only in a positive direction, but also how barriers to change can lead to negative identity changes and mental health issues. If we then consider recent estimates that around 25% to 30% of the population live with one or more chronic conditions13,32 and that potentially less than 15% of those adjust optimally and more than 20% not at all, 14 then we are looking at a lot of people living a life that may be unnecessarily difficult and lacking in quality. If our understanding of the process of adjustment is systematically developed, we have the potential to provide health service structures and interventions, both early and more complex, which could improve the lives of many. This in turn would have social and health economic benefits, potentially reducing the current burden, which sees, as an example, 70% of the National Health Service budget being spent on management of chronic conditions. 13
In conclusion, the IMACC is the first biopsychosocial process model of adjustment that has been shown to map comprehensively to the ICF. As the model is directly clinically applicable it provides a framework for research and development with potential to link assessment, intervention, and outcome measures within the wider context of the ICF classification system.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors contributed to the development and design of the study. APF and LDH coded and analyzed the data. LDH drafted the manuscript. All authors contributed to the article and approved the submitted version.