
Abstract
Published research exploring confidence and perceptions of effectiveness in performing a manually assisted cough on children with neuromuscular disease is not available. This descriptive study aimed to describe confidence and perceived effectiveness of parents, children, and therapists in parent performed manually assisted cough. A total of 28 children with neuromuscular disease, one of their parents, and physiotherapist participated. Overall, 40% of parents, 52% of children, and 46% of therapists were very confident in parents’ ability to perform effective manually assisted coughs. Parents, children, and therapists largely perceived the parental manually assisted coughs as somewhat effective (68%, 60%, and 57%, respectively). Approximately, half of parents (48%), children (52%), and therapists (50%) felt very confident in parents’ ability to retain the technique between clinic visits. Interestingly, percentage agreement statistics indicate that a reasonable proportion (30%) of pairs of respondents did not agree in their ratings. Overall, high percentages of favourable ratings were noted for all questions.
Keywords
Introduction
Neuromuscular diseases (NMDs) are a group of multifaceted inherited diseases which have detrimental effects on the body by impairing the neuromuscular and respiratory systems. 1
Acute respiratory infection as a result of impaired respiratory muscle strength is the most common cause of unintended hospital admission and mortality in this population.1–5 Respiratory muscle weakness in the early stage of NMD increases the risk of chest infections6,7 and predisposes to respiratory failure once it has reached the advanced stages.5,8–12 Generally, a deterioration in respiratory function, and to a greater extent respiratory failure, occurs between 8 and 20 years of age in children with NMD 13 and, indeed, seems to be directly related to increased mortality rates.1,14 However, with the appropriate treatment, the incidence of unplanned hospital admissions may decline, with a subsequent improvement in longevity.1,14
Cough augmentation techniques encompassing mechanical insufflation-exsufflation and manually assisted cough (MAC) are treatment methods used in the management of respiratory complications in children with NMD,6,8,11 with the primary goal of increasing cough peak flow (CPF)11,15 and therefore cough effectiveness, to enable sufficient elimination of airway secretions.6,11,12 Although mechanical insufflation-exsufflation is commonly considered superior to other techniques,11,16 there is limited evidence to ascertain the effectiveness and safety of this technique compared to other cough augmentation techniques.6,11 In addition to this technique being minimally evaluated, it remains to have limited clinical application as it is expensive,6,11,17 thereby necessitating greater incorporation of MACs.
MAC is a technique that involves applying an external pressure to the chest wall or abdomen of the child, which is timed with their own coughing effort, in an attempt to increase expiratory flow and thereby movement of respiratory secretions.11,12,18 Augmented cough techniques are currently performed by therapists within the hospital setting as well as being taught to parents to perform at home as part of the management for their child’s condition.
Adherence to therapeutic treatment seems to be a complex issue, particularly in children. Non-adherence to treatment regimens has been reported as the main cause of treatment failure in paediatric chronic conditions 19 and thus may be a strong predictor of poor outcomes.20,21 As perceptions and expectations have a critical role in determining adherence, attentiveness to these factors is essential in the management of children with chronic disease. 20 When performing manual techniques, various patient factors such as age and cognition may indeed impact on utility and adherence, especially in regard to long-term use within the domiciliary environment. 12 Confidence and perceived effectiveness of parents performing an MAC may also be a factor in determining adherence and therefore is a useful parameter, which could be investigated.
No published research explores parent, child, and therapist confidence and perceived effectiveness of MAC being performed by anyone other than the therapist. Therefore, developing an understanding of these perceptions is warranted. The purpose of this descriptive, cross-sectional study was to investigate confidence and perceived effectiveness of parents, children, and therapists in parent performed MAC. It was hypothesised that parents, children, and therapists would feel confident in the parents’ ability to effectively perform a MAC.
Patients and Methods
This study was approved by the Australian Catholic University Ethics Committee (2016-70N) and the Sydney Children’s Hospitals Network (SCHN) Ethics Committee (LNR/14/SCHN/553).
Subjects
Children with NMD, who attended neuromuscular outpatient clinics at either Sydney Children’s Hospital Randwick or The Children’s Hospital at Westmead, were invited to participate in this study. In addition, one parent of the identified children were also invited to participate in the study. Children (and their parents) were eligible for inclusion in the study if the child was aged between 6 and 18 years, had a diagnosis of NMD, and had a CPF <270 L/min. Parents (and children) were not approached if the child had contraindications, which precluded them from receiving MACs, or if they had severe cognitive and/or language deficits, which precluded them from participating in the study.
Procedure
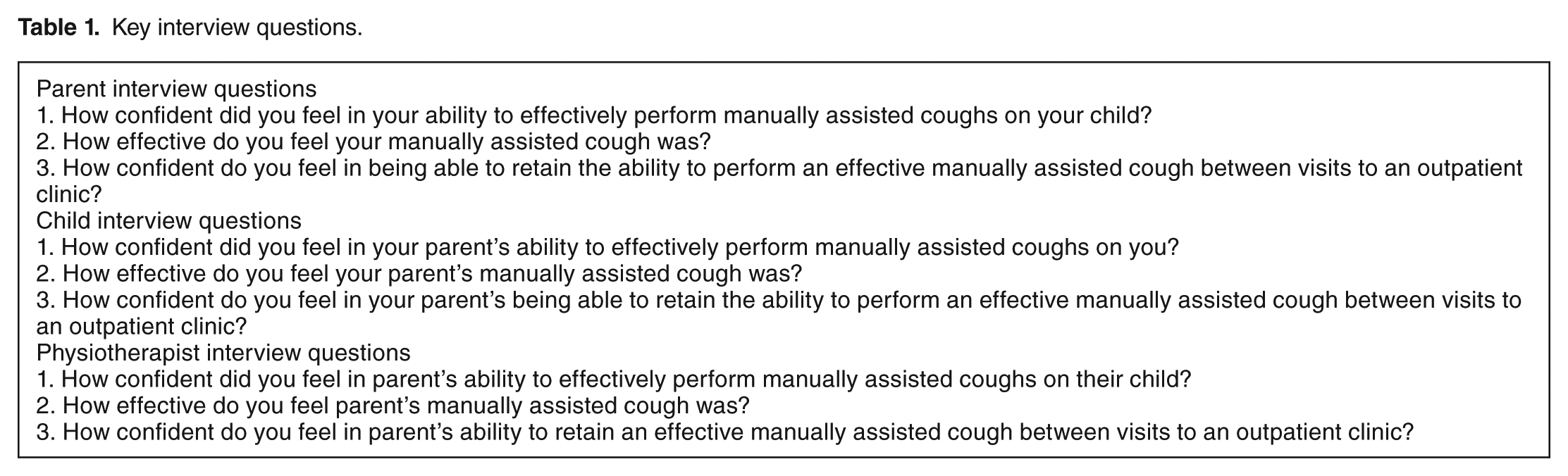
After informed consent was obtained, the physiotherapist provided a training session to the parent in performance of MACs in keeping with international recommendations that children with a CPF <270 L/min be taught augmented coughing techniques. 1 Subsequent to this training, the parent, child, and physiotherapist were interviewed in a semi-structured format by using a set of key questions intended to guide the interview process (Table 1). Each interviewee was questioned in isolation of one another as a means to attempt to control for measurement bias. If the subject did not understand a question, or if a question did not prompt a relevant answer from the subject, the interviewer was free to seek clarification in order to ensure a more accurate response.
Key interview questions.
Outcome measure
Parents, children, and physiotherapists were asked to rate 3 statements which best described their confidence and perceived effectiveness in parents performing an MAC on children with NMD (Table 1). The 3 statements related to confidence in parents performing an effective MAC, perceived effectiveness in parents performing an MAC, and confidence in the parent’s ability to retain an effective MAC between visits to an outpatient clinic. Subjects were required to rate these statements in terms of being very, somewhat, or not at all confident/effective.
Statistical analysis
The analysis of subject responses was performed using IBM SPSS Statistics 23.0 and Microsoft Excel Version 2011. Frequency tables were generated for each variable as a means of checking data entry errors and to determine the frequency of responses for each of the 3 groups. Microsoft Excel, which has been shown to be a conservative approach to establish event-based interobserver agreement, 22 was used to determine percentage agreement between parent, child, and physiotherapist responses.
Results
A total of 30 consecutive children who met the inclusion criteria and their parents (n = 30) were approached and agreed to participate in this study. However, 2 children subsequently withdrew from the study due to fatigue during teaching of the manually assisted coughing and therefore 28 children (24 males, 4 females; aged between 6 and 17 years with a mean age of 12 years) completed the study. In addition, one parent of each child (n = 28) and the physiotherapist providing the training were interviewed. The characteristics of the children who participated in the study are presented in Table 2.
Group characteristics of children with neuromuscular disease (n = 28).

Abbreviations: CPF, cough peak flow; MAC, manually assisted cough.
Levels of confidence in parents performing an effective MAC on their child with NMD were largely consistent between the 3 groups of respondents, with high percentages of respondents reporting being ‘very confident’ or ‘somewhat confident’ in parents’ ability to perform an effective MAC (Figure 1).

Percentage of parent, child, and physiotherapist responses to confidence in parents performing an effective MAC. MAC indicates manually assisted cough.
In relation to perceived effectiveness of parent performed MAC, the majority of respondents in each group perceived the technique to be ‘somewhat effective’ (Figure 2). The responses about confidence in the parents’ ability to maintain an effective MAC between clinic visits were also remarkably similar across the 3 groups of respondents; however, the percentage of respondents with an unfavourable response was higher than for the previous questions in all 3 groups (Figure 3).

Percentage of parent, child, and physiotherapist responses to perceived effectiveness in parents performing an MAC. MAC indicates manually assisted cough.

Percentage of parent, child, and physiotherapist responses to confidence in parents’ ability to retain an effective MAC between visits to an outpatient clinic. MAC indicates manually assisted cough.
To determine if parents, children, and therapists agreed about individual cases, percentage agreement among the groups was calculated. Starting with confidence in the parents’ ability to perform an effective MAC, parents and children gave the same response 68% of the time, children and therapists gave the same response 60% of the time, and parents and therapists gave the same response 60% of the time. Similarly, when rating perceived effectiveness, 68% of children and parents, 60% of children and therapists, and 56% of parents and therapists were in agreement. Also similarly, when rating confidence in the parents’ ability to maintain an effective MAC until the next clinic visit, 72% of children and parents, 60% of children and therapists, and 76% of parents and therapists were in agreement.
Discussion
This is the first study to evaluate the confidence that parents, children, and therapists have in the parents’ ability to perform an effective MAC and to maintain its effectiveness between clinic visits. Similarly, it has not previously been reported how parents, children, and therapists perceive the effectiveness of the parental MAC technique. Overall, there were high percentages of favourable ratings (ie, ‘very’ or ‘somewhat’) by the 3 respondent groups for all questions.
The above findings are encouraging because confidence and perceived effectiveness may have an influence on treatment outcomes and compliance. Indeed, it has been noted that health care providers who promote and ensure a high level of patient satisfaction improve compliance with therapy interventions and promote positive health outcomes. 23 Similarly, the degree to which parents believe physiotherapy assists their child is indicative of how they perceive home treatment, and thus understanding parental beliefs about the necessity of physiotherapy is a strong predictor of adherence within the home environment.24,25
Additionally, it has previously been demonstrated in children with visual and motor deficits that the level of confidence parents feel in performing interventions is associated with their ability to adequately participate in home programs. 26 A study in children with cystic fibrosis reported parental barriers to treatment regimens such as being overwhelmed by the burden of daily care and their lack of experience with caring for a child with a debilitating and chronic illness. 27 Therefore, the identified levels of confidence and perceived effectiveness in parents performing an MAC on children with NMD may potentially be assisting compliance to treatment regimens. Although the impact of exploring perceptions on therapy adherence and treatment outcomes could not be explained within the scope of this study, further research may provide clarification.
While the ratings of confidence and perceived effectiveness with respect to parents performing the technique of an MAC were promising, clearly there is some concern as a proportion of subjects completely lacked confidence in parents’ ability. It is important to note that therapists completely lacked confidence in the ability of 11% of parents to perform an effective MAC while 4% of parents completely lacked confidence in their own ability to effectively perform an MAC. In addition, physiotherapists tended to have poorer perceptions of parents’ ability when compared to parents and children. This was particularly evident in relation to parents maintaining an effective technique between clinic visits. Of the 3 questions, the third question had the highest percentages of ‘not at all’ responses. It is reasonable to assume that all 3 groups of respondents felt that the parents’ MAC technique could deteriorate during time between clinical visits.
Overall, the percentage agreement results were close to 70%. While this is good, it is important to remember that – with only 3 categories of response – the percentage agreement by chance alone would be 33%. Overall, the percentage agreement statistics indicate that a reasonable proportion (30%) of pairs of respondents did not agree in their ratings. Therefore, if therapists were to invite parents and children to verbally rate their confidence and perceived effectiveness with respect to the parental MAC technique, therapists can be alerted when the ratings do not match their own.
Strengths and limitations of the study
More than half of parents and children who participated in the study were learning the technique of MAC for the first time. In a retrospective medical record review, it was revealed that 12 parents had previously learnt how to perform an MAC (ie, 16 parents were learning the technique of MAC for the first time). Whether these parents continued to perform the technique outside of the therapy environment remains unclear. Importantly, prior exposure with the technique may have influenced confidence and perceived effectiveness with respect to parent performed MACs. Pertaining to the limitations of the technique, MAC requires a great deal of coordination between the parent and child as well as sufficient physical strength, 11 both of which could have influenced perceived effectiveness. A single time period of data collection only allowed the examination of the immediate perceptions of subjects on the technique of MAC and did not assess how past experience with the technique may have affected these perceptions. The study had a relatively small sample size and given that there is substantial heterogeneity among individuals with NMD, 12 this may therefore limit the generalisability of results to the wider NMD population. An additional limitation is that this study examined reported levels of subjective confidence and perceived effectiveness. Due to social acceptability bias, some subjects might have been reluctant to report feeling ‘not at all’ confident/effective, thereby higher than actual ratings of confidence and perceived effectiveness may have been obtained. In a similar manner, prevailing pathology, baseline lung volumes, and lung compliance are factors, which may influence the perception of MAC effectiveness, however could not be explored within the scope of this study. Finally, the age range of children (6-17 years) in this study was relatively large. Since children are still developing their cognitive processes, which in turn may have influenced their perceptions, it may have been more appropriate to have separated the children into pre- and post-adolescent ages and analysed their results separately. Nevertheless, the wide age range improves the external validity of the study. While this study provides valuable insights, it is the first to investigate confidence and perceived effectiveness of parent performed MAC on children with NMD. Therefore, larger and more robust descriptive studies with follow-up need to be conducted to confirm the findings of this study.
Conclusions
This study found an overall consistency between parents, children, and therapists, with high percentages of favourable ratings (ie, ‘very’ or somewhat’) by each of these 3 groups in relation to confidence and perceived effectiveness in parent performed MAC. However, it may be important for physiotherapists to ask parents and children about their perceptions of manual assisted cough effectiveness, so therapists can be alerted when the perceptions do not match their own. This descriptive study adds to the body of knowledge currently available by providing some valuable insights into assisting parents of children with NMD to feel confident in their support of their child’s respiratory management.
Footnotes
Acknowledgements
The authors would like to thank Associate Professor Mark Elkins and Professor Jenny Peat for providing assistance in the statistical analysis and interpretation of data. They would also like to thank all the children and their parents who agreed to actively participate in this study. Without the time and effort that they all invested, this study would not have been possible. This study was performed at the Australian Catholic University in Sydney, NSW, Australia; Sydney Children’s Hospital Network, Randwick, NSW, Australia; and The Children’s Hospital at Westmead, Westmead, NSW, Australia. The research data was presented by ANP at the Bachelor of Physiotherapy Honours Presentation Conference Day at Australian Catholic University on November 2, 2016. The research was submitted to the Australian Physiotherapy Association Momentum Conference and presented on October 21, 2017.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
ANP, MAD, and JMB contributed to the literature search. ANP, MAD, and MH contributed to the acquisition of data. ANP, MAD, MH, JMB, JW, and KJ contributed to the study design. ANP, MAD, MH, and JMB contributed to the analysis and interpretation of data as well as the manuscript preparation. ANP, MAD, MH, JMB, JW, and KJ contributed to the review of the manuscript and approved the version to be published.