
Abstract
Objectives:
To apply a modified ADAPTE process to adapt best practices to a local context for successful implementation of electrical stimulation therapy (EST) for treating pressure injuries in persons with spinal cord injury (SCI).
Participants:
An expert team of health care professionals and a consumer participated in a 2-day workshop to assist in the development of the locally adapted EST document in Southwest Ontario, Canada.
Results:
A process map illustrating the flow of activities to initiate EST for treating pressure injuries in persons with SCI based on the challenges and opportunities existing within this region was created. The team also developed a summary of roles and responsibilities delineating tasks specific to providing EST and identified a set of challenges likely to be encountered.
Conclusions:
The modified ADAPTE process provided a clear and flexible structure to adaptation when used for implementation planning. This article shares some challenges associated with using this process for local adaptation and shares strategies of improvement for future studies aimed at adapting a practice to their local environment.
Introduction
Good clinical practice guidelines deliver research evidence to care providers and health settings (eg, hospitals, community agencies) in a format that is usable. 1 However, to ensure the likelihood that the guidelines will be used, it is important and necessary to adapt the guideline or specific recommendations to the local context, 2 which requires significant involvement of end users.2,3 Adapting practice guidelines/recommendations to a particular environment has many advantages; it enhances the applicability so the adaptation “fits” the local environment, it ensures relevancy and improves the acceptance and adherence to the recommendations, it facilitates users in effective implementation planning, it optimizes the use of existing resources, and it engages knowledge/end users resulting in greater chance of uptake.4,5
Frameworks such as Knowledge-to-Action (KTA) 6 and the National Implementation Research Network (NIRN) 7 refer to adaptation as a critical step to knowledge translation and implementation. KTA recommends selecting and tailoring the intervention to identified barriers and end users. 6 Although the KTA provides useful guidance for implementation, it does not provide a concrete direction on how adaptation to the local context should occur. 6 Comparatively, NIRN recommends a process for local self-assessment and identification of core components to implementation, known as drivers, which would generate change in a specific organization or setting.7–9
In 2009, a group of international researchers, guideline developers, implementers, and users developed the ADAPTE process, 10 a systematic approach for adapting guidelines to enhance the use of evidence-based research. 11 The ADAPTE process consists of 3 phases including setup, adaptation, and finalization. The setup phase outlines the required tasks to be completed before the adaptation process begins, including identifying necessary resources and skills and organizing a panel. The adaptation phase contains the core components of adaptation, including selecting a topic, searching and assessing guidelines, making decisions around how to adapt the guidelines, and drafting an adapted guideline document. Finally, the finalization phase includes an external review in which the feedback of the adapted guidelines is obtained from relevant stakeholders and an updated version would be created. 11 The ADAPTE process is supported by a Web-based tool kit that includes a manual and related tools to help facilitate the process. 12
The ADAPTE process was designed to be flexible, where knowledge/end users are encouraged to customize the process to their own needs and context. Aside from a few studies that illustrated practical examples of how one may use the ADAPTE process for guideline adaptation,11,13–16 there has not been any clear initiative that incorporates the ADAPTE process as part of the implementation planning process for a local context, with a variety of health care providers, working across the care continuum within a regional system of care. However, the elements and approach of the ADAPTE are compatible with achieving an objective of designing a successful implementation process as it can encourage users to detail the practice by operationalizing it to the local environment. 17
In December 2013, a group of researchers centered at Western University in London, Ontario, Canada, undertook an initiative with Parkwood Institute (a local health care organization focused on physical and mental health, with a specialty in spinal cord injuries), the South West Community Care Access Centre (“SW-CCAC”—a regional health agency that coordinates publicly funded home and community care), and local health care providers to improve the management of pressure injuries (previously known as pressure ulcers or pressure sores) in community-dwelling individuals with spinal cord injury (SCI). The use of electrical stimulation therapy (EST) for treating pressure injuries in this population was selected from the Canadian pressure injury best practice guidelines 18 as the therapy to adapt and implement. EST involves applying low levels of electrical current to the wound and/or surrounding tissues. Numerous clinical trials and meta-analyses have shown that EST can speed healing and promote wound closure of pressure injuries.19–21 Despite strong evidence and recommendations by many best practice guidelines, the therapy continues to be unused by frontline community providers due to a number of perceived barriers expressed by a group of local stakeholders. 22 Given these findings, it became apparent that the adaptation process could facilitate the necessary details to enable effective implementation and ensure that the adaptation reflects the local context.
Therefore, the objective of this initiative was to apply a modified ADAPTE process to adapting best practice, with a focus of using EST as a treatment for healing pressure injuries in community-dwelling individuals with SCI in South Western Ontario. A summary of the findings are briefly reported including the challenges and opportunities with implementing EST, identifying task-specific EST duties, and a detailed process map for providing EST to community-dwelling individuals with SCI with pressure injuries. Furthermore, the lessons learned from using a modified ADAPTE process within implementation planning are summarized.
Methods
This initiative was guided by the 3 phases of the ADAPTE process 12 : setup, adaptation, and finalization, including the steps within each. The specific components of each phase and the ordering of the steps were modified to meet the requirements for the EST implementation planning.
Ethics approval was obtained from the Western University Research Ethics Board and the Lawson Health Research Institute. Because the adaptation process formed part of a research study, it was a requirement of the University Ethics Board that all participants of the adaptation process provide written informed consent for their participation.
Setup phase
Step 1: Check whether adaptation is feasible and select a topic
For this exercise, the organizing committee combined steps 1 and 3 of the formal ADAPTE Set Up Phase into an initial step 1. The feasibility of the adaptation (formal step 1) and the selection of the specific topic for adaptation (formal step 3) were informed by a previous extended exercise, known as the “exploration phase” in the NIRN framework. 7 The process and results of that work have been reported in a previous publication. 22 An expert panel of consumers, health care providers, health care system managers, and researchers reviewed the opportunities presented by EST best practices for the treatment of pressure injuries and then identified the barrier and facilitators to EST implementation. Furthermore, a preliminary pressure injuries model of care using EST as a treatment for healing was developed by the expert panel. 22
Step 2: Establishing an organizing committee, and adaptation team
An organizing committee comprised of 6 researchers from Western University, Lawson Health Research Institute, and Saint Elizabeth Health Care led the adaptation initiative. The committee’s responsibilities included identifying members to be a part of the local interdisciplinary adaptation team, organizing the adaptation process (ie, ADAPTE workshop), and overseeing the entire project.
The adaptation team was selected to be representative of key stakeholders across the region that could potentially address and advise on the opportunity for EST implementation and the barriers and facilitators identified in step 1. The team consisted of 17 individuals, of which 12 were from the community including a client service manager from a provincial health agency that coordinates community care (SW-CCAC), a regional service coordinator from Spinal Cord Injury Ontario (a not-for-profit organization dedicated to providing services and advocacy for people living with spinal cord injuries), a clinical lead for the regional wound care program, 2 physiotherapists (PT), a occupational therapist (OT), a registered dietitian (RD), 2 registered nurses in which one was an enterostomal therapy nurse, a personal support worker supervisor, and a team leader for senior supports for daily living. An individual with SCI was involved to ensure that the consumer’s perspective was represented. 23 In addition, there were 4 members of the Pressure Injury Consultation (PIC) team (previously known as the Spinal Cord Injury Pressure Ulcer Team [SCIPUT]) from Parkwood Institute including a PT, OT, RD, and an advanced practice nurse. PIC is a specialized interdisciplinary team that was specifically developed after an EST model of care was created during the exploration phase of this study. 22 Specific clinicians were chosen to be members of the PIC team given their experience working with one another and their expertise in working with individuals with SCI.
The adaptation team was invited to commit to 2 consecutive 8-hour days to attend the ADAPTE workshop. The entire PIC team (9 members) was required to attend 3 additional, 1- to 2-hour sessions to adapt the process of rehabilitation services within Parkwood Institute to complement the EST implementation.
Step 3: Organizing the ADAPTE workshop—the preparatory phase
Over a 3-month period, the organizing committee prepared for the 2-day ADAPTE workshop at Western University and for subsequent meetings with the PIC team. Information regarding the initiative, including the barriers and facilitators to implementing EST that were collected in phase 122 and resources related to the application of EST, was shared with the group to review in advance. The workshop was held on May 17-18, 2015. The additional PIC meetings were held in June 2015.
Adaptation
In the formal ADAPTE process, most of the adaptation phase is focused on collecting, assessing, and coalescing various existing best practices and clinical guidelines (steps 7-14), and the 15th step—“Assess acceptability and applicability of the recommendations”—addresses the questions specific to this initiative (Figure 1). 12 As steps 1 and 3 of the Set Up stage had identified the best practices that would be the subject of this exercise, the work of the adaptation phase in this study was on the 15th step and called step 4.
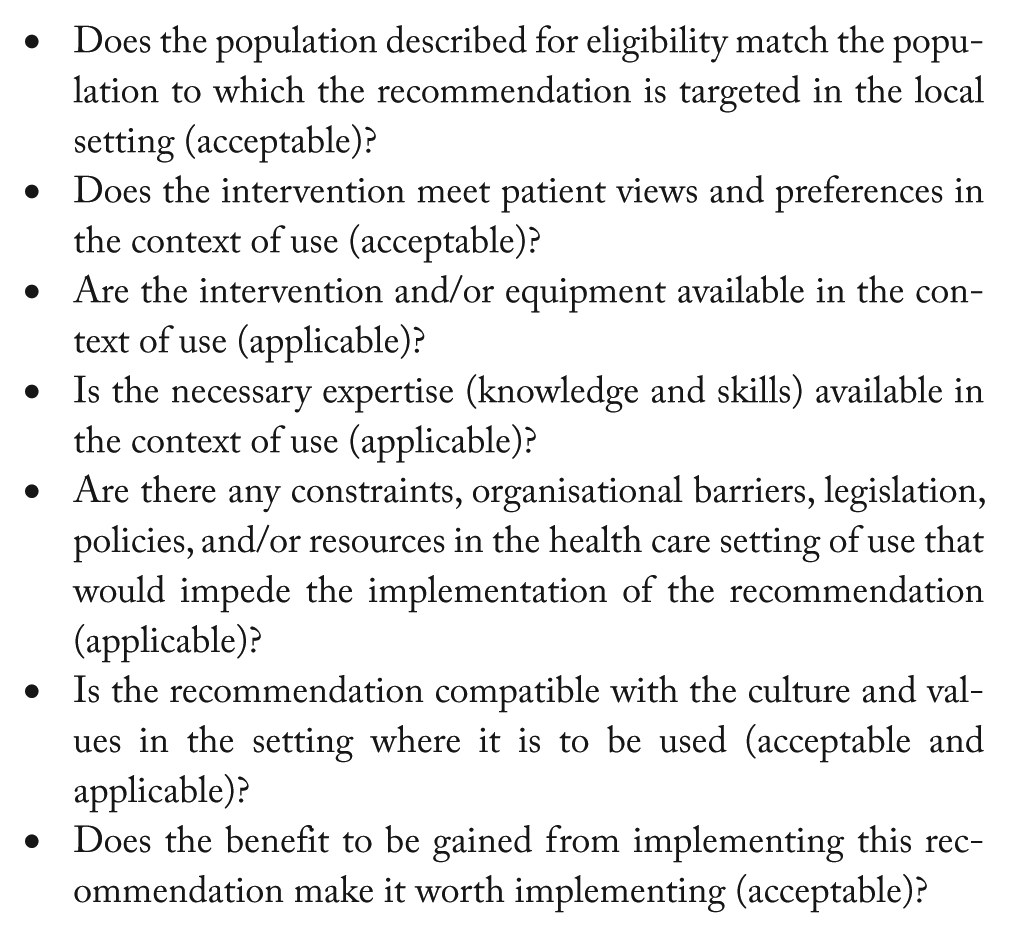
Step 15 of the ADAPTE process: assess acceptability and applicability of the recommendations. 12
Step 4a: The ADAPTE workshop
Two organizing committee members trained in facilitation delivered the workshop. Two members of the organizing committee independently took notes and compared their records after each day to identify critical observations. The workshop was audiotaped for field note verifications. At the end of each day, the organizing committee met and discussed the field notes and observations of progress, contentious issues, and overall progress toward the objectives. Three weeks after the ADAPTE workshop, the organizing committee met again to review the findings and confirm the lessons learned from the workshop. Similarly, a trained facilitator led the PIC team meetings and gathered and consolidated the learning after each meeting. The findings were shared and reviewed with the PIC team within 2 weeks of the final meeting in July 2015.
On the first day, the adaptation team was provided with an overview of the overall research study, with a significant focus on the evidence for the use of EST in pressure injury management. Each member of the adaptation team was then asked to articulate the challenges and opportunities with working in their health care setting and how it may affect the implementation of EST. The team then reviewed the model of care, 22 and discussed issues that might arise as the community aspects of this model are operationalized, with the goal of developing a process map.
At the end of the first day, the task of creating the process map had been delayed due to an extensive debate related to clarity of roles of health care providers who might be involved in EST. The debate centered on whether the providers should be designated in terms of discipline (eg, PT or nurse) or on the basis of a specific skill set acquired by an individual (eg, experience in EST).
On day 2, task-focused assistance was provided by the facilitators to support the adaptation team in mapping out a process illustrating the flow of activities of community providers in initiating EST as a treatment modality for pressure injury management in community-dwelling individuals with SCI. Once a draft process was complete and confirmed by the team, the team worked through a simulated case that had been prepared by the organizing committee in advance. The purpose of the case simulation was to validate the appropriateness of the process map.
Step 4b: The PIC team meetings
The meetings with the PIC team were similarly organized with the objective to develop a process that will guide how the team would work together to provide a comprehensive assessment of the patient with SCI with a pressure injury to provide client-specific recommendations and support to the health care providers who would be involved in delivering the community-based EST.
To test the PIC’s process map, a test patient with a pressure injury was recruited to evaluate a simulated clinical experience. Unfortunately, the test patient had a severe wound infection and was admitted to a local acute hospital for a few weeks to receive treatment. However, the team did learn some valuable lessons and insight from undergoing part of the simulated clinical experience and revised their initial process map accordingly.
Following the workshop and the meetings, the organizing committee reviewed the meeting notes and recordings and categorized and refined the challenges and opportunities to implementing EST in the local environment. The committee also further refined the sequential process maps and created a visual interpretation of the activity flow.
Finalization
Step 5: Drafting a document for local adaptation of EST
A summary of the issues discussed and resolved in the ADAPTE workshop, and the PIC team meetings was merged with the sequential process maps in a draft document and shared with the PIC team and the adaptation team for content verification.
Step 6: External review by local stakeholders
The draft document for local adaptation of EST was also shared with a broad group of local stakeholders. This group included regional managers of SW-CCAC, regional directors and managers of local community agencies, local vendor for EST devices, and the director of rehabilitation and the coordinator of SCI rehabilitation at Parkwood Institute. The local stakeholders were asked to review the document and provide specific feedback. Because the SW-CCAC stakeholders had an extensive list of comments on the draft documents, additional face-to-face and teleconference communications were facilitated over a 4-month period until consensus was reached.
Results
Challenges and opportunities to EST implementation
Seven challenges and opportunities with implementing EST in the local environment emerged from the discussions during the ADAPTE workshop (Table 1). The challenges reported included lack of communication among providers, inconsistent care providers in the community, and lack of training and knowledge of pressure injury and EST. The opportunities to implementing EST included the multitude of funding models accessible to clients, the ability to facilitate interdisciplinary care, and the transition into self-management in the community.
Challenges and opportunities with implementing electrical stimulation therapy in the local environment.

EST-specific tasks and responsibilities
The adaptation team was also asked to review the various steps associated with applying EST and delineate which regulated and/or unregulated care provider could perform specific tasks. Throughout this discussion, there was considerable debate over whether implementation should be guided by designating specific disciplines as the key providers of EST or whether by designating any health care provider with the requisite skill set and experience. Consensus was eventually reached to delineate roles and responsibilities of EST-specific tasks (Table 2).
Roles and responsibilities involved in providing EST for treating pressure injuries in community-dwelling individuals with SCI.
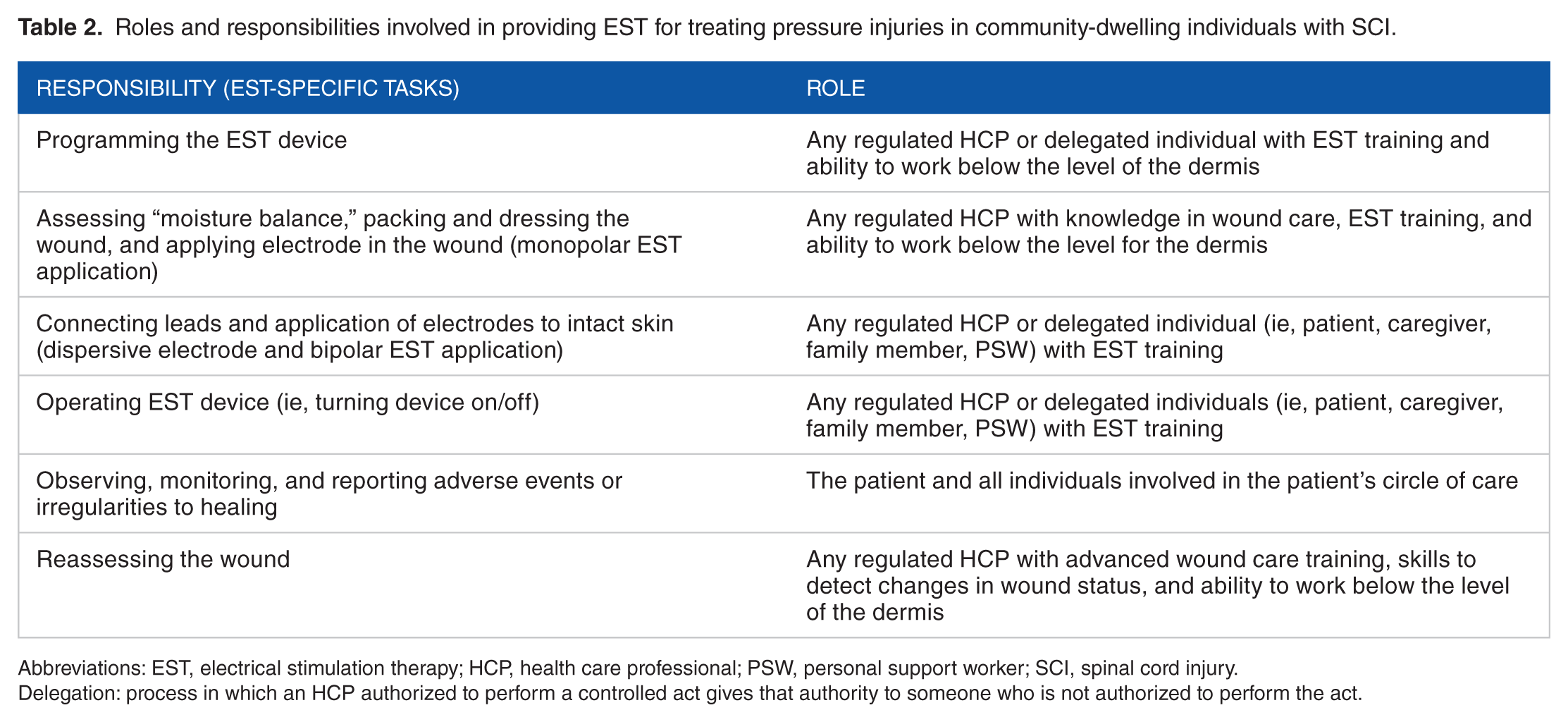
Abbreviations: EST, electrical stimulation therapy; HCP, health care professional; PSW, personal support worker; SCI, spinal cord injury.
Delegation: process in which an HCP authorized to perform a controlled act gives that authority to someone who is not authorized to perform the act.
Process map
A process map for providing pressure injury best practices, specifically EST, to individuals with SCI (Figure 2) may not be feasible or useful for all environments; however, sections can be taken or adapted to fit another local context.
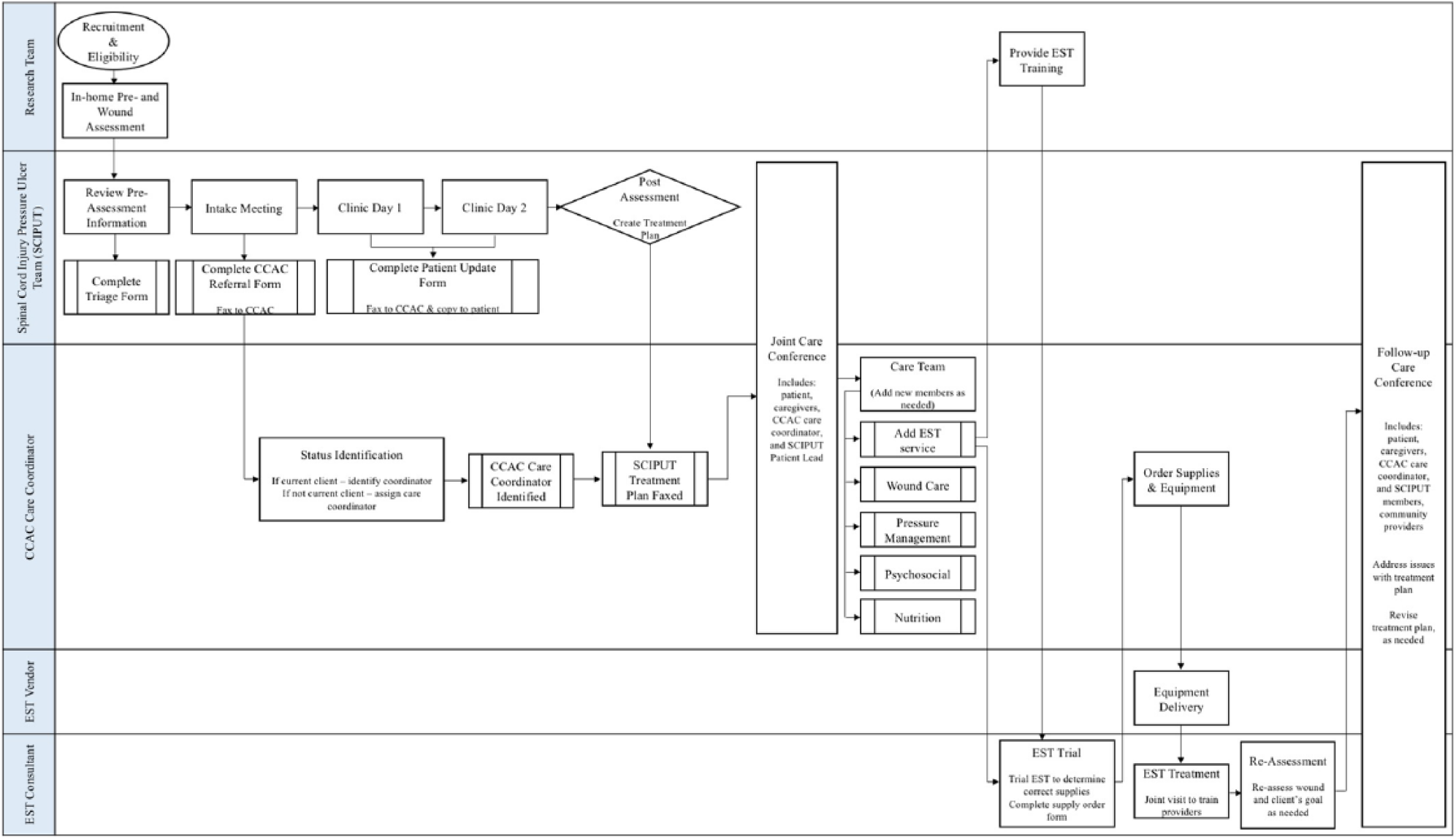
Initial process map for initiation of EST in community-dwelling persons with SCI with pressure injuries that will be tested in cycle 1. EST indicates electrical stimulation therapy; SCI, spinal cord injury.
There are 4 main organizations in Southwest Ontario that frequently interact with one another: the PIC team CCAC care coordinator including the contracted agencies, the vendor of EST equipment, and the EST consultant who has the expertise in overseeing the treatment with EST. As this is also a research initiative, the process map includes the research team to assist with screening, recruiting, and supporting the patient throughout the process. The subsequent sections briefly summarize the key components to this process map.
Pressure Injury Consultation
From intake assessment to debrief—Once a patient is referred to the PIC team, the team will meet to review the patient’s pre-assessment documents, including medical history, medications, nutrition, wound assessment, and blood work, if available, and the triage form which includes data regarding patient’s home environment, equipment, and transfers. This will allow the team to determine which assessments are valuable to complete when the client attends the clinic days. In addition, a lead from the PIC team will be identified for the patient. Following the clinic days, the PIC team will have a debrief meeting where they will review their clinic findings and develop a treatment recommendation suitable for the patient. This treatment recommendation may or may not include EST depending on the client’s eligibility for this therapy.
Initial joint care conference
A teleconference will be scheduled to review and negotiate the treatment plan with the CCAC care coordinator, the patient and their caregivers, and the PIC team patient lead. The patient must agree to the treatment recommendations in order for the services to be provided.
Treatment
Each treatment recommendation including EST will be conducted in the community using CCAC-contracted service providers or the client’s existing care team. If EST is recommended, a member of the research team with significant EST experience will perform bedside training with the community provider so they have hands-on experience with EST and are able to provide the therapy using the recommended protocol.
Follow-up joint care conference
After a few months of service, a follow-up joint care conference including the PIC team, CCAC care coordinator, the client and their caregivers, and the providers delivering community-based services will be scheduled. During this meeting, the group will review the client’s progress, address any issues that arose with any of the recommendations, identify wound status, and revise the treatment recommendations as required.
Reflection
In addition to the components summarized above, we asked the team to take some time and reflect independently and record things they learned or were feeling at the end of each workshop day. Many members of the adaptation team appreciated the collaborative nature of the meeting and valued the unique views of different providers across organizations and setting. Furthermore, the adaptation team understood the importance of improving pressure injury care and was motivated to develop a process that establishes best practices, specifically EST, in treating pressure injury in community dwelling persons with SCI. Although there were positive reactions to the initiative after the first day, many felt frustrated at the complexity of the current system and trying to develop a quality process that is efficient, cost-effective, and realistic within the local health care system. However, following the second day, the perceptions shifted to a state of relaxation and excitement as the process map became clearer through discussion and illustration.
Discussion
Using a modified ADAPTE process, a group of local stakeholders developed a guide for the adaptation of EST for treating pressure injuries in individuals with SCI living in Southwest Ontario. A sequential process map illustrating the flow of activities to initiate this therapy was developed while taking into account the challenges and opportunities to implementing EST.
Throughout the 3 stages of the ADAPTE process—setup, adaptation, and finalization, we faced a multitude of challenges and learned some lessons that may be useful to others interested in using the ADAPTE process during implementation planning.
The composition of the adaptation team is critical, as they are the dominant factor in the adaptation of guidelines and will ensure its relevancy and applicability to the local organizations. Our multidisciplinary group, composed of local providers from the community and a tertiary rehabilitation facility, and an SCI consumer representative, exposed us to diverse areas of expertise and perspectives. Although we had great success working with the adaptation team, there were some key lessons learned.
First, consider reducing the number of members on the adaptation team. Given the size of the adaptation team and their distinct views, a great number of challenges to EST implementation were brought to the table and unfortunately could not all be resolved in the course of 2 days. Reaching consensus took considerable amount of time given the various perspectives. A group of 9 or 11 relevant and informative stakeholders has been shown to be an optimal size for guideline adaptation, 5 and so, perhaps, it would be advisable to convene 2 separate groups with some time in between—one to raise the issues and the second to negotiate the solutions. We also found that it was imperative that all adaptation team members attend the entire workshop. Although the adaptation team included a client services manager from South West CCAC, the representative was only able to attend for a few hours on the second day and was more heavily involved as an external reviewer. Receiving community care in Southwest Ontario is highly dependent on CCAC as they coordinate community-based services using contracted agencies. In retrospect, their involvement during the ADAPTE workshop would have been critical to assist in sorting out many of the issues that arose during the external review phase with the process map and therefore would have limited the negotiation time period.
During the adaptation phase, including the ADAPTE workshop and the drafting of the document for local adaptation of EST, we were faced with 3 main challenges. One perceived challenge was the lack of initial understanding of the purpose of the workshop by the adaptation team. When asked to reflect on the workshop at the end of the first day, many felt uncertain or confused and did not completely understand the objective the ADAPTE workshop. Supplementary material (ie, agenda and background data) was provided to the adaptation team in advance, and due to time constraints, only a brief introduction was provided on the first day of the ADAPTE workshop. Interestingly, when each member had a chance to do their own personal reflection that night, many had a better understanding of the initiative on the following workshop day. It seemed as though a “light-switch” had turned on in their minds, which allowed them to contribute in a more productive manner on the second day. Many realized the complexity of the current issues and the difficulties of implementation.
The adaptation phase requires sustained dedication, time, and commitment by the organizing committee and adaptation team. We allocated 2 full workshop days and subsequent PIC meetings to create a guide for EST adaptation that encompasses detailed information and a process map to EST implementation. In Canada, there are 2 different streams or models in which patients can receive care. The public care model involves the client receiving provider services through CCAC, and the private care model involves the client hiring their own provider services through personal income or private insurance. Due to lack of time and resources, the team was unable to create a process map for the private stream. Therefore, based on our experience, we would consider increasing the number of workshop/meeting days; however, there are repercussions for doing so. Although our adaptation team was invested and very motivated in participating in this initiative, most of them had full-time caseloads making it difficult for them to take time away. Therefore, increasing the number of days will most likely lead to less involvement or the need for greater financial compensation to team members.
During the external review process in the finalization phase, we were faced with the most significant challenge. Representatives from CCAC viewed the process map and reported significant policy and procedural barriers. Multiple meetings over a 4-month period were held to resolve these issues and create a practical process map. Within the first couple of meetings, we realized the importance of hiring professional facilitators with no stake in any outcome to mediate these meetings. Although hiring professionals can be costly, it can result in significant benefits. The meetings were more productive, resulting in fewer and shorter meetings, and improved the relationship between the research team and the stakeholders from CCAC. As stated previously, these meetings may have also been less challenging if full participation by a CCAC representative was available during the 2-day workshop; however, the creation of the process map did provoke discussion, and without it, the issues may have not been obvious at the beginning.
Conclusions
We developed a document for adapting EST locally using a modified ADAPTE process.
A detailed process map outlining the flow of activities for providing EST to community-dwelling individuals with SCI was developed based on the opportunities and challenges to implementing EST into practice expressed by local representatives. The team also delineated roles and responsibilities for tasks associated with performing EST.
A number of challenges were faced throughout the ADAPTE process; however, we were able manage the issues as they came and provide some lessons learned to those who wish to pursue a similar approach of using the ADAPTE process during the planning phase of implementation.
Future research
We will be field-testing this locally adapted EST plan using iterative Plan, Do, Study, Act cycles 24 with a sample of community-dwelling individuals with SCI experiencing pressure injuries. The field tests will examine not only clinical outcomes such as healing but also, more importantly, outcomes related to practice change such satisfaction with the program/model, frequency of consultations, cost-effectiveness, and EST utilization. By testing this model locally, we will be able to determine the feasibility of implementing best practices such as EST in the community in individuals with SCI and pressure injuries at a provincial or national level.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Rick Hansen Institute (Grant #G2015-34). Deena Lala received support from Ontario Graduate Scholarship and the Siskind Studentship in Spinal Cord Injury Research (Grant #017-1516). Dr. Dalton Wolfe was supported by a collaborative mentorship agreement from Ontario Neurotrauma Foundation and Rick Hansen Institute through grant # 2011-ONF-RHI-MT-930.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
PEH, PH, DW and DL were involved in study conception and design and drafting the manuscript. Analysis and interpretation of data were completed by PEH, PH and DL.