
Abstract
Background:
Hip fractures are common, expensive and lead to considerable morbidity and mortality. An ageing population in the United Kingdom means that rates of this injury are increasing, making them a pressing public health issue. The National Institute of Health and Care Excellence (NICE) recommends that extramedullary implants are used over intramedullary nails to fix intertrochanteric fractures, which make up half of all hip fractures. However, there is currently no guidance on the preferred type of extramedullary device whether this be the commonly used dynamic hip screw (DHS) or another newer device. It has been suggested that a percutaneous compression plate (PCCP) can reduce complications and improve functional outcome compared with the traditional DHS.
Review Question:
In patients with intertrochanteric hip fractures, is the PCCP more effective than the DHS in terms of relevant intraoperative and postoperative outcomes such as blood loss, implant failure, and mortality?
Literature Search:
We first searched for relevant information in the NICE Clinical Guideline on Hip Fracture Management (CG124), then National Health Service (NHS) evidence for Clinical Knowledge Summaries, then the Cochrane library for systematic reviews. Finally, we conducted an electronic search of the PubMed database.
Review Findings:
We selected five systematic reviews and eight primary studies for review. The main findings were that the PCCP was associated with significantly less blood loss, fewer blood transfusions, and shorter operating times compared with the DHS. However, no significant differences were found in postoperative pain, orthopaedic performance, and mortality rates between the two methods. There was no comparison of cost-effectiveness between the two methods.
Conclusions:
The PCCP is superior to the DHS in terms of intraoperative blood loss and, potentially, non-orthopaedic postoperative complications such as deep vein thrombosis and nosocomial infection. However, there was no significant difference in mortality rates between the two methods. Current studies on this topic have several methodological issues and some are of relatively poor quality. Further higher quality research and cost-effectiveness are necessary to further evaluate the efficacy of these methods.
Introduction
Hip fractures are a very common cause of hospital admission in the United Kingdom. Around 75 000 patients suffer a hip fracture each year, at considerable cost to the National Health Service (NHS) – more than £2 billion. 1 Hip fractures are becoming more common due to an ageing population, with an approximate year on year increase of 1%. 2 Over 90% of patients are more than 65 years of age and often have multiple comorbidities. 3 Unsurprisingly, hip fractures are a leading cause of mortality and morbidity among elderly patients. 4 Therefore, hip fractures represent a crucial public health issue with their optimal management being vital for both patient and health service, particularly in the current climate of budget cuts and increasing pressure on the service.
In this evidence review, we will focus on the management of extracapsular fractures (distal to hip joint). In particular, we will look at trochanteric fractures, which make up around half of hip fractures, and their surgical outcomes. The best management has been debated for over 30 years; the aim is to achieve a stable fixation while simultaneously allowing early recovery. The failure of these implants is related either due to the type of fixation used or the stability of the fracture. 5 Over the years, several methods have been proposed to provide optimum fixation. 6 It has been shown recently that prompt surgical management (within 24 hours) using internal fixation under regional anaesthesia reduces mortality rates. 7
The National Institute for Health and Care Excellence (NICE) guidelines for hip fracture management detail the surgical procedure for these trochanteric fractures: Use extramedullary implants such as a sliding hip screw in preference to an intramedullary nail in patients with trochanteric fractures.
8
It has been shown elsewhere, such as in a 2014 Cochrane Review, that a sliding hip screw (dynamic hip screw in this review) is superior to an intramedullary nail and further comparison with intramedullary nail methods is not a priority. 9 However, NICE does not explicitly state the optimum extramedullary implant, highlighting the uncertainty and debate surrounding this. In this evidence review, we will be comparing the use of 2 different extramedullary implants: dynamic hip screw (DHS) and percutaneous compression plating (PCCP).
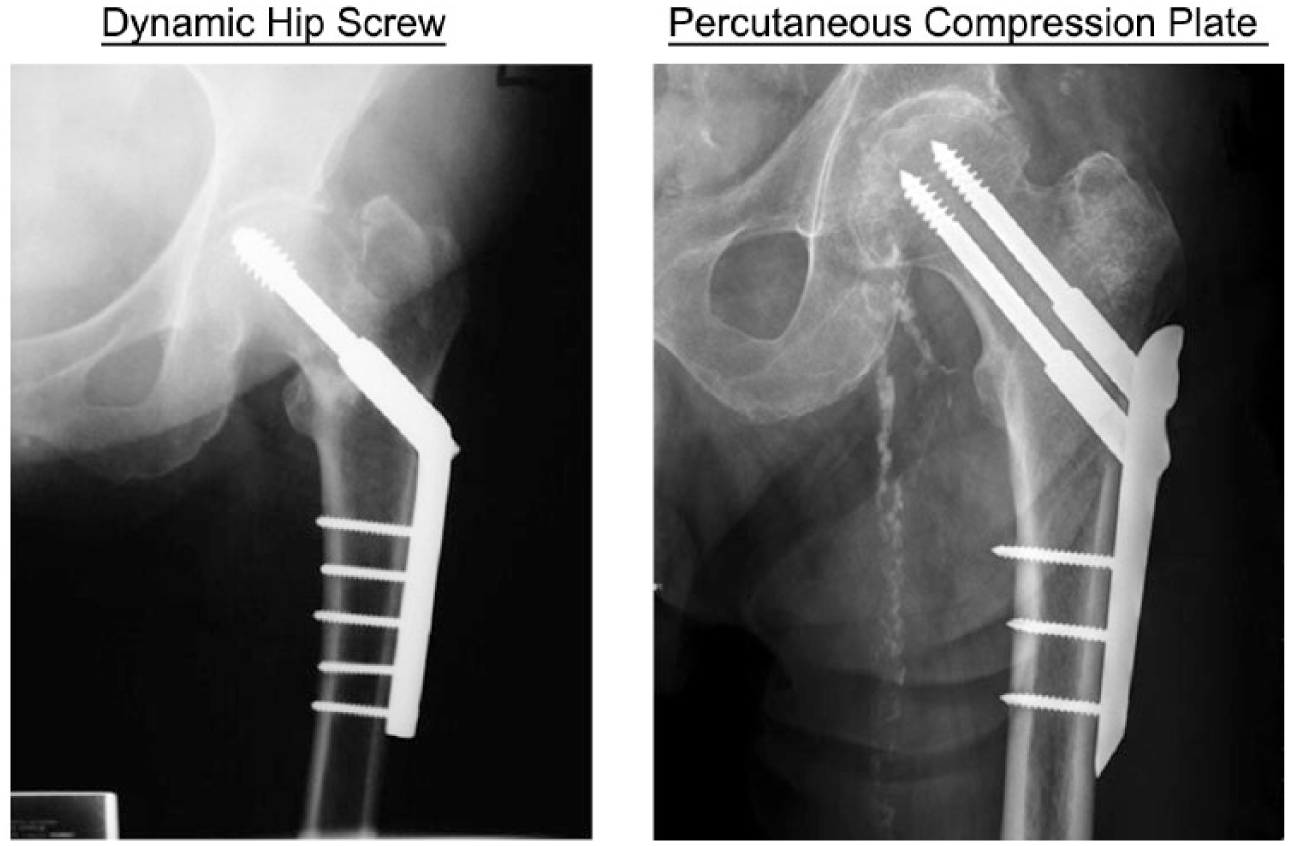
Over several years, the DHS has demonstrated effective stabilisation of trochanteric fractures with excellent functional outcomes. 10 The DHS comprises a plate and screws applied to the lateral side of the femur and allows the fracture to collapse in a controlled fashion, providing stability while allowing prompt postoperative weight bearing.11,12 The DHS is used extensively in NHS practice, and results from the National Hip Database for 2016 show that around 80% of trochanteric fractures receive the DHS implant. 13
In the late 1990s, Gotfried proposed a new surgical technique for the management of intertrochanteric fractures using the PCCP. It was suggested this new implant has fewer complications and better outcomes when compared with the DHS. 14 Percutaneous compression plate is a minimally invasive technique (inserted via 2 small ports) and provides increased rotational stability (uses 2 screws instead of 1). 15 Figure 1 shows a radiological comparison of the 2 implants.
In this literature review, we will evaluate current literature to examine important intraoperative and postoperative complications to determine whether PCCP is a preferable method of fixation compared with DHS.
Methods
Search strategy and inclusion/exclusion criteria
We first searched for high-quality secondary sources such as clinical guidelines from NICE. Percutaneous compression plate was not mentioned in the most recent guideline on hip fracture management in CG124 published in June 2011 and last updated in March 2014.
Therefore, we then searched for Clinical Knowledge Summaries on this subject using NHS evidence. The following search terms were used sequentially:
However, this did not return any relevant documents.
Following this, we consulted the Cochrane library for systematic reviews on this subject with the following search term:

This returned one relevant systematic review which was included in this study. 11
Finally, we searched for primary sources with an electronic search of the PubMed database using the search term on February 21, 2017:

We reviewed the identified studies according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 18 with a pre-defined set of inclusion/exclusion criteria. Studies were first reviewed by title, with all eligible studies proceeding to abstract review. Then, studies deemed ineligible on abstract review were excluded, with the remaining studies proceeding to full-text review. The reference list of reviewed articles was consulted to potentially identify further studies not identified at electronic search.
Inclusion/exclusion criteria
All included studies compared intraoperative and postoperative outcomes for PCCP and DHS methods of fixation for intertrochanteric fractures of the hip. Studies were excluded if they were not conducted on humans, cadaveric, or not in English language. Furthermore, studies were excluded if they did not compare the PCCP method with DHS, included fractures other than intertrochanteric, or did not report relevant outcomes. Finally, one study was excluded as it was not available in full-text form. Figure 2 displays the literature search process.
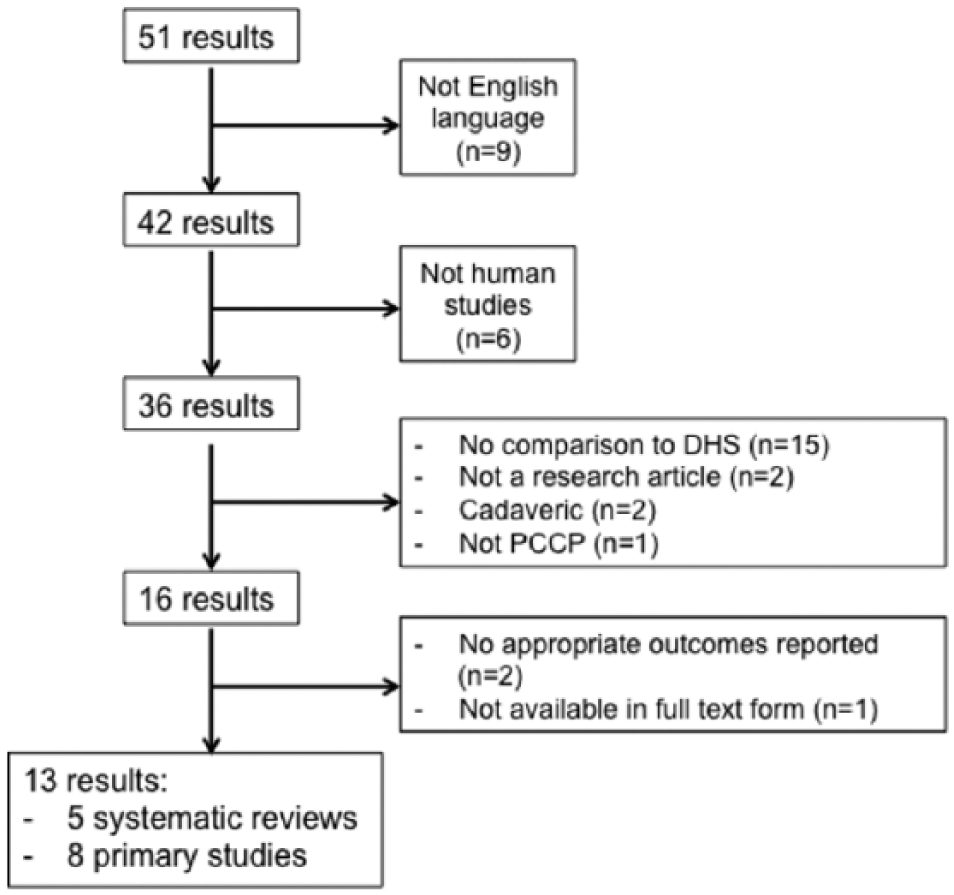
Literature search. DHS indicates dynamic hip screw; PCCP, percutaneous compression plating.
Data extraction
From each included study, relevant intraoperative and postoperative outcomes for both PCCP and DHS groups were obtained. An outcome was only included in this review if more than one primary study and more than one meta-analysis reported it.
Data analysis
No original data analysis has been undertaken as part of this review. Instead, findings of the included studies have been described.
Quality assessment
The studies we reviewed were assessed using CASP (Critical Appraisal Skills Programme) checklist tools by at least 2 of the authors. 19
Results
Characteristics of included studies
Five systematic reviews were included in this review.11,20–23 Four of these were from China20–23 and one was from the United Kingdom. 11 The number of studies included in these reviews ranged from 5 to 14.20,21,23 Both randomised and non-randomised studies were included in these reviews (Table 1).
Characteristics of included systematic reviews.

Abbreviations: NRS, non-randomised study; qRCT, quasi-randomised controlled trial; RCT, randomised controlled trial.
Eight primary studies from different countries were included in this review17,24–30 (Table 2). Seven of the primary studies were randomised controlled trials (RCTs)17,24,26–30 and one was a retrospective non-randomised trial 25 (Table 4). The number of participants ranged from 68 to 280.25,26
Characteristics of included primary studies.

Abbreviations: NRS, non-randomised study; P-RCT, prospective randomised controlled trial; qRCT, quasi-randomised controlled trial; SB, single blinded.
Systematic review and meta-analyses review results
The findings from the 5 meta-analyses from the systematic reviews are summarised in Tables 3 and 4. Every study except that by Parker and Das 11 found that the PCCP method was associated with significantly less intraoperative blood loss. All of the meta-analyses found that a significantly higher number of blood units were given to DHS patients compared with PCCP patients.11,20–23 The study by Cheng et al 23 was the only one to find that PCCP was associated with a significantly reduced fall in haemoglobin compared with the DHS technique. The studies by Cheng et al 23 and Ma et al 22 found that the PCCP technique had significantly shorter operation times and fewer patients that received a blood transfusion compared with the DHS group. The studies by Long et al 20 and Cheng et al 23 found that the PCCP group had significantly fewer postoperative complications (Tables 3 and 4).
Intraoperative outcomes for PCCP and DHS as reported by meta-analyses included in this review.

Abbreviations: DHS, dynamic hip screw; Hb, haemoglobin; NSD, no significant difference; PCCP, percutaneous compression plating.
Bold formatting indicates significant difference at P = .05 as reported; — indicates not reported.
Postoperative outcomes for PCCP and DHS as reported by meta-analyses included in this review.
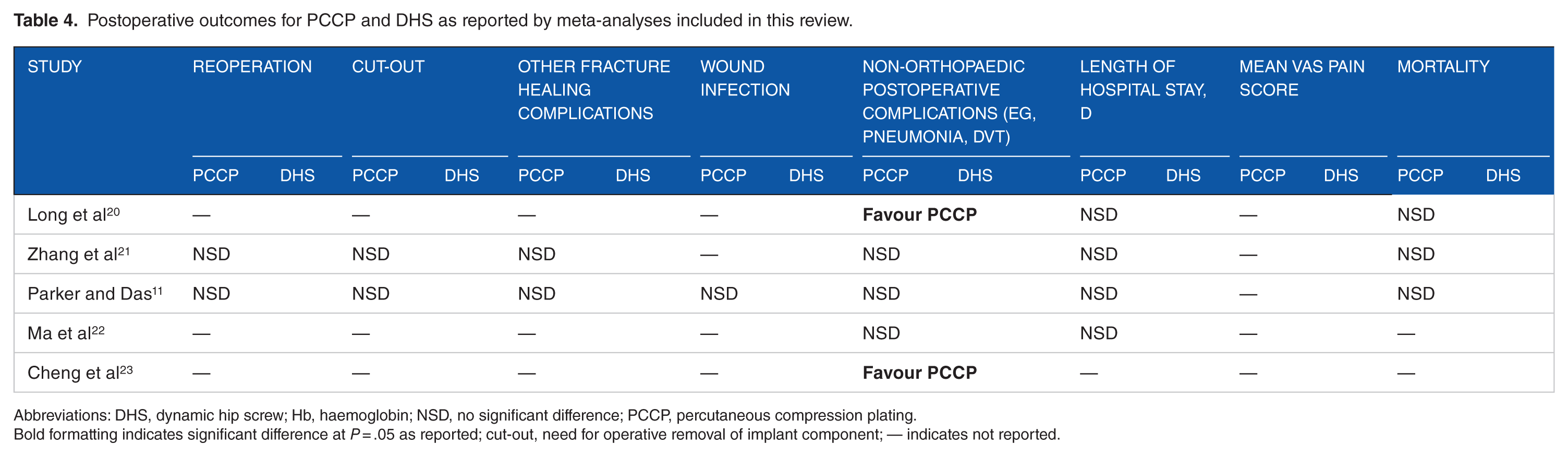
Abbreviations: DHS, dynamic hip screw; Hb, haemoglobin; NSD, no significant difference; PCCP, percutaneous compression plating.
Bold formatting indicates significant difference at P = .05 as reported; cut-out, need for operative removal of implant component; — indicates not reported.
No significant difference was found between the PCCP group and DHS group in terms of postoperative length of stay,11,20–22 orthopaedic complications,11,21 or mortality rates11,20–23 (Tables 3 and 4). Notably, none of these meta-analyses included postoperative pain in their analyses (Table 4).
Primary study review results
The 8 primary studies that were identified were selected for review. Their findings are summarised in Tables 5 and 6. Of the 8 studies, 5 found that the operating time for PCCP was significantly shorter than that for DHS.24,26–28,30 Only 1 study reported that DHS operating times were significantly shorter than PCCP times, 29 whereas the remaining 2 studies found no significant difference between the 2 methods.17,25 In addition, 3 studies found that DHS was associated with a significantly higher intraoperative blood loss compared with PCCP.17,24,26 The remaining study by Kosygan et al 29 reported no significant difference between the 2 methods. The study by Brandt et al 28 found that significantly more DHS patients received a blood transfusion compared with PCCP patients. The other 2 studies found no significant difference between the 2 techniques.17,24 Janzing et al 30 were the only group to report a significantly lower mean visual analog scale postoperative pain score in the PCCP group compared with the DHS group.
Intraoperative outcomes for PCCP and DHS as reported by primary studies included in this review.

Abbreviations: DHS, dynamic hip screw; Hb, haemoglobin; PCCP, percutaneous compression plating.
Bold formatting indicates significant difference at P = .05 as reported; — indicates not reported.
Postoperative outcomes for PCCP and DHS as reported by primary studies included in this review.

Abbreviations: DHS, dynamic hip screw; Hb, haemoglobin; PCCP, percutaneous compression plating.
Bold formatting indicates significant difference at P = .05 as reported; cut-out, need for operative removal of implant component; — indicates not reported.
Measured 6 months postoperatively.
No significant difference was found between the PCCP group and DHS group in terms of length of stay,17,24,27,29 mortality,17,25,26,29,30 non-orthopaedic postoperative complications,17,28 reoperation rate,17,28–30 implant failure,17,26,29,30 fracture healing,17,24,26,28–30 postoperative fall in haemoglobin,17,25,29,30 or units transfused.17,25,26,29,30
Quality Assessment of Included Studies
The quality of each study included in this review was critically appraised. In terms of patient inclusion and exclusion criteria, only Ma et al 22 excluded studies with pathological or metastatic fractures, unstable fractures, and contralateral fractures.
The search strategies used by the reviews were thorough. Adequate databases, including EMBASE, MEDLINE, the CCRCT, and the World Health Organization (WHO) International Clinical Trials Registry, were searched with definitive search terms in all reviews. However, Zhang et al, 21 Parker and Das, 11 and Long et al 20 did not search for any non-English literature and only Cheng et al, 23 Parker and Das, 11 and Ma et al 22 looked through reference lists for relevant studies. Ma et al 22 was the only study to search for unpublished literature, giving it the greatest scope in terms of search strategy. Sample sizes throughout the trials were small which may underpower the results of the reviews.
Bias assessment was performed by 2 authors independently in all reviews. A number of acceptable methods were used, including the Cochrane tool and Coleman methodology score. Zhang et al 21 and Long et al 20 had strict exclusion criteria, excluding quasi-randomised controlled trials (qRCTs). However, Cheng et al 23 and Ma et al 22 allowed non-randomised trials and found a high risk of selection bias. Ma et al 22 found a universally unclear risk of performance, attrition, and detection bias but a low risk of reporting bias. Zhang et al 21 identified 2 trials with a high risk of attrition bias, and both Zhang et al 21 and Long et al 20 found an unclear risk of performance and detection bias in all but one trial. Only one trial, by Yang et al, 26 blinded outcome assessment which may reduce risk of detection bias. The only review to account for surgeon experience in assessing bias was the work by Parker and Das 11 ; they found that only 2 RCTs, those by Kosygan et al 29 and Peyser et al, 17 included this. The presence of publication bias was found in all reviews apart from Parker and Das. 11 This may over-represent studies that indicate a difference between PCCP and DHS.
Two RCTs, Janzing et al 30 and Brandt et al, 28 used the same data set. These were included in the reviews by Zhang et al, 21 Ma et al, 22 and Long et al 20 and may be over-represented in meta-analyses. However, these studies scored well in the bias assessment and so their data are likely valid.
Discussion
This review compares the performance of the DHS and PCCP for fixation of intertrochanteric fractures in terms of intraoperative and postoperative outcomes. The outcomes of 5 systematic reviews and 8 primary studies were compared. The main finding is that PCCP reduces intraoperative blood loss compared with DHS while providing good fixation for intertrochanteric fractures, which has also been shown elsewhere. 31
The systematic reviews focused on slightly different outcomes which made comparison more difficult. For example, blood loss was measured, either through postoperative haemoglobin drops or intraoperative losses in millilitre. Nevertheless, all reported length of surgery, blood loss, and postoperative complications. Of the 5 reviews, 4 reported mortality,11,20,21,23 transfusion rate,11,22,23 volume,11,20,21 and hospital stay.11,20–22 Only 2 of the reviews reported implant-specific complications (eg, reoperation11,21), fall in Hb,11,23 and fracture healing complications.11,21
The data regarding operation time, blood loss, transfusion rate, and hospital stay length were highly heterogeneous, with almost all consistently scoring in the high 90% range on the I2 test (χ2 was also used) in all systematic reviews.
There are issues concerning some of the outcomes. For example, operation time is affected more by fracture type than procedure, 32 something which was taken into account only by Ma et al, 22 which included only AO/OTA 31.A1-A2 type fractures (stable fractures). In addition, other reviews included trials which used different fracture classifications, either the American Orthopaedic or the Evans fracture type, which could potentially lead to patients having different severity of fracture. Surgeon experience and familiarity with the procedures is also a crucial factor influencing operating time. Some RCTs did provide a learning curve for surgeons to become familiar with the procedure, such as Cheng et al 24 ; only the review by Parker and Das 11 specifically considered this.
Length of hospital stay is relevant yet difficult to compare between reviews as it is heavily impacted by country and hospital-specific factors, patient comorbidity, and rehabilitation, none of which were controlled for. Other outcomes are also dependent on various confounding factors such as transfusion rate as different hospitals/countries use different guidelines for transfusion.
There were some problems identified with the PCCP method in the studies, which may hinder wide-scale use. For example, the PCCP is a more challenging operation than the DHS 30 which may make it unfeasible to train surgeons in the time-pressured environment of the NHS. In addition, the cost of this implant has not been compared with the DHS. 33 The lack of information regarding the cost of PCCP may be indicative of high cost. Cost-effectiveness is extremely important and decisive factor in many treatments.
The most recent studies improved in quality, including only randomised trials. This is important to consider when interpreting the results, as this may have reduced the number of significant differences seen in later trials between the 2 methods. Generally, the methodology in these systematic reviews, in particular, those by Zhang et al 21 and Long et al, 20 is valid. The review by Ma et al 22 had good methodology but included qRCTs which introduced risk of selection bias into the results. The study by Cheng et al 23 was generally well conducted, with an extensive search strategy and large number of trials, although the inclusion of non-randomised trials and qRCTs makes its data less reliable than other reviews. The review by Parker and Das 11 had generally good study design and considered factors such as the impact of surgeon experience, which the other studies did not, as well as looking at more comprehensive outcomes. The outcomes chosen by the other reviews could have been more complete with pain levels, a very important surgical outcome 34 and mobility largely absent. The heterogeneity associated with some of the outcomes measured was unavoidable but significant. Overall, we thought that all of the reviews met an acceptable level of evidence while also highlighting the need for further research.
This study comprehensively reports the findings of all relevant studies comparing the performance of PCCP and DHS for intertrochanteric fractures and assesses the quality of the evidence thoroughly. A limitation of this work is the lack of an original meta-analysis.
The number of patients used in the systematic reviews was relatively small and from different countries which makes it difficult to apply these results directly to a UK population. However, we believe that these results warrant further research into the possible benefits of PCCP for the UK population. It may be helpful to set up a registry for trochanteric fracture implants and their outcomes, similar to the National Joint Registry. This could be useful as it may track differences in the UK setting between treatment modalities and their outcomes and highlight any important differences in outcomes.
Conclusions
In conclusion, PCCP appears to demonstrate an advantage over DHS in intertrochanteric hip fractures by reducing blood loss. Current RCTs and the subsequent systematic reviews are of varying quality. Further research is warranted in this area as the PCCP may reduce postoperative complications making it an attractive option in particularly frail patients. Further cost-based analysis would be useful first before this could be applied to the UK situation.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
JHS performed the literature search and JHS and AC wrote the manuscript. All authors reviewed the papers and the manuscript.