
Abstract
Background:
Knowledge of osteoporosis plays an important role in developing attitudes toward the disease which in turn affects health care behaviors of both public and patients.
Objective:
Despite the increasing incidence of osteoporosis in Malaysia, many people still have limited information about the risks of this disease. This information includes knowledge of physical activity, adequate calcium intake, and adequate vitamin D intake. This study aims to assess the osteoporosis knowledge using osteoporosis knowledge test and to find the associated factors influencing osteoporosis knowledge of the users and nonusers of warfarin.
Methods:
A case-control study was used to assess the osteoporosis knowledge from the study sample. A self-administered questionnaire was used for data collection.
Results:
A total of 140 controls and 130 patients using warfarin were included in this study. This study indicated that most of the participants (84.2%) have a low score of knowledge of osteoporosis, and only 15.8% of the study sample was found to have a high score of knowledge. Patients using warfarin were more knowledgeable about osteoporosis compared with controls.
Conclusions:
The findings of this study revealed that most people have inadequate knowledge about osteoporosis. The health care professionals should play an active role in educating their patients and community about the risk factors of osteoporosis.
Keywords
Introduction
The ways that people take to manage their health are influenced by their knowledge and attitude toward osteoporosis. Knowledge is the basics of understanding and reacting toward health issues. In terms of disease prevention, knowledge of osteoporosis is integral to patients in preventing and reducing risk of fractures. The knowledge involved those with suitable physical activities, sufficient dietary requirement of calcium and vitamin D, fall prevention, and osteoporosis test. 1 The prevalence of osteoporosis-related fractures has increased in many countries around the world, and this trend is expected to continue as the population ages. 2 A study in Malaysia reported that the incidence of hip fracture in Malaysia among people aged 50 years and older was 90 per 100 000. There was a marked increase in the incidence among the older age group and women. In addition, Chinese people had the highest incidence of hip fractures compared with Malays and Indians. 3 Patients’ knowledge and osteoporosis preventive behavior could be increased with the help of health care professionals 4 and screening programs. 5 Some behaviors associated with the lifestyle indeed influenced the level of osteoporosis knowledge. 6 Lack of awareness is the main reason for high prevalence of low bone mass. 7 However, few studies have focused on patients with chronic diseases or use of such medicines that may lead to risk of secondary osteoporosis. 8 It is important to explore patients’ knowledge of osteoporosis by identifying the source of information. However, numerous measures have been taken to improve bone health and osteoporosis management through published Malaysian guideline. 9 Therefore, education is necessary to increase the level of knowledge of patients to improve their bone health. This study aimed to assess the osteoporosis knowledge in users and nonusers of warfarin and to find the associated factors that affect the total score of osteoporosis knowledge.
Methods
Study design
A case-control study was conducted on the users and nonusers of warfarin to assess their osteoporosis knowledge. This study design will be helpful to find the incidence of osteoporosis between patients and healthy people. This study was approved by the Clinical Research Centre of Hospital Pulau Pinang (HPP), and ethical approval was granted from the National Institutes of Health, Ministry of Health Malaysia NMRR-13-1281-18077 (Investigator-Initiated Research). This study was conducted from November 2013 to August 2014. This study included participants who are more than 18 years old for both groups. All respondents must be able to read and write in Bahasa Malaysia to answer the questionnaire. For both men and women, the exclusion criteria were as follows: prolonged immobility, chronic disease, nursing or pregnant women, patients with a history of osteoporosis and/or use of medications for osteoporosis, and participants unlike to share this study.
Study sampling and sample size
A convenience sampling method was used to recruit the required sample for this study. This study included participants who are more than 18 years old of both sexes. All respondents must be able to read and write in Malay language to answer the questionnaire. The sample size was calculated based on the sample size of unmatched case-control studies. 10 According to the previous studies, the prevalence of osteoporosis in warfarin users was 13.9% and 9.2% for nonusers. 11 Furthermore, the estimation of hip fracture in Iran in 2003 was 16% for women and 6% for men, 12 which is similar to that in Malaysia in 2005 which was 24%. 13 The level of statistical significance (α) and power of the study (1 − β) used were 0.05 and 0.8, respectively. The sample size was calculated according to unmatched case-control sample size calculator which indicated that the required sample size is 128 in each group. In addition, 20% was added to the study sample in case of missing or incomplete data. In total, the sample size was 151 in each group.
Osteoporosis knowledge test
The original osteoporosis knowledge test (OKT) is a 24-item tool with multiple choice questions which was developed by Kim, (1991) 14 to assess the general knowledge of osteoporosis. The instrument has 3 subscales: OKT risk of osteoporosis scale (items 1-9), OKT exercise scale (items 10-16), and OKT calcium scale (items 17-24). The OKT has a possible score of 0 to 24. A higher score represents a higher level of knowledge.
The tool has been used successfully in studies with many populations and has been translated into several languages. It was designed to determine the knowledge of osteoporosis risk factors and the way to prevent the disease according to exercise and calcium intake. Therefore, the instrument has 2 subscales: OKT exercise and OKT calcium. The total possible score of the OKT ranges from 0 to 24. Higher scores indicate a better knowledge level of osteoporosis. 14 This study was conducted using the OKT. After obtaining permission for using the OKT questionnaire from the original author, forward translation to the Malay language was done by language experts in the School of Languages, Literacies and Translation, Universiti Sains Malaysia. The questionnaire comprised 2 sections. The first section was used to obtain the sociodemographic information of the participants, including sex, age, employment, family history of fracture, education level, and financial status. The second section was used to assess osteoporosis knowledge. A pilot study was conducted among 30 subjects from controls and patients at the community and outpatient clinic of HPP in Penang State. An acceptable reliability value of this questionnaire was obtained after statistical analysis (Cronbach α = 0.705).
Data collection method
A self-administered questionnaire was used for data collection after screening the bone mineral density (BMD) of the participants using quantitative ultrasound (QUS). The calcaneus was the first site to be investigated with QUS. 15 The speed of sound (SOS), in meters per second, and broadband ultrasound attenuation (BUA), in decibels per megahertz, were used as a measure of frequency-dependent attenuation of the ultrasound wave passing through the heel 16 —methods used to detect the status of the osteoporosis condition. 17 For the patient group, users of warfarin for more than 1 year were invited from the outpatient clinic in HPP. In addition, the control group included healthy adult volunteers (nonwarfarin user) from the community in the State of Penang. All participants provided written consent prior to participation, and all the personal information collected was considered confidential in this study. A total of 270 questionnaires were successfully completed and returned to the researcher on the spot. The time taken to fill the questionnaire was approximately 10 minutes.
Data analysis
The data were analyzed by SPSS. 18 The results were expressed using descriptive and inferential statistics with 95% confidence level and P value of less than .05 which was considered significant. For the purpose of the analysis, both groups were combined to find the factors that affect the osteoporosis knowledge in the study sample. However, the Kruskal-Wallis test was used to find the differences between race, education levels, and monthly income, whereas the Mann-Whitney test was used to find the differences between 2 groups, such as sex, age group, family history of osteoporosis, family history of fracture, smoking status, alcohol habit, employment status, living place, and use of warfarin. A cutoff point of 14 was used to categorize the osteoporosis knowledge scores into low and high levels. The best cutoff was chosen according to the agreement between the total OKT-M score and the QUS parameter. 19 For the incidence of osteoporosis, the T score was measured to identify BMD. This measurement was based on World Health Organization criteria, which had been standardized by the manufacturer for the Asian population. In addition, the osteoporotic condition was stratified into 2 groups: low risk of abnormal BMD (T score >−1) and high risk of abnormal BMD (T score ⩽−1). 17
Results
Sociodemographic information of the respondents
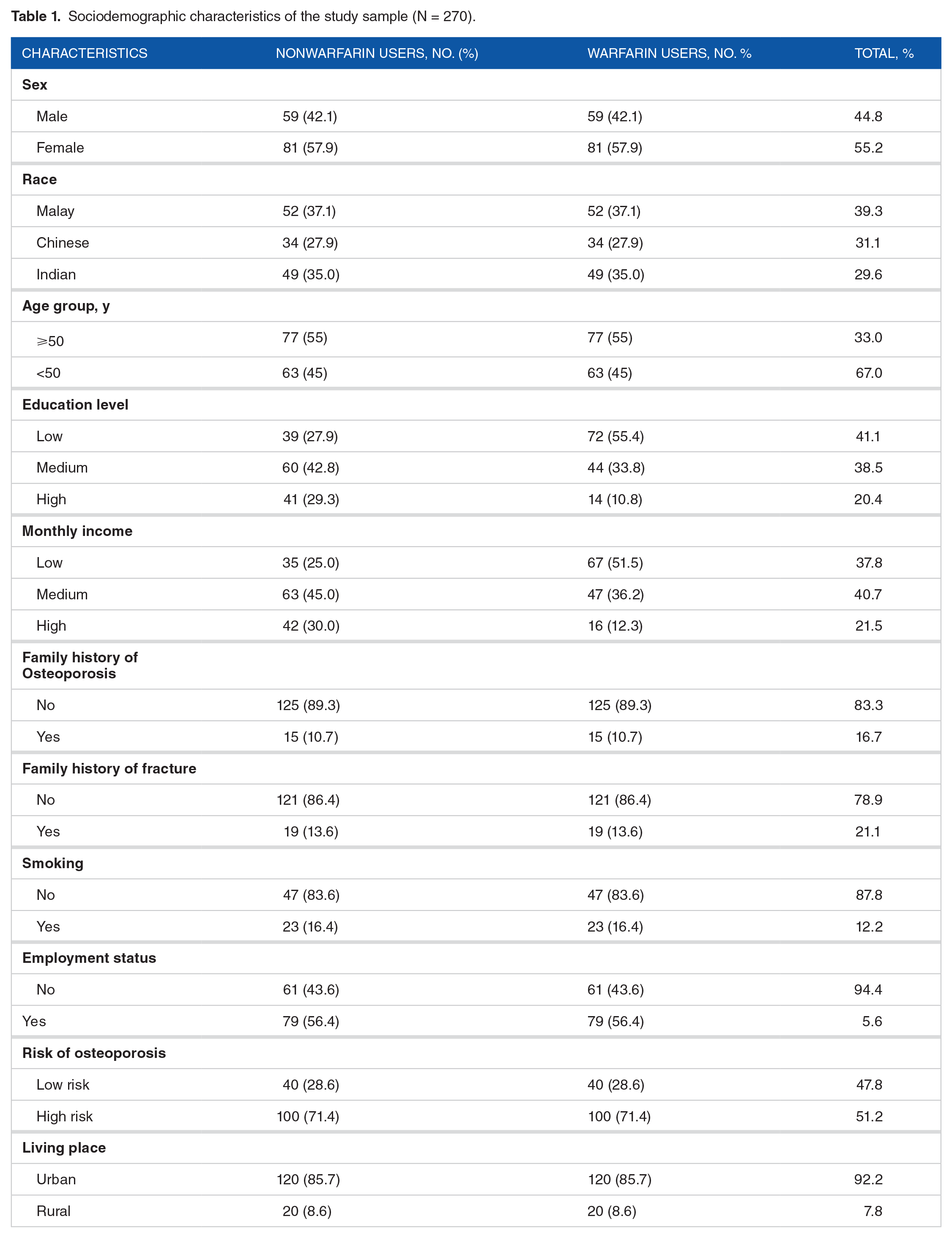
A total of 270 participants were recruited, of which 130 were patients (68 women and 62 men) with a mean age (±SD) of 65.06 ± 11.37 years who were long-term warfarin users (Table 1) and 140 were controls (nonwarfarin users) (81 women and 59 men) with a mean age (±SD) of 46.56 ± 14.55 years.
Sociodemographic characteristics of the study sample (N = 270).
Osteoporosis incidence
The incidence of osteoporosis risk was determined based on the T-score value of QUS which indicated that 82% of warfarin users were at high risk of osteoporosis. In addition, most of the control group participants (71%) were at high risk of osteoporosis (Figure 1).
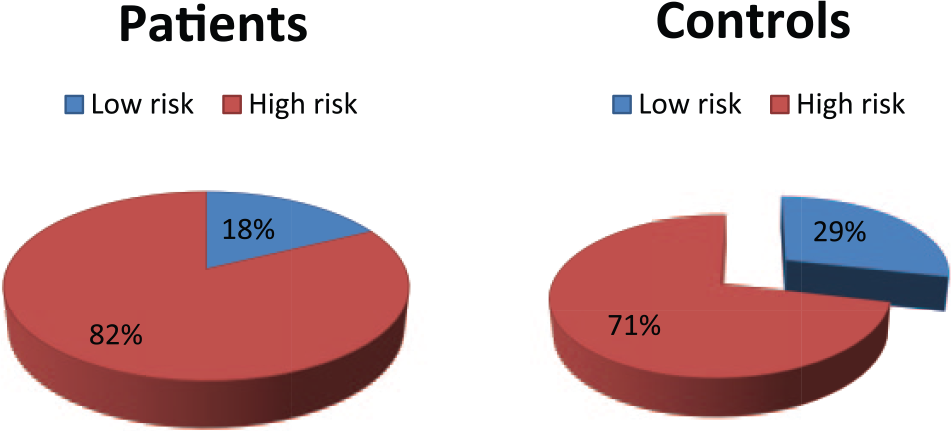
Incidence of osteoporosis in patient and control groups.
Knowledge of osteoporosis
Most of the respondents have incorrectly answered the questions relating to risk factors of osteoporosis, such as the impact of ovary surgically removed (89.3%), taking cortisone (85.2%), having a mother or grandmother diagnosed of osteoporosis (78.1%), being menopausal (73.7%), and having big bone (61.5%) (Table 2). In addition, most of the respondents did not know that hard exercise makes bone strong (74.8%), the required time for exercise (66.7%), the best type of exercise that reduces the chance of getting osteoporosis (63%), and the frequency of such exercise a week (60%). However, most of the respondents knew the foods that have a good source of calcium, such as cheese (78.1%), broccoli (63.7%), and yogurt (55.6%), whereas most of them (76.3%) did not know the recommended daily amount of calcium intake for adults.
Respondents’ knowledge about osteoporosis in patient and control groups (N = 270).
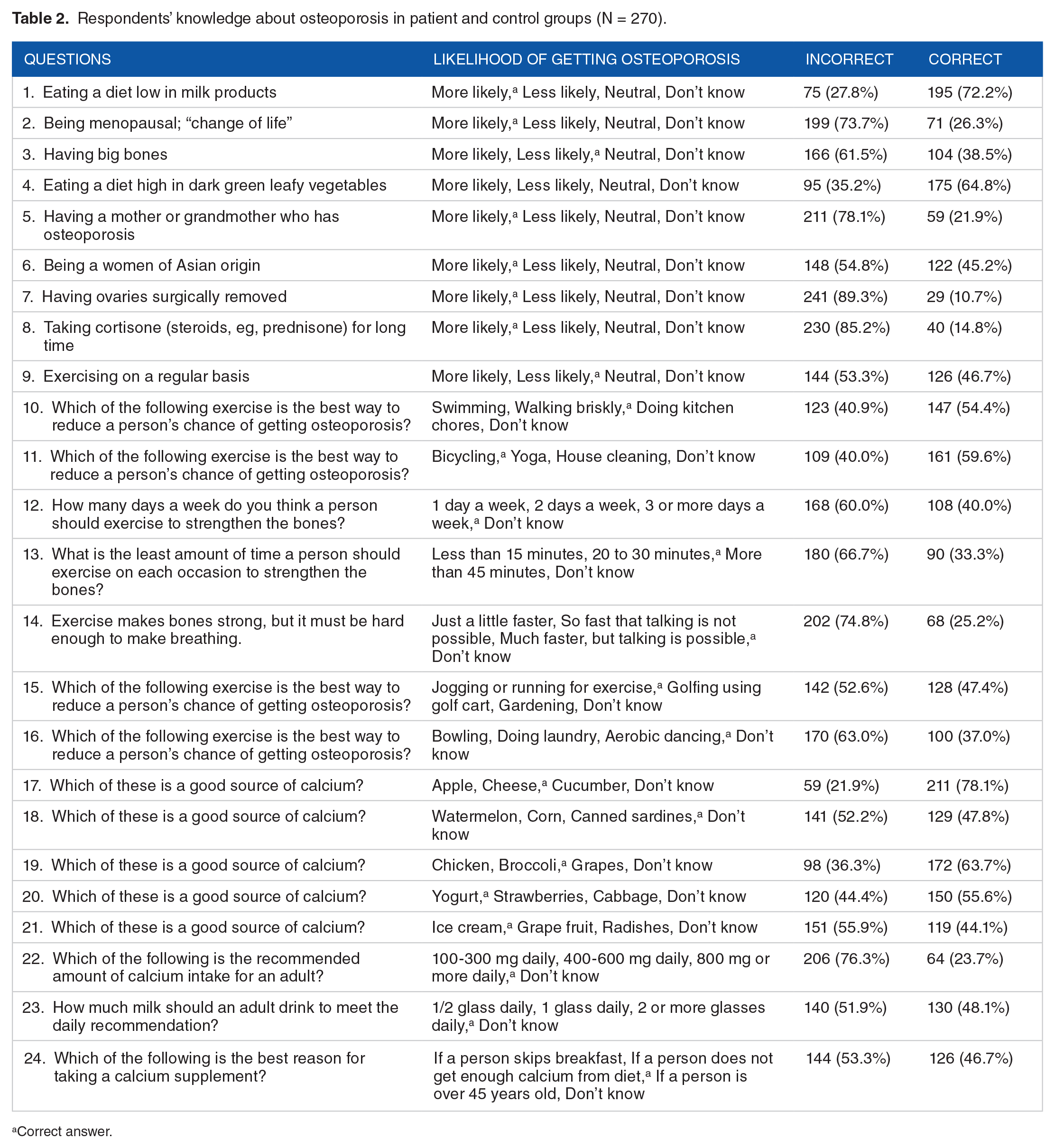
Correct answer.
According to Table 3, the average mean of total score was low (10.46 ± 2.918). The distribution of 2 levels of osteoporosis knowledge indicated that most of the respondents (84.2%) had a low level of knowledge and only 15.8% had a high level of knowledge.
Distribution of 2 levels of osteoporosis knowledge (N = 270).
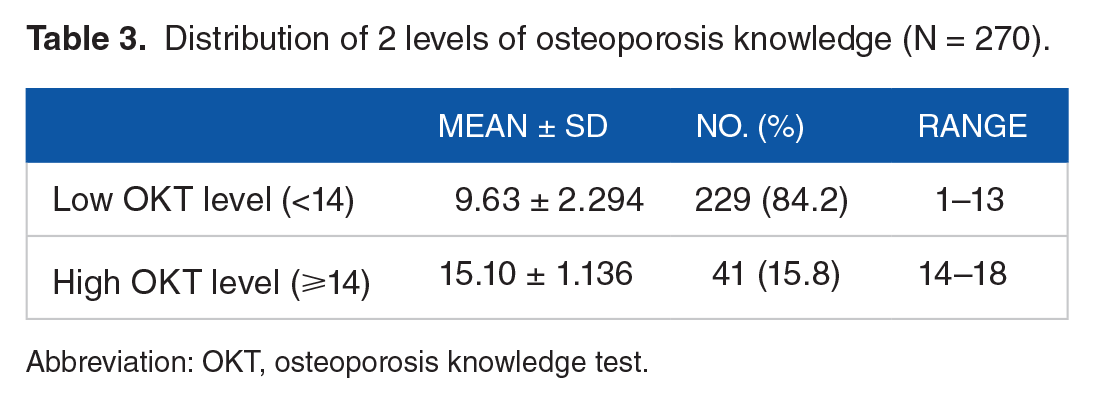
Abbreviation: OKT, osteoporosis knowledge test.
According to the level of osteoporosis knowledge in both groups, Figure 2 shows that most of the patients (76%) and 92% of the control group have a low score of osteoporosis knowledge.
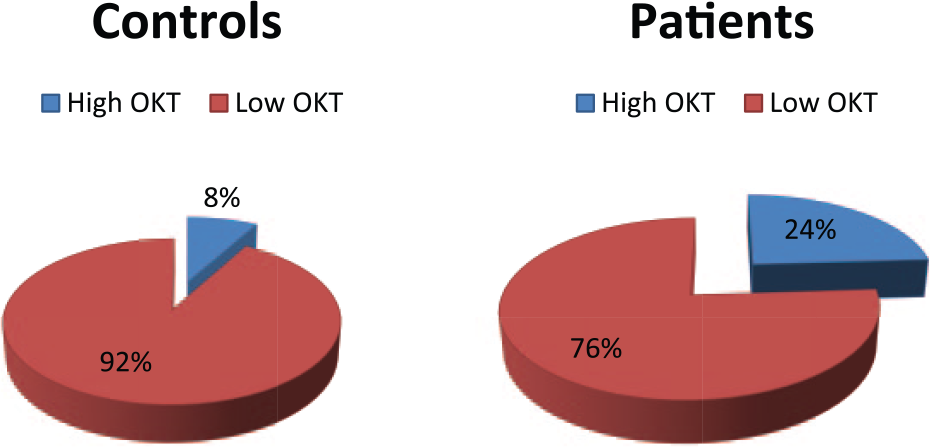
Level of osteoporosis knowledge in patient and control groups.
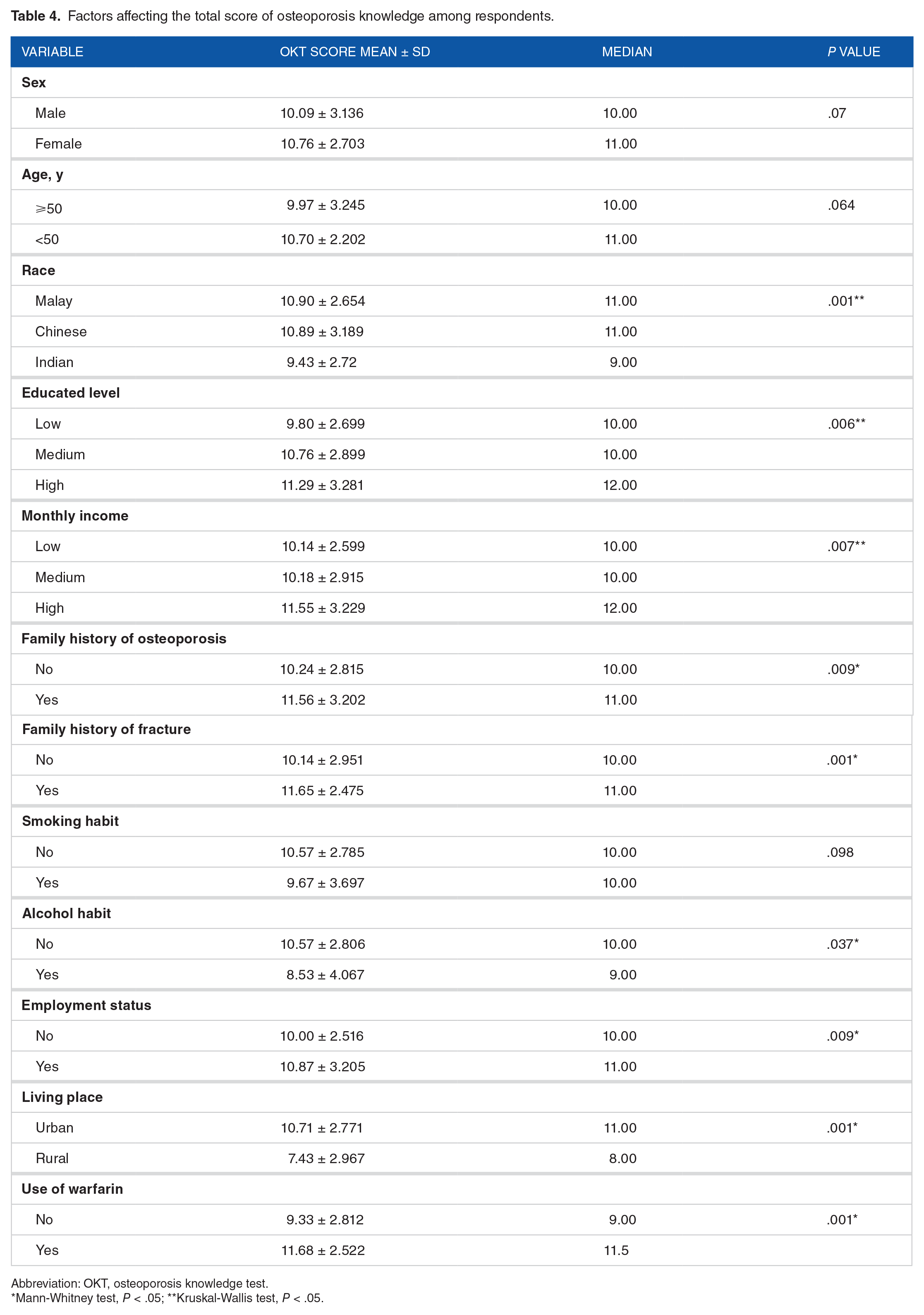
It can be seen from Table 4 that the total score of osteoporosis knowledge was significantly affected by the sociodemographic data of the respondents. Indian respondents have lower score of knowledge compared with Malay and Chinese respondents (P = .001). However, respondents with high education level and high monthly income were more knowledgeable compared with respondents with low education level and low monthly income (P < .05). In addition, family history of osteoporosis and fracture, nonalcoholic drink, employed people, living in urban places, and warfarin users were significantly associated with high score of knowledge about osteoporosis and bone health.
Factors affecting the total score of osteoporosis knowledge among respondents.
Abbreviation: OKT, osteoporosis knowledge test.
Mann-Whitney test, P < .05; **Kruskal-Wallis test, P < .05.
Discussion
This study showed that the incidence of osteoporosis in Malaysia was high in users and nonusers of warfarin compared with Western countries. This might be due to the fact that Asian people have lower body mass index, and lack of good bone health management. 20
This study showed that many people have inadequate knowledge related to risk factors of osteoporosis, physical activity, and calcium intake. In Asia, lower calcium intake has been reported as one of the risk factors for developing osteoporosis. 21 Malaysian studies reported a lower consumption of calcium intake of less than 500 mg/day. 22 Most people had low osteoporosis knowledge and lower calcium intake because they were unaware of the value of calcium intake. Previous community-based studies using OKT or other tests of knowledge indicated that many people still have limited osteoporosis knowledge.6,23-25 Improving people’s behavior toward healthy lifestyle is required in both sexes to increase their knowledge about bone health and prevent the incidence of osteoporosis. 26 However, osteoporosis knowledge in this study appears to be affected by socioeconomic factors, such as race, education, monthly income, family history of osteoporosis and fracture, alcohol habit, employment status, living place, and use of warfarin, which were significant factors in determining the level of the OKT exercise and calcium subscales. According to race, Indian people have lower knowledge compared with Chinese and Malays, whereas other studies demonstrated that ethnicity factor had no effect on the OKT level. 19 This might be because most Indians came from low socioeconomic families that are less likely to obtain health care information and have less access to health care services. Furthermore, the knowledge of osteoporosis was associated with people with high education level and high monthly income. Similar results showed that a higher educational level may be related to a higher income, and therefore, choosing better sources of calcium intake, such as milk and dairy products, leads to a healthier diet. 27 Previous research indicated that there was a positive correlation between knowledge of osteoporosis and higher education levels. 28 However, having a family history of osteoporosis and fracture increases knowledge about osteoporosis. This may increase the degree of knowledge about osteoporosis toward significant views by changing their lifestyle and behavior because they believed that osteoporosis has a serious impact on their personal and social life. 19 In addition, employed people, nonalcoholic people, and people living in urban places are associated with good knowledge about osteoporosis. This might be due to the high chance of getting health educational programs which talk about osteoporosis as a chronic disease and the ways to prevent it. 29 This study demonstrated that osteoporosis knowledge increased with chronic use of warfarin. The positive view toward patients who used warfarin and their knowledge was high due to advices that can be taken from health care professionals, especially the pharmacists when they visited the hospital for taking warfarin and checking their international normalized ratio. 30 It is worth mentioning that the low score of knowledge does not mean a lack of intelligence in any of the patient and control groups. In addition, due to the lack of any published data in Malaysia or any data from warfarin clinical setting worldwide, no direct comparison was made between the results of this study and other studies.
Study Limitations
This study only targeted outpatient warfarin users in HPP. It does not represent all Malaysian patients. The convenient sampling and the case-control study further limit the generalization of the finding to the entire Malaysian population. However, unequal number of ethnicity, age, and gender groups may have an impact on the results when compared with a randomized control study or a longitudinal study. The tools used to determine osteoporosis knowledge of participants might tend to report what they believe the researcher expects to see or they wish to present themselves in a socially acceptable manner. Many variables were unavailable for the study inclusion, such as the information on dietary habits or dietary calcium intake and physical activity. Assessment of these factors might provide a clearer picture about osteoporosis knowledge
Conclusions
This study showed that a low moan of correct answers of osteoporosis knowledge scores among the sample population was 43.6%. Moreover, this study demonstrated that 75.6% of 41 participants who had high osteoporosis knowledge were patients with chronic use of warfarin—participants with high monthly income or more knowledgeable compared with others. The clinical finding of this study will provide the fundamental basis for health care professionals to understand the logic and appropriate use of health services in the management of osteoporosis in Penang. With this tool, selecting and screening participants for a densitometry test and educational program are easier by applying the suggested cutoff point. The study outcomes will lead to better patient care, enhance patient quality of life, and avoid possible adverse effects. Therefore, the OKT is considered a very useful tool for scientific researchers. Moreover, it can be used to identify an individual’s need for a bone health–promoting intervention regarding lifestyle behavior. This study claims that knowledge about osteoporosis among patients taking warfarin and control group was low. This study helps to increase people’s knowledge in the management of osteoporosis, thus improving their behavior in caring for bone health. This includes the improvement of knowledge on suitable physical activities and dietary requirements to prevent osteoporosis by maintaining the recommended daily intake of calcium and vitamin D.
Footnotes
Peer review:
Five peer reviewers contributed to the peer review report. Reviewers’ reports totaled 1207 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AH is the lead author of this article and was responsible for the study design and supervision. SA and OT provided disciplinary expertise, constant guidance during the research and assisted in multiple edits of the manuscript, figures, and tables. HA and HH assisted in data collection and data analysis.